
Abstract
Objective:
To investigate the clinical value of fucosylated GP73 (Fuc-GP73) levels for differential diagnosis of hepatocellular carcinoma from other liver diseases.
Methods:
Serum specimens were collected from 50 patients with hepatocellular carcinoma, 60 patients with other digestive system diseases (ODSD), and 40 normal controls. Lectin affinity chromatography column combining with the enzyme-linked immunosorbent assay (ELISA) using the ELISA index was utilized to measure the level of Fuc-GP73. By receiver operating characteristic (ROC) curve analysis its sensitivity and specificity were used to evaluate the diagnostic significance of Fuc-GP73 in hepatocellular carcinoma.
Results:
The median serum Fuc-GP73 level of hepatocellular carcinoma (20.4 μg/L) was much higher than that of ODSD patients (1.8 μg/L) and the normal controls group (0.3 μg/L), significantly (P <0.01). There was no significant correlation between serum Fuc-GP73 level and sex, age, and tumor size in the hepatocellular carcinoma group (P > 0.05); however, it was related to tumor, node, metastasis stage and lymph node metastasis (P <0.05). The area under the ROC curve (AUC) of Fuc-GP73 to detect hepatocellular carcinoma alone was 0.885; with the prespecified specificity of 95%, the sensitivity and the cutoff value were 82% and 3.1 μg/L. In addition, the combined test of Fuc-GP73 with other biomarkers can improve the clinical diagnostic efficiency; the AUC can reach to 0.983; and with the prespecified specificity of 95% its sensitivity increased to 94%.
Conclusion:
Fuc-GP73 can act as a superior glycobiomarker for the differential diagnosis of hepatocellular carcinoma; its combined detection with other biomarkers can improve diagnostic accuracy.
Introduction
Liver cancer is one of the most common malignant tumors in the world, with a high mortality rate—90% of which is hepatocellular carcinoma (HCC). 1 Among cancer-caused deaths in China, HCC accounts for one-third of deaths in males and is the second leading cause in females. 2 At present, HCC is often in the late stage when it is clearly diagnosed, which delays treatment and leads to a poor prognosis. 3
Currently, serum alpha fetoprotein (AFP) is the common biomarker used in clinical medicine for the diagnosis of HCC. However, it can be elevated, to a certain extent, in pregnant women and patients with viral hepatitis or cirrhosis, 4 which reduces its detection specificity. When the tumor is small in the early stage of HCC, the increase in AFP is often not detected; thus this reduces its sensitivity. 5 In recent years, it has been reported that one of the fucosylated AFP isoforms (AFP-L3) has a high binding affinity to lectin Lens Culinaris Agglutinin and can act as a better glycobiomarker for the diagnosis of HCC. 6 It was approved by the U.S. Food and Drug Administration (FDA) as a biomarker for HCC in 2005 and is currently widely used in Japan. 7
The glycosylation of protein is an important posttranslational modification that may contribute to the occurrence and progression of diseases. 8 It has been reported that glycosylation changes of serum proteins are closely related to the progression of cancer.9,10 The glycosylation change of Asn241 of the haptoglobin β chain in patients with HCC was significantly higher than that in patients with chronic hepatitis B and cirrhosis, 11 and the change of fucosylation as one important type of glycosylation was especially significant. 12 Therefore, the relationship between glycosylation and human disease, as well as the glycosylation of some biomarkers and cancer, has become a focus for research.
Golgi body protein 73 (GP73) is a type II Golgi transmembrane glycoprotein expressed primarily in epithelial cells and is strongly up-regulated in patients with liver diseases. 13 Our previous research results showed that the levels of GP73 in the serum of patients with HCC or small HCC were significantly higher than that of patients with other digestive system diseases and normal controls. 14 The sensitivity and specificity of serum GP73 for HCC were 72% and 95%, respectively, indicating that it could be used as an effective biomarker for the early diagnosis of HCC.15,16 Block et al. 17 used targeted glycoproteomics technology to find serum GP73 and fucosylated GP73 (Fuc-GP73) were significantly elevated in patients with HCC. Drake et al. 18 found that the altered level of Fuc-GP73 related to varying HCC disease states by lectin capture strategies combining with mass spectrometry analysis. Ma et al. 9 also testified that core fucosylation of GP73 happened in patients with HCC through his method of precise core fucosylation site identification. In addition, Jiang et al. 11 verified that the significant glycan alterations of serum GP73 in liver cirrhosis and HCC patients by antibody overlapped lectin microarrays and lectin blotting analysis.
Currently, only a few studies have focused on the clinical significance of Fuc-GP73 in the diagnosis of HCC patients, so we specifically investigated the relationship between serum Fuc-GP73 protein and HCC. In this study, we used the agglutinin affinity chromatography column and the enzyme linked immunosorbent assay (ELISA) to determine the level of Fuc-GP73 and evaluated its value as a candidate glycosylation marker for the detection of HCC before clinical application.
