
Abstract
Background:
Long non-coding RNAs (lncRNAs) Hox transcript antisense intergenic RNA (HOTAIR) has been suggested to be implicated in gastric cancer tumorigenesis and progression; however, little is known about the role of the plasma HOTAIR in gastric cancer diagnosis and prognosis.
Objective:
The current study was aimed at investigating the clinical relevance of plasma long non-coding HOTAIR as a non-invasive diagnostic biomarker in gastric cancer.
Methods:
Plasma HOTAIR expression was measured in 50 patients with newly diagnosed gastric cancer and 50 age- and sex-matched healthy controls using quantitative reverse transcription polymerase chain reaction.
Results:
Plasma level of HOTAIR was significantly higher in gastric cancer patients compared with healthy controls (P < 0.001). By using receiver operating characteristic curve analysis, it was found that plasma HOTAIR could diagnose gastric cancer with 88% sensitivity and 84% specificity. Furthermore, increased HOTAIR expression was associated with advanced tumor stages, higher grades, and metastasis.
Conclusion:
Plasma HOTAIR might serve as a potential non-invasive biomarker for diagnosis of gastric cancer.
Introduction
The incidence and mortality of gastric cancer (GC) has declined over the last 50 years in many countries. However, it still remains the second most common cause of cancer-related deaths worldwide.1,2 The diagnostic approaches and the treatment strategies for GC, including surgical resection techniques and adjuvant chemotherapy, have advanced greatly in recent years. Nevertheless, GC is still a highly fatal disease, mainly due to late discovery after malignant invasion and metastasis. 3 Therefore, early detection of GC is mandatory to allow radical treatment.
In countries with a high prevalence of GC, such as South Korea and Japan, upper endoscopy is used with photofluorography for GC screening. However, countries outside Asia do not routinely use endoscopy for screening, either because of the low prevalence of GC or the cost implications. 4 Thus, blood-based cancer biomarkers are ideal candidates for screening and early detection.
The already available blood-based tumor markers for GC, such as carcinoembryonic antigen (CEA), carbohydrate antigen 19–9 (CA 19–9), CA72-4, and CA125 are used mainly for disease monitoring. However, low sensitivity and specificity of these markers restrict their use in screening and early diagnosis.5,6 Recently, circulating non-coding RNAs have emerged as a new source of non-invasive cancer biomarkers.7,8
Long non-coding RNAs (lncRNAs) account for a large portion of the non-coding transcripts. They consist of more than 200 nucleotides and have no or limited protein-coding potential. Previously, they were believed to be transcriptional noise, but now they have attracted attention as a new participant in carcinogenesis.9,10 Expression analyses of lncRNAs in a wide range of tissues has revealed their importance for different homeostatic and physiological functions, such as gene imprinting, cell differentiation, and organogenesis.11,12
A strong association has been found between deregulated lncRNA expression and the development of diseases. Through the modulation of oncogenic and tumor-suppressing pathways, it was noted that aberrant expression of lncRNAs contributed to the development and progression of cancer.13–16
Hox transcript antisense intergenic RNA (HOTAIR) lncRNA is one of the most important regulatory RNAs in human cells. It was first described by Rinn et al. 17 as a spliced and polyadenylated RNA with six exons and 2.2 kb nucleotides. This RNA is transcribed from the antisense strand of the HoxC gene, which is located on chromosome 12q13.13 between the HoxC11 and HoxC12 genes.
Accumulating evidence has uncovered the implication of overexpressed HOTAIR in GC tumorigenesis and progression, confirming its oncogenic role.18,19 Nevertheless, only one study has evaluated the role of plasma HOTAIR in the diagnosis of GC, although only an insignificant association was obtained. 21
Therefore, the current study aimed to investigate the clinical relevance of plasma long non-coding HOTAIR as a non-invasive biomarker in GC.
Materials and methods
After approval of the ethics committee of the Faculty of Medicine, Alexandria University, 100 participants were enrolled in the current study, and divided into two groups. The first group included 50 newly diagnosed GC patients recruited from the Gastrointestinal and Clinical Oncology Units, Alexandria Main University Hospital. The second group included 50 age- and sex-matched healthy individuals as a control group.
