
Abstract
Purpose:
The incidence, pathogenesis, molecular pathways, and outcomes of colorectal cancer vary depending on the location of the tumor. This study aimed to compare the difference in tumor characteristics and the outcome between right-sided colon cancer and left-sided colorectal cancer (LCRC).
Materials and methods:
A total of 1503 patients with colorectal cancer who underwent surgery at the Taipei Veterans General Hospital between 2000 and 2010 were enrolled in this study. Right-sided colon cancer was defined as cancers in the cecum, ascending colon, and transverse colon, while LCRC was defined as cancers in the splenic flexure colon, descending colon, sigmoid colon, and rectum. The endpoint was overall survival. The mutations were detected via polymerase chain reaction and MASS array. The prognostic value was determined using the log-rank test and the Cox regression analysis.
Results:
A total of 407 and 1096 cases were classified as right-sided colon cancer and LCRC, respectively. Compared to patients with LCRC, those with right-sided colon cancer had more mucinous type cancer (7.4% vs. 3.5%), poorly differentiated tumor (11.5% vs. 3.6%), and advanced tumor-node-metastasis stage. The risk for peritoneal tumor seeding was higher in the right-sided colon cancer group (12.8% vs. 5.7%). Overall survival was better in LCRC than in right-sided colon cancer (P=0.036).
Conclusions:
In our study, right-sided colon cancer had a more advanced tumor stage, a higher risk of peritoneal metastasis, and a poorer outcome than LCRC. Moreover, right-sided colon cancer had more gene mutations in BRAF, KRAS, SMAD4, TGF-β, PIK3CA, PTEN, AKT1, and high microsatellite instability.
Introduction
Colorectal cancer (CRC) is no longer regarded as a single disease according to recent studies. In embryogenesis, the right colon, which comprises the cecum to the proximal two-thirds of the transverse colon, arises from the midgut. Meanwhile, the left colon, which comprises the distal third of the transverse colon to the rectum, arises from the hindgut. Many studies have reported that apart from anatomic and embryologic differences, the risk factors, incidence, pathogenesis, molecular pathways, and outcome also vary in colorectal cancer depending on the location of the tumor.1,2
In 1990, Bufill et al. 1 reviewed studies that showed differences in the development and biological origins of proximal and distal colon cancer. Proximal colon cancer is a more genetically stable form of the disease, while distal colon cancer has greater genetic instability. Since then, an increasing number of studies have described the differences in colorectal cancer according to the site of the tumor. Lee et al. 2 described the differences in incidence, presentation, genetics, immunology, molecular aspects, and outcomes between right-sided colon cancer and left-sided colorectal cancer (LCRC). They reported that the incidence of LCRC was higher than that of right-sided colon cancer. However, the incidence of right-sided colon cancer has continuously increased over the years.2,4 Right-sided colon cancer tends to initially present as anemia and weight loss, while changes in bowel movement and hematochezia are the initial symptoms of LCRC. 5 Patients with right-sided colon cancer tend to be women, elderly, have more advanced tumor staging, and have a mucinous type.2,6,7 The prognosis of LCRC has improved since 1980, but that of right-sided colon cancer remains poor.2,6,8 The risk of distal metastasis, particularly peritoneal and nodal metastasis, is higher in right-sided colon cancer than in LCRC.9,10 Many studies have discussed the different treatment modalities for right-sided colon cancer and LCRC according to the molecular features of the malignancy.3,11
This study aimed to compare the differences in tumor characteristics and outcome between right-sided colon cancer and LCRC.
Material and methods
Molecular and clinicopathological data of 1503 patients with CRC were collected from previous studies.12–14
All 1503 patients underwent surgery at the Taipei Veterans General Hospital from 2000 to 2010. Exclusion criteria were preoperative radio-chemotherapy, emergency operations, or death within 30 days of surgery. Clinical information that had been prospectively obtained and stored in the database included age, sex, personal and family medical history, location of tumor, tumor-node-metastasis (TNM) stage, differentiation, pathological prognostic features, and follow-up conditions. The colon, starting from the cecum to the splenic flexure colon, was defined as the right-sided colon. Meanwhile, the colon extending from the splenic flexure to the rectum was considered as the left-sided colon. When synchronous tumors were noted, we chose the most advanced tumor as the main tumor for defining the location.
Following surgery, patients were monitored every 3 months for the first 2 years and every 6 months thereafter. The follow-up protocol included physical examination, digital rectal examination, carcinoembryonic antigen analysis, chest radiography, abdominal sonogram, and computerized tomography if needed. Positron emission tomography or magnetic resonance imaging was arranged for patients with elevated levels of carcinoembryonic antigen but with an uncertain site of tumor recurrence.
Written informed consent for sample collection was obtained from all patients. Samples were meticulously dissected and collected from different quadrants of the tumors, snap frozen in liquid nitrogen, and stored at the Taipei Veterans General Hospital Biobank.