Material and methods
Estimation of sample size and study design
Through preliminary experiments, the sensitivity and specificity of Fuc-GP73 for differential diagnosis of HCC were found to be approximately 84% and 95%. We assumed that significant level (α) was 0.05 and allowable error (δ) was 0.10, and then Zα was 1.96 for bilateral test. According to the following formula, the sample sizes of the HCC group (n1) and the non-HCC group (n2) were calculated to be 52 and 18 cases, respectively. 19
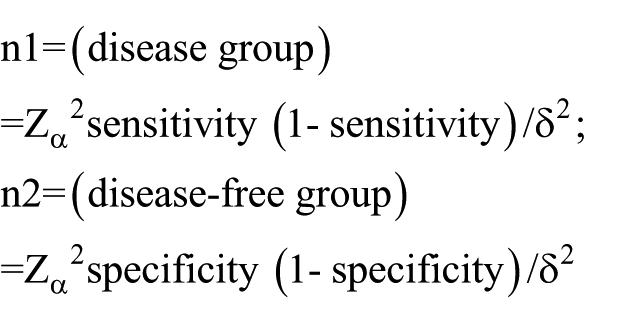
Because the Fuc-GP73 protein is stored at −80℃ for more than 6 months with a certain degree of degradation, which can affect the detection results of sensitivity and specificity, so in this study we collected limited serum specimens of HCC patients within 6 months. Only 50 patients with HCC were used to investigate the diagnostic significance of Fuc-GP73. Nevertheless, more extensive multicentric data will be obtained in further studies.
The study was performed as a case-control design: the HCC disease group comprised 50 cases; the non-HCC group comprised 60 cases of other digestive system disorders (ODSD); and the control group comprised 40 cases of normal controls (NC). The diagnostic significance of individual and combined tests were evaluated by the sensitivity and specificity through receiver operating characteristic (ROC) analysis.
Preparation of patients
A total of 150 samples were obtained from the inpatients, outpatients, and healthy individuals in the First Hospital of Qinhuangdao, from July 2016 to December 2016. Informed consent was obtained from each patient and this study was approved by the Research Ethics committee of the First Hospital of Qinhuangdao. Such samples comprised of 50 cases of HCC, 60 cases of ODSD, and 40 cases of NC. Among them, the 50 HCC patients all conformed to the diagnostic standard of “NCCN Clinical Practice Guidelines in Oncology of 2015.” 20 All of them were definitely diagnosed with HCC by pathological examination that as the gold standard method, and they did not have surgical treatment, interventional therapy, chemotherapy and molecular targeted therapy, the staging of HCC follows the tumor, node, metastasis (TNM) staging standard of NCCN guidelines. The detailed clinical characteristics data of the HCC patients are provided in Table 1 and Table 2.
Clinical characteristics of every group patients.
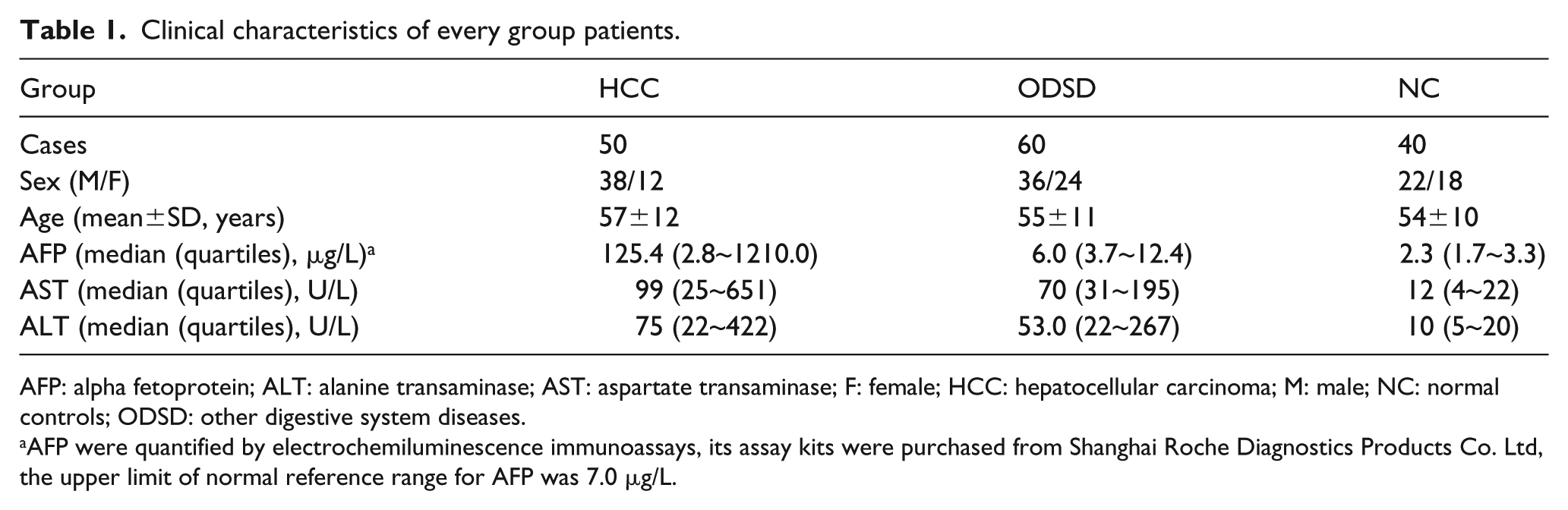
AFP: alpha fetoprotein; ALT: alanine transaminase; AST: aspartate transaminase; F: female; HCC: hepatocellular carcinoma; M: male; NC: normal controls; ODSD: other digestive system diseases.
AFP were quantified by electrochemiluminescence immunoassays, its assay kits were purchased from Shanghai Roche Diagnostics Products Co. Ltd, the upper limit of normal reference range for AFP was 7.0 μg/L.
Relationship between serum Fuc-GP73 expression and clinical characteristics in patients with HCC.
