
Abstract
Background:
Hepatocellular carcinoma is a serious health problem worldwide, especially in Asian countries, such as China. However, there are difficulties in diagnosing and treating hepatocellular carcinoma. The alteration of fucosylated proteins was closely associated with carcinogenesis. This study is designed to evaluate the early diagnostic value of associated detection of fucosylated alpha-fetoprotein (fuc-AFP), fucosylated des-γ-carboxy prothrombin (fuc-DCP), and fucosylated glypican 3 (fuc-GPC3) in hepatocellular carcinoma.
Methods:
All serum specimens collected from patients were diagnosed by complete clinicopathological examination and then subjected to the associated detection of fuc-AFP, fuc-DCP, and fuc-GPC3 by protein microarray. Canonical discriminant analysis was adopted to discriminate between the hepatocellular carcinoma group and the benign liver disease group.
Results:
A total of 51 patients with hepatocellular carcinoma and 47 patients in the benign liver disease group were included in this study. Fuc-AFP, fuc-DCP, and fuc-GPC3 were significantly higher in the hepatocellular carcinoma group than in the benign liver disease group. The sensitivity, specificity, and accuracy of canonical discriminant analysis classification were 80.4%, 97.9%, and 88.8%, respectively.
Conclusions:
Fuc-AFP, fuc-DCP, and fuc-GPC3 are effective and useful tumor biomarkers. Associated measurement of these biomarkers with canonical discriminant analysis classification is a promising method for the early diagnosis of hepatocellular carcinoma.
Introduction
Hepatocellular carcinoma (HCC) is a leading cause of cancer-related global death and the fifth most common cancer around the world.1-3 Compared with western countries, the incidence of HCC is much higher in Eastern and South-Eastern Asia, especially in china. The increased prevalence of chronic hepatitis B virus and hepatitis C virus (HCV) infection has resulted in approximately 70% of liver cirrhosis (LC).3,4 HCC has the characteristics of high morbidity and mortality, poor prognosis, difficult early diagnosis and treatment, and a low 5-year survival rate. Most patients with HCC are in advanced stages, so the treatment is palliative and will not include radical liver resection and liver transplantation. Thus, HCC has seriously depressed patients’ quality of live and has aggravated the economic burden of society. Therefore, there is an urgent need to find new biomarkers or novel methods for improving the early diagnosis rate and the survival rate of HCC.
In order to diagnose HCC early, a lot of technology (e.g. magnetic resonance imaging (MRI) and computed tomography) is currently available and often used, including massive candidate tumor biomarkers, such as Golgi protein 73(GP73),5,6 alpha-fetoprotein (AFP), glypican 3 (GPC3), 7 vitamin K absence or antagonist-Ⅱ(PIVKA-Ⅱ, also known as des-γ-carboxy prothrombin (DCP)). 8 The level of AFP especially, is currently widely applied to diagnose HCC in clinical practice. As an excellent protein research method, protein microarray has been extensively applied to measure AFP.9-11 For instance, in our previous research, we have shown that the AFP serum level can be detected faithfully and correctly by protein microarray with a sensitivity of 91.67% and a specificity of 93.24%. 12 However, the serum level of AFP could also be increased in benign liver diseases, such as LC and hepatitis, and up to 40% of HCC patients’ AFP levels can be normal. 13 Thus, the poor specificity of AFP is an inherent concern for its application in cancer diagnosis.
In Chinese and Japanese hospitals, DCP is also a commonly tested biomarker for HCC diagnosis and monitoring for tumor relapse. Studies have shown that the combined measurement of AFP and DCP was more useful than measuring AFP alone to diagnose HCC.4,14,15 Libbrecht et al. 7 have reported that GPC3 was expressed more in HCC tissues than in benign liver lesions, which correlated with the degree of dysplasia and was even positively associated with HCC-related genes. It has been estimated that GPC3 could play a more important role in HCC diagnosis than AFP. An alteration of the cellular glycosylation phenotype may affect the normal cellular biological processes, such as cell–cell interaction, and result in tumor development and progression. Abnormal protein glycosylations were closely related to carcinogenesis and metastasis formation, and provided new biomarkers for tumor diagnosis and specific targets for tumor therapeutic intervention.16,17 One of the most commonly investigated abnormal glycosylations was fucosylation. Several researchers have estimated that the abnormal enrichments of fucosylated proteins had strongly promoted tumor dissemination and growth.18-20 Some representative biomarkers, such as fuc-AFP, fuc-haptoglobin and α1-antitrypsin, have been screened for cancer diagnosis.21-23
However, the diagnostic value and the presence of fuc-DCP and fuc-GPC3 in HCC have rarely been studied. Thus, the purpose of this study is to investigate the possible diagnostic utility of fuc-AFP, fuc-DCP, and fuc-GPC3 in HCC using high through-put protein microarray and canonical discriminant analysis (CDA) method.
