
Abstract
Introduction
Liver cancer is the sixth most prevalent malignancy worldwide and the third leading cause of cancer-related deaths. 1 HCC is the most common histological type of primary liver cancer, accounting for 80%–90% of cases. 2 The complex etiology and high heterogeneity of HCC make its diagnosis and prognosis challenging. 3 Early-stage HCC can be treated with radical interventions, such as surgical resection, local percutaneous ablation, and liver transplantation. 4 However, due to the asymptomatic onset of the disease, most HCC patients are diagnosed at advanced stages, resulting in missed opportunities for radical surgery and a high risk of recurrence. 5 Therefore, there is an urgent need to identify new diagnostic and prognostic markers for HCC.
Cyclophilins (Cyps) are a family of chaperone proteins with peptidyl proline isomerase (PPIase) activity, playing key roles in regulating cellular physiology and disease under various inflammatory conditions.6,7 As a member of the cyclophilin family, Ppih plays an essential role not only in protein folding but also in pre-mRNA splicing and the assembly of the U4/U5/U6 tri-snRNP complex. 8 Similar to the role of RNA-binding proteins, including Ppih, in the development of HBV-related HCC as reported by Li et al., 9 our previous studies also revealed that Ppih is highly overexpressed in HCC and is associated with advanced disease, poor differentiation, and TP53 mutation. 10 Additionally, Li et al. 11 and Gao et al. 12 reported that Ppih expression is closely related to the development of gastric adenocarcinoma (STAD) and lung adenocarcinoma (LUAD). In our study, we also found that Ppih is overexpressed in breast and colorectal cancer tissues and is strongly associated with poor prognosis. Collectively, the role of Ppih in cancer is gaining increasing attention, and its mechanisms of action and potential as a biomarker warrant further investigation.
The tumor microenvironment (TME) is a critical mediator of cancer progression and treatment outcomes, with tumor-infiltrating immune cells (TIICs) being an important component of the TME and playing a crucial role in tumor progression. 13 In recent years, immunotherapy has gained increasing recognition for its effectiveness against many types of tumors, 14 with cytokine and immune checkpoint inhibitor (ICI) therapies emerging as significant treatment strategies for various cancers. 15 Therefore, the identification of biomarkers as potential therapeutic targets is of great importance for predicting the efficacy of immunotherapy, determining outcomes, and guiding individualized treatment plans. However, the molecular mechanisms and clinical significance of Ppih in HCC, particularly its relationship with immune cell infiltration and immune responses, remain underexplored. To date, no studies have confirmed whether Ppih can serve as a biomarker to guide immunotherapy in HCC.
In this study, we employed various bioinformatics approaches to assess the differential expression of Ppih in HCC tissues compared to adjacent normal tissues. We developed a risk score based on Ppih expression to classify patients into high- and low-risk groups, then evaluated the prognostic differences between these groups. Additionally, we performed a comprehensive analysis of the immunological characteristics of the risk groups, focusing on the association between macrophage subpopulation infiltration density and poor prognosis in HCC. We also analyzed the correlations of Ppih with clinical subtypes, immune cell infiltration scores, immunotherapy response, and immune cytokine expression. Our findings offer a new perspective on the role of Ppih, providing novel targets for the diagnosis, treatment, and prognosis of HCC.
Methods
Clinical specimen
Serum samples from 40 HCC patients were collected at the Second Affiliated Hospital of Guizhou Medical University between January and March 2024. Inclusion criteria included no history of other malignancies, histologically confirmed solid tumors, and comprehensive clinical and follow-up data (Table S1). Exclusion criteria included recent systemic infection, autoimmune or active immune disease, severe hypertension, heart disease, or pregnancy. Control serum samples were collected from 40 healthy participants undergoing routine health examinations. All patients provided informed consent, and the hospital’s ethics committee approved the study protocol. In addition, Perl extracted survival data, eliminated incomplete entries, and aligned the complete survival information with PPIH data, yielding a dataset comprising 370 eligible patients. The follow-up period extended over 10.5 years, with a retention rate of 91.13% (370 out of 406 patients).
DriverDBV3 database
DriverDBV3 utilizes various -omics techniques to identify cancer driver genes and presents them with different molecular features, including somatic mutations, RNA expression, miRNA expression, DNA methylation, copy number variations, and clinical data, in addition to base annotations. 16 The gene summary of Ppih in various cancer tissues and its mRNA expression in HCC were analyzed using the DriverDBV3 database. A survival analysis with a log-rank p < 0.05 was considered statistically significant.
Survival analysis based on risk score
Patients were classified into high-risk and low-risk cohorts according to the median risk score. A time-dependent receiver operating characteristic (ROC) curve was generated to evaluate the predictive value of the prognostic gene signature for overall survival using the R package “survivalROC.” The Kaplan-Meier survival curve, combined with a log-rank test, was used to compare survival differences between the high- and low-risk groups using the R package “survival”. 17
Immunologic features and immunotherapeutic effect in the two risk groups
To evaluate the immune features of HCC samples in different risk subgroups, we used CIBERSORT (perm = 1000) to calculate the relative proportions of 22 types of immune cells. These relative proportions were then compared between the two risk subgroups, and the results were presented in a landscape map. Additionally, the IMvigor210 dataset 18 was used to validate the links between the risk signature and immunotherapy response.
Infiltrating immune cells prognostic analysis in HCC
We integrated data from 406 HCC samples and calculated the relative proportions of 22 key immune cell types for survival analysis. Kaplan-Meier analysis was performed to assess survival outcomes in the high-risk and low-risk groups.
Elisa analysis
An ELISA kit (Jingmei Biotechnology Co., LTD, Jiangsu, China) was used to measure protein concentrations. The instructions for using the kit are as follows: (1) Dilute the standard; (2) Add the test sample to the specified well plate; (3) Incubate at 37°C for 30 min; (4) Wash the plate four times; (5) Add enzyme reagents; (6) Incubate again and wash; (7) Perform color development; (8) Terminate the reaction; (9) Set the blank well reading to zero and record the absorbance (OD value) at 450 nm using an enzyme-linked immunosorbent assay. The concentrations of IFN-γ, Granzyme B, IgG, and PPIH were calculated from the standard curve. Two-group comparisons were made using Student’s t-test, with p-values less than 0.05 considered statistically significant.
Statistical analysis
Statistical analysis was performed using GraphPad Prism (v.9.0), SPSS 27.0 and R software 4.2.3. Kruskal-Wallis test was used for multiple consecutive independent samples, and Wilcoxon signed rank test was used for two consecutive independent samples. Kaplan-Meier survival analysis was performed using log-rank test, and student t test was used to compare serum immune cytokines and PPIH secretion levels in HCC patients and healthy controls. p-value less than 0.05 was considered statistically significant.
