
Abstract
Background:
HE4 is a useful tumor marker for the diagnosis of ovarian, endometrial, and fallopian tube carcinoma.
Aim:
The aim of our study was to investigate the value of serum HE4 compared with CA125 in the diagnosis of primary peritoneal carcinoma and the estimation of treatment response and recurrence.
Methods:
Serum HE4 and CA125 concentrations were measured in both primary peritoneal carcinoma patients and benign gynecological disease controls. The treatment response and recurrence were assessed by serum HE4 and CA125 levels in primary peritoneal carcinoma patients.
Results:
Serum HE4 and CA125 levels were significantly increased in primary peritoneal carcinoma patients compared with benign disease controls (P<0.001). Compared with CA125, HE4 had lower sensitivity (84.2% vs. 94.7%), but higher specificity (99.2% vs. 85.3%); the combination of HE4 and CA125 led to higher sensitivity and specificity. In the receiver operating characteristic analysis, the area under the curve was 0.956 for HE4, for CA125 was 0.953, for HE4+CA125 was 0.979. Furthermore, HE4 and CA125 were closely associated with treatment response, and our results indicated that primary peritoneal carcinoma patients displayed a larger drop of HE4 compared with CA125 (75.8% vs. 61.5%). Combined with CA125, HE4 elevation better predicted recurrence in primary peritoneal carcinoma patients during the remission period after treatment.
Conclusions:
This study indicated that the detection of serum HE4 changes may enhance the effectiveness for detecting primary peritoneal carcinoma and estimating the outcome of treatment and recurrence in female primary peritoneal carcinoma patients.
Keywords
Introduction
Primary peritoneal carcinoma (PPC), first reported by Swerdlow in 1959, is a rare gynecological malignancy, which is similar to stage III–IV ovarian serous carcinoma in clinical and histological features.1–3 Tumor cells in PPC patients can propagate extensively inside the peritoneal cavity involving the majority of the omentum with minimal or no involvement of the ovary. Many names are used to describe these tumors such as peritoneal mesothelioma, serous surface papillary carcinoma, peritoneal papillary serous carcinoma, and extraovarian peritoneal serous papillary carcinoma. Although some publications indicate that PPC has some similarities with ovarian serous cancer, PPC has an undefined origin site, which means that the surgery method may be different from ovarian cancer. Moreover, recent studies have indicated that there are some differences between PPC and ovarian serous cancer in molecular and epidemiological characteristic. PPC has a worse prognosis than ovarian cancer.4,5 Much of the detailed behavior of PPC remains unclear. Currently, its treatment consists of surgery and adjuvant chemotherapy, and 80% of ovarian cancer patients will obtain effective response by surgery treatment and adjuvant chemotherapy.6,7 Therefore, it is necessary to establish effective methods to diagnose PPC and monitor the results of its treatment. Before now, carbohydrate antigen 125 (CA125) was a widely used tumor marker for diagnosing and monitoring curative effect, and for evaluating recurrence. Owing to the limitation of the low specificity of CA125, human epididymis protein 4 (HE4) is often used with CA125 for elevating the specificity and sensitivity in the field of tumor diagnosis and prognosis. The specificity of HE4 is higher than that of CA125 and the HE4 concentration is correlated with tumor stage.8,9 Furthermore, many studies have indicated that HE4 is an effective marker for the diagnosis and prognosis of gynecological malignancies, such as ovarian cancer, endometrial carcinoma, and primary fallopian tube cancer.10–14 Therefore, it is obvious that HE4 may be used as a promising tumor marker for peritoneal carcinoma diagnosis and prognosis.
In this study, we collected the clinical data and investigated the diagnostic significance of serum HE4 levels in female patients with PPC, and we further analyzed the prognostic value of HE4 for treatment response and PPC recurrence.
Materials and methods
Patients
A total of 76 female PPC patients diagnosed and treated in Tianjin Central Hospital of Obstetrics and Gynecology from February 2011 to May 2016 participated in our study. The clinical data of each PPC patient were collected. We selected 228 patients with benign diseases as a control group, including 86 cases with benign fallopian tube masses and 142 cases with benign ovarian masses, which were matched for the same proportion of pre- and post-menopausal patients and were the same age as the PPC group. There was no significant difference for the levels of CA125 and HE4 between benign fallopian tube disease and benign ovarian disease cases. Another group included 130 high-grade ovarian serous cancer patients, with a mean age of 53.2 years (range 32–75). All patients in our study provided written informed consent, and the ethics of this research was approved by the faculty committee.