Materials and methods
Serum specimen collection
The serum specimens included in this study were collected from patients at the Beijing YouAn Hospital and were classified as the HCC group and the benign liver disease (BLD) group. The BLD group was set as the control. Patients in the HCC group had their diagnoses confirmed through histological findings or imaging technological characteristics, and then classified with the American Joint Committee on Cancer malignant tumors staging system (tumor–node–metastasis). Moreover, to exclude the potential HCC, the control subjects were screened by MRI. Patients who had been diagnosed with HCV, alcoholic liver disease, biliary cirrhosis, and intrahepatic cholangiocarcinoma were excluded from this study. A blood sample of 5 mL was obtained from each patient. All experimental procedures were approved by the Institutional Ethics Committee of the Beijing YouAn Hospital and informed consent was obtained from each patient before collection. Blood specimens were centrifuged at 3500 rpm/min for 30 min after clotting. The specimens were then sub-packed, coded, and stored at −80℃. (To avoid the degradation of proteins, each aliquot should not be thawed for five times before use.)
Antibodies and reagents
Rabbit horseradish peroxidase (HRP)-labeled polyclonal AFP antibody and mouse monoclonal AFP antibody were purchased from Fapon Biotech Inc. (Shenzhen, China). HRP conjugation kits were purchased from Abcam Trading Company Ltd. (Shanghai, China). Mouse monoclonal DCP antibody was purchased from Fujirebio Inc. (Tokyo, Japan). Prothrombin factor II antibody was purchased from Fitzgerald Industries International, Inc. (North Acton, MA, USA). Mouse monoclonal to human glypican 3 antibody was obtained from R&D Bio-techne China Co. Ltd. (Shanghai, China). Bovine serum albumin (BSA) and normal goat serum were purchased from Abcam Company Ltd (Cambridge, MA, USA). The Hotgen Biotech glycosyl capture spin column was supplied by Beijing Hotgen Biological Technology Co., Ltd. (Beijing, China). Chemiluminescent HRP substrate RapidStep™ ECL was purchased from Merck KgaA Ltd. (Darmstadt, Germany). Aldehyde-coated microscope slides were purchased from Shanghai BaiO Technology Co., Ltd. (Shanghai, China).
Protein microarray fabrication
Approximately 100 pL of mouse monoclonal AFP antibody solution (1.25 mg/mL), mouse monoclonal prothrombin factor II antibody (2.5 mg/mL), mouse monoclonal glypican 3 antibody (1 mg/mL), and 10% BSA were spotted on the surfaces of slides in triplicates at 8℃ with relative humidity of 50% by using the GeSiM Nano-Plotter™ Micropipetting System (Radeberg, Germany), as shown in Figure 1. BSA was spotted as a negative control. The detailed process of protein microarray making was carried out according to the manufacturer’s instructions and settings. The spotted slides were placed at 4℃ for at least 24h and then blocked with a mixed buffer (10% normal goat serum with 0.1% sodium azide) at 37℃ for 1.5h. Then all slides were briefly rinsed with 1 × PBS with 0.1% Tween-20 (PBST0.1) three times for 3 min each. The slides were dried by centrifugation in a plastic tube and then placed at 4℃ ready for use.