Results
Ppih expression and its correlation with prognosis of HCC
We analyzed Ppih expression using the TCGA and GTEx datasets. As shown in Figure 1(a) and (b), 31 tumors were analyzed and differential expression was found in 14,the mRNA levels of Ppih were upregulated in HCC compared to adjacent normal liver tissues. In the risk model, risk scores for all samples were calculated using the formula: Risk score = [Expression value × gene coefficient]. The performance of the risk score in predicting prognosis was evaluated using Kaplan-Meier survival curves and log-rank tests on TCGA cohorts. With the median risk score as the cutoff, samples were divided into low-risk and high-risk groups. It was found that patients in the low-risk group had better overall survival (OS) compared to those in the high-risk group (Figure 1(c)–(d)). Visual summary of the prognostic value of Ppih in HCC. (a and b) Comparison of mRNA expression of Ppih between tumor (Red) and normal samples (Gray) (TCGA and GTEx datasets); (c and d) Kaplan–Meier analyses demonstrate the prognostic significance of the risk model in HCC-TCGA cohort. All patients were divided into the high-risk group and the low-risk group by the median risk scores. Survival analysis was performed to compare overall survival (OS) of 2 groups. The figure 1(c) is the 5-years survival, and the figure 1(d) shows OS. *p < 0.05; **p < 0.01; ***p < 0.001.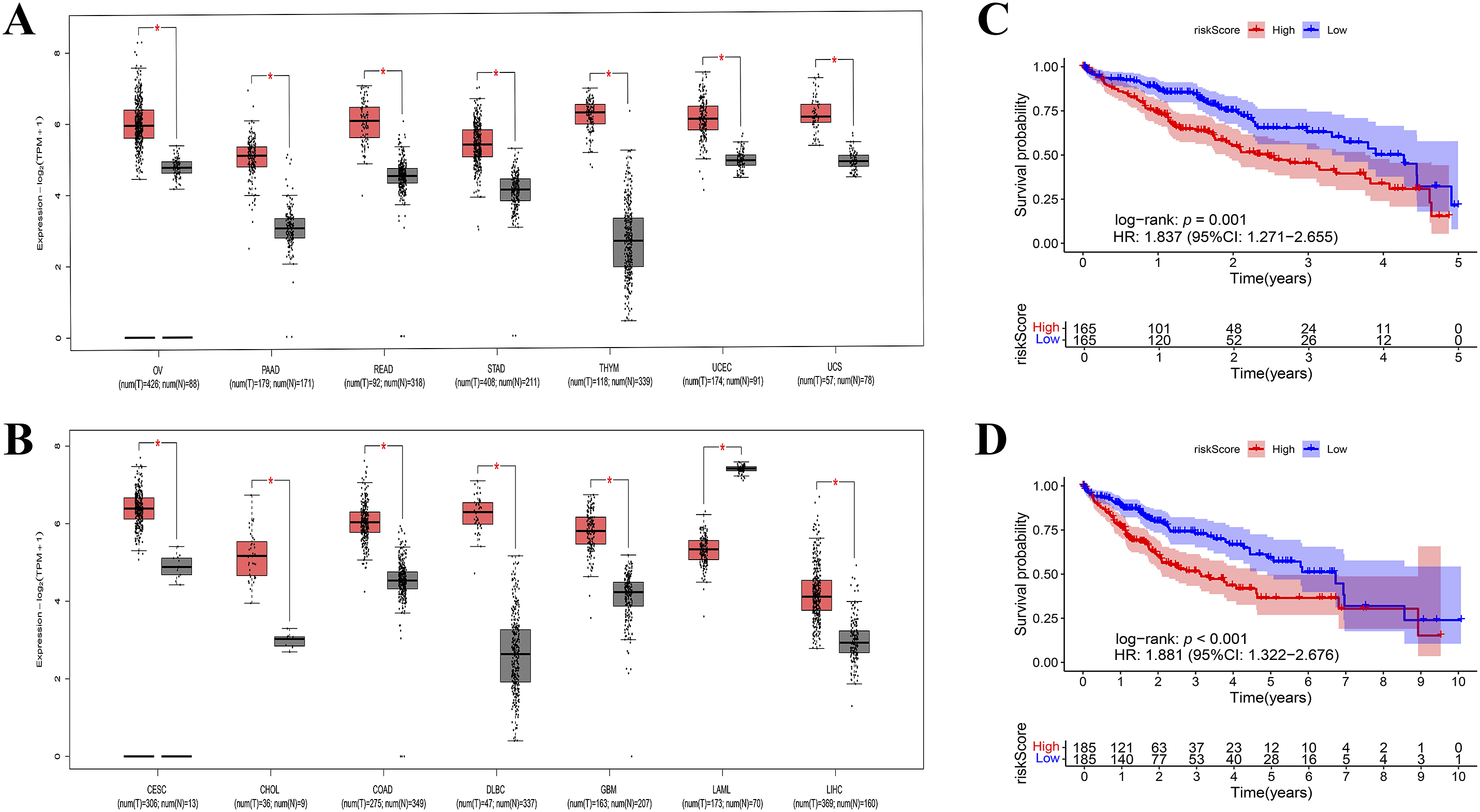
Immunologic features of the two risk groups
We examined the immune cell composition in the two risk groups. The results showed that the high-risk group had a higher proportion of activated memory CD4 + T cells (p < 0.05), while the low-risk group had higher proportions of resting memory CD4 + T cells (p < 0.01), monocytes (p < 0.05), and naive B cells (p < 0.01) (Figure 2(a)–(b)). The correlations among 14 types of immune cells in HCC tissues were then analyzed (Figure 2(c)). For example, CD8 + T cells were positively correlated with follicular helper T cells, while CD8 + T cells were negatively correlated with resting memory CD4 + T cells. Significant correlations between the risk score and the fraction of tumor infiltrating immune cells (TICs) in HCC. (a) Barplot showing the proportion of 22 kinds of TICs in the high-risk group and the low-risk group. (b) The ratio differentiation of 22 kinds of TICs between HCC samples with high and low risk score. (c) Multivariate regression analysis the correlation between 14 kinds of TICs in HCC (Fonts with a correlation coefficient >0.3 are marked in yellow).
