
Abstract
Objectives
The objective is to evaluate the prognostic value of serum human epididymis protein 4 (HE4) as a tumor marker in patients with cervical cancer.
Methods
Sixty-seven patients with cervical cancer treated at Seoul National University Bundang Hospital from September 2014 to May 2018 were retrospectively reviewed. Serum HE4 levels were measured by immunoassay before starting primary treatment. A mean serum HE4 level of 72.6 pmol/L was used to divide the patients into low and high HE4 groups. Patient characteristics, clinicopathological variables, and survival outcomes were compared between the two groups.
Results
The low and high HE4 groups included 55 (82.1%) and 12 (17.9%) patients at diagnosis, respectively. Higher HE4 levels were significantly associated with older age at diagnosis (age <50: .0% vs age ≥50: 100.0%; P = .002), menopause (premenopause: 8.3% vs postmenopause: 91.7%; P = .009), higher FIGO stage (stage I–II: 33.3% vs III–IV: 66.7%; P = .017), large tumor size (<4.0 cm: 41.7% vs ≥4.0 cm: 58.3%; P = .029), positive lymph node metastasis (negative: 41.7% vs positive: 58.3%; P = .049), and involvement of the parametrium (negative: 25.0% vs positive: 75.0%; P = .002). Higher HE4 level was a predictive factor for worse overall survival but not for progression-free survival. Elevated HE4 levels were not independent factors for the prediction of either overall survival or progression-free survival. Subgroup analysis by histological type revealed similar results for patients with squamous cell carcinoma.
Conclusions
High levels of HE4 expression correlated with poor overall survival, indicating that elevated HE4 levels are associated with a poor prognosis for patients with cervical cancer.
Introduction
Over the past few decades, efforts have been made to reduce the incidence and mortality of cervical cancer through early detection and prevention. Nevertheless, cervical cancer remains the fourth most commonly diagnosed cancer and the fourth leading cause of cancer-related death in women worldwide. 1 Histologically, approximately 80% of cervical cancer cases are that of squamous cell carcinoma (SCC) and approximately 20% are that of adenocarcinoma (ADC).2,3 Currently, squamous cell carcinoma antigen (SCC-Ag) and cancer antigen 125 (CA 125) are the most used tumor markers for cervical cancer. However, increased levels of SCC-Ag are present in only 64% of patients with SCC and 25% of patients with ADC, while increased levels of CA 125 are present in only 42.6% of patients with SCC and in 18.9% of patients with ADC. 3 Therefore, the identification of novel markers that improve the detection rate of cervical cancer is required.
Cervical cancer is a preventable disease, and its morbidity and mortality has been dramatically reduced by the introduction of cervical cytology. 4 However, cervical cytology has low sensitivity and a high false positive rate, partially due to inadequate specimen collection.3,5 Adjunctive tests such as colposcopy and screening for human papillomavirus (HPV) have been suggested to overcome this low accuracy. 6 In addition, tumor markers for the diagnosis and follow up of cervical cancer are necessary. SCC-Ag is the most widely used tumor marker in the diagnosis of cervical cancer. Elevated levels of SCC-Ag are related to tumor size and stage of disease before treatment, as well as to the response to treatment. 7 However, the diagnostic sensitivity is only 30% for early cervical cancer. 8 Further, the utility of SCC-Ag in other histologic types remains unclear. These limitations demonstrate the importance of identifying other tumor markers for cervical cancer.
Human epididymis protein 4 (HE4) is a promising biomarker that has been shown to have great potential for clinical use.9-11 HE4 was first isolated from the epithelial cells of the human epididymis and can also be detected in serum. 12 HE4 expression has also been identified in normal human tissues outside of the male reproductive system, as well as in various types of malignancies.13,14 Previous studies have demonstrated that HE4 levels are higher in tumors of gynecologic origin,15-17 and HE4 is well established in ovarian and endometrial cancers.18,19 It has been reported that serum HE4, both alone and in combination with CA 125, has great potential to predict prognosis.20-22 Based on previous studies in ovarian cancer cells, the biological role of HE4 in malignant cells is controversial. One study reported that HE4 could inhibit cell proliferation by regulating the MAPK PI3K/AKT pathway. 23 Meanwhile, other studies reported that HE4 promotes proliferation, invasion, and metastasis of ovarian cancer cells.24,25 Additionally, in another study, knockdown of HE4 mediated the reduced cell proliferation, invasion, migration and tumor growth, and increased apoptosis through inhibiting of the JAK/STAT3 pathway. 26
Although it is known that serum levels of HE4 are significantly increased in ovarian and endometrial cancers, research on cervical cancer has been minimal. A tumor marker that enables better stratification of patients with cervical cancer may improve individualized primary treatment and help prevent over- or under-treatment of these patients. Therefore, we sought to evaluate the prognostic value of serum HE4 as a tumor marker for cervical cancer patients.