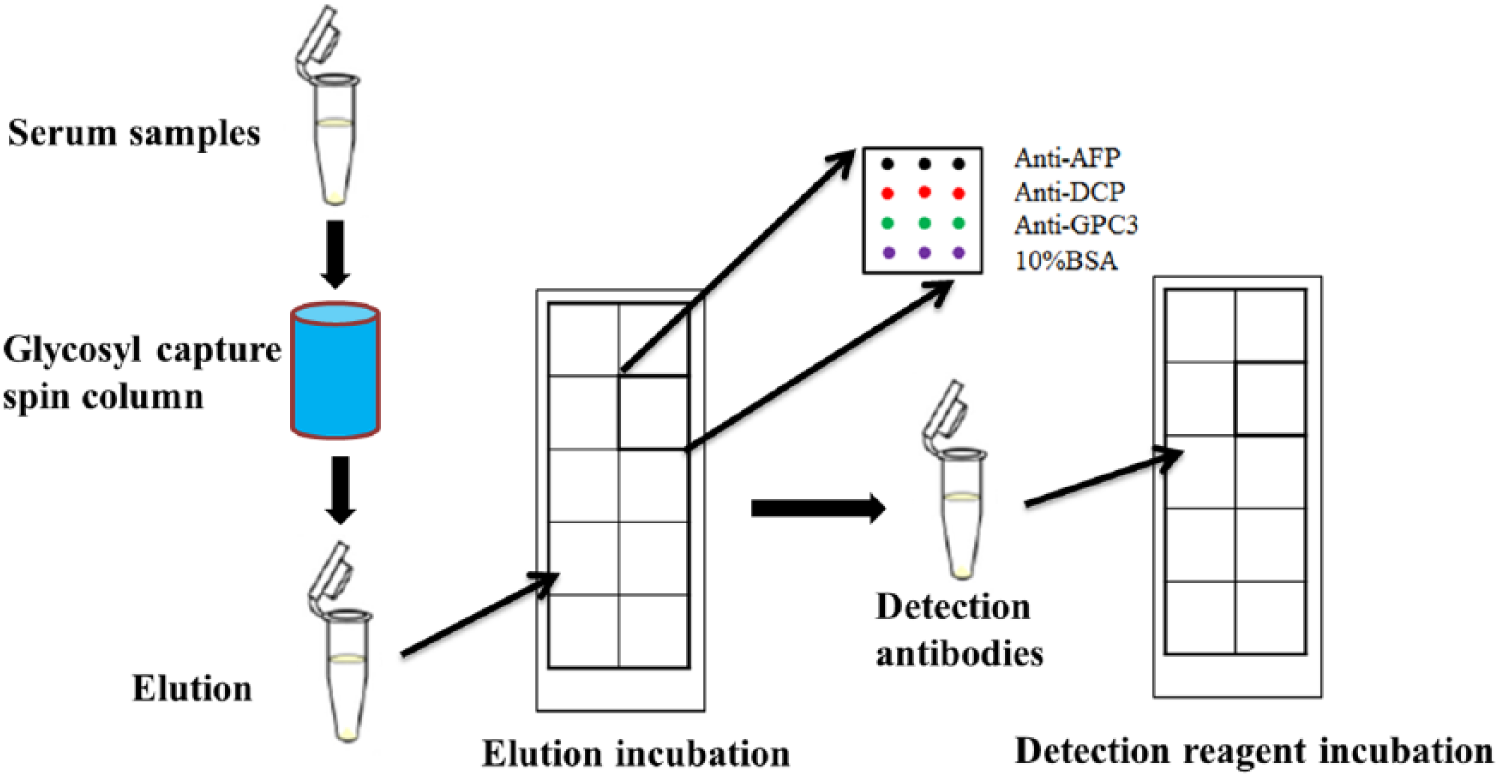
The workflow of serum alpha1,6-fucosylated protein analysis using protein microarray.
Enrichment of serum alpha1,6-fucosylated proteins
Serum alpha1,6-fucosylated proteins, including fuc-AFP, fuc-DCP, and fuc-GPC3, were enriched from serum specimens by using the Hotgen Biotech glycosyl capture spin column. This has been commonly used to detect glycosyl proteins in Chinese hospitals. The fundamental principle of the Hotgen Biotech glycosyl capture spin column is that, Lens culinaris agglutinin (LCA) is preassembled in the kit to catch the fucosylated proteins, and then monosaccharide is used to compete with the captured fucosylated proteins for binding to LCA. Thus, the serum fucosylated proteins, including fuc-AFP, fuc-DCP, and fuc-GPC3, are finally eluted out of the spin column.
Processing of antibody arrays
All serum elutions were measured by prepared protein microarrays. For the protein microarray measuring, 15 uL serum elution was added to each microscope slide and incubated at 37 for 30 min. The slides were rinsed with PBST0.1 three times for 3 min each. Then 15 uL of the mixed HRP-labeled detection antibodies, including 1 ug/mL HRP-labeled polyclonal AFP antibody, 20 ug/mL HRP-labeled polyclonal DCP antibody, and 20 ug/mL HRP-labeled monoclonal GPC3 antibody, was added to each microscope, and incubated at 37°C for 30 min again, as summarized in Figure 1. The slides were rinsed again as above. Chemiluminescent HRP substrate was added to each microscope and then the slides were scanned by a chemiluminescent scanner, Chemi DocTM MP System (Bio-Rad, CA, USA). Image Lab software Version 5 was employed to quantify the data.