The diagnosis of GC was confirmed by histopathological examination of excised tumors. The staging was done based on The American Joint Committee on Cancer’s TNM (Tumor size, lymph Node involvement, and distant Metastasis) staging system. 22 Patients received neo-adjuvant therapy, and patients with recurrent GC were excluded from the study.
Plasma HOTAIR expression, as well as the serum CEA level, were assessed for all study participants.
Assessment plasma HOTAIR expression using quantitative real-time polymerase chain reaction
Blood sample
From each participant in the study, 2 mL of venous blood were collected in ethylenediaminetetraacetic acid (EDTA)-containing tubes before receiving any treatment either gastrectomy or chemotherapy. Blood samples were centrifuged within two hours after collection at 1200 g for 10 min at 4°C. The supernatants were transferred to new micro-centrifuge tubes and then centrifuged at 12,000 g for 10 min at 4°C to ensure removal of all cellular components. Supernatant was collected and stored at −80°C until RNA extraction.
RNA extraction
Total RNA was extracted from 200 µL of supernatant plasma using miRNeasy Mini Kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions. Purity and concentration of RNA were assessed using Nanodrop 2000/2000c (Thermo Fisher Scientific, Waltham, MA, USA). Purified RNA was stored at −80°C until further use.
Quantitative reverse transcription polymerase chain reaction
cDNA was synthesized using High Capacity cDNA Reverse Transcription Kit (Applied Biosystems, Waltham, MA, USA). RNA was added to reverse transcription master mix (10 µL) to a final volume of 20 µL. Then, incubation was done at 25°C for 10 min, at 37°C for 120 min, and then at 85°C for five min.
Quantitative real-time polymerase chain reaction (PCR) was performed using Applied Biosystems 7500 Real-Time PCR Systems (Applied Biosystems). PCR amplification mix contained 12.5 µL 1× QuantiFast Multiplex PCR Master Mix (Qiagen), 1.25 µL 20× HOTAIR QuantiFast Probe Assay labeled with FAM (cat No. QF00115059), 1.25 µL of 20× G6PDH primer–probe mix (labeled with MAX), cDNA (100 ng/reaction), and RNase-free H2O to a final volume of 25 µL. G6PDH was used as a reference gene.
The real-time PCR amplification mix was incubated at 95°C for five min for Taq activation followed by 45 cycles of 95°C for 30 s for denaturation and 60°C for 30 s annealing and extension.
Comparative CT method (2-∆∆Ct) was used to calculate HOTAIR expression in plasma of GC patients’ samples normalized to GAPDH expression and relative to healthy controls.
Statistical analysis of the data
Data were analyzed using IBM SPSS software package version 20.0. Comparisons between groups for categorical variables were assessed using the Chi-square test. Abnormally distributed quantitative variables were expressed with median, minimum and maximum, and were compared using the Mann–Whitney test. The area under the receiver operating characteristic (ROC) curve denotes the diagnostic performance of the test. Area more than 50% gives an acceptable performance and area approximately 100% is the best performance for the test. The Spearman coefficient was used to correlate between HOTAIR expression and serum CEA. Significance of the obtained results was judged at the 5% level.
Results
Study participants
The GC group consisted of 29 males (58%) and 21 females (42%), whereas the control group consisted of 26 males (52%) and 24 females (48%). The ages of the GC patients ranged from 31 to 62 years, while that of the controls ranged from 30 to 62 years. No statistically significant difference was found between both groups regarding age and gender (P = 0.792 and 0.792, respectively).
Based on TNM staging, the most prevalent stage among our patients was stage III (40%), followed by stage IV (30%), then stage II (20%), and finally stage I (10%). Distant metastasis was present in 15 patients (30%). Histopathological examination of the tumors revealed adenocarcinoma in all cases. Eleven patients (22%) had well-differentiated tumors, while 26 patients (52%) had moderately differentiated tumors, and 13 patients (26%) had poorly differentiated tumors. According to the World Health Organization classification, 27 patients (54%) had tubular adenocarcinoma, 19 patients (38%) had papillary adenocarcinoma, while only four patients (8%) had mucinous adenocarcinoma.
Plasma HOTAIR expression in the studied groups
Plasma HOTAIR was significantly up-regulated in GC patients compared with controls (P < 0.001) as illustrated in Table 1
Plasma HOTAIR expression and CEA level in both studied groups.
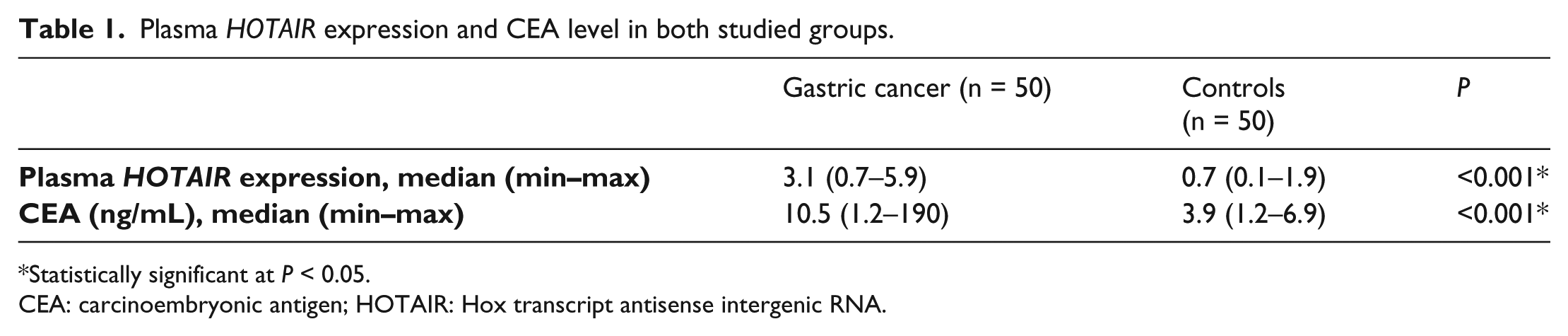
Statistically significant at P < 0.05.
CEA: carcinoembryonic antigen; HOTAIR: Hox transcript antisense intergenic RNA.
Moreover, a statistically significant difference was found in HOTAIR expression level between different TNM stages (P < 0.001), being higher in advanced stages, where patients with distant metastasis showed significantly higher HOTAIR expression. In addition, HOTAIR expression was overexpressed in patients with poorly differentiated tumor compared with other grades (P < 0.001) (Table 2).
Association between plasma HOTAIR expression level and clinicopathological parameters in gastric cancer patients.
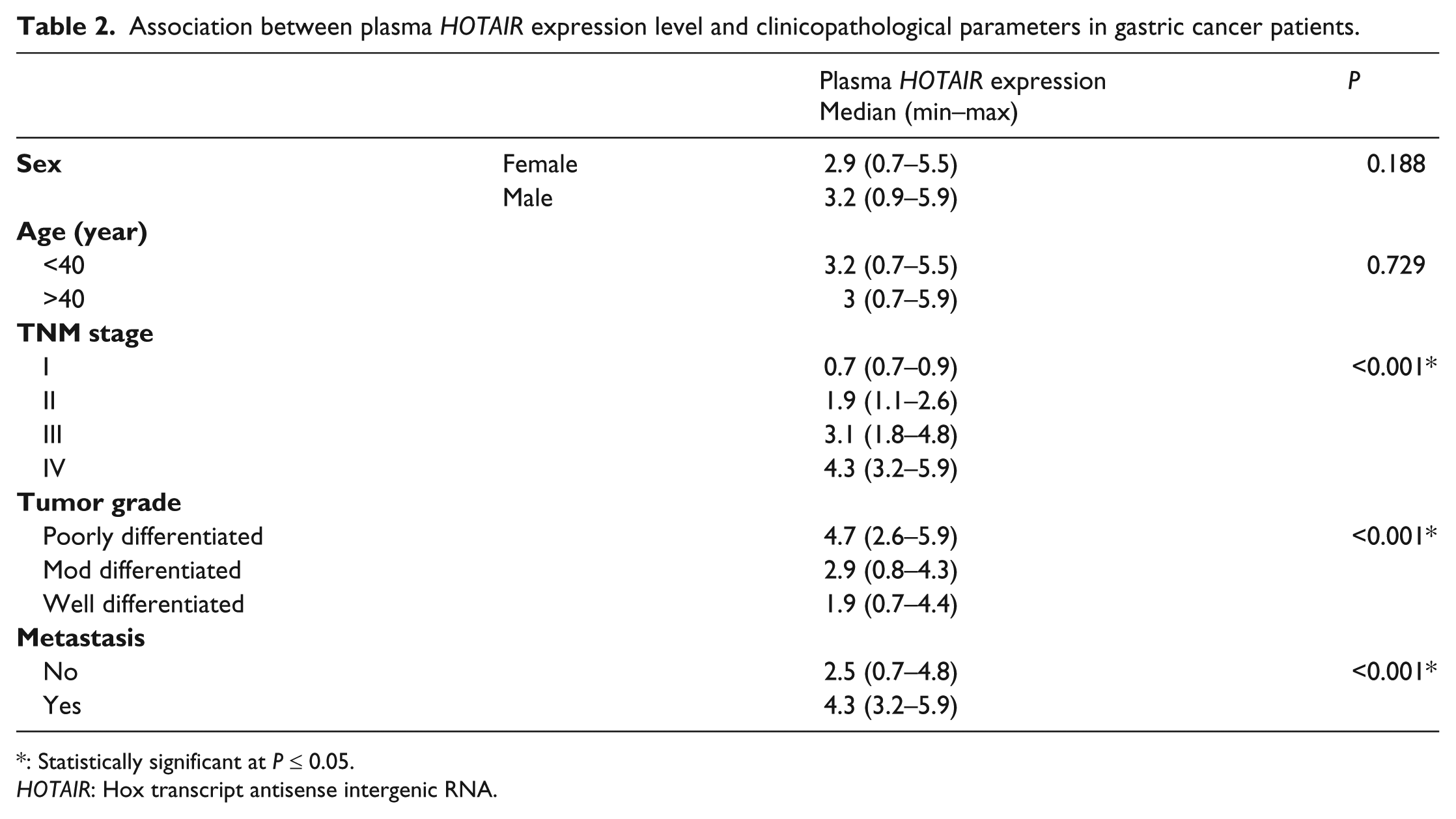
: Statistically significant at P ≤ 0.05.
HOTAIR: Hox transcript antisense intergenic RNA.
Furthermore, plasma HOTAIR was positively correlated with the CEA level (r 0.426; P = 0.002), while no significant association was observed between plasma HOTAIR and age or gender.
By using the ROC curve analysis, the plasma HOTAIR expression could be used for the diagnosis of GC with 88% sensitivity, 84% specificity, 84.6% positive predictive value (PPV), 87.5% negative predictive value (NPP) at a cutoff value of 1.2, and the area under the curve (AUC) was 0.944.
When the diagnostic performance for both plasma HOTAIR expression and CEA was evaluated, it was found that by using both markers together, GC could be detected with 86% sensitivity, 94% specificity, 93.5% PPV, and 87% NPP, with an AUC of 0.954.
Discussion
Unfortunately, GC is almost always diagnosed at an advanced stage with limited effective therapeutic modalities. 3 Therefore, there is an imminent demand for discovery of new biomarkers for its screening and early diagnosis, which could greatly help in early treatment resulting in an increased survival rate of these patients. The use of biological fluids, such as blood, as a provenance for non-invasive cancer biomarkers has aroused a considerable amount of attention.
Previous research has shown that circulating microRNAs could be used as a non-invasive biomarker for the early detection of cancers.23–25 Similarly, other types of non-coding RNA, such as lncRNAs, also can be detected in body fluids, and may have diagnostic and prognostic roles in cancer. Recent studies have investigated the clinical implication of cell-free lncRNAs in cancer patients.26,27 Dong et al. 28 studied 39 cancer-associated lncRNAs in serum and identified a three-lncRNA panel, including CUDR, LSINCT-5, and PTENP1, which could detect GC with high diagnostic accuracy. 28
Recent studies done at the tissue level have shed light on the role of lncRNA HOTAIR in the pathogenesis and progression of GC.29,30 Despite proving that HOTAIR was significantly up-regulated in GC tissues compared with paired healthy tissues, the only study evaluating its expression in plasma of GC patients did not find any association between HOTAIR and GC. In that study, Arita et al. 21 confirmed the presence and stability of lncRNAs in the plasma of GC patients, and reported that H19 levels were significantly higher in the patients than in the controls. However, there was no significant difference in the levels of HOTAIR between patients and controls.
Therefore, we decided to replicate this study with a larger number of patients and controls to investigate whether the plasma HOTAIR expression was associated with GC or not, hoping to discover a non-invasive biomarker for screening and early detection of GC.
Interestingly, in contrast to the Arita et al. 21 study, our results showed a significant up-regulation of plasma HOTAIR in GC patients compared with healthy controls, and its capability of discriminating between GC patients and healthy controls with 88% sensitivity and 84% specificity. Furthermore, plasma HOTAIR was more up-regulated in advanced grades and stages of the disease and in the presence of metastasis.
Our results are emphasized by previous reports that demonstrated significantly up-regulated HOTAIR expression levels in human gastric adenocarcinoma tissues compared with normal gastric epithelium. These studies also showed an association between increased HOTAIR expression and perineural invasion, advanced TNM staging, and lymph node and distant metastasis of gastric tumors.18,19
When the expression levels of some epithelial-to-mesenchymal transition (EMT) and metastasis-related genes (e.g. ICAM-1, MMP1, MMP3 and MMP9) were compared between GC tissues with high and low HOTAIR expression in a study by Xu et al. 31 it was found that in the (high) HOTAIR group, most of the epithelial markers were down-regulated, while most of the mesenchymal markers were up-regulated. Additionally, the four metastasis-related genes were significantly over-expressed in the HOTAIR (high) group. When HOTAIR expression was down-regulated in GC cells by RNA interference, in vitro migration and invasiveness were reduced, as well as the expression of MMP1 and MMP3. These findings corroborate our results by explaining the association between increased HOTAIR expression and advanced tumor stages.
A considerable amount of research has been done exploring the oncogenic role of HOTAIR in GC pathogenesis. Hajjari et al. 19 found a strong positive correlation between the expression levels of HOTAIR and SUZ12 in GC tissues. SUZ12, is a part of Polycomb Repressive Complex 2 (PRC2). PRC2 represses transcription through the methylation of lysine (K) 27 of histone H3 (H3). Gupta et al. 20 confirmed this association between the increased level of HOTAIR and SUZ12 expression, but in breast cancer tissues. They suggested that changed HOTAIR expression could promote genomic re-localization of the PRC2 and H3K27 tri-methylation.
Another interesting study proposed that HOTAIR is implicated in GC pathogenesis through the down-regulation of poly r(C)-binding protein-1 (PCBP1) expression using proteomic analysis of GC cell lines. When they examined PCBP1 in GC tissues, they found that it was almost absent with increased expression of HOTAIR. It was suggested that PCBP1 acted as a strong tumorigenic and metastatic inhibitor. They extended their work to investigate the effect of HOTAIR on tumor invasiveness through the induction of HOTAIR overexpression in GC cell lines. They found that ectopic expression of HOTAIR in the GC cells induced more in vitro migration. 32
Recently, it has been hypothesized that HOTAIR may also serve as a competitive endogenous RNA (ceRNA). 33 In GC, it prevents transcriptional suppression of HER2 mRNA through competition for miR-331-3p. HER2 is a direct target of miR-331-3. It acts as an oncogene implicated in various malignant cell functions, such as proliferation, motility, angiogenesis, and apoptosis.34-36 Thus, overexpression of HOTAIR results in a simultaneous increase in HER2 expression, which promotes GC tumorgenesis and invasiveness.
A recent meta-analysis investigated the role of HOTAIR polymorphisms on cancer susceptibility. They identified a significant association between the rs920778 polymorphism and the increased susceptibility to cancer, including GC. 37
In addition, different studies provided evidence for the important roles of HOTAIR in the initiation and progression of various types of cancers, such as breast cancer, 38 esophageal squamous cell carcinoma, 39 hepatocellular carcinoma, 40 colon cancer, 41 renal cancer, 42 pancreatic cancer, 43 as well as pediatric brain tumors. 44
Moreover, in a recent important study, Ma et al. 45 proposed that HOTAIR could be used as a target for therapeutic intervention in GC. They found that dioscin, an anti-tumor drug, could inhibit the proliferation of GC cell lines through the down-regulation of overexpressed HOTAIR.
Inspired by the present data and previous findings, we could conclude that plasma HOTAIR overexpression might be used as a non-invasive diagnostic marker for GC. However, further large-scale studies are required to confirm the diagnostic accuracy of HOTAIR as well as its prognostic potential using larger homogenous groups of patients and controls with adequate follow-up.
Footnotes
Declaration of conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.