Elevated macrophages subsets infiltrating density in HCC patients associated with poor prognosis
Given the differences in immune cell infiltration in HCC patients, we analyzed the relationship between tumor-infiltrating immune cells (TIICs) and prognosis. Kaplan-Meier analysis revealed that higher infiltration levels of resting dendritic cells, M0 macrophages, and M1 macrophages were associated with poor prognosis in HCC patients (Figure 3(a)–(c)), the expression level of PPIH was positively correlated with the invasion of M0 macrophages and negatively correlated with the expression level of M1 macrophages (Figure 3(e)–(f)). In contrast, higher infiltration levels of CD8 + T cells were linked to improved survival rates (Figure 3(d)), however, there was no significant correlation between the expression level of PPIH and the infiltration level of t resting dendritic cells and CD8 + T cells. Effect of TICs level on survival of HCC patients. (a–c) Kaplan-Meier analysis revealed that resting dendritic cells (A), M0 macrophages (b), M1 macrophages (c) higher infiltration level correlated with poor survival outcomes. (d) Kaplan-Meier analysis showed that lower infiltration levels of CD8 + T cells were associated with poor prognosis in HCC patients. (e and f) The expression level of PPIH is positively correlated with the infiltrating level of M0 macrophages. It is negatively correlated with the infiltration level of M1 macrophages.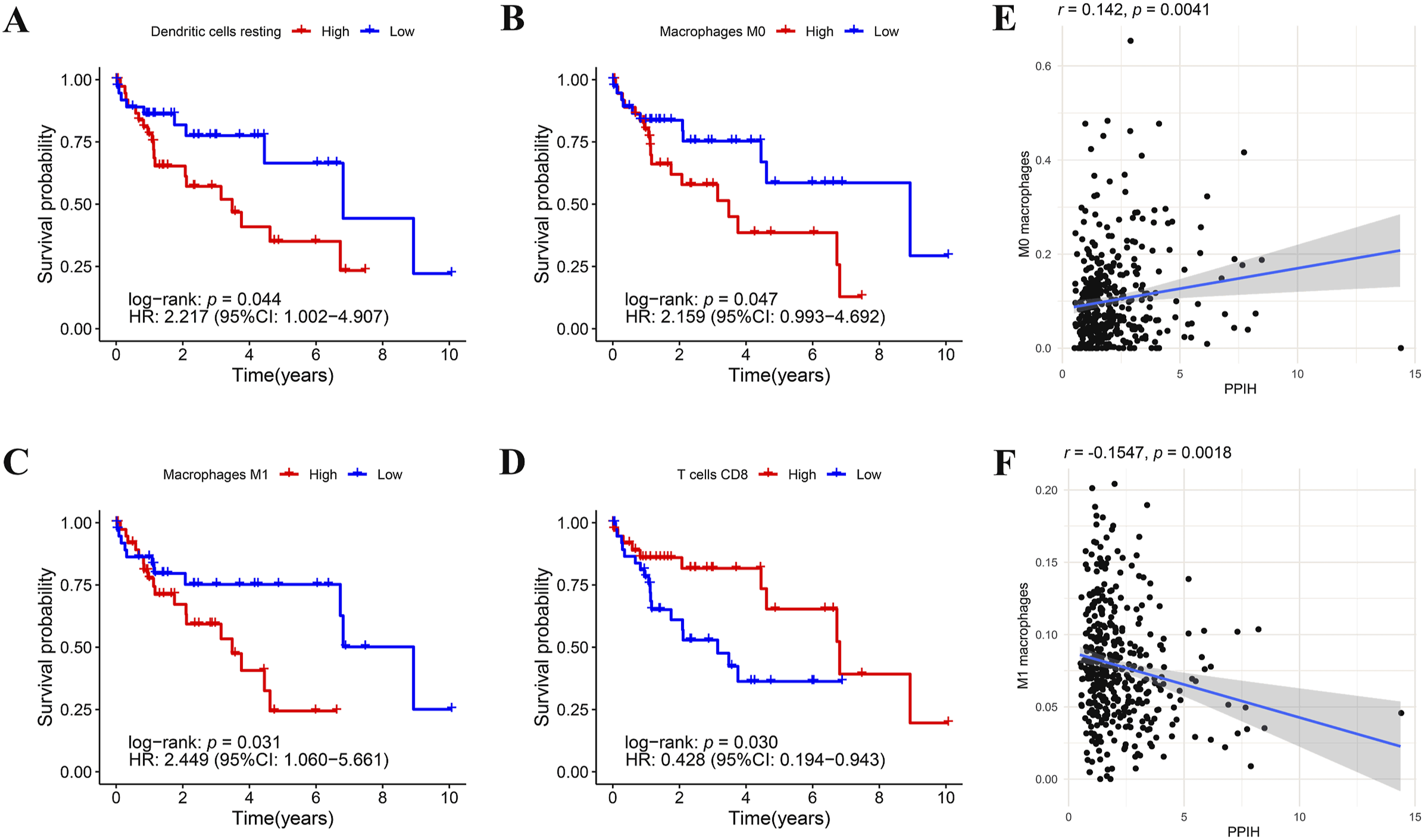
Relationship between risk score and clinical subtypes
Figure 4(a) shows the clinical characteristics of the high- and low-risk groups, where it was evident that the risk score was related to tumor grade, stage and AFP, the forest plot illustrating the relationship between PPIH expression and the clinical data of HCC patients using multivariate Cox regression analysis. Additionally, we found that PPIH expression is correlated with tumor grade and alpha-fetoprotein levels (Figure S1). Relationship between risk model and clinical subtypes. (a and b) Heat map and circle chart of the risk groups and clinical subtypes for HCC patients in the TCGA cohort. Age, gender, grade, stage, History other malignancy, viral infection status and laboratory index are shown as patient annotations. (c) Comparison of the differences in immune subtype (C1-C4) between high- and low-CD8T+ groups. **p < 0.01, ***p < 0.001.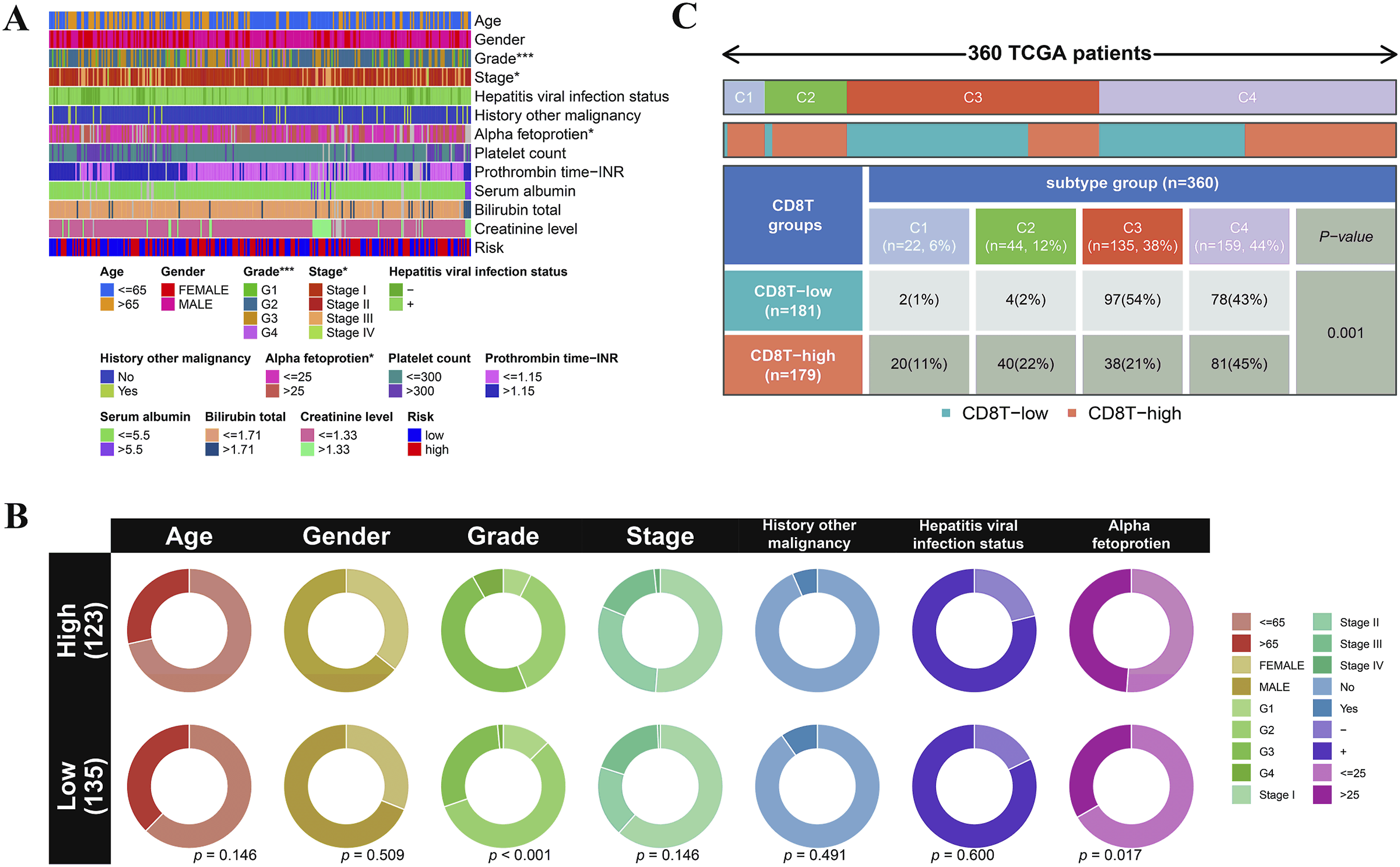
As shown in Figure 4(b), compared to the low-risk group, the percentage of patients with Grade 3-4 tumors was significantly higher in the high-risk group. Additionally, we compared the proportions of immune subtypes in HCC based on the infiltration level of CD8 + Tcells, revealing significant differences in immunophenotypes between the groups (Figure 4(c)).
Correlations between immune cell infiltration scores and Ppih expression levels