Statistical analysis
GraphPad Software version 7 (GraphPad Software, San Diego, CA, USA) and SPSS version 22.0 (IBM, Armonk, NY, USA) were used to analysis the data. The test of normal distribution was conducted for all data. The Mann–Whitney test for non-normally distributed data, and the student t test for normally distributed data were applied to compare the difference between the HCC group and the BLD group. CDA was performed to distinguish the HCC group and the BLD group, and the classification results were compared with the clinicopathological diagnosis. A leave-one-out cross validation was carried out to evaluate the classificatory power of CDA. The sensitivity, specificity, and accuracy were also calculated. A P-value <0.05 was considered to be statistically significant in all instances.
Results
In this study, 51 patients in the HCC group and 47 patients in the BLD group were included. The BLD group contained 18 patients with liver cirrhosis and 29 patients with chronic hepatitis. The clinical features of all patients are summarized in Table 1. The HCC group samples show higher levels of fuc-AFP, fuc-DCP, and fuc-GPC3 than the BLD group samples (Figure 2A). The levels of fuc-AFP and fuc-DCP were significantly higher in the HCC group than in the BLD group. However, there was no statistical difference in the value of fuc-GPC3 between the HCC group and the BLD group (Figure 2B). Furthermore, the association relationship of fuc-AFP, fuc-DCP, and fuc-GPC3 in all patients was analyzed (Figure 3). The Pearson correlation coefficient of fuc-AFP and fuc-DCP was 0.528 (P <0.001). In addition, the Pearson correlation coefficient of fuc-AFP and fucGPC3 was 0.332 (P =0.001). However, the Pearson correlation coefficient of fuc-DCP and fuc-GPC3 was 0.659 (P <0.001), which showed a relatively high correlation.
Summary of patients’ demographics and cancer characteristics.
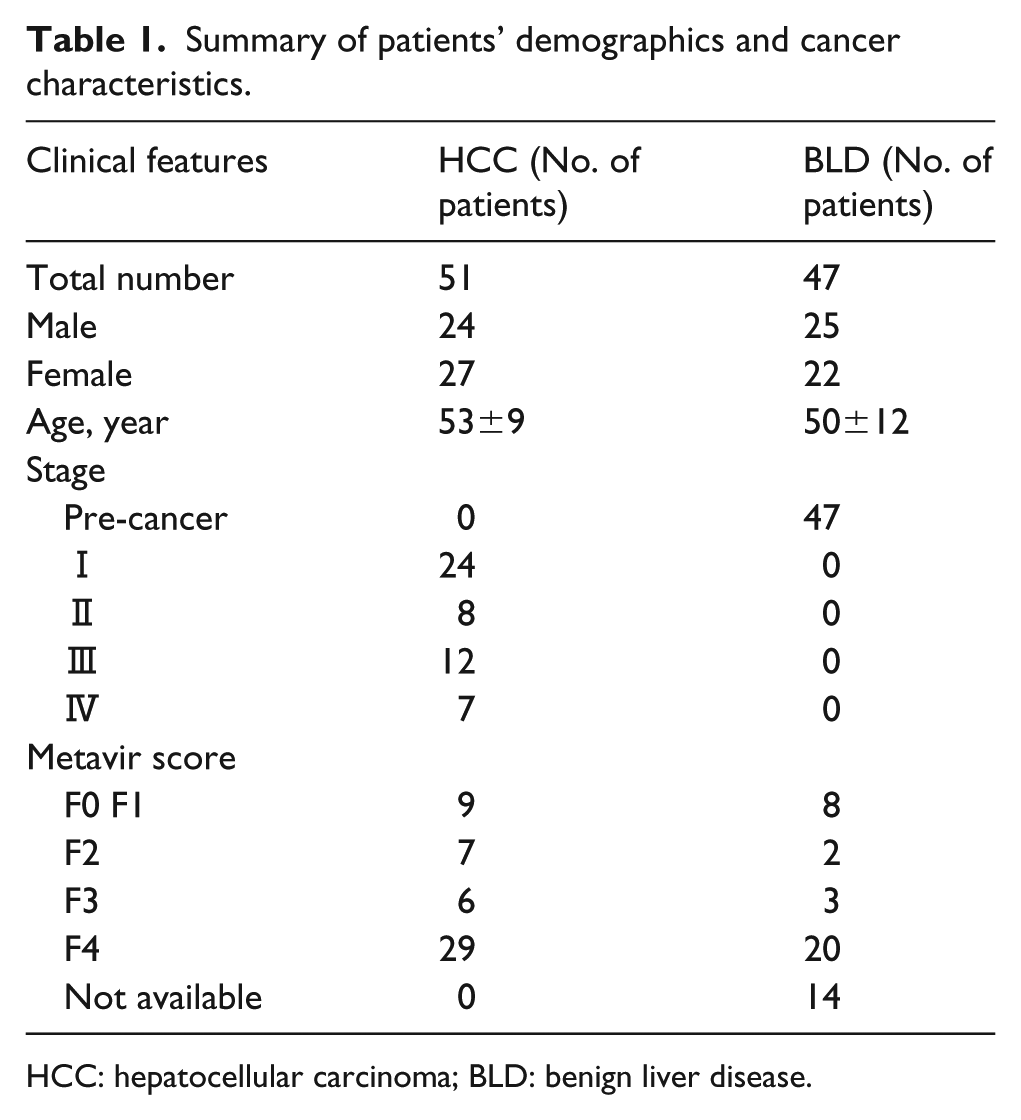
HCC: hepatocellular carcinoma; BLD: benign liver disease.