Specimen collection
The venous blood specimens of all patients for HE4 and CA125 detection were obtained through venipuncture before or after treatment. Two to four weeks after treatment, blood samples were collected for treatment response assessment, and samples were collected once every other month as usual for assessing the disease status of PPC patients. The supernatants of all blood specimens were separated and stored at −80°C until use.
HE4 measurement
After all sera were thawed at 4°C and gained room temperature, the quantitative assay of HE4 and CA125 concentrations were measured on the Cobas e601 analyzer. The cut-off values of HE4 and CA125 were 140 pmol/L and 35 U/mL, respectively.
Definitions for evaluation of serum HE4 in treatment response and recurrence
To date, the effective response between two continuous assays of tumor marker levels during surgery was assessed as at least a 50% drop according to the Gynecological Cancer Intergroup (GCIG) criteria, which is recommended as a monitor of CA125. 15 As a similar tumor marker to CA125, HE4 was also applicable for GCIG criteria. After surgery treatment, the detection of HE4 and CA125 behavior in 76 PPC patients was followed for several months. A total of 760 serum samples (mean 10 samples, range 6–24) were collected to measure HE4 and CA125 levels. An increase in postoperative HE4 level was used to evaluate PPC recurrence compared with CA125. The elevation of HE4 and CA125 was defined for recurrence assessment by the following method: (a) tumor marker increases 20% or two-fold more than the lowest value; and (b) tumor marker rises more than the cutoff value.15,16 Positron emission tomography–computed tomography (PET-CT), or specifically CT, during remission was used to evaluate disease status. Combining the results of PET-CT, or specifically CT, examinations with marker level examinations, all recurrences were preliminarily diagnosed. Then all suspected recurrent PPC patients were further proved through histopathology.
Statistical analysis
All statistical analysis in this study was performed by SPSS Software Version 19.0; P-values of less than 0.05 were considered to have statistical significance. The sensitivity and specificity of HE4+CA125 were calculated with the method offered by DeLong et al. 17 Receiver operating characteristic (ROC) curves were gained by SPSS software.
Results
Clinical characteristics of PPC patients
