
Abstract
Background: Type 2 diabetes mellitus (T2DM) significantly contributes to sepsis, with patients suffering from both conditions exhibiting greater severity and higher mortality rates compared to those with sepsis alone. Elderly individuals in the intensive care unit (ICU) are particularly prone to these comorbidities. A nomogram prediction model was developed to accurately assess prognosis and guide treatment for elderly patients with sepsis and T2DM. Methods: Data from 1489 patients with sepsis and T2DM in the Medical Information Mart for Intensive Care IV (MIMIC-IV) database were analyzed and categorized into 28-days survival (n = 1156) and 28-days death groups (n = 333). The dataset’s clinical characteristics were employed to create a nomogram predicting 28-days mortality in elderly ICU patients with sepsis and T2DM. The least absolute shrinkage and selection operator (LASSO) regression identified candidate predictors, followed by a multivariate logistic regression analysis incorporating variables with p < .05 into the final model. A nomogram was then constructed using these significant risk predictors. The model’s discriminatory power was evaluated through a receiver operating curve (ROC) and the area under the curve (AUC). Additionally, model performance was assessed using a calibration plot and the Hosmer-Lemeshow goodness-of-fit test (HL test), and clinical utility was examined via decision curve analysis (DCA). Results: Risk factors incorporated into the nomogram included age, ICU length of stay, mean blood pressure (MBP), metastatic solid tumor, Sequential Organ Failure Assessment (SOFA) score, Logistic Organ Dysfunction System (LODS) score, blood urea nitrogen (BUN), and vasopressor use. The predictive model demonstrated robust discrimination, with an AUC of 0.802 (95% CI 0.768–0.835) in the training dataset and 0.753 (95% CI 0.697–0.809) in the validation set. Calibration was confirmed with the HL test (p > .05), and DCA indicated clinical usefulness. Conclusion: This new nomogram serves as a practical tool for predicting 28-days mortality among elderly ICU patients with sepsis and T2DM. Optimizing treatment strategies based on this model could enhance 28-days survival rates for these patients.
Introduction
Sepsis is a critical condition characterized by organ dysfunction arising from an unregulated host response, posing a life-threatening risk. 1 It frequently serves as the proximate cause of death for critically ill patients in the intensive care unit (ICU), remaining a leading contributor to global morbidity and mortality. 2 Annually, sepsis affects over three million patients worldwide, with mortality rates reaching 30%–50%, thus imposing significant burdens on both individuals and society. 3 Sepsis typically presents with rapid onset and swift progression, affecting multiple organs and proving difficult to reverse, necessitating immediate treatment upon diagnosis.
The etiology of sepsis is complex and perilous, originating from various factors and impacting multiple organ functions. Diabetes, a globally escalating metabolic disorder, mirrors this trend. Its prevalence approaches pandemic levels due to lifestyle shifts and the widespread adoption of Western diets rich in processed foods. 4 Patients with diabetes form a significant group at increased risk for post-sepsis complications and elevated mortality. 5 Numerous indicators suggest that patients with diabetes6–9 have a 2 to 6 times higher susceptibility to sepsis than their non-diabetic counterparts. 10 Furthermore, diabetic individuals face higher sepsis-related morbidity and mortality compared to non-diabetic individuals. 11 Preclinical studies reveal that diabetes alters elements of the innate immune system and suppresses the adaptive immune system. 12 Particularly in type 2 diabetes, chronic inflammation, immune response suppression, and significant infection-related morbidity occur. In diabetes, inflammatory pathways are activated via toll-like receptors such as TLR2 and TLR4, along with indirect activation through TLR signaling.13,14
Elderly patients often present to the ICU with complex and severe conditions, frequently leading to poor prognosis. There is controversy regarding the ICU admission of elderly patients, as studies indicate that over half of these admissions involve patients nearing the end of life. 15 The incidence of sepsis increases with age, especially in the extremely elderly population (age ≥80 years), showing a strong association with significantly higher mortality in this demographic. 16
Currently, no effective scale exists to assess the prognosis and condition of elderly patients with sepsis and T2DM, leading to treatment delays and additional challenges. The Sequential Organ Failure Assessment (SOFA) score and the Logistic Organ Dysfunction System (LODS) provide some utility in assessing patient conditions by focusing on organ physiological functions. However, these metrics lack specificity and sensitivity in evaluating clinical practices and prognoses for elderly patients with sepsis and T2DM. Consequently, these scoring systems are inadequate for guiding treatment in this patient population. To address the absence of an effective evaluation scale for predicting 28-days outcomes in elderly patients with sepsis and T2DM, this study analyzed risk factors for 28-days mortality using the Medical Information Mart for Intensive Care (MIMIC-IV) database. A nomogram prediction model was developed and compared with the SOFA score and LODS to thoroughly evaluate patient conditions, predict prognostic outcomes, and guide treatment for elderly patients with sepsis and T2DM.