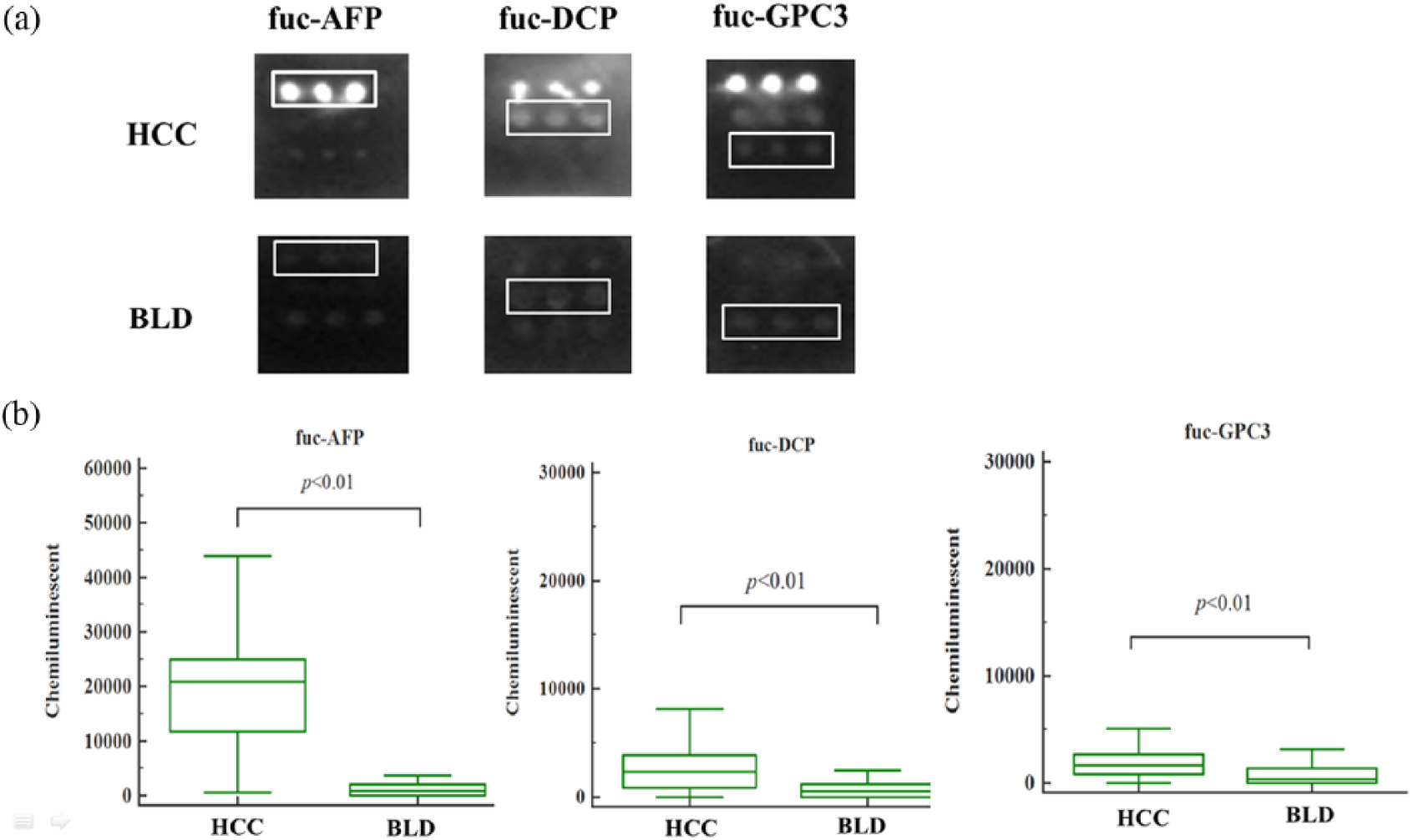
The variation of fuc-AFP, fuc-DCP and fuc-GPC3 in HCC group and BLD group sera. (a) Representative array images of the fuc-AFP, fuc-DCP and fuc-GPC3 in HCC group and BLD group. (b) The levels of fuc-AFP, fuc-DCP and fuc-GPC3 in HCC group and BLD group. HCC: hepatocellular carcinoma; BLD: benign liver disease; fuc-AFP: fucosylated alpha-fetoprotein; fuc-DCP: fucosylated des-γ-carboxy prothrombin; fuc-GPC3: fucosylated glypican 3.