After approval by the Institutional Review Board of Taipei Veterans General Hospital (number 2013-04-042B), samples were obtained from the Biobank. DNA was extracted using the QIAamp DNA Tissue Kit (Qiagen, Valencia, CA, USA) according to the manufacturer’s recommendations. The DNA quality was confirmed using Nanodrop 1000 Spectrophotometer (Thermo Fisher Scientific).
The MassDetect CRC panel (v2.0), which allows the identification of 139 mutations in 12 genes, was selected from hotspots found in previous studies and the COSMIC database.15,16
Polymerase chain reaction (PCR) and extension primers for the mutations were designed using MassArray Assay Design 3.1 software (Sequenom, San Diego, CA, USA). The details of the MassArray-based mutation detection methods are described in the Supplementary file. The PCR products of the multiplexed reactions were spotted onto SpectroCHIP II arrays, and the DNA fragments were resolved on MassArray Analyzer 4 System (Sequenom). Each spectrum was then analyzed using Typer 4.0 software (Sequenom) to identify mutations. In this study, we defined putative mutation as 5% abnormal signal. Putative mutations were then filtered via manual review. Any detected mutation in BRAF, KRAS, and NRAS was selected for confirmation via Sanger sequencing. The concordance of MassArray and Sanger sequencing was 99.1%.
Microsatellite instability analysis
Following international criteria, five reference microsatellite markers were used to determine microsatellite instability (MSI): D5S345, D2S123, BAT25, BAT26, and D17S250. The primer sequences for these genes were obtained from GenBank (www.gdb.org). The method for detecting MSI was performed as previously described. 17
Samples with ⩾2 MSI markers were defined as having high MSI (MSI-high), and those with 0-1 MSI markers were classified as microsatellite stable.
Statistical analysis
The statistical endpoint for overall survival (OS) was measured from the date of surgery. Patients not known to have died were censored at the date of last follow-up. Kaplan–Meier survival curves were plotted and compared using the log-rank test. The impact of clinicopathological features on OS was assessed using univariate and multivariate Cox regression analyses. The chi-square test and two-tailed Fisher’s exact procedure were used to compare the genotype frequency of the clinicopathological features. The numerical values were compared using the student’s t-test. Data were expressed as mean ± SD. Statistical significance was defined as P < 0.05. Statistical analyses were performed using SPSS for Windows version 16.0 (IBM Corp., Armonk, NY, USA).
Results
A total of 1503 patients with colorectal cancer were enrolled in this study. Of these, 407 were categorized as having right-sided colon cancer, while 1096 had LCRC. There were 31 patients (2%) with synchronous tumor, and 8 patients (2%) were defined as having right-sided colon cancer, while 23 patients (2.1%) had LCRC. No significant difference in age was noted between the patients with right-sided colon cancer and LCRC (70.9 vs. 69.8; P=0.09). A total of 989 patients (66%) were men, while 514 (34%) were women. However, the proportion of female patients was higher in the right-sided colon cancer group than in the LCRC group (42.0% vs. 31.7%; P<0.001). In terms of pathological characteristics, the Borrmann type was not significantly different between the two groups. The left colon tended to have more cases of adenocarcinoma (91.2% vs. 96.1%; P<0.001), while the right colon tended to have more mucinous type (mucin >50%) (7.4% vs. 3.5%; P=0.002). Patients with right-sided colon cancer also had more advanced TNM stage and more poorly differentiated tumors (11.5% vs. 3.6%; P<0.001) (Table 1). Another subset analysis within right-sided colon cancer, left-sided colon cancer and rectal cancer was done. The result showed that rectal cancer has similar characteristics to left-sided colon cancer but is different from the right-sided colon cancer group (Supplementary Table 1).
Epidemiological, colon tumor pathology, and tumor grade of patients with right-sided colon cancer vs. LCRC.