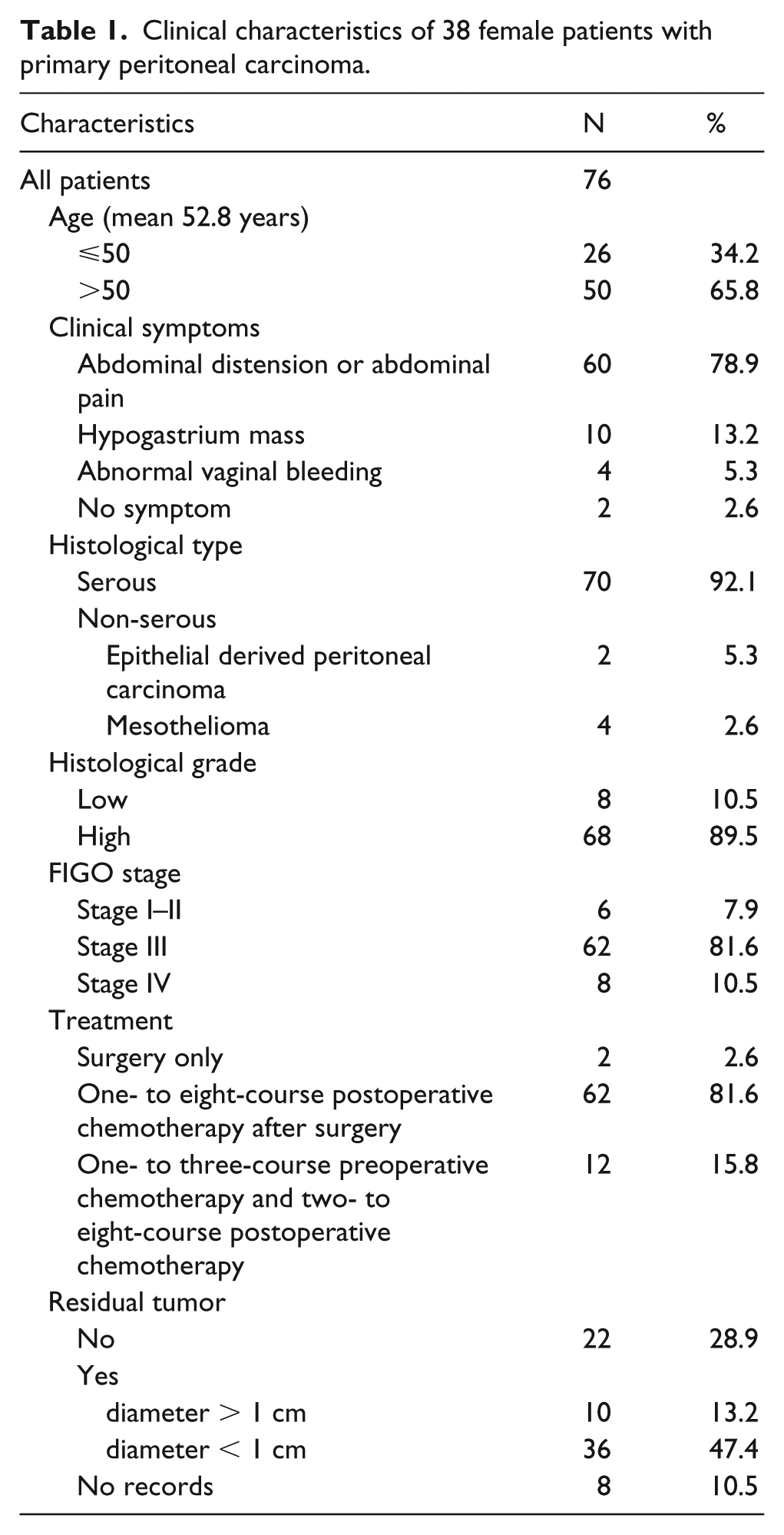
The clinical data of the studied PPC patients are listed in Table 1. The mean age of the patients was 52.8 years (range 33–74 years). Abdominal pain and abdominal distension were the most common complaints encountered in 78.9% of patients, followed by a hypogastrium mass and abnormal vaginal bleeding at 18.5%. Two cases had no clinical symptoms (2.6%), which were found when checking for endometrial disease. Of the 76 patients, 12 underwent one- to three-course preoperative chemotherapy and two- to eight-course postoperative chemotherapy after surgery; 2 patients only underwent surgery and did not receive any adjuvant chemotherapy; and 62 patients underwent an average of six (range 1–8) courses of postoperative chemotherapy. After surgery, 46 patients had a residual tumor, including 10 patients with a tumor diameter of more than 1 cm, and 36 patients less than 1 cm; 22 patients had no residual tumors; and the records were incomplete for 8 patients regarding residual tumors. So far 32 PPC cases have recurred in patients with residual tumors, while only 8 cases recurred in patients without residual tumors and those without records. Table 1 also shows that among the 76 PPC patients who received pathology examinations, 70 had serous adenocarcinoma, 2 had epithelial-derived peritoneal carcinoma, and 4 had malignant mesothelioma. In the PPC patients, 68 were at high grade; only 8 cases were at low grade. The proportion of stage III–IV and I–II was 92.1% and 7.9%, respectively.
Clinical characteristics of 38 female patients with primary peritoneal carcinoma.
HE4 is effective for the diagnosis of PPC
All PPC patient and control samples were measured for HE4 and CA125 levels. Table 2 shows that serum HE4 and CA125 levels were significantly higher in PPC patients than in those with benign diseases (P<0.001). It also indicates that HE4 had lower sensitivity in PPC, but higher specificity compared with CA125, and the combination of HE4 and CA125 led to higher sensitivity and specificity. ROC analysis demonstrated that the area under the curve (AUC) in PPC patients was 0.956 for HE4, 0.953 for CA125, and 0.979 for HE4+CA125 (Supplementary Fig. 1). Supplementary Figure 1 also indicates that both CA125 and HE4 are sensitive and specific markers for PPC patients despite the fact that a combination of the two is more effective.