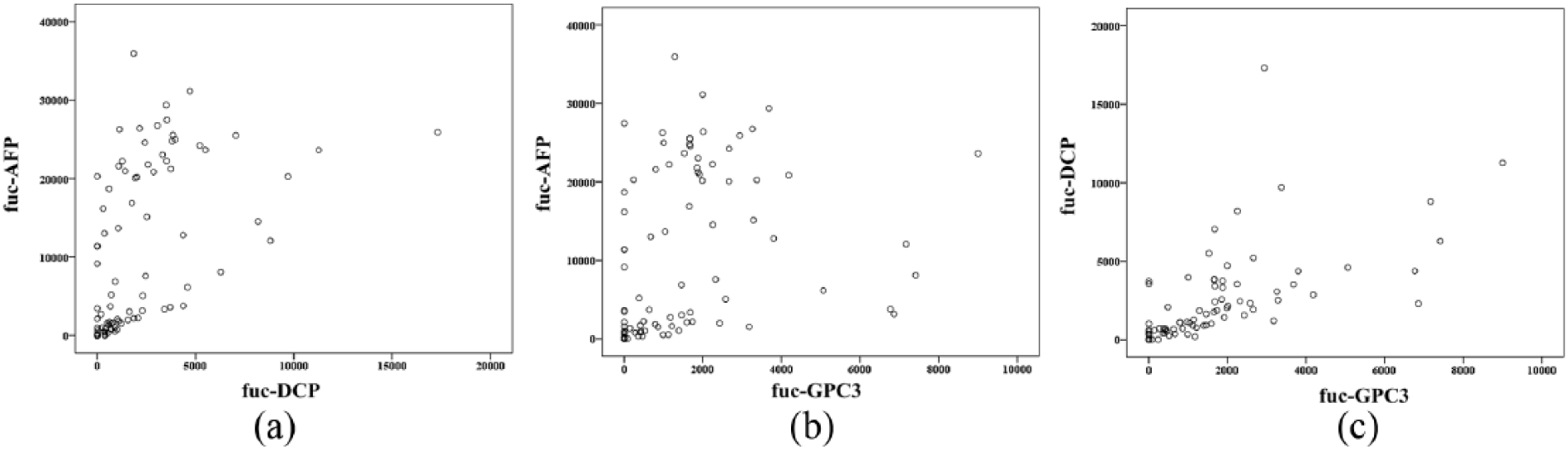
Correlation analysis of the values of fuc-AFP, fuc-DCP and fuc-GPC3 in all patients. (a) The Pearson correlation coefficient was 0.528, P <0.001. (b) The Pearson correlation coefficient was 0.332, P =0.001. (c) The Pearson correlation coefficient was 0.659, P <0.001. fuc-AFP: fucosylated alpha-fetoprotein; fuc-DCP: fucosylated des-γ-carboxy prothrombin; fuc-GPC3: fucosylated glypican 3.
The chemiluminescent values of fuc-AFP and fuc-DCP, except fuc-GPC3, were automatically selected as independent factors for the linear discriminant function of CDA. The function was listed as:
where χ1 represents the chemiluminescent value of fuc-AFP, and χ2 represents the chemiluminescent value of fuc-DCP.