Materials and methods
Study design
Research data were obtained from the MIMIC-IV database, which includes ICU patients from Beth Israel Deaconess Medical Center.1,17 Structured Query Language (SQL) combined with Navicat Premium facilitated data retrieval, while R software was used for subsequent data processing. The MIMIC-IV database (version 2.2, https://mimic.physionet.org/) is publicly accessible and offers comprehensive clinical research information, including demographic characteristics, examination results, disease diagnoses, and treatment modalities. It also includes in-hospital and post-discharge patient outcomes. Following authorization from the institutional review boards of both Beth Israel Deaconess Medical Center (Boston, MA, USA) and the Massachusetts Institute of Technology (Cambridge, MA, USA), and approval to access the MIMIC-IV database, data extraction was conducted for our study. The database ensures absolute confidentiality by anonymizing patient identities and private information, thereby maintaining adherence to stringent privacy standards. The data analysis for this study was conducted from January 2024 to February 2024.
Patient admission and data extraction
The inclusion criteria were as follows 1 : initial ICU admission, 2 diagnosis of both sepsis and T2DM, and 3 age over 65 years. The exclusion criteria included 1 : Sequential Organ Failure Assessment (SOFA) score <2 and 2 ICU stay duration of less than 24 h.
The Sepsis 3.0 Definition
1
was utilized, identifying patients with life-threatening organ dysfunction due to an uncontrolled host response to infection, with a SOFA score of ≥2. T2DM diagnosis was confirmed using the ninth edition of the International Classification of Diseases (ICD-9) codes applied to patient data in the MIMIC-IV database. Data extraction from the MIMIC-IV database was conducted using SQL with Navicat Premium. The sampling procedure is illustrated in Figure 1. Patients diagnosed with sepsis and T2DM based on ICD-9 codes were identified, and relevant data, including patient ID, SOFA score, and basic characteristics, were extracted. Ineligible patients (age <65 years, SOFA score <2, ICU stay <24 h) were excluded. Demographic data, vital signs, laboratory tests, comorbidities, scoring systems, and interventions were extracted using patient HADM_ID and ICUSTAY_ID. Demographic information included age, sex, and length of ICU stay. Vital signs encompassed heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), mean blood pressure (MBP), and