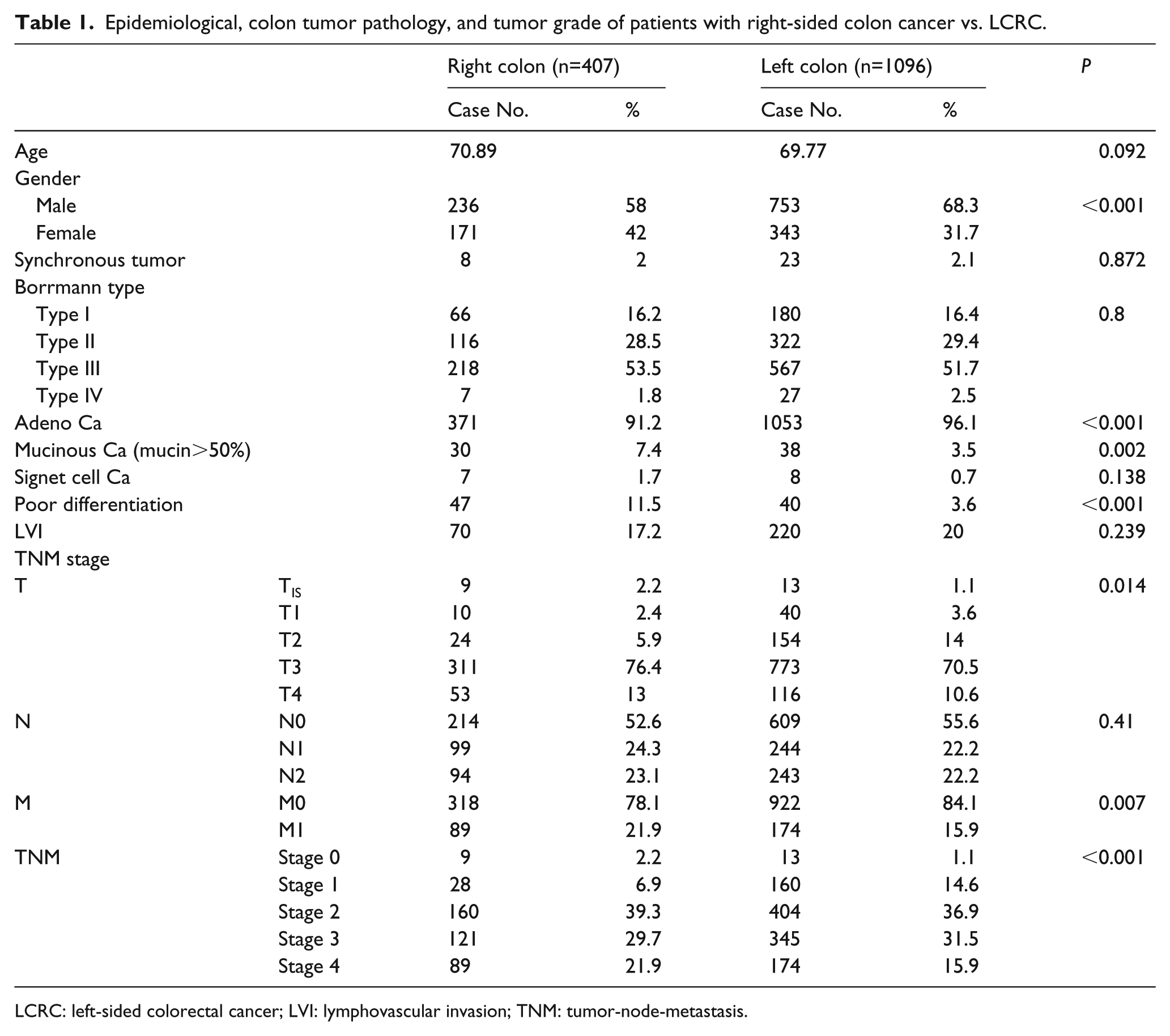
LCRC: left-sided colorectal cancer; LVI: lymphovascular invasion; TNM: tumor-node-metastasis.
In terms of molecular characteristics, gene mutations in BRAF (8.4% vs. 2.9%; P<0.001), KRAS (46.2 vs. 37.4%; P=0.001), SMAD4 (5.7% vs. 3.5%; P=0.042), TGF-β (7.4% vs. 1.6%; P<0.001), PIK3CA (18.4% vs. 12.2%; P=0.002), PTEN (1.5% vs. 0.5%; P=0.049), AKT1 (1.7% vs. 0.5%; P=0.036) and MSI-high (19.2% vs. 6.9%; P<0.001) were more abundant in the right-sided colon cancer group than in the LCRC group. On the other hand, no significant differences were noted in HRAS, NRAS, APC, TP53, and FBXW7 between the right-sided colon cancer and LCRC groups (Table 2).
Difference in molecular characteristics between right-sided colon cancer and LCRC.