The original classification and cross-validation results of CDA established by fuc-AFP and fuc-DCP are summarized in Table 2. Of the 98 patients, 42 cases were categorized as the HCC group and 56 cases were diagnosed as the BLD group. Compared with the clinicopathological diagnosis, the sensitivity and specificity of CDA were 80.4% and 97.9%, respectively, with an accuracy of 88.8%. The receiver operating characteristic curve (ROC) analysis of CDA established by fuc-AFP and fuc-DCP is presented in Figure 4, which shows the high value of the area under the curve (AUC) 0.95, with a 95% confidence interval (CI) (0.901, 0.998).
Protein microarray classification compared with clinicopathological diagnosis of HCC.
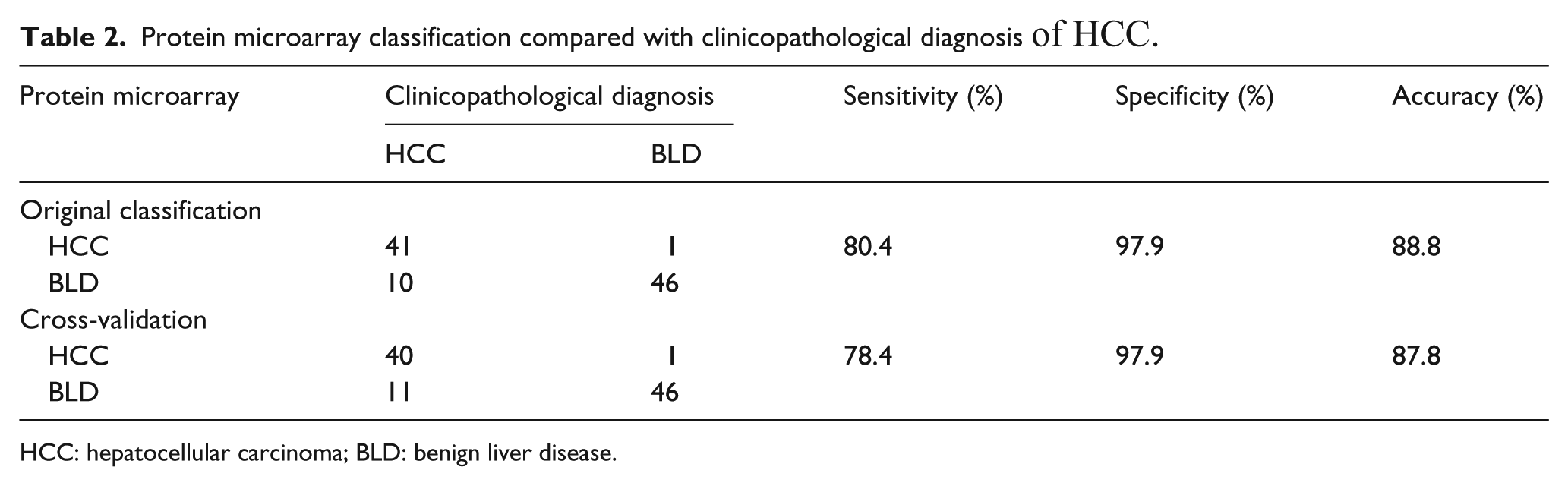
HCC: hepatocellular carcinoma; BLD: benign liver disease.
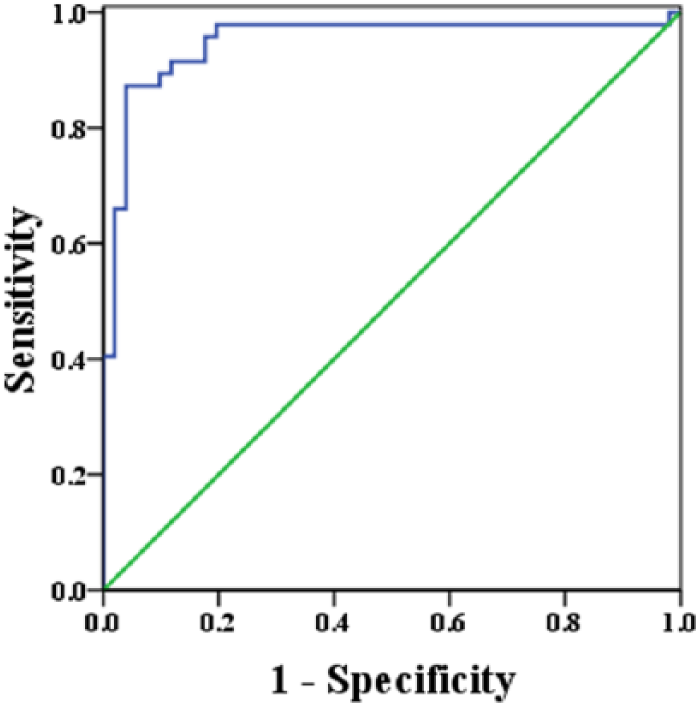
ROC analysis of CDA; the value of AUC is 0.95, 95% CI (0.901, 0.998), P<0.001. AUC: area under the curve; CDA: canonical discriminant analysis; CI: confidence interval; ROC: receiver operating characteristic.