oxygen saturation (SpO2). Laboratory tests included hematocrit (HCT), hemoglobin (HB), platelet count (PLT), white blood cell count (WBC), anion gap (AG), standard bicarbonate (SB), chloride, blood urea nitrogen (BUN), creatinine, sodium, and potassium. Comorbidities included congestive heart failure, myocardial infarction, peripheral vascular disease, cerebrovascular disease, chronic pulmonary disease, rheumatic disease, peptic ulcer disease, mild liver disease, renal disease, malignant cancer, severe liver disease, metastatic solid tumor, acquired immune deficiency syndrome (AIDS), and acute kidney injury (AKI). Scoring systems included the simplified acute physiology score II (SAPS II), SOFA score, logistic organ dysfunction system (LODS), and Charlson comorbidity index. Interventions included active dialysis, ventilation, vasopressin, epinephrine, norepinephrine, and neuroblock. Vital signs and laboratory data from blood examinations, basic blood biochemical indexes, and arterial blood gas were collected during the initial 24 h of ICU stay. If a variable was recorded multiple times, the most severe value was used. Flow chart of patient selection (MIMIC-IV, Medical Information Mart for Intensive Care I).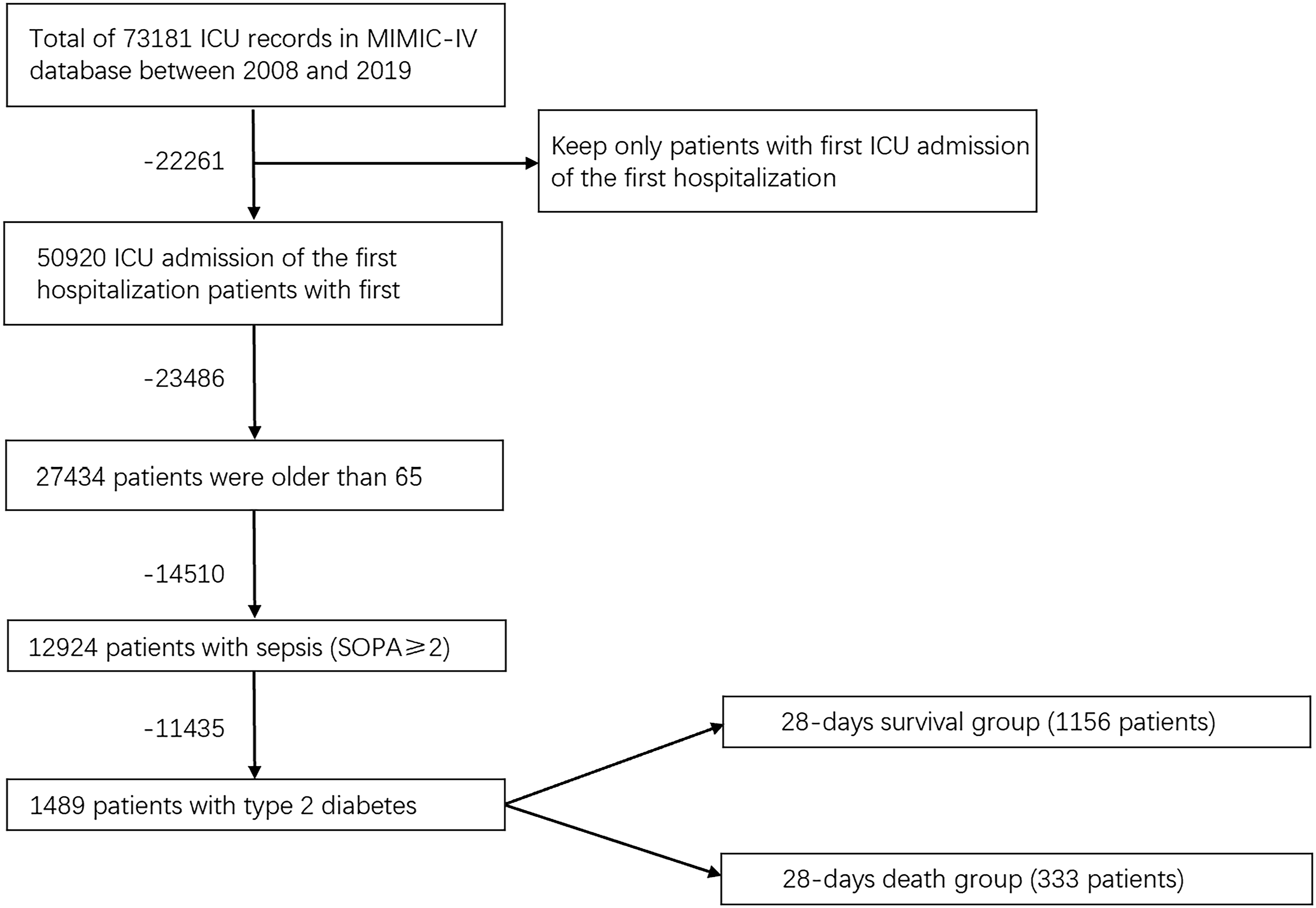
Statistical analysis
Continuous variables were summarized using the median and interquartile range, with the Wilcoxon rank-sum test applied for between-group comparisons. Categorical variables were presented as frequencies and proportions, and intergroup comparisons utilized Chi-square tests or Fisher’s exact test, as appropriate. Internal validation followed the bootstrap method, adhering to the Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) guidelines. 18 Data preprocessing involved handling missing data with the Multiple Imputation by Chained Equations (MICE) R package 19 using the neighbor interpolation method. We discarded data with missing values >20% and performed multiple imputation by chained equations (MICE) for data with missing values ≤20%. Sensitivity analyses were performed to ensure that the imputation did not significantly affect our results. Post-imputation, the least absolute shrinkage and selection operator (LASSO) method identified predictors of 28-days mortality . 20 Final candidate variables were determined based on cross-validation results, selecting lambda = min. 21 A multivariate logisticregression model was then constructed using these variables, with multicollinearity assessed through variable inflation factors (VIF).