To assess the impact of Ppih expression on HCC, we examined the associations between Ppih levels and the infiltration of specific immune cell types in HCC tissues. Ppih expression was significantly correlated with the infiltration scores of 15 immune cell types. Notably, Student’ s t‐test was used to generate p-values; after Bonferroni correction for multiple measures, the adjusted p-value remained below 0.05, indicating statistical significance. There were negative correlations with the infiltration scores of natural killer cells, immature dendritic cells, gamma delta T cells, memory B cells, and monocytes (Figure 5(a)), multivariate regression analysis showed that PPIH expression level and macrophage infiltration level could be used as independent prognostic factors for HCC (Figure 5(b)). Correlations between immune cell infiltration scores and Ppih expression levels. (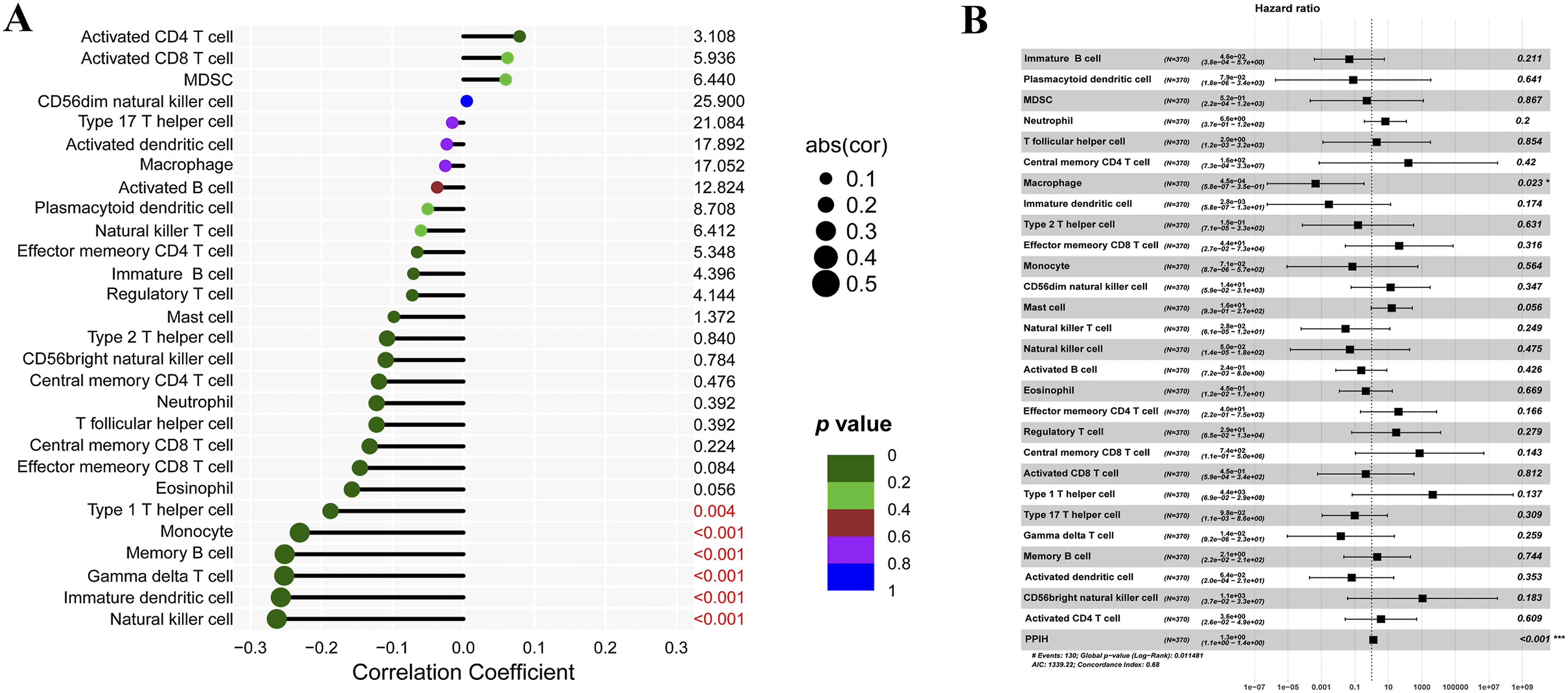
Relationship between risk score and immunotherapy
To explore the role of the risk score in predicting immunotherapeutic efficacy, we analyzed expression profiles from HCC patients in the TCGA dataset. The analysis revealed that HCC patients who responded to immunotherapy had lower risk scores compared to those who did not respond (Figure 6(a)), ROC curve analysis was performed (Figure 6(b)), However, the analysis indicated that the AUC value was relatively low, with limited specificity and sensitivity. This limitation may stem from the relatively small sample size or the need for more detailed subgroup analyses in hepatocellular carcinoma patients. These findings suggest that the risk score could serve as a predictive marker for immunotherapy response in HCC patients. Box plot presents the association of risk score with immunotherapy response in the IMvigor210 cohort (a) and ROC analysis (b). CR/PR represents complete response/partial response; SD/PD represents stable disease/progressive disease.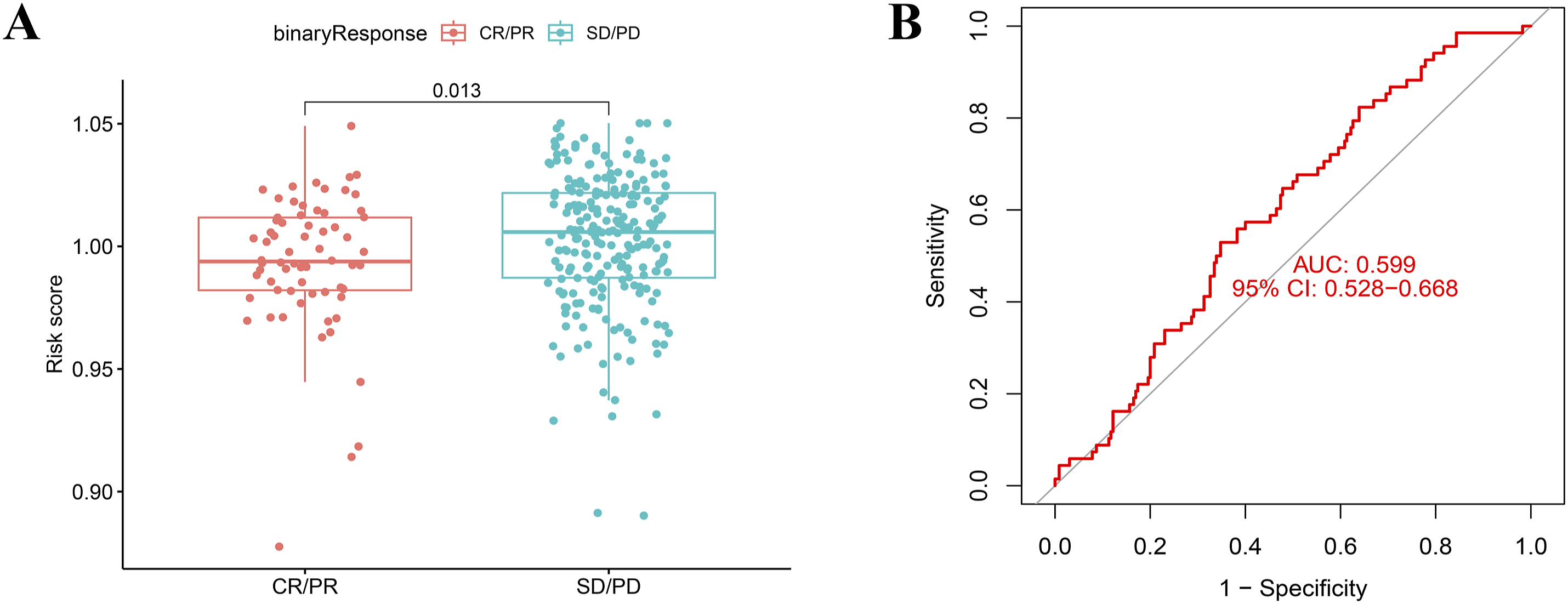
Correlation between serum immune cytokines and PPIH secretion levels
To investigate the effect of Ppih expression on HCC, we measured serum PPIH and related cytokine levels (IFN-γ, Granzyme B, IgG) in 40 clinical HCC patients using ELISA (Table S3 with raw data). The results showed that the serum levels of PPIH, IFN-γ, Granzyme B, and IgG were significantly elevated in liver cancer patients compared to healthy controls (Figure 7(a)–(d)). The differences were statistically significant, with p-values indicating increasing levels of significance (*p < 0.05; **p < 0.01; ***p < 0.001; ****p < 0.0001). Serum PPIH、IFN-γ、Granzyme B and IgG levels of HCC patients.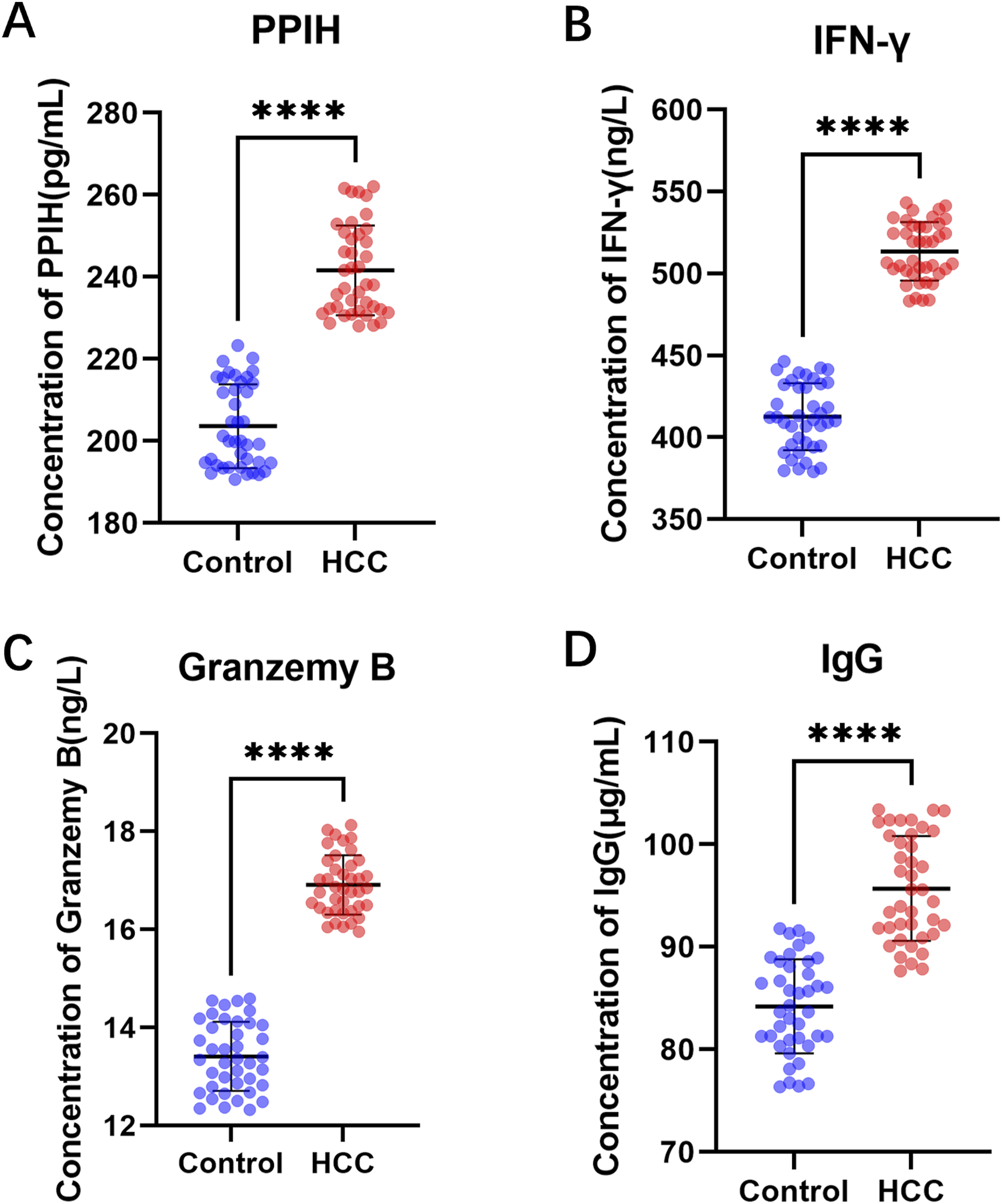
Discussion
HCC is one of the most lethal malignancies worldwide and is the only one among the top five deadliest cancers whose incidence is increasing year by year. 19 Further research is urgently needed to identify valuable prognostic markers and therapeutic targets. In recent years, immunotherapy, represented by immune checkpoint inhibitors, has revolutionized the traditional treatment of HCC, marking a new chapter in HCC management with promising results. 20 However, despite the success of immunotherapy in improving clinical outcomes for HCC, only a small percentage of patients benefit from it. Factors such as tumor cell immunogenicity, mutations in antigen-presenting cells, and the functionality of tumor-infiltrating T cells in the tumor microenvironment limit the efficacy of immunotherapy. 21 Additionally, some patients do not respond to immunotherapy or experience significant immune-related side effects, and a small subset of patients may even develop hyperprogressive disease (HPD) after receiving immunotherapy. 22 Therefore, there is an urgent need to discover effective predictive biomarkers to aid in the diagnosis, treatment, and prognosis of HCC.
As a member of the cyclophilin family, Ppih is involved in various important biological processes, and previous studies have linked Ppih to the progression of several malignancies.9,11,12 Our study aims to explore the potential of Ppih as a prognostic and immunotherapeutic marker for HCC patients. While prior research has shown Ppih to be implicated in the progression of some malignant tumors,9,11,12 its specific role in treatment response, prognosis, and regulatory mechanisms in HCC remains unclear. We focused on the abnormal expression of Ppih in HCC and investigated its correlation with immune cell infiltration and immune response. By employing bioinformatics analyses and clinical specimen validation, our study sought to assess the feasibility of Ppih as a prognostic and immunotherapeutic marker for HCC patients.
We first examined mRNA sequencing data from HCC patient samples in the TCGA and GTEx datasets. Previous studies have shown that Ppih mRNA levels are upregulated in HCC compared to normal liver tissue,23,24 consistent with our findings of Ppih overexpression in solid liver tumors (Figure 1(a)–(b)). Additionally, we developed a risk scoring model based on Ppih expression in HCC patients, categorizing them into high-and low-risk groups, and evaluated differences in prognosis between these groups. The results indicated that patients in the high-risk group had significantly lower overall survival compared to those in the low-risk group (Figure 1(c) and (d)), suggesting that high Ppih expression is associated with poor prognosis in HCC. Overall, Ppih appears to be a potential prognostic biomarker for HCC.