Methods
This retrospective study received approval from the Institutional Review Board of the Seoul National University Bundang Hospital (SNUBH; No. B-1602/336-103) and was performed in accordance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived due to the retrospective nature of the study.
We retrospectively reviewed the medical records of 67 patients with cervical cancer who were treated at Seoul National University Bundang Hospital, a tertiary hospital in Korea, from September 2014 to May 2018. All patients were restaged based on the revised 2018 International Federation of Gynecology and Obstetrics (FIGO) staging system for cervical cancer. 27 We included patients who met the following inclusion criteria: (1) patients who had histologically confirmed cervical cancer of any stage; (2) those who underwent initial treatment, such as radical hysterectomy with lymphadenectomy, concurrent chemoradiation therapy, radiation therapy or chemotherapy only; and (3) those who had HE4 levels assessed at diagnosis, before initiation of first treatment. Patients were excluded if they had: (1) incomplete treatment for any reason; (2) insufficient clinical and pathological data; (3) other malignancies that had the potential to influence survival outcomes; and (4) a history of renal failure or creatinine ≥1.5 mg/dL.
The medical records, surgical records, pathological findings, and clinical characteristics of included patients were reviewed. Histology was pathologically evaluated in all patients. Tumor size, lymphovascular space invasion (LVSI), lymph node (LN) metastasis, and involvement of the parametrium (PM) were evaluated pathologically only in patients who initially received surgery, while magnetic resonance imaging (MRI), computed tomography (CT), and positron emission tomography computed tomography were evaluated in patients who received initial treatment other than surgery.
The serum HE4 concentration was measured before initiation of patient treatment using the Architect Analyzer (Abbott Laboratories, USA). This is a two-step immunoassay that quantitatively measures HE4 levels in human serum using chemiluminescent microparticle technology. The inter-assay precision for measurement of HE4 was 3.5% (49.7 pmol/L), 3.6% (168.1 pmol/L), and 3.8% (648.2 pmol/L).
The mean serum HE4 level prior to the initiation of treatment of the 67 included patients were 72.6 pmol/L (standard deviation = 95.0). We evaluated the differences in clinicopathological characteristics between patients with lower (<72.6 pmol/L) and higher (≥72.6 pmol/L) HE4 levels at initial diagnosis.
Statistical Analysis
For comparison of continuous variables, the Student’s t-test and Mann–Whitney U test were used. Ordinal and categorical variables were analyzed using Pearson’s chi-squared test or Fisher’s exact test, as applicable. The association between HE4 levels and the survival outcomes of patients with cervical cancer was assessed by comparing patients with lower HE4 levels (<72.6 pmol/L) and those with higher HE4 levels (≥72.6 pmol/L) before the start of treatment. Progression-free survival (PFS) and overall survival (OS) rates were calculated by the Kaplan–Meier method and the differences between curves were assessed using the log-rank test. Univariate analysis was performed using the Cox proportional hazards model to evaluate the impact of patient characteristics and clinical factors on survival. For multivariate survival analysis, Cox proportional hazards analysis was used to estimate the prognostic effects of several variables. All analyses were performed using SPSS software for Windows (version 25.0; SPSS Inc., Chicago, IL, USA). P<.05 indicated statistical significance.
Results
Characteristics of the overall study population (N = 67).

Data are mean ± SD or N (%) unless otherwise specified.
Abbreviations: SD, standard deviation; FIGO, International Federation of Gynecology and Obstetrics; CCRT, concurrent chemoradiation therapy; RTx, radiation therapy; CTx, chemotherapy.
aP values were calculated by Student’s t-test.
bP values were calculated by Pearson’s chi-squared test.
cP values were calculated by Fisher’s exact test.
Comparison of study population according to low and high levels of mean HE4.

Data are N (%) unless otherwise specified.
Abbreviations: HE4, human epididymis protein 4; FIGO, International Federation of Gynecology and Obstetrics; LVSI, lymphovascular space invasion; LN, lymph node; PM, parametrium.
aP values were calculated by Pearson’s chi-squared test.
bP values were calculated by Fisher’s exact test.