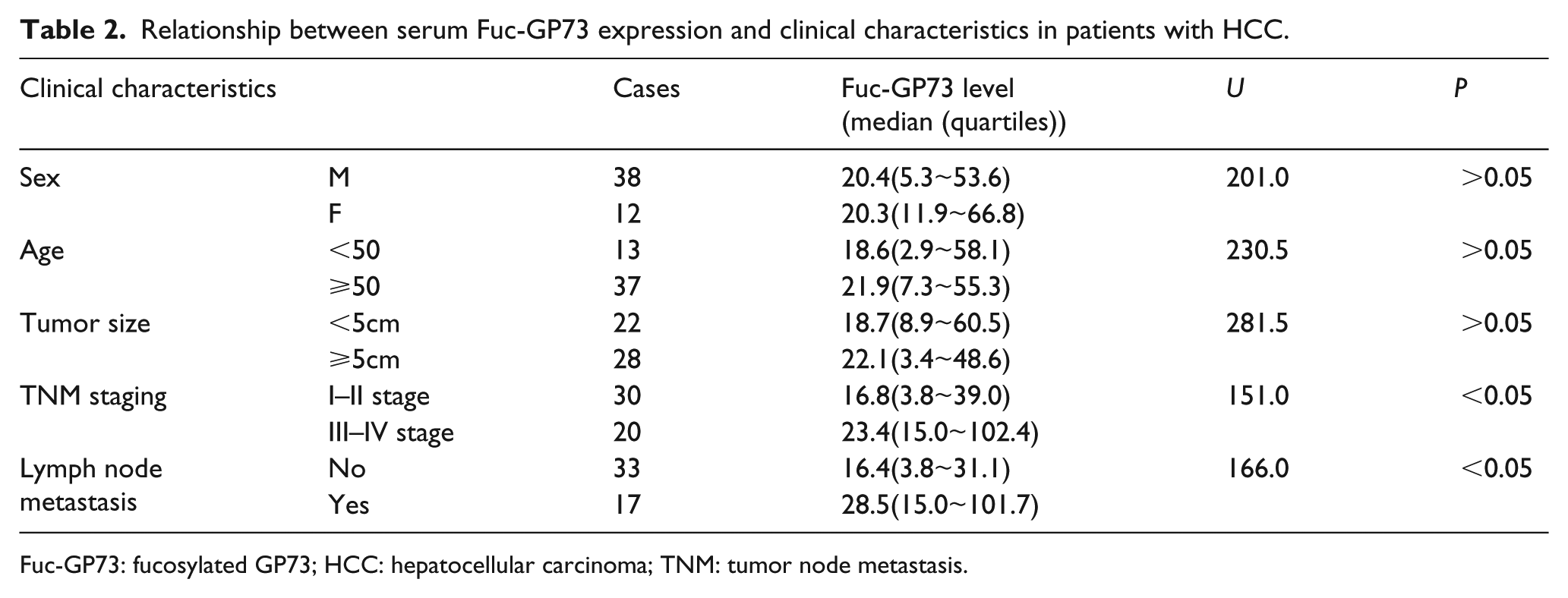
Fuc-GP73: fucosylated GP73; HCC: hepatocellular carcinoma; TNM: tumor node metastasis.
The 60 cases in the ODSD group comprised 20 cases of hepatitis, 20 cases of liver cirrhosis, and 20 cases of malignant tumors of the digestive system except HCC. Among them, 20 cases of hepatitis and 20 cases of liver cirrhosis were diagnosed according to the diagnostic criteria of the “Viral Hepatitis Prevention Program,” which is jointly revised by the Society for Infectious Diseases and Parasitasis and the Society for Hepatology of the Chinese Medical Association in 2000, 21 and they were not combined with other tumors. There were 20 cases of malignant tumors of the digestive system, except HCC, which included 6 cases of cholangiocarcinoma, 5 of gastric cancer, 4 of colorectal cancer, and 5 of colon cancer. Also, they were definitively diagnosed by pathological examination and conformed to the diagnosis standard of “NCCN Clinical Practice Guidelines in Oncology.”
In addition, in order to explore the significance of Fuc-GP73 more accurately, 40 cases of healthy controls aged 40~70 years were selected from 200 healthy individuals, to age-match with the HCC group. This excluded those with a history of hepatitis, cirrhosis, liver and gallbladder cysts, benign and malignant tumors, and other diseases after their medical history was taken, and a physical examination and common biochemical and immunological tests were done.
Preparation of agglutinin affinity chromatography column
A total of 1.5 g agarose gel Sepharose 4B (GE Healthcare, USA) activated by hydrogen bromide was added to 1 mmol/L HCl and was stirred for 20 minutes until it completely swelled; the upper liquid was removed and then washed repeatedly with 300 mL 1 mmol/L HCl three times. It was then transferred to a 7.5 mL coupling buffer containing 50 mg lentil agglutinin (Vetor Labs, USA) after being washed once with a coupling buffer and was lightly mixed for 2 h at room temperature. The medium was then washed once with 10 mL of a coupling buffer and transferred to the blocking buffer, which contained 0.2 mol/L glycine to incubate at room temperature for 2 h. After washing three times alternately with the acetate buffer and 0.1 mol/L tris buffer it was washed once with phosphate-buffered saline, which contained 0.1% BSA, 1 mmol/L CaCl2 and 0.1 mmol/L MnCl2; then a 300 uL coupling medium was packed into a micro centrifugal column and a 1.5 mL lectin storage buffer was added, which contained 1 mmol/L CaCl2, 1 mmol/L MnCl2, and 50 mmol/L Tris-HCl buffer, the prepared column was stored at 4 ℃ for use. 22
The purification and separation of Fuc-GP73 and its enzyme-linked immunosorbent assay
The prepared agglutinin affinity chromatography column was taken out and the liquid in the lower collection tube was discarded. The collected serum specimens were blended after thawing at 37 ℃ and 250 μL serum was taken to be diluted with 350 μL cleaning solution; then the 450 μL diluted sample was added to the prepared agglutinin affinity chromatography centrifuge column and placed for 15 min at 37 ℃; discarded the liquid in the lower collection tube and washed the column with 600 μL cleaning solution for 3 times; centrifuged the column and completely discarded the liquid in the lower collection tube, then added 450 μL eluent in column and incubated at 37 ℃ for half an hour, then centrifuged at 3000 rpm to collect eluate. 22 The level of Fuc-GP73 in the eluent was detected by enzyme-linked immunosorbent assay kit for GP73 (Beijing Rejing Diagnostics Products Co. Ltd). The detailed testing steps were strictly operated according to kit instructions.