Next, we analyzed the immunological characteristics of the high-and low-risk groups (Figure 2). CD4 + memory T cells are a subgroup of antigen-specific CD4 + T cells that serve as a prognostic factor in several cancers, including kidney, lung, pancreatic, and breast cancers. For example, activated CD4 + memory T cells infiltrate significantly more in colorectal cancer tissues compared to normal tissues. 25 Furthermore, in gastric cancer, a higher infiltration level of activated CD4 + memory T cells is associated with a better prognosis, whereas resting CD4 + memory T cell infiltration has the opposite effect. The inverse correlation between these two cell types suggests that metabolic reprogramming may drive the transformation between activated and dormant CD4 + memory T cells, influencing prognosis in gastric cancer patients. 26 In our study, the high-risk group exhibited a greater infiltration of activated memory CD4 + T cells, while the low-risk group showed an increase in resting memory CD4 + T cells, monocytes, and naive B cells. This finding suggests that the elevated infiltration level of activated memory CD4 + T cells may promote the development and progression of HCC. Additionally, Chaoul N et al. 27 proposed that the recruitment of terminally differentiated CD4+ and CD8 + T cells to tumors is impaired, whereas effector memory CD4 + T cells are more likely to infiltrate tumor sites. While CD4+ and CD8 + T cells in tumors exhibit a higher activation level than their circulating counterparts, they often display an exhausted phenotype. This controversy warrants further investigation. “Quiescent” refers to a specific state of cells. 28 In homeostasis, T cells typically remain in a resting state, and their abnormal activation can lead to disease. Researchers from Yale University have discovered that T cells lacking BTG1/2 undergo increased mRNA abundance, resulting in spontaneous proliferation and activation, which lowers the activation threshold. 29 In Figure 2(b), we found no significant association between the HCC risk score and the proportion of Treg cells infiltrating the tumor. However, recent studies, 30 have indicated that the occurrence and progression of HCC are linked to the unique immune response profile of CD4 + CD25+ Foxp3 cells within the liver microenvironment. Regulatory T cells are the most abundant suppressor cells in the tumor microenvironment. They highly express checkpoint molecules, such as cytotoxic T-lymphocyte-associated antigen (CTLA-4) and programmed cell death receptor-1 (PD-1), and play critical roles in tumor progression, invasion, and metastasis. As such, they are considered promising direct targets for immune checkpoint inhibitors (ICIs). Various reports have demonstrated that CD8 + T cells and CD4 + T cells have opposite cancer-promoting and anticancer effects, both of which are inhibited by Treg cells. 31 However, the role of B cells in HCC remains controversial. 32 In conclusion, these findings suggest that Ppih expression induces distinct immune microenvironments in HCC.