Figure 1 shows the PFS and OS of patients in each group. There was no significant difference in PFS between the two groups (hazard ratio [HR]: .650; 95% confidence interval [CI]: .145–2.921; P = .572) (Figure 1(A)). However, patients with higher HE4 levels had significantly worse OS than those with lower HE4 levels (HR: 3.726; 95% CI: 1.182–11.747; P = .016) (Figure 1(B)). We also performed subgroup analysis of patients with the SCC histological type (N = 50), and the results were consistent with those of the overall study population. There was no significant difference observed in PFS (HR: .974; 95% CI: .198–4.805; P = .975) (Figure 1(C)), but patients with higher HE4 levels were associated with worse OS than those with lower HE4 levels (HR: 5.449; 95% CI: 1.460–20.332; P = .005) (Figure 1(D)). Comparisons of survival outcomes between patients with low (<72.6 pmol/L) and high (≥72.6 pmol/L) HE4. (A) Progression-free survival in the entire cohort; (B) overall survival in the entire cohort; (C) progression-free survival in patients with squamous cell carcinoma; and (D) overall survival in patients with squamous cell carcinoma.
Factors associated with survival in the overall population.
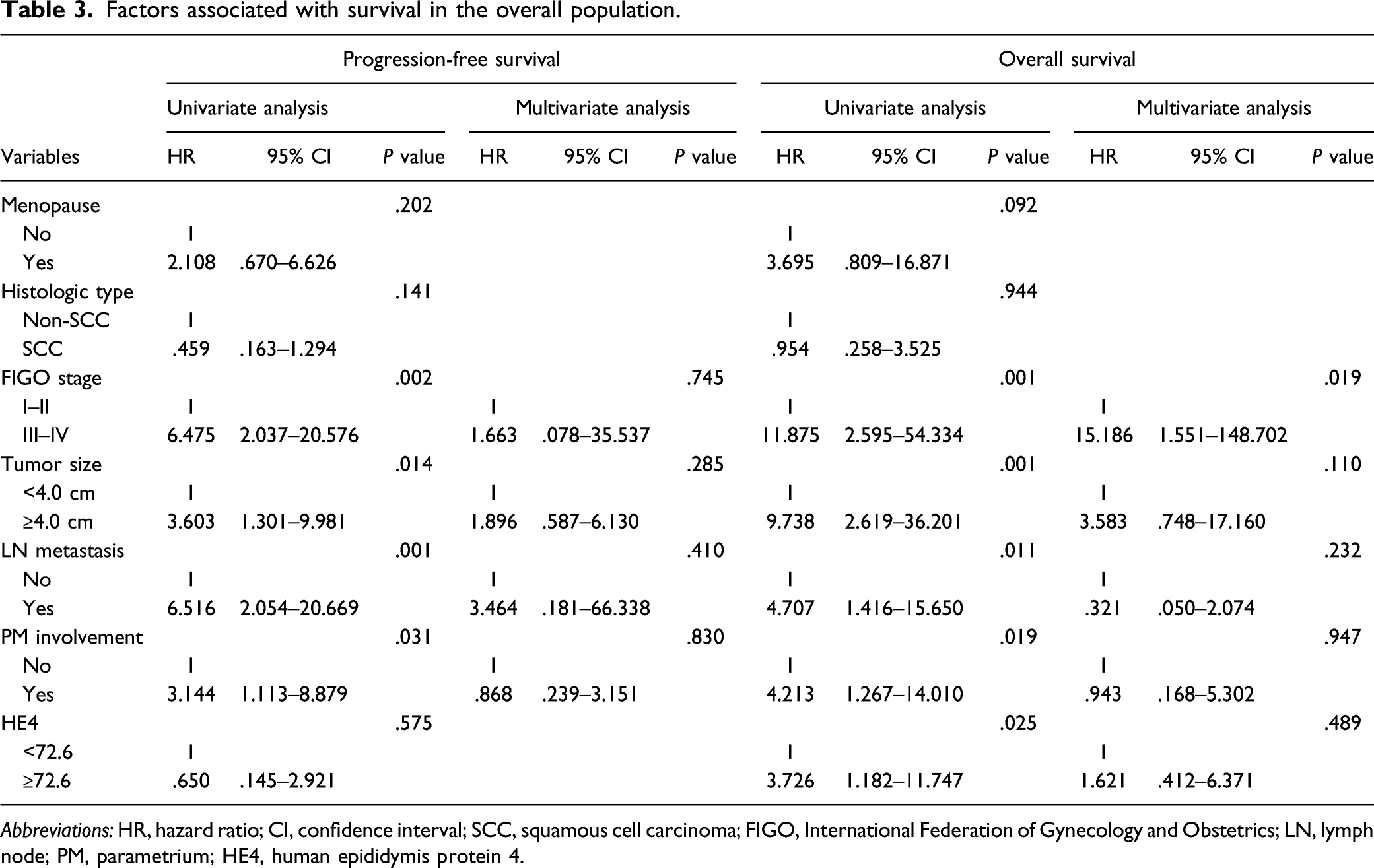
Abbreviations: HR, hazard ratio; CI, confidence interval; SCC, squamous cell carcinoma; FIGO, International Federation of Gynecology and Obstetrics; LN, lymph node; PM, parametrium; HE4, human epididymis protein 4.