Model performance was evaluated using the area under the receiver operating curve (AUC), sensitivity, and specificity, with the optimal cutoff point determined by the Youden index. A nomogram was generated using the R package “regplot.” Consistency between observed and predicted outcomes was assessed using the calibration C index (based on 1000 bootstrap resamplings), 22 calibration curve (illustrating the relationship between observed and predicted probabilities), Hosmer-Lemeshow goodness-of-fit test (HL test), and Brier score. Decision curve analysis (DCA) evaluated the net clinical benefit. 23 All statistical analyses were conducted using R (version 4.2.1), with a significance level of p < .05.
Results
Patient characteristics
Baseline characteristics of 28-days survival group and death groups.
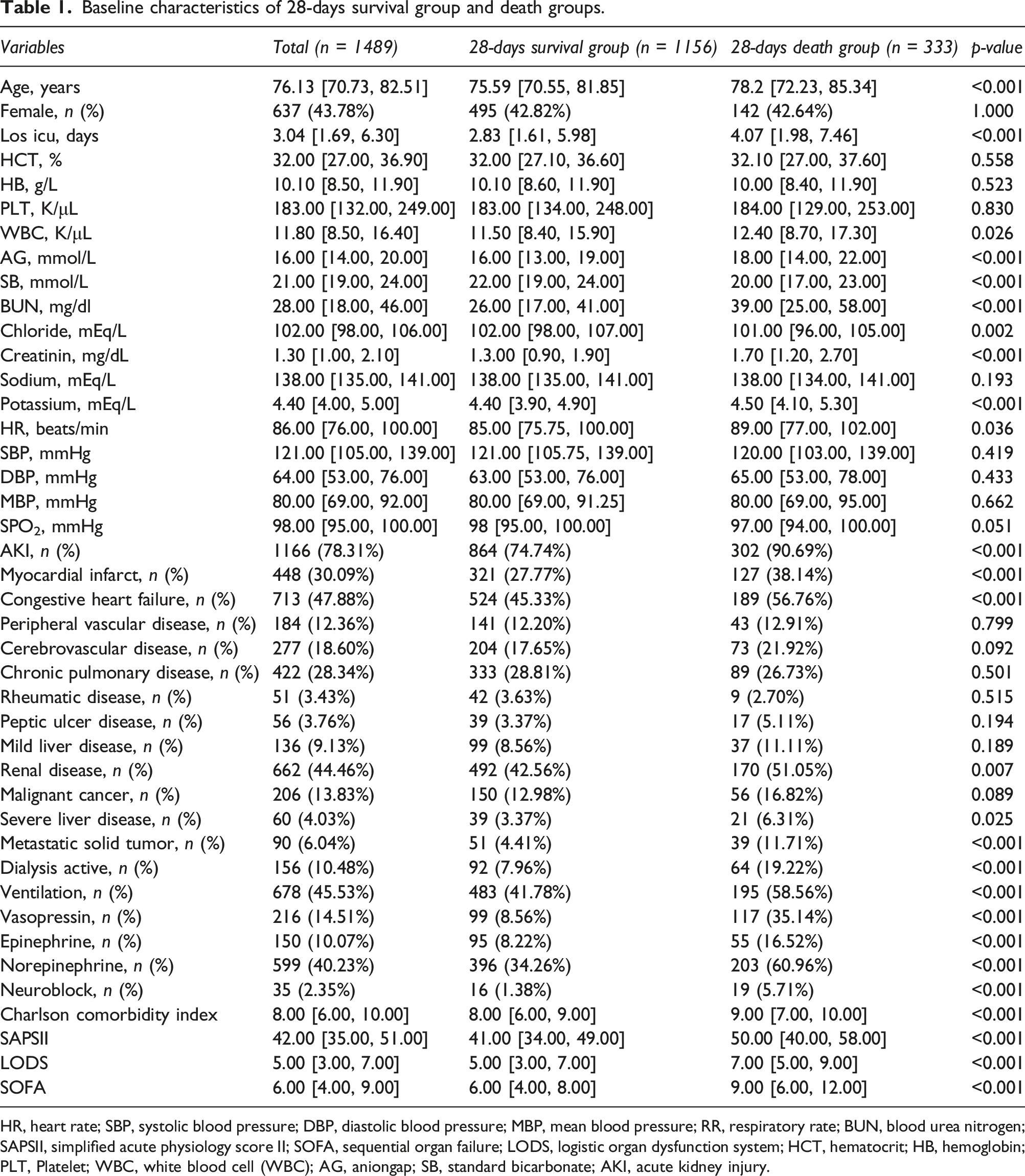
HR, heart rate; SBP, systolic blood pressure; DBP, diastolic blood pressure; MBP, mean blood pressure; RR, respiratory rate; BUN, blood urea nitrogen; SAPSII, simplified acute physiology score II; SOFA, sequential organ failure; LODS, logistic organ dysfunction system; HCT, hematocrit; HB, hemoglobin; PLT, Platelet; WBC, white blood cell (WBC); AG, aniongap; SB, standard bicarbonate; AKI, acute kidney injury.