Discussion
Protein glycosylation plays an important role in various biological processes, such as cellular differentiation, cell signaling, especially in cancer progression, tumor invasion, and metastatic potentials, which has aroused a great deal of interest in researching its alterations in various tumor transformations in the scientific community.16,24 Crucial glycosyltransferases have been intensively investigated in HCC. 16 The activity of these enzymes was closely related to the development of HCC and is very much increased in the HCC sera or tissues.
Fucosylation is one of the most commonly observed post-translation modifications in relation to types of cancer. Several fucosylated proteins have been identified by using mass spectrometry, such as fibulin-1C, GP73, hemopexin, haptoglobin, and AFP.18,25,26 Among these, fuc-AFP is the best known marker and is widely used in HCC diagnosis. Related investigations show that the level of alpha1,6-fucosyltransferase is positively correlated with the degree of dedifferentiation in HCC tissues and then with a subsequent increment of fuc-AFP, which means that the fuc-AFP level is closely related to the cancer behavior and prognosis. 27 Thus, fuc-AFP is more specific to malignant tumors rather than benign diseases, and can be used to screen and monitor patients at a high risk of progression to HCC.
Currently, DCP, an abnormal prothrombin, has been detected together with AFP for the early diagnosis of HCC in East Asian countries, such as China, South Korea and Japan. DCP has been reported as a more useful biomarker for screening small HCC with a sensitivity of 51.7% and a specificity of 86.7%. 8 However, some studies also found that the combined detection of AFP and DCP could achieve a higher sensitivity of 78.3% than testing AFP or DCP alone.28,29 GPC3, a heparin sulfate glycoprotein linked to the cell surface through a glycosylphosphatidylinositol-anchored membrane protein, is absent in hepatitis but is overexpressed in HCC tissues. 30 Several studies have reported that GPC3 could be used as a sensitive and specific serological tumor marker for HCC diagnosis.30,31 However, fuc-DCP and fuc-GPC3 have rarely been researched. Therefore, in the present study, the levels of serum fucosylated proteins, such as fuc-AFP, fuc-DCP, and fuc-GPC3, were tested together and were found to be significantly higher in the HCC group than in the BLD group, indicating their potential utility in the diagnosis of HCC. A single tumor biomarker is not sufficiently sensitive and specific for the diagnosis of HCC. Thus, in this study, fuc-AFP, fuc-DCP, and fuc-GPC3 were detected together with protein microarray and then assessed by the CDA method. Compared with the clinicopathological diagnosis results, the CDA analysis shows a strong discriminant power and the potential to distinguish HCC from benign liver diseases, with a high accuracy of 88.8%. However, the value of fuc-GPC3 was not selected as a factor to establish the above linear discriminant equation for optimal discriminant performance. The reason for this might be that there was no significantly statistical difference in fuc-GPC3 between the HCC and the BLD group. Some studies have investigated the combined diagnosis value of AFP, fuc-AFP, and DCP in HCC with a sensitivity of 40.51% and a specificity of 96.7%. 29 Our study shows a higher sensitivity and specificity than those studies, indicating that the level of fucosylated proteins may be more helpful in diagnosing HCC.
One of the limitations of this study was the relatively small number of serum specimens included. Thus, in subsequent research, our most urgent task is to include more patients from multicenter hospitals in the study. We believe that the protein microarray combined CDA method will then be more powerful. Another aspect in future research is that more emphasis should be placed on including more HCC patients at an early stage, with the aim of analyzing the early diagnostic value of fucosylated proteins.
Conclusion
This study has demonstrated that fucosylated proteins, including fuc-AFP, fuc-DCP, and fuc-GPC3, could be useful in the diagnosis of HCC. Our results also demonstrated that protein microarray combined with CDA could be an accurate and cost-effective method in HCC diagnosis with a high sensitivity and specificity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by Beijing Municipal Science & Technology Commission (D171100003117004).