Specimen collection
There was 5 mL of fasting venous blood collected from patients via coagulant tubes, which was then centrifuged at 4000 rpm (about 2000×g) for 20 min to separate the sera, which were stored at −80 ℃ until use.
Assessment objects
The levels of serum Fuc-GP73 and other biomarkers were determined, and the levels of different biomarkers among the groups were compared by this method: we used a prespecified specificity of 95% for the definition of cutoff values and to report the sensitivities of different biomarkers, and then compared the sensitivities using the McNemar test. By ROC analysis, the area under the curve (AUC) for the 95% confidence interval (CI), the cutoff value, and the sensitivity and specificity of biomarkers were analyzed by individual and combined assays for the diagnosis of HCC. The relationships between serum Fuc-GP73 levels and its clinical characteristics in HCC patients were evaluated. The repeatability of the detection method regarding Fuc-GP73 and the stability of the Fuc-GP73 protein were preliminarily investigated.
Statistical analysis
SPSS 19.0 was used for statistical analysis. The levels of Fuc-GP73 and other biomarkers were in a skewed distribution, using the median (quartiles) as indicators; the three groups were compared using the Kruskal–Wallis test, and further study between the two groups were compared using the Nemenyi test; the relationships between serum Fuc-GP73 levels and its clinical characteristics of HCC patients were evaluated by the Mann–Whitney U test; two mean values were compared by independent samples’ T-test; and the ROC curve analysis was used to evaluate the diagnostic significance of Fuc-GP73 or any other single biomarker in HCC. By binary logistic regression analysis, the prediction models of combined tests were established according to the ROC analysis and AUC of subjects, to assess the diagnostic sensitivity and specificity. The 95% CI for sensitivity, specificity, and cutoff were calculated by the exact Clopper–Pearson interval, and with prespecified specificity of 95%, the sensitivities were compared using the McNemar test. P <0.05 was considered statistically significant.
Results
The detection levels of Fuc-GP73 and other biomarkers in every group and the comparison between groups
Serum Fuc-GP73 levels in 150 patients were determined by Lectin affinity chromatography column combining with the ELISA assay. Meanwhile the serum levels of AFP-L3, DCP, and GPC-3 in HCC were determined through the method of our previous study, by using the corresponding commercial ELISA kits. 14 The results are shown in Table 3 and Figure 1.
Comparison of the serum Fuc-GP73 and other biomarkers levels in every group (median (quartiles), SD, CV).
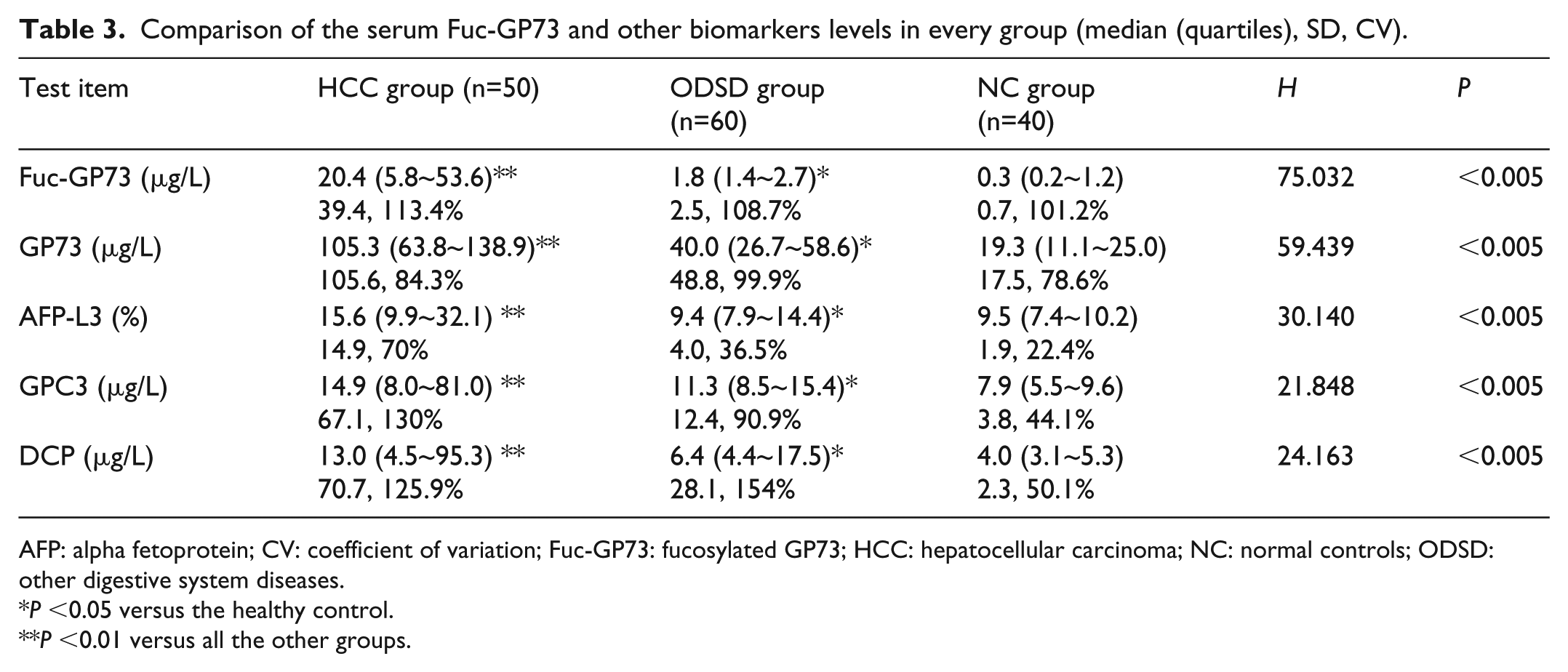
AFP: alpha fetoprotein; CV: coefficient of variation; Fuc-GP73: fucosylated GP73; HCC: hepatocellular carcinoma; NC: normal controls; ODSD: other digestive system diseases.
P <0.05 versus the healthy control.
P <0.01 versus all the other groups.
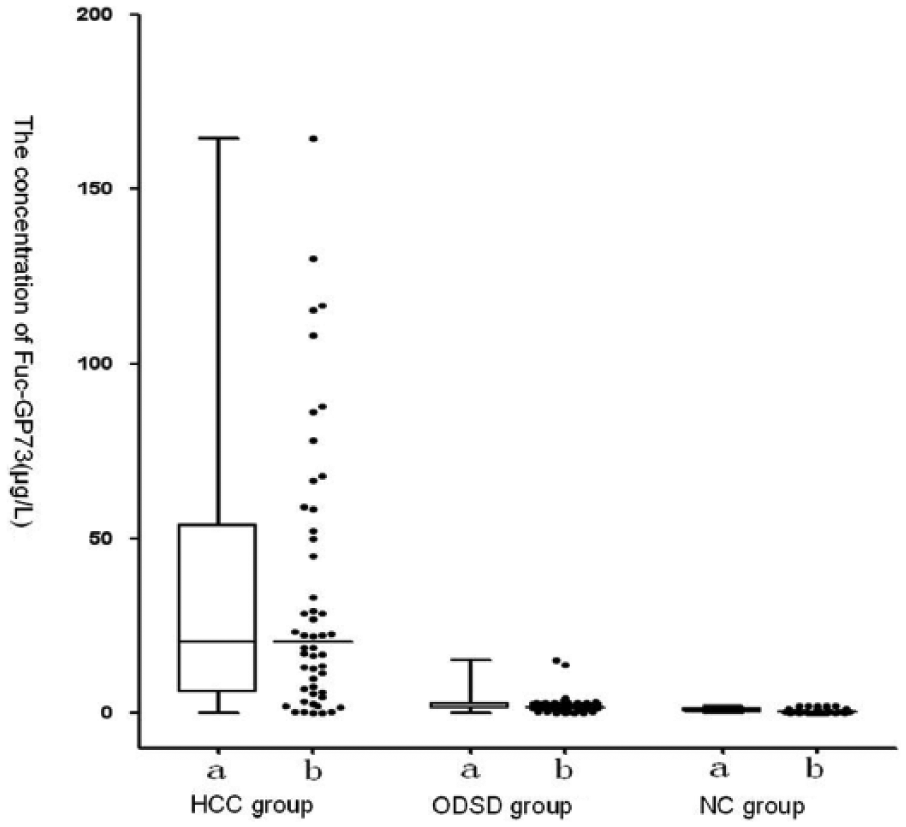
Box plots and scatter dot plots of Fuc-GP73 concentration in every group. Fuc-GP73: fucosylated GP73.
The diagnostic value of individual and combined detection of Fuc-GP73 in the diagnosis of HCC
The ODSD and NC groups were taken as non-HCC groups; the diagnostic significance of individual and combined tests were evaluated by the sensitivity and specificity through ROC analysis. The results of ROC curve analysis of Fuc-GP73 and other biomarkers in the diagnosis of HCC are shown in Table 4, Table 5, and Figure 2. The AUC of Fuc-GP73 to detect HCC alone was 0.885; with the prespecified specificity of 95%, the sensitivity and the cutoff value were 82.0% and 3.1 μg/L. In addition, the combined test of Fuc-GP73 with other biomarkers improved the clinical diagnostic efficiency, the AUC reached to 0.983 and with the prespecified specificity of 95% its sensitivity increased to 94.0%.
Area under the ROC analysis curves of Fuc-GP73 and combined with other biomarkers for diagnosis of HCC.
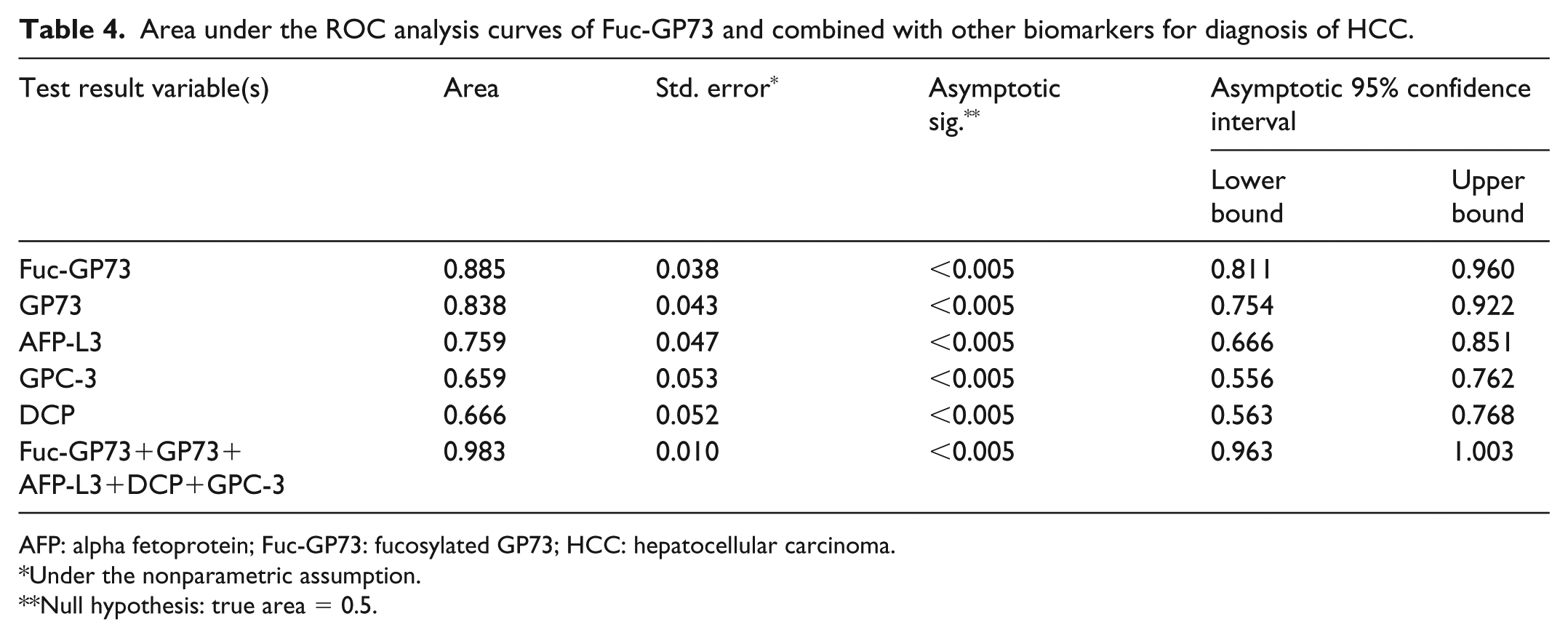
AFP: alpha fetoprotein; Fuc-GP73: fucosylated GP73; HCC: hepatocellular carcinoma.
Under the nonparametric assumption.
Null hypothesis: true area = 0.5.
Comparison of diagnosis value about Fuc-GP73 and combined with other biomarkers for HCC.
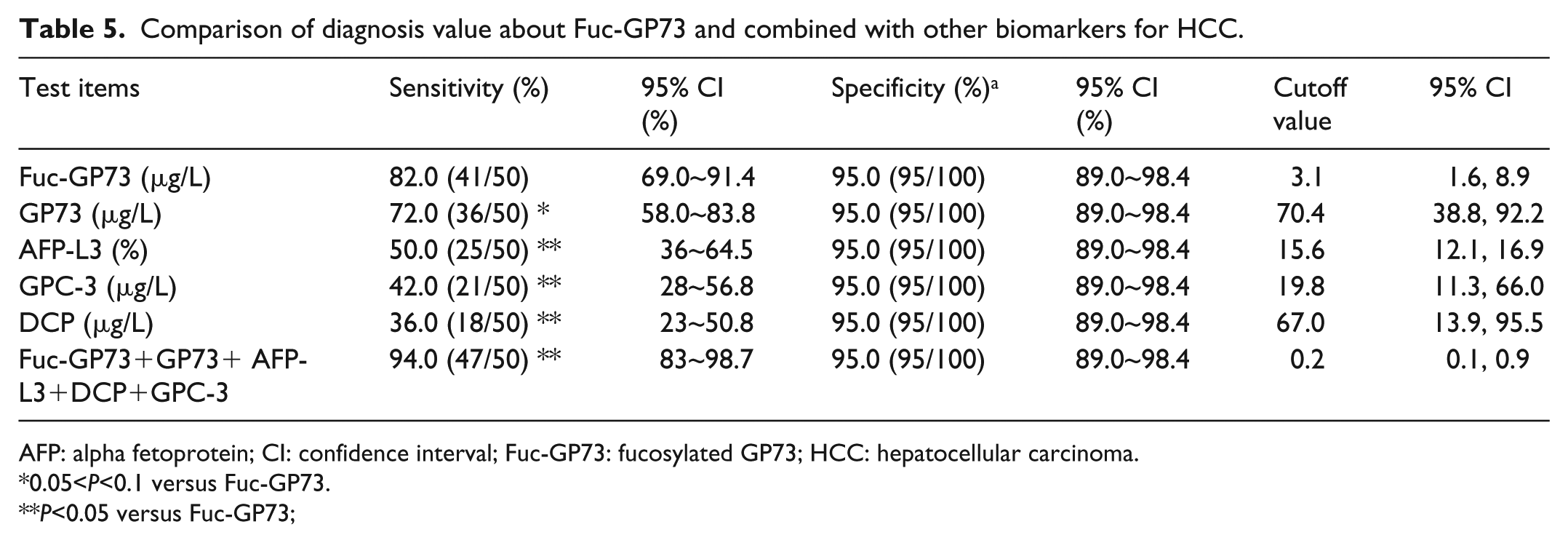
AFP: alpha fetoprotein; CI: confidence interval; Fuc-GP73: fucosylated GP73; HCC: hepatocellular carcinoma.
0.05<P<0.1 versus Fuc-GP73.
P<0.05 versus Fuc-GP73;
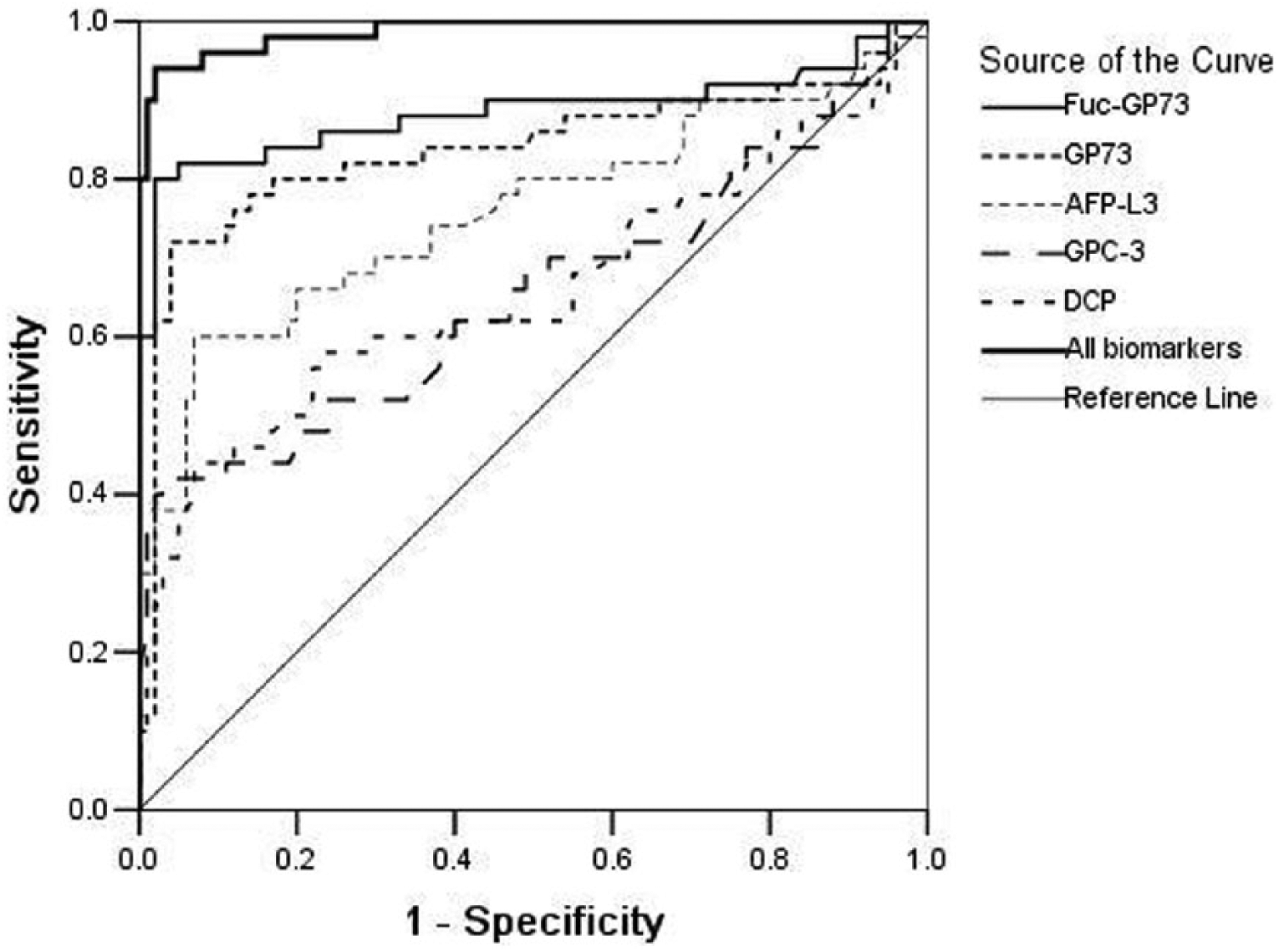
ROC analysis curves of Fuc-GP73 and combined with other biomarkers for diagnosis of HCC. Fuc-GP73: fucosylated GP73; HCC: hepatocellular carcinoma; ROC: receiver operating characteristic.
The relationship between serum Fuc-GP73 levels and its clinical characteristics of HCC patients
The results of relationship analysis are shown in Table 2. There was no significant correlation between serum Fuc-GP73 levels and sex, age, and tumor size in the HCC group (P > 0.05). However, it was related to TNM stage and lymph node metastasis (P <0.05).
Repeatability of detection method about Fuc-GP73
Three serum samples with different concentrations of Fuc-GP73 were collected and detected repeatedly five times by the Lectin affinity chromatography column combining with the ELISA assay. Using mean±SD as an indicator, the results were 6.2±0.7 (μg/L), 20.9±2.2 (μg/L), and 55.4±3.7 (μg/L), respectively, and the corresponding variable coefficients were 11.6%, 10.35%, and 6.6%, respectively.
The stability of Fuc-GP73 protein
A serum sample with concentration of 25.4±2.1 (mean±SD, μg/L) was divided into several parts and stored in −80 ℃. Every part was determined after it had been stored for 2, 4, 6, 8, and 10 months, and each determination was repeated three times. The concentrations of Fuc-GP73 protein after storage of 2, 4, 6, 8, and 10 months were 24.6±2.1, 22.7±1.9, 20.2±2.2, 18.9±2.2, and 17.6±2.0. Compared with the origin level, there were no significant differences in the results before 6 months (P >0.05), but after 6 months the concentrations of Fuc-GP73 decreased significantly (P<0.05).
Discussion
HCC as a common malignant tumor in China is often not discovered in the early stage because of its onset of concealment. AFP is the most commonly used clinical marker for the detection of HCC. Its sensitivity and specificity were found to be 52.0% and 92.5% by our previous study for the diagnosis of HCC; 15 especially for HCC with a tumor less than 3 cm its sensitivity was only 25%. 23 In order to achieve the early diagnosis of HCC, it is always the goal of researchers to seek higher sensitivity and specificity of tumor markers.
Currently, there are many reports regarding the high expression of GP73 in the serum of HCC patients. Our previous study found that the detection of GP73 had certain clinical significance in the diagnosis of HCC and small HCC,14-16 so it can be used as a reliable tumor marker for the early diagnosis of HCC and small HCC. 24 However, some studies have found that the expression of GP73 in patients with liver cirrhosis was significantly higher than in patients with liver cancer, 25 which may be related to the level of glycosylated serum GP73 and its stability. The detection of some serum glycosylated protein levels tends to increase the diagnostic effectiveness of cancer. For example, compared with total AFP, fucosylated AFP (AFP-L3) has been shown to significantly improve the specificity for HCC. 26 Today there are only a few reports about the glycosylation change of GP73 in patients with HCC, and a combination of the ELISA method and lectin is often used to determine the concentration of glycobiomarkers. 27 Therefore, by using Lin’s patent technique of purification and separation of Fuc-GP73 protein, 22 we applied the combination method of agglutinin affinity chromatography and ELISA to detect the Fuc-GP73 levels in 50 cases of HCC patients, to preliminarily investigate the relationship between the expression of Fuc-GP73 and HCC. The results showed that the AUC of Fuc-GP73 to detect HCC alone was 0.885, so it has high accuracy for the diagnosis of HCC. With the prespecified specificity of 95%, the sensitivity was 82.0%, which means it has very good sensitivity and specificity—better than AFP—in the diagnosis of HCC. However, this is lower than that reported by Drake et al. 18 using mass spectrometry (sensitivity and specificity were 90% and 100%). However, some reports have shown that its sensitivity and specificity were 85.2% and 63.0%, respectively. 11 It seems that there are some differences in the results, which may be related to the detection method, the number of cases, the origin of participants, and the heterogeneity of subgroups, which can lead to the variety of test performances. Compared with ODSD group and the NC group, the expression of Fuc-GP73 significantly increased in HCC patients. This means that the level of Fuc-GP73 has certain significance in the differential diagnosis of HCC. The expression of Fuc-GP73 in the ODSD group was also significantly higher than the NC group, which may be related to the change in normal liver structure in chronic liver disease, which leads to the ultimate decline in liver function. Because the levels of Fuc-GP73 and other biomarkers had a skewed distribution, the SD and coefficient of variation (CV) values were higher. Previous studies have found that AFP-L3, DCP, and GPC3 also have certain significance in the diagnosis of HCC.14,15 Nevertheless, limited sensitivity and specificity for the diagnosis of HCC with every biomarker alone stimulated the combined detection. As expected, through the combined detection of Fuc-GP73 and other biomarkers together, the sensitivity, specificity, and AUC were up to 94.0%, 95.0%, and 0.983, respectively, indicating better diagnostic efficacy than an individual biomarker. Therefore, in order to improve the diagnostic efficiency for HCC, Fuc-GP73 and other biomarkers, such as AFP, can be detected simultaneously in clinical work, so that they can be used for complementary diagnosis or combined analysis in HCC patients. The detection method of Fuc-GP73 is rapid and simple; therefore, it can be used for the early diagnosis of HCC.
Currently, there is no commercial kit of Fuc-GP73 on the market; therefore, the self-made agglutinin affinity chromatographic column combined with ELISA was used to determine the level of Fuc-GP73. The repeatability test showed that the detection results were relatively stable and the CV was <15%. In addition, the stability test of the GP73 protein showed that the protein degraded after being stored for 6 months at −80℃, which was significantly different from the original concentration.
Diagnostic test performances reported by some studies may be artificially overestimated if they are of a case-control design where a healthy population (“fittest of the fit”) is compared with a population with advanced disease (“sickest of the sick”); that is, two extreme populations are compared rather than typical healthy and diseased populations. 28 Therefore, there is a limitation in our research, which is known to considerably overestimate the diagnostic accuracy due to the spectrum bias.
The results of the relationship analysis between serum Fuc-GP73 levels and its clinical characteristics in HCC patients showed that there was no significant correlation between serum Fuc-GP73 levels and sex, age, and tumor size in HCC patients; however, serum Fuc-GP73 levels were related to TNM stage and lymph node metastasis. This suggests that the expression of Fuc-GP73 may have certain clinical value in monitoring the metastasis of HCC. The volumes of clinical data collected in this article were limited; our preliminary results showed that Fuc-GP73 could be used as a useful target glycoprotein for the detection of HCC; however, more definite conclusions require more clinical data. Our further studies are underway, including the collection of more extensive clinical data, and the correction of the sensitivity and specificity, to reveal the significance of individual and combined tests of Fuc-GP73 for the differential diagnosis of HCC, to explore its significance in evaluating the performance of surgical resection, to predict recurrence, and to judge the prognosis of HCC.
Currently, there are few studies regarding the molecular biological characteristics of Fuc-GP73, and many related problems remain to be solved; for example, can GP73 be divided into different subtypes like AFP? Is there an anti-Fuc-GP73 antibody to establish a rapid and accurate monitoring method for Fuc-GP73? These problems need to be further studied.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Science and Technology Project of Qinhuangdao, China (201602A108).