Further analysis of the relationship between tumor-infiltrating immune cells (TIICs) and prognosis in HCC patients showed that high infiltration levels of resting dendritic cells, M0 macrophages, and M1 macrophages were associated with poor prognosis (Figure 3(a)–(c)). Dendritic cells capture, process, and present antigens to T cells via MHC-II, playing a key role in coordinating the immune response. 33 Higher dendritic cell numbers in tumors are typically associated with better survival outcomes.34,35 However, in the resting state, dendritic cells exhibit low levels of MHC and B7 molecules on their surface, limiting their ability to present antigens to T cells. Macrophages are a major component of leukocyte infiltration in tumor stroma and play a crucial role in tumor development. 36 Zheng et al. demonstrated that large numbers of macrophages infiltrating HCC tissues contribute to tumor progression by inducing immunosuppression, promoting tumor cell metastasis, and enhancing angiogenesis. 37 It is important to note that our results do not contradict previous findings, 38 which show that high CD8 + T cell infiltration is associated with a favorable prognosis (Figure 3(d)). Although we found no significant correlation between PPIH expression levels and the infiltration levels of resting dendritic cells and CD8 + T cells, Figure 5(a) shows that PPIH levels were inversely associated with two subtypes of CD8 + T cells: central memory CD8 + T cells (TCM) and effector memory CD8 + T cells (TEM). Long-lived memory CD8 + T cells play a critical role in tumor immunity, with TCM and TEM cells exhibiting strong anti-tumor activity. An increased proportion of TCM/TEM cells in the blood correlates with an elevated expression profile of inflammatory genes in tumors, underscoring the importance of TCM cells in the anti-tumor immune response. 39 It is widely accepted that tumor-associated macrophages (TAMs) can exist in two distinct states: anti-tumor M1 macrophages and pro-tumor M2 macrophages. In Figures 3(e), (F), and 5(b), we observed that the expression level of PPIH was positively correlated with the infiltration of M0 macrophages but negatively correlated with M1 macrophages. Compared with the low PPIH expression group, the high PPIH expression group exhibited significantly reduced infiltration of resting memory CD4 + T cells and M1 macrophages, whereas M0 macrophage infiltration was significantly increased. These findings suggest that PPIH may promote the development and progression of HCC, potentially influencing the infiltration of distinct immune cell populations. However, this hypothesis requires further validation.
In addition, we confirmed the role of Ppih in the clinicopathological characteristics of HCC. By comparing the clinical features of different risk assessment groups, we found that high Ppih expression was associated with advanced pathological grade, stage and AFP (Figure 4(a)–(b) and Figure S1). The correlation coefficient between the risk score and tumor grade (r = 0.2516) was statistically significant (p < 0.05), whereas the correlation coefficient between the risk score and AFP (r = 0.0928) was not statistically significant (p > 0.05), This may be due to the limited availability of clinical information on AFP levels in some samples, which reduced the sample size available for analysis (see Table S2).
Mutations in TP53 eliminate the tumor-suppressive activity of p53, drive tumor progression, and are associated with poor prognosis in various cancers. Our previous studies revealed that the expression level of PPIH in hepatocellular carcinoma (HCC) patients was correlated with TP53 mutation status. Specifically, the expression of PPIH mRNA was significantly higher in HCC patients with TP53 mutations than in those without TP53 mutations. 10 Lee et al. 40 reported that CypA transcription is directly regulated by two key transcription factors involved in cancer development: p53 and hypoxia-inducible factor-1α (HIF-1α). Since both PPIH and CypA are cyclophilin proteins, it is plausible that TP53 regulates PPIH mRNA expression.
Furthermore, whether PPIH participates in alternative splicing (AS) events or mediates HCC development under the regulation of HIF-1α,41,42 thereby influencing tumor formation and metastasis, remains to be fully understood.
Similarly, in our team’s previous studies, we found that PPIH overexpression in HCC is closely associated with TP53 mutation. The overexpression of PPIH primarily results from elevated mRNA levels, likely driven by changes in its upstream transcription factors, such as TP53. 43 Furthermore, significant differences were observed in CD8 + T cell infiltration levels between HCC immune subtypes in high- and low-risk groups (Figure 4(C)). These findings support our earlier conclusion that Ppih can serve as an indicator of HCC progression, and as previously reported, 44 high CD8 + T cell infiltration is predictive of a favorable prognosis.
Next, we evaluated the relationship between Ppih expression and specific immune cell types infiltrating HCC tissues. The liver contains a large number of immune cells, including natural killer (NK) cells, natural killer T (NKT) cells, innate lymphoid cells (ILCs), gamma delta T cells (γδ T cells), macrophages, and dendritic cells (DCs), all of which patrol the liver and contribute to its immune-tolerant environment.45,46 Our study found that Ppih expression was significantly negatively correlated with the infiltration scores of NK cells, immature dendritic cells, γδ T cells, memory B cells, and monocytes in HCC (Figure 5), suggesting that patients with high Ppih expression may exhibit signs of immunosuppression.The liver is a complex organ with vital physiological functions, including metabolism, glucose storage, and drug detoxification. Its unique immune properties—such as the abundance of cytotoxic CD8 + T cells and innate lymphocytes, including natural killer cells, γδ T cells, MAIT cells, and iNKT cells—highlight its significant role in anti-tumor immune surveillance. Despite the strong immune surveillance in the liver, especially the large population of NK cells, the classical tumor microenvironment (TME) presents challenges. Poor perfusion in the TME leads to the accumulation of tumor cell metabolites, decreased oxygen levels, and reduced nutrient availability, all of which impair the number and function of immune cells. 47 It is hypothesized that PPIH may influence the TME by promoting the occurrence and progression of HCC. However, this speculation requires further experimental validation.
Although immunotherapy has greatly improved clinical outcomes for HCC patients by enhancing the immune system, only a small subset of patients responds favorably to treatment.48,49 To assess the potential of using risk scores to predict patient responses to immunotherapy, we analyzed data from the TCGA database. Our results showed that patients in the complete response/partial response (CR/PR) group had lower mean risk scores compared to those in the stable disease/progressive disease (SD/PD) group (Figure 6). This strongly suggests that Ppih may serve as an effective marker for predicting immunotherapy efficacy. In conclusion, high expression of PPIH in HCC is associated with poor prognosis, immune cell infiltration levels, and immunotherapy response. With the increasing understanding and characterization of the immunological features of the tumor microenvironment, immune checkpoint inhibitor (ICI) therapies have further expanded the scope of systemic treatments for HCC. Evidence suggests that atezolizumab combined with bevacizumab demonstrates greater efficacy compared to sorafenib. 50 Additionally, our team has found that PPIH may influence the development of HCC through the spliceosomal pathway. These findings suggest that PPIH could serve not only as a novel biomarker for diagnosing HCC but also as a potential target for anti-cancer strategies.10,43
Finally, we investigated the secretion levels of PPIH and related cytokines (IFN-γ, Granzyme B, and IgG) in serum samples from clinical HCC patients. The results were consistent with mRNA sequencing data, with elevated PPIH levels observed in the serum of HCC patients (Figure 7(a)), indicating the potential of PPIH as a serological biomarker. However, in contrast to our earlier findings (Figure 5), serum levels of IFN-γ, Granzyme B, and IgG were positively correlated with PPIH and were also significantly elevated in HCC patients (Figure 7(b)–(d)). IFN-γ and Granzyme B are synthesized and secreted by NK cells and have anti-proliferative, antiviral, and anti-tumor functions.51,52 The interactions between NK cells, tumor cells, and other immune cells in the microenvironment remain complex and are not fully understood. Some studies report lower levels of IFN-γ in HCC, alongside reduced NK cell numbers in peripheral blood and tumors. 53 Variations in these findings may be related to factors such as tumor treatment and size. For instance, Saxena et al. 54 found that IFN-γ levels were highest in HCC patients, followed by healthy controls. Their multiple regression analysis indicated that genotype significantly influenced IFN-γ expression, suggesting that genetic background may account for the differences in these results. While B cells are primarily responsible for producing antibodies and inducing anti-tumor responses, pathogenic antibodies can also promote chronic inflammation and tumorigenesis. 55 Studies have confirmed that pathogenic antibodies promote tumor progression by targeting tumor antigen HSPA4, 56 which explains why high circulating immunoglobulin levels are generally associated with tumor metastasis and poor prognosis.
In addition, we classified the causes of 40 HCC patients according to whether they had viral infection (Table S1), and we found that about 30% of HCC patients had viral infection, which was often accompanied by cirrhosis and fatty liver. An epidemiological study has shown that hepatitis B virus (HBV) and hepatitis C virus (HCV) remain the most important global risk factors for HCC. 57 The presence or absence of infection and the status of infection may affect the level of tumor microenvironment and immune cytokine secretion. Li et al. showed that the malignant development of HBV-related HCC is closely related to RNA-binding proteins, including Ppih. 58 At the same time, it has been reported that approximately 90% of HCV-associated HCC cases have prior cirrhosis, so HCV may promote tumorigenesis through repeated injury, regeneration, and fibrosis. 9 In this study, the levels of PPIH were inconsistent with the levels of immune cell infiltration and may have been caused by the inconsistencies in the infection information we collected from patients.
Our study focused on exploring the role of PPIH in immune infiltration in HCC patients and its response to immunotherapy, yielding some preliminary conclusions. However, as with most studies, there are limitations to the current study design. Due to the insufficient sample size caused by various objective factors, as well as incomplete clinical information and pathological features, the generalizability of these results is limited.
The tumor microenvironment and immune status are influenced by multiple factors. For example, we were unable to analyze differences in serum cytokine levels among HCC patients with different clinical stages or grades, nor could we determine whether these indicators accurately reflected disease severity. This limitation may also explain the inconsistency between serum cytokine levels and the results of tissue immune cell infiltration. Additionally, in evaluating the role of the risk score in predicting immunotherapy efficacy, our analysis relied solely on data from the TCGA database. The absence of an independent external validation cohort further limits the ability to confirm the accuracy and reliability of the risk score in predicting immunotherapy responses.
The single-center sample will have selection bias in our paper data. Therefore, these findings must be interpreted cautiously, and the limitations outlined should be taken into account. We acknowledge that increasing the cohort size, adding more clinical samples, and incorporating additional experiments will be essential to further validate and refine our conclusions. Future studies will also focus on functional assays to build upon these preliminary findings. Specifically, we plan to investigate the impact of Ppih on proliferation, migration, and invasion capabilities in hepatocellular carcinoma (HCC) cell lines by constructing stable Ppih knockout and overexpression models. These studies will allow us to elucidate the mechanistic role of Ppih in HCC progression and verify its involvement in cellular proliferation, migration, and invasion, ultimately strengthening our preliminary findings.
Conclusions
In conclusion, our study confirms that increased Ppih expression in HCC is associated with poor prognosis in patients. Furthermore, Ppih is linked to immune cell infiltration in HCC, and patients with high Ppih expression appear to be less responsive to immunotherapy. Ppih shows great potential as a prognostic and immunotherapeutic marker for HCC. However, further research is needed to elucidate the specific mechanisms by which Ppih induces immunosuppression and contributes to poor outcomes in HCC.
Supplemental Material
Supplemental Material - PPIH associated with immune infiltrates and immunotherapy response in hepatocellular carcinoma
Supplemental Material for PPIH associated with immune infiltrates and immunotherapy response in hepatocellular carcinoma by Haini Chen, Haixia Chen, Renjie Wang, Peng Ren and Jun Ye in European Journal of Inflammation
Supplemental Material
Supplemental Material - PPIH associated with immune infiltrates and immunotherapy response in hepatocellular carcinoma
Supplemental Material for PPIH associated with immune infiltrates and immunotherapy response in hepatocellular carcinoma by Haini Chen, Haixia Chen, Renjie Wang, Peng Ren and Jun Ye in European Journal of Inflammation
Supplemental Material
Supplemental Material - PPIH associated with immune infiltrates and immunotherapy response in hepatocellular carcinoma
Supplemental Material for PPIH associated with immune infiltrates and immunotherapy response in hepatocellular carcinoma by Haini Chen, Haixia Chen, Renjie Wang, Peng Ren and Jun Ye in European Journal of Inflammation
Supplemental Material
Supplemental Material - PPIH associated with immune infiltrates and immunotherapy response in hepatocellular carcinoma
Supplemental Material for PPIH associated with immune infiltrates and immunotherapy response in hepatocellular carcinoma by Haini Chen, Haixia Chen, Renjie Wang, Peng Ren and Jun Ye in European Journal of Inflammation
Footnotes
Acknowledgments
We appreciate the physicians’ and the patients’ involvement in the research.
Statements and declarations
Author Contributions
All of the authors have given their approval to the final version of the paper. JY and PR conceived the research, evaluated the data, and authored the manuscript, and Haini Chen, Haixia Chen and RW carried out the experiments.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Guizhou Provincial Basic Research Program (Natural Science) (No. Basic of Guizhou Science Cooperation Foundation - ZK [2023] General 337), Southeast Guizhou Basic Research Program (Natural Science) (No. Basic of Southeast Guizhou Science Cooperation Foundation [2022] number 18), and Guizhou Province high-level innovative talent Training Program (No: Qian thousand layers of talent (2024) 202214).
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.