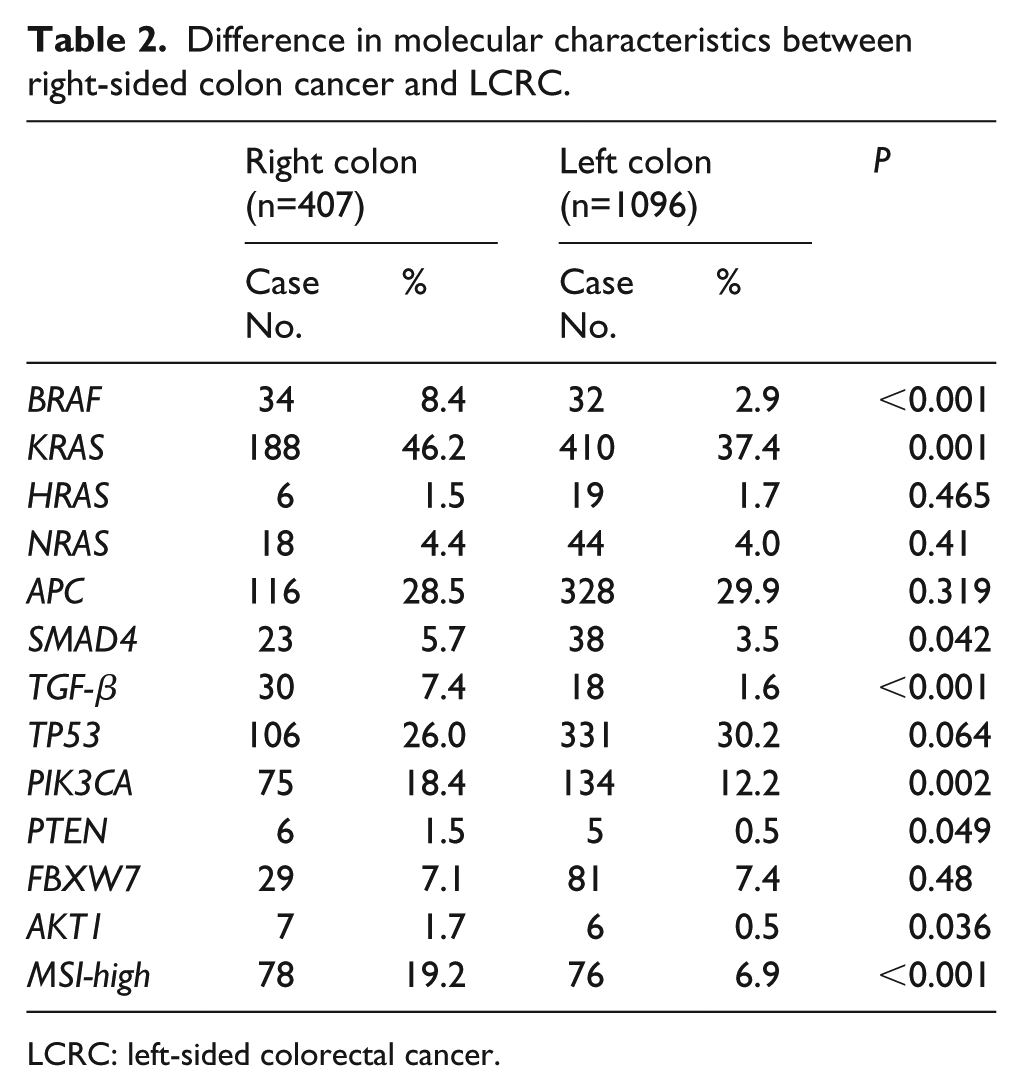
LCRC: left-sided colorectal cancer.
In terms of distal metastasis and local recurrence, there was no significant difference in incidence and metastasis number between the right-sided colon cancer and LCRC groups (34.4% vs. 31.8%; P=0.3). However, in cases of tumor recurrence, the risk for peritoneal tumor seeding was higher in the right-sided colon cancer group than in the LCRC group (12.8% vs. 5.7%; P<0.001). No difference in local recurrence or liver, lung, and bone metastasis were observed in our study (Supplementary Table 2). Survival outcomes were better in the LCRC group (146 months, 95% confidence interval (CI) 134, 159 months) than in the right-sided colon cancer group (88 months, 95% CI 81, 95 months) (P=0.036) (Figure 1). However, there was no difference in a subset analysis of OS between left-side colon cancer and rectum cancer (P=0.269) or between right-sided colon cancer, left-side colon cancer and rectum cancer (P=0.063) (Supplementary Figure 1).
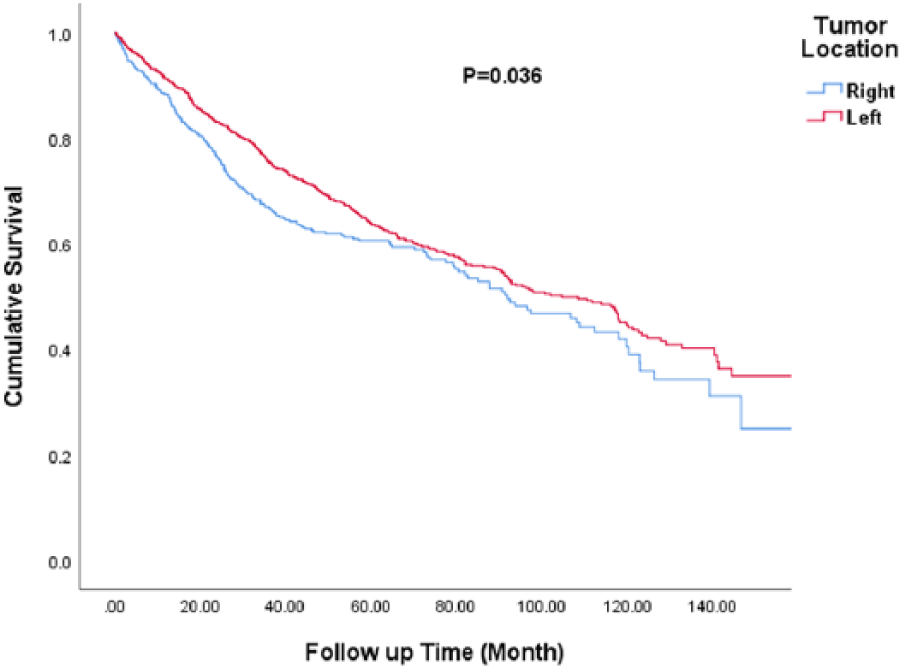
Overall survival between the right-sided colon cancer and LCRC groups, P=0.036. LCRC: left-sided colorectal cancer.
We also analyzed the difference in survival between patients according to tumor stage. However, survival outcomes were not different between right-sided colon cancer and LCRC in patients with early stage (TNM stages 1, 2, and 3; P=0.572) (Figure 2(a)) and advanced-stage (stage 4; P=0.572) (Figure 2(b)), respectively.
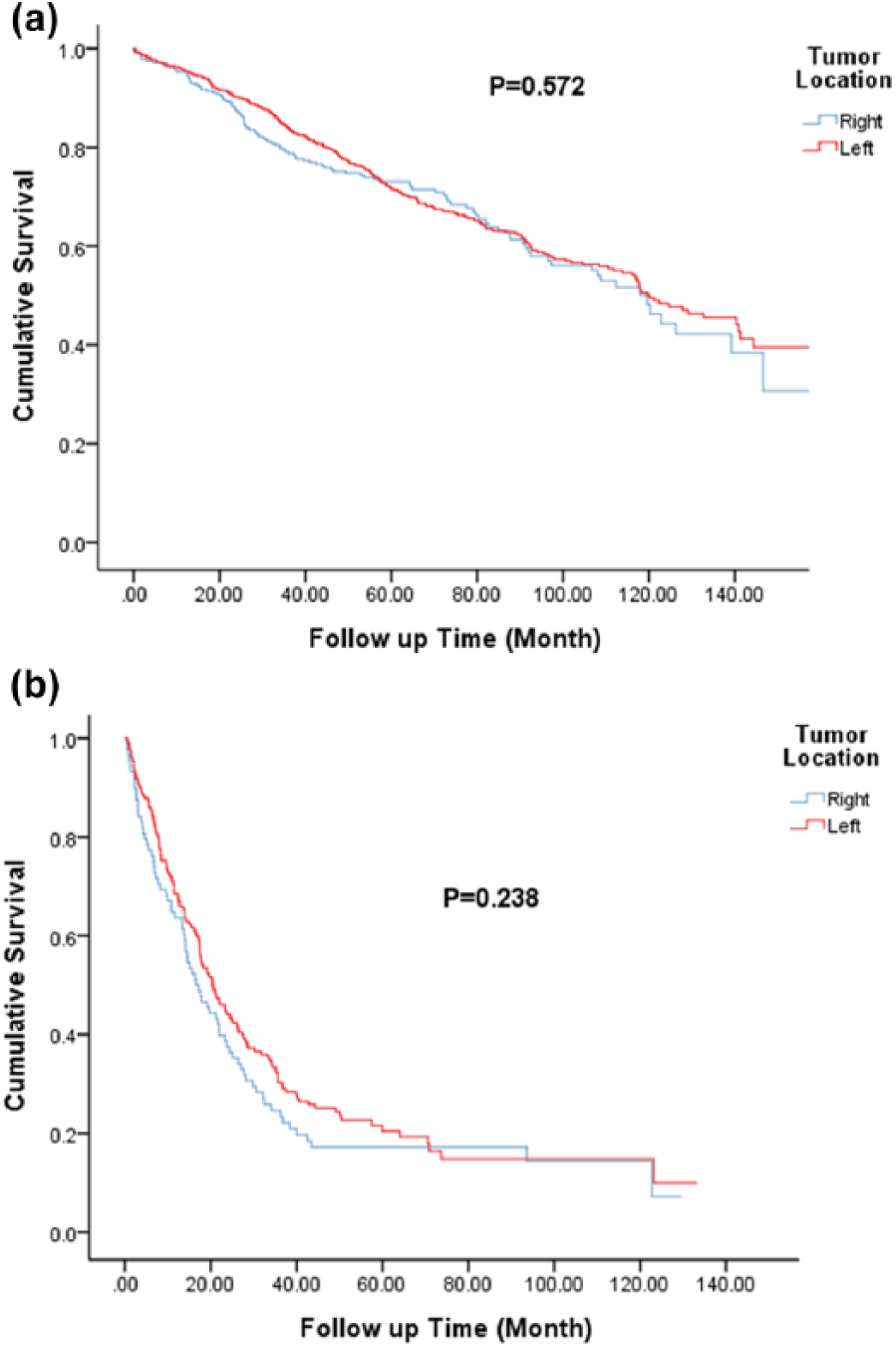
Comparison of overall survival among differently located colorectal cancers stratified by stage. (a) TNM stage 1, 2, and 3 colorectal cancers, P=0.572. (b) TNM stage 4 colorectal cancers, P=0.238. TNM: tumor-node-metastasis.
Clinical characteristics were significantly different between those with right-sided colon cancer and LCRC. Univariate analysis showed that right-sided colon cancer, old age (>70 y), male sex, mucinous adenocarcinoma, signet cell cancer, poor differentiation, lymphovascular invasion (LVI), T⩾3, N⩾1, and M=1 were poor risk factors for survival. However, adenocarcinoma cancer and TGF-β positive were good predictors of survival. Meanwhile, in a multivariate analysis, old age (>70 y), male sex, LVI, poor differentiation, N⩾1, M=1, BRAF, NRAS, and TGF-β, were independent risk factors for survival (Supplementary Table 3). Another subset analysis of survival between right-sided colon cancer and LCRC was conducted. In the right-sided colon cancer group, old age (>70 y), poor differentiation, N⩾1, M=1 were independent poor risk factors for survival in the multivariate analysis (Supplementary Table 4). In the LCRC group, old age (>70 y), male sex, LVI, N⩾1 and M=1 were independent poor risk factors, but adenocarcinoma cancer was a good predictor of survival in the multivariate analysis (Supplementary Table 5).
Patients with MSI-H were known to have better survival. We compared the impact of mismatch repair (microsatellite stable (MSS) and MSI) on survival between right-sided colon cancer and LCRC, respectively. In the right-sided colon cancer group, patients with MSI had better survival than those with MSS (P=0.006) (Figure 3(a)). However, survival was not different between those with MSI and MSS in the LCRC group (P=0.57) (Figure 3(b)).
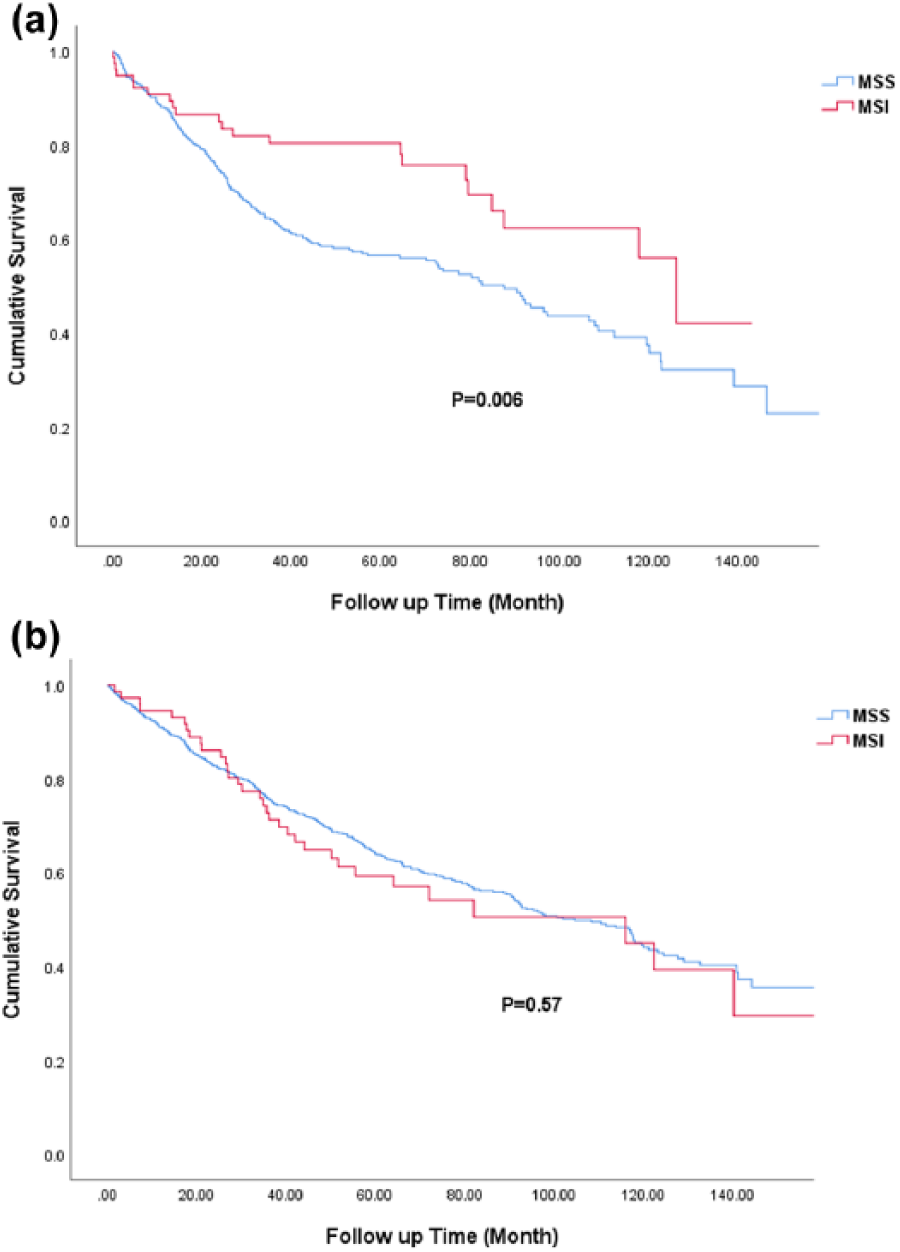
Comparison of overall survival among differently located colorectal cancers stratified by MSI status; (a) Right-sided colon cancer, P=0.006. (b) Left-sided colorectal cancer, P=0.57. MSI: microsatellite instability.
Disease-free survival (DFS) was also analyzed between right-sided colon cancer and LCRC in stage 1, 2, and 3 colorectal cancer patients. However, there was no significant difference between these two groups regarding postoperative DFS (P=0.33) (Supplementary Figure 2).
Discussion
Right-sided colon cancer and LCRC have significantly different disease characteristics due to differences in their embryological origin. Many studies focused on the differences in clinical characteristics, pathophysiology, genetic basis, and prognosis between such malignancies.1,2 These differences between right-sided colon cancer and LCRC indicate the need for different treatments and survival.3,11 In this study, we compared 1503 patients with CRC to evaluate the differences in basic characteristics, pathophysiology, and survival between those with right-sided colon cancer and those with LCRC.
Patients with right-sided colon cancer were older than those with LCRC (70.9 y vs. 69.8 y; P=0.09). The proportion of female patients was higher in the right-sided colon cancer group than in the LCRC group (42% vs. 31.7%; P<0.001). This result is compatible with other papers that showed that patients with right-sided colon cancer were significantly older and predominantly women.2,7,18 In terms of pathological characteristics, the right-sided colon cancer group had more mucinous type cancer (7.4% vs. 3.5%), more poorly differentiated tumors (11.5% vs. 3.6%), and more advanced TNM stage. The same result was reported by Yang et al. 7 who showed that the right-sided colon cancer group had more mucinous cancer, poorly differentiated tumor, and more advanced stage. Some studies suggest that there are differences in clinicopathological and molecular features between left-sided colon cancer and rectal cancer. 4 We compared a subset analysis of right-sided colon cancer, left-sided colon cancer, and rectal cancer. However, the results showed that rectal cancer had similar characteristics to left-sided colon cancer (Supplementary Table 1). These results showed that it seems reasonable to group colorectal cancer into right-sided and left-sided ones, which is compatible with other studies.7,18
In terms of molecular differences, the right-sided colon cancer group had more mutations in BRAF (8.4% vs. 2.9%), KRAS (46.2% vs. 37.4%), SMAD4 (5.7% vs. 3.5%), TGF-β (7.4% vs. 1.6%), PIK3CA (18.4% vs. 12.2%), PTEN (1.5% vs. 0.5%), AKT1 (1.7% vs. 0.5%), and MSI-high (19.2% vs. 6.9%) than the LCRC group. Missiaglia et al. 19 also reported more BRAF, MSI-H, and KRAS mutations in proximal colon cancer, which is similar to our results.
In our study, those with right-sided colon cancer tended to have more distal metastasis than those with LCRC (34.4% vs. 31.8%; P=0.3). The incidence of peritoneal seeding was higher in right-sided colon cancer than in LCRC. This finding was similar to that of one German multicenter observational study, which showed that the incidence of peritoneal carcinomatosis was higher in right-sided colon cancer, while the incidence of hepatic and pulmonary metastases was higher in LCRC. 18 However, there was no significant difference in the rate of local tumor recurrence, liver, lung, and bone metastasis in our study.
Patients with LCRC had better survival outcomes than those with right-sided colon cancer (P=0.036). However, this difference did not show in the early stage (TNM stages 1, 2, and 3; P=0.572) and advanced-stage (stage 4; P=0.572) (Figure 2). This may be due to the relatively small number of patients in our study. One systemic review performed in 2017 also showed that the risk of death was significantly lower in the LCRC group than in the right-sided colon cancer group (hazard ratio (HR) 0.82; 95% CI 0.79, 0.84; P<0.001). 20 Another report showed better outcomes in stages 1 and 2 right-sided colon cancer, while disease-specific survival was worse in those with stages 3 and 4 right-sided colon cancer. 7 However, there was no specific difference in DFS between right-sided colon cancer and LCRC in our study. This finding was compatible with one study which showed right-sided colon cancer increased the risk of death but DFS was similar between the two locations. 24
Basic clinicopathologic characteristics were significantly different between right-sided colon cancer and LCRC, which might affect patient survival. In the univariate analysis, patients with right-sided colon cancer, elderly (age >70 years), male, and with mucinous cancer, signet cell cancer, poorly differentiated tumor, LVI, T⩾3, N⩾1, and M1 had worse survival. In the multivariate analysis, old age (>70 years), male sex, LVI, N⩾1, M1, and mutation on BRAF and NRAS had poor prognosis in our study. One meta-analysis study in 2017 also showed that females had significantly better OS than males (HR 0.87; 95% CI 0.85, 0.89). 21 In the VICTOR trial, there was no difference in DFS in terms of KRAS, BRAF, NRAS, PIK3CA, TP53, and FXCW7, but DFS was better among those with MSI and chromosomal instability phenotype. 22 Adenocarcinoma cancer and TGF-β were good predictors of survival in our study. This result was also noted in another study, which reported that the mutation of the type II receptor for TGF-β1 in MSI patients had improved OS. 23 The correlation between TGF-β and MSI might have the same impact on OS. However, in the right-sided colon cancer group, only old age (>70 y), poor differentiation, N⩾1, and M=1 were independent poor risk factors for survival in the multivariate analysis (Supplementary Table 4). In the LCRC group, old age (>70 y), male sex, LVI, N⩾1, and M=1 were independent poor risk factors, but adenocarcinoma cancer was a good predictor of survival in the multivariate analysis (Supplementary Table 5).
In a previous study, patients with CRCs with MSI had a significantly better prognosis compared to those with intact MSS (HR 0.49; P = 0.013). 22 In our study, patients with right-sided colon cancer with MSI had significantly better survival compared to those with MSS (P=0.003). However, no significant difference in survival was noted in patients with LCRC between MSS and MSI (P=0.614). Overall, in this study, patients with right-sided colon cancer with MSI had the best survival, while those with right-sided colon cancer with MSS had the worst survival.
This study has some limitations. The first is its retrospective nature. We were not able to record the lifestyle factors and symptoms of disease. Second, an analysis of entire cases of colorectal cancer was not performed. In addition, some patients did not provide informed consent, and some patients with advanced stage did not agree to surgical intervention. We also excluded patients who underwent emergent operations, which was often due to the obstruction of LCRC. It may increase the incidence of right-sided colon cancer in our study. Third, we did not analyze the treatment effects for CRC, which might have an important impact on survival. More studies are needed in the future for further understanding of the impact of location on CRC.
Conclusion
In this study, right-sided colon cancer tended to develop more in women than LCRC. Although no significant differences in Borrmann type, those with right-sided colon cancer had a more mucinous type, a more poorly differentiated tumor, and a more advanced tumor stage. The right-sided colon cancer group also had a higher risk for peritoneal metastasis and poor outcome. In terms of molecular characteristics, the right-sided colon cancer group had more gene mutations in BRAF, KRAS, SMAD4, TGF-β, PIK3CA, and MSI-high. OS was better in the LCRC group. Meanwhile, in the right-sided colon cancer group, those with MSI had significantly better survival.
Supplemental Material
Supplementary_Figure_1and2 – Supplemental material for Clinicopathological and molecular differences in colorectal cancer according to location
Supplemental material, Supplementary_Figure_1and2 for Clinicopathological and molecular differences in colorectal cancer according to location by Yu-Lun Hsu, Chun-Chi Lin, Jeng-Kai Jiang, Hung-Hsin Lin, Yuan-Tzu Lan, Huann-Sheng Wang, Shung-Haur Yang, Wei-Shone Chen, Tzu-Chen Lin, Jen-Kou Lin, Pei-Ching Lin and Shih-Ching Chang in The International Journal of Biological Markers
Supplemental Material
Supplementary_tables_1-5 – Supplemental material for Clinicopathological and molecular differences in colorectal cancer according to location
Supplemental material, Supplementary_tables_1-5 for Clinicopathological and molecular differences in colorectal cancer according to location by Yu-Lun Hsu, Chun-Chi Lin, Jeng-Kai Jiang, Hung-Hsin Lin, Yuan-Tzu Lan, Huann-Sheng Wang, Shung-Haur Yang, Wei-Shone Chen, Tzu-Chen Lin, Jen-Kou Lin, Pei-Ching Lin and Shih-Ching Chang in The International Journal of Biological Markers
Footnotes
Author contributions
Pei-Ching Lin and Shih-Ching Chang contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by grants from the Taipei Veterans General Hospital (V101E2-005) and Ministry of Science and Technology, Taiwan (105-2314-B-075 -010 -MY2) and the Depart-ment of Health of Taipei City (10401-62-031; 10601-62-059).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.