Characteristics selection and development of a nomogram
Out of 43 variables, 10 were retained in the LASSO logistic regression model based on the binomial deviance minimum criteria (ratio 5:1) (Figure 2). The multivariable logistic analysis of these 10 variables is presented in Table 2. Eight predictors were included in the final multivariable logistic model: Age (OR: 1.055; 95% CI 1.035–1.076), ICU length of stay (OR: 0.962; 95% CI 0.940-0.984), metastatic solid tumor (OR: 2.902; 95% CI 1.594–5.283), SOFA score (OR: 1.185; 95% CI 1.121–1.253), vasopressin usage (OR: 2.974; 95% CI 1.998–4.427), LODS (OR: 1.075; 95% CI 1.012–1.142), mean blood pressure (OR: 1.013; 95% CI 1.006–1.021), and BUN (OR: 1.007; 95% CI 1.002-1.012). Based on this model, a nomogram was constructed to predict 28-days mortality in elderly ICU patients with sepsis and T2DM (Figure 3). Demographic and clinical feature selection using the LASSO logistic regression model. Multivariate logistic regression model of elderly patients with sepsis and T2DM in the training set. SOFA, sequential organ failure; LODS, logistic organ dysfunction system; MBP, mean blood pressure; BUN, blood urea nitrogen. Nomogram to predicting 28-days mortality in ICU elderly patients with sepsis and Type 2 Diabetes Mellitus. SOFA, sequential organ failure; LODS, logistic organ dysfunction system; MBP, mean blood pressure; BUN, blood urea nitrogen; ** means p < .01, ***means p < .001.


Apparent performance of the nomogram
The AUC for the model was 0.802 (95% CI 0.768–0.835) for the training set and 0.753 (95% CI 0.697–0.809) for the validation set (Figure 4(a) and 4(b)). The optimal cutoff values for the nomogram-predicted probability were set at 25.8% in the training set and 26.7% in the validation set, based on the maximum Youden index. Sensitivity, specificity, PPV, and NPV were 64.9%, 80.0%, 48.2%, and 89.3% in the training set, and 63.0%, 79.6%, 49.6%, and 87.1% in the validation set. The ROC values for the SOFA and LODS scoring systems incorporated into the regression were 0.712 and 0.709 in the training set, and 0.736 and 0.648 in the validation set, respectively, indicating that the model demonstrated superior predictive performance compared to commonly used clinical scoring systems. The calibration plot showed a good fit for the nomogram in both cohorts (Figure 5(a) and (b)). Additionally, the HL test of multivariable analysis demonstrated perfect consistency between predicted and observed values (training set, χ2 = 7.713, p = .462; validation set, χ2 = 5.986, p = .469). ROC curve and AUROC of SOFA, nomogram and LODS in training set Calibration curves of the predicted nomogram in the training set 

Clinical practice