Comparison of HE4 and CA125 levels between primary peritoneal carcinomas and benign diseases.
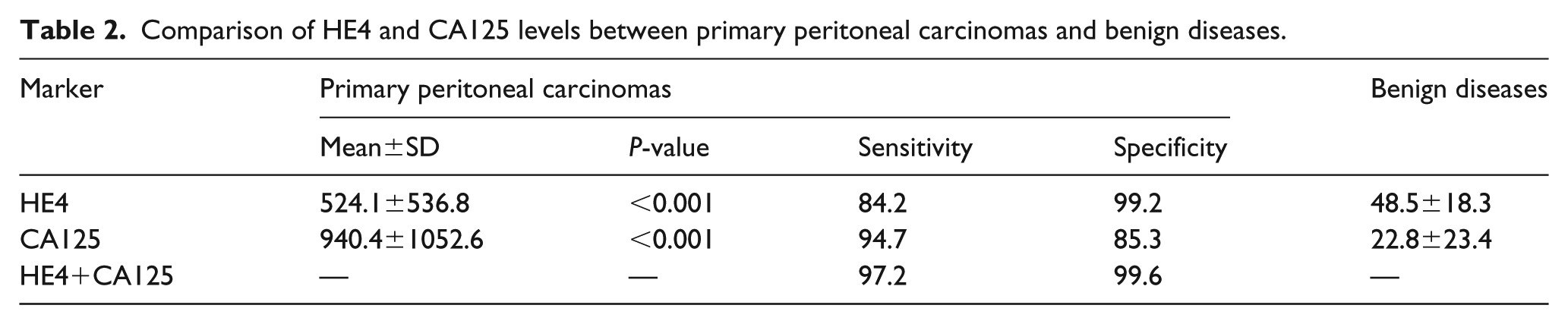
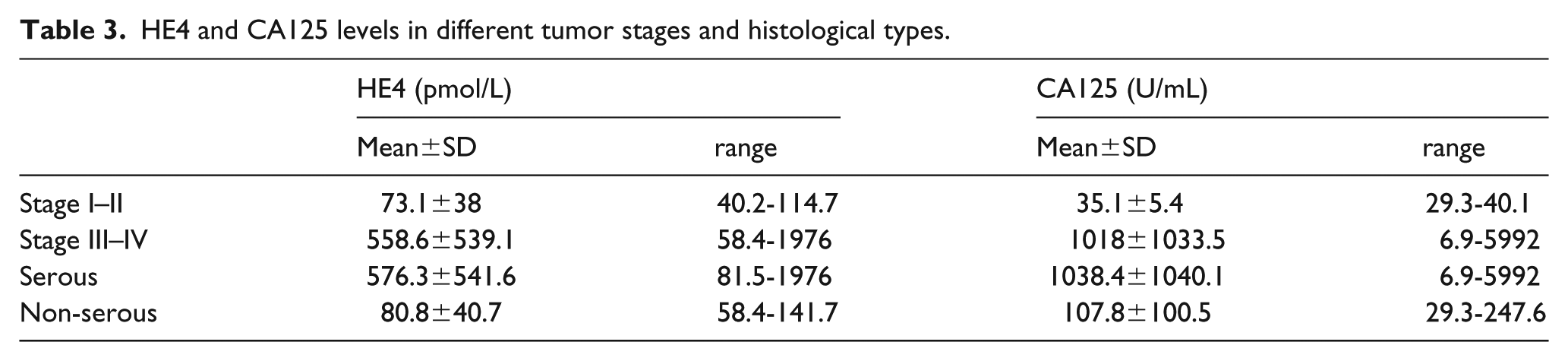
Table 3 indicates that HE4 and CA125 levels are correlated with tumor stage and histology type, and were higher in serous PPC than those in non-serous PPC (P<0.01). HE4 and CA125 levels were also elevated with the progression of the tumor. The levels of HE4 in stage I–II and III–IV were 73.1±38 and 558.6±539.1, respectively, while the levels of CA125 were 35.1±5.4 and 1018±1033.5, respectively.
HE4 and CA125 levels in different tumor stages and histological types.
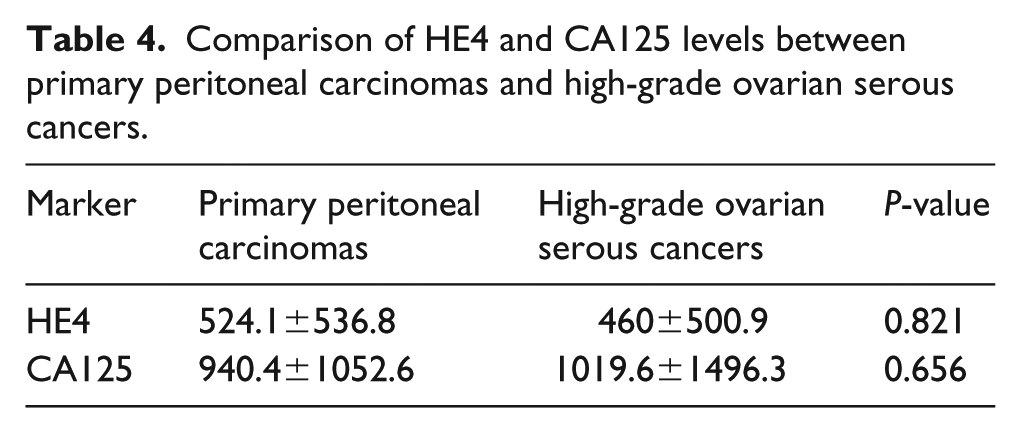
Moreover, HE4 levels were compared between PPCs and high-grade ovarian serous cancers. Table 4 shows that there were no significant differences in HE4 and CA125 levels between PPCs and high-grade ovarian serous cancers (P>0.05), although HE4 and CA125 levels were also significantly elevated in both PPC and high-grade ovarian serous cancers compared with benign diseases.
Comparison of HE4 and CA125 levels between primary peritoneal carcinomas and high-grade ovarian serous cancers.
Serum HE4 levels are closely correlated with PPC treatment response
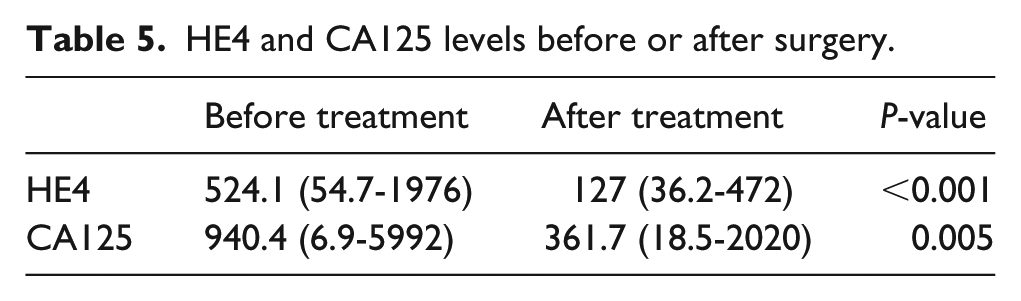
To evaluate surgical treatment response, we analyzed serum HE4 and CA125 levels in all PPC patients who underwent surgery, and compared these with the levels collected before surgery. Table 5 and Supplementary Figure 2(a) indicate that postoperative levels of both HE4 and CA125 decreased from an average of 524.1 to 127 pmol/L for HE4, and 940.4 to 361.7 U/mL for CA125 (P<0.001). Moreover, there was a larger decrease in HE4 level than CA125 (75.8% vs. 61.5%, P<0.01). Obviously, the PPC patients exhibited a larger decline in HE4 compared with CA125 (Supplementary Fig. 2(b)). Furthermore, 58 PPC patients demonstrated a greater than 50% reduction in HE4, while only 44 cases showed a greater than 50% reduction of CA125. Therefore, the effective response rate for therapy treatment shown by HE4 (76%) was higher than CA125 (58%). The reliability of surgery treatment response evaluation for PPC may be improved by HE4 assessment.
HE4 and CA125 levels before or after surgery.
HE4 is effective for the prognosis of PPC
After surgery, the detection of HE4 and CA125 behavior in 76 PPC patients was followed for several months (mean 10 months, range 6–24). PET-CT, or specifically CT, was used for the assessment of disease status. The majority of patients showed a decline in HE4 or CA125 levels after surgery, which was maintained below the threshold during the remission period, but rose again several months before recurrence. Supplementary Figure 3 shows that while 12 patients experienced no increase in the HE4 level before recurrence, the CA125 level was above threshold or rose more than 20% before recurrence. Interestingly, all patients experienced an increase in CA125 level before recurrence. Among the recurrent patients (n = 40), CA125 predicted all recurrences and HE4 predicted 28 recurrences, while in six patients, recurrences were detected by both biomarkers at the same time. There were 16 patients in which CA125 elevation occurred earlier than HE4, while there were only 6 cases in which HE4 elevation occurred earlier than CA125. Combined with CA125, HE4 can better predict recurrence.
Discussion
Currently, CA125 is considered as an effective tumor marker for the diagnosis and prognosis of PPC and is found elevated in PPC patients, which correlates with the clinical status of disease.18,19 For example, one PPC case was found because of an increase of CA125 concentration. 20 However, because of the limitation of low specificity, CA125 is not very effective in the diagnosis and prognosis of malignancy. Undoubtedly, HE4 is a most promising candidate for diagnosis and assessment of surgery response in women with suspected PPC. When combined with CA125, HE4 has been proved to enhance sensitivity and specificity for the diagnosis of ovarian cancer and primary fallopian tube carcinoma.14,21–23 Furthermore, HE4 combined with CA125 was effective for the prognosis of ovarian cancer and primary fallopian tube carcinoma in patients after surgical treatment. Owing to its similarity to ovarian cancer, PPC can be evaluated by HE4 in diagnosis and prognosis.
In this study, we analyzed the diagnostic and prognostic value of serum HE4 compared with CA125 in 76 PPC patients. Our results indicated serum HE4 and CA 125 levels were significantly increased in PPC, compared with benign disease (P<0.001). Compared with CA125, HE4 has a higher specificity in PPC, but a lower sensitivity, and the combination of HE4 + CA125 further elevated both the sensitivity and the specificity. Therefore, HE4 is effective in discriminating PPC from benign diseases.
We also compared the behavior of HE4 in PPC and high-grade ovarian serous cancer. It was evident that HE4 levels were significantly elevated in both PPC and high-grade ovarian serous cancer patients compared with benign disease cases; however, there was no significant difference in the levels of HE4 and CA125 between PPCs and high-grade ovarian serous cancers (P>0.05). These data suggest that the behavior of HE4 may be similar in PPC as well as in high-grade ovarian serous cancer.
In the 76 PPC patients in this study who underwent surgery followed by chemotherapy, postoperative HE4 levels significantly declined from 524.1 to 127 pmol/L (P<0.01). Furthermore, the reduction in HE4 level was larger than that of CA125 (P < 0.01). Our results indicate that HE4 is more effective than CA125 in assessing surgical response.
Our results also show that HE4 is an effective prognostic factor for PPC. During the remission period after surgical treatment followed by chemotherapy, HE4 predicted 28 recurrences in PPC patients, and CA125 predicted all 40 recurrences. In this study, all of the recurrences were detected by CA125, in these recurrences there were 10 cases with elevated HE4 levels below threshold before recurrence. There were 16 recurrences in which CA125 elevation occurred earlier than HE4. Another 6 recurrences were detected by both markers at the same time. In 6 recurrences, HE4 elevation occurred earlier than that of CA125. There were 12 recurrence cases in which HE4 elevation did not occur.
In brief, both HE4 and CA125 can be used as tumor markers for PPC treatment and recurrence. Our data suggest that the detection of serum HE4 changes could help to diagnose PPC and evaluate treatment response and early recurrence in PPC patients.
Supplemental Material
supplementary_material – Supplemental material for Diagnostic and prognostic value of HE4 in female patients with primary peritoneal carcinoma
Supplemental material, supplementary_material for Diagnostic and prognostic value of HE4 in female patients with primary peritoneal carcinoma by Dong Mi and Yuexiang Zhang in The International Journal of Biological Markers
Footnotes
Acknowledgements
Authors thank the women participated in our study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical standards
The study was approved by the IRB of Tianjin Central Hospital of Obstetrics and Gynecology.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.