Factors associated with survival in patients with squamous cell carcinoma.

Abbreviations: HR, hazard ratio; CI, confidence interval; FIGO, International Federation of Gynecology and Obstetrics; LN, lymph node; PM, parametrium; HE4, human epididymis protein 4.
Discussion
In this study, we found that high expression of HE4 is correlated with poor OS, indicating that HE4 is a potential candidate biomarker for predicting the prognosis of cervical cancer. Our findings revealed that, in cervical cancer patients, elevated serum HE4 levels were significantly correlated with FIGO stage as well as tumor size, LVSI, LN metastasis, and PM involvement but not with histological type. Moreover, we found that in univariate analysis, serum HE4 levels were associated with worse OS. However, HE4 levels were not found to be an independent prognostic factor for PFS. Similar results were observed in the subgroup analysis of patients with histologically confirmed SCC.
Previous studies regarding serum HE4 as a biomarker in cervical cancer are limited. Some studies have shown that patients with cervical cancer may also have higher levels of HE4.17,28 However, as these studies were limited by their small sample size, it remains unclear whether HE4 is a valuable marker for cervical cancer. A more recent study evaluating the role of pre-treatment serum HE4 levels in cervical cancer reported that serum HE4 could be a preoperative tumor biomarker of poor prognosis in cervical cancer. 29 Consistent with our own results, this study also demonstrated that higher levels of serum HE4 correlate with advanced stage, larger tumor size, and high tumor grade, while no significant association was found with LVSI, PM involvement, and LN involvement, which is not consistent with our study.
Careful attention is required in interpreting serum HE4 levels as they can be affected by numerous factors. 30 Previous studies have shown that age, menopausal status, smoking, renal function, chronic liver disease, ethnicity, and detection method may influence serum HE4 levels.17,31-33 Thus, our results should be interpreted with caution. Currently, there is no consensus established for optimal baseline serum HE4 cutoff values. 34 According to previous published investigations, a serum HE4 cut-off value of 70 pmol/L yields the best sensitivity and specificity. 30 The positive serum HE4 cut-off values previously identified in ovarian and endometrial cancer patients were similar to the mean value of HE4 in our study.28,35 In other previous studies, serum HE4 levels were higher in cervical cancer patients compared to healthy controls, but lower than ovarian cancer patients, showing similar results to our study.28,29
This study has several limitations. First, the existence of underlying selection bias is possible due to the retrospective design. Second, the sample size of the study population and the number of recurrence and death events might be insufficient for a comparison of survival outcomes between lower and higher serum HE4 levels. Third, no subgroup analysis was performed for the ADC histology type because of the small sample size of this population. Last, we did not perform power calculations for the estimation of sample size.
Conclusions
In conclusion, our study showed that elevated serum HE4 was associated with poor prognostic factors for cervical cancer and was correlated with poor OS, suggesting the potential of HE4 as a novel biomarker for predicting the survival of patients with cervical cancer.
Supplemental Material
Supplemental Material - Serum Human Epididymis Protein 4 as a Prognostic Marker in Cervical Cancer
Supplemental Material for Serum Human Epididymis Protein 4 as a Prognostic Marker in Cervical Cancer by Woo Yeon Hwang, Dong Hoon Suh, Kidong Kim, Yong Beom Kim, and Jae Hong No in Cancer Control.
Footnotes
Acknowledgments
Thanks to all the authors who contributed to this article, and to the publisher for supporting this article.
Authors’ contributions
W Y Hwang, D H Suh, and J H No designed the research of study. W Y Hwang and J H No performed the research. W Y Hwang and J H No analyzed data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Seoul National University Bundang Hospital Research Fund [grant number 02-2014-0048]. The funding source played no role in the study design; the collection, analysis, or interpretation of the data; the writing of the report; or the decision to submit the article.
Ethics approval and consent to participate
This retrospective study received approval from the Institutional Review Board of the Seoul National University Bundang Hospital (SNUBH; No. B-1602/336-103) and was performed in accordance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived due to the retrospective nature of the study.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.