DCA for the nomogram was performed on both the training and validation sets (Figure 6(a) and (b)). In the figure, the gray curve represents the scenario where all patients receive intervention, the straight black line indicates no patients receive intervention, and the red curve illustrates the clinical benefit provided by our model. Predicted probability thresholds were set at 10%–89% for the development cohort and 13%–85% for the validation cohort, with net benefits ranging from 0% to 24% and 0%–19%, respectively. Notably, as the threshold decreases, the net benefit also decreases. Our results indicate that the model provides superior net clinical benefit compared to the SOFA and LODS scoring systems. The DCA curve of medical intervention in patients with the nomogram, SOFA, and LODS in the training et 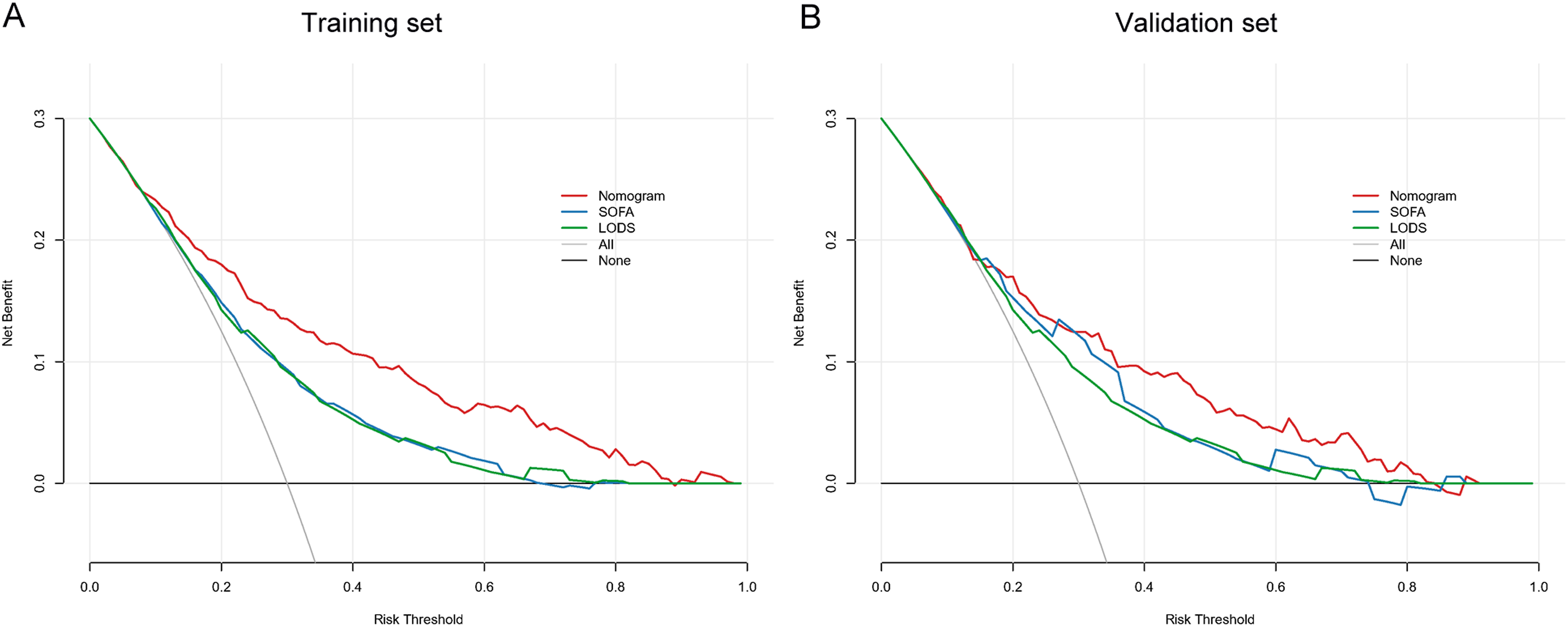
Discussion
Since the clinical definition of sepsis was established, physicians have faced significant challenges in diagnosing and treating this condition, largely due to its high mortality rates, reduced quality of life, and substantial economic burdens on patients. 24 Sepsis primarily induces systemic organ damage through an inflammatory response, with capillary endothelial damage and loss of peripheral circulation regulation being critical processes that can lead to septic shock. Physiopathological factors such as leukocyte extravasation, coagulation dysfunction, and inflammation-induced capillary dilation are major contributors to widespread tissue edema. 25 A nationwide observational study of over 500,000 individuals with type 2 diabetes revealed that type 2 diabetes is an independent risk factor for mortality in sepsis. 26 Given its increased prevalence 27 and association with impaired host defense against infections, 8 diabetes is a particularly significant risk factor for sepsis. The global incidence of diabetes is rising, with projections indicating it will affect over 500 million individuals by 2030, most of whom will develop type 2 diabetes. 28 Elderly patients, characterized by reduced immunity, 29 decreased organ reserve function, and a higher prevalence of comorbidities such as diabetes and coronary heart disease compared to younger individuals, 30 often present atypical clinical symptoms post-infection. This makes the diagnosis prone to oversight or misdiagnosis, leading to the rapid progression of sepsis to multiple organ failure 31 and subsequently high clinical mortality rates. Additionally, findings from a prospective cohort study indicate that older survivors of sepsis endure a greater burden of persistent disability and a higher 12-months mortality rate compared to younger patients. 32
Despite the scarcity of studies examining the risk factors influencing the prognosis of elderly patients with sepsis and T2DM, developing a nomogram to assist clinicians in identifying high-risk patients and understanding the impact of various risk factors on the 28-days prognosis in this population is essential. The predictive nomogram includes eight predictors: age, length of stay in the intensive care unit (LOS ICU), metastatic solid tumor, Sequential Organ Failure Assessment (SOFA), vasopressin, blood urea nitrogen (BUN), Logistic Organ Dysfunction System (LODS), and mean blood pressure (MBP). The model demonstrated robust performance, with an area under the curve (AUC) of 0.802 in the training set and 0.753 in the validation set. Conversely, the receiver operating characteristic (ROC) values for the SOFA and LODS scoring systems included in the regression were 0.712 and 0.709 in the training set and 0.736 and 0.648 in the validation set, respectively. These results indicate that the model exhibits superior predictive performance compared to commonly used clinical scoring systems. Decision curve analysis (DCA) further validates and endorses the use of this model.33,34 DCA evaluates prediction models by calculating the clinical net benefit. Findings suggest that interventions guided by the nomogram yield more favorable prognoses in both the training and validation sets compared to those guided by the SOFA score and LODS. The calibration of the prediction model was assessed using the Hosmer–Lemeshow test and calibration plots, 35 both of which demonstrated satisfactory calibration ability. Elderly patients with sepsis and T2DM exhibit higher 28-days mortality, and their clinical treatments pose greater challenges. Current sepsis guidelines do not recommend specific treatment methods and evaluation programs for patients with different infection sources and complications. Several systems are available for clinically evaluating patients with sepsis, such as the SOFA score, qSOFA, SAPSII, LODS, APACHE III, and APACHE IV. The SOFA score and qSOFA are primarily used for early and rapid disease assessments of patients with sepsis. 36 The Logistic Organ Dysfunction System (LODS) provides an objective tool for assessing the severity levels of organ dysfunction in the ICU, 37 with each variable in the LODS score screened and weighted by logistic regression. Research indicates that the LODS score exhibits higher accuracy than the qSOFA score and SOFA score. 38 However, the prediction efficacy for elderly patients with sepsis and T2DM remains uncertain.
Among the critical variables for predicting sepsis in elderly patients with both sepsis and T2DM, the most influential factors are the administration of vasopressors, mean blood pressure (MBP), blood urea nitrogen (BUN), Logistic Organ Dysfunction System (LODS), and Sequential Organ Failure Assessment (SOFA) scores following admission to the intensive care unit (ICU). These parameters are essential indicators for assessing circulatory disorders, respiratory complications, and other organ dysfunctions in elderly individuals with sepsis and T2DM. 39 The integration of vasopressors and MBP into scoring systems such as SOFA, LODS, SAPSII, and APSIII underscores their significance in disease prediction. 40 For instance, existing research has shown that BUN is associated with the 28-days mortality risk in sepsis. 33 Additionally, the inclusion of metastatic solid tumor as a new variable is significant. Intensive cytotoxic chemotherapy reduces the absolute neutrophil count in malignancies or solid tumors, leading to decreased patient survival rates. 41 The presence of metastatic solid tumors is closely linked to the immune status of each patient. Numerous studies have emphasized that immunocompromised individuals exhibit significantly higher incidence and mortality rates of sepsis compared to their immunocompetent counterparts.42,43 Cancer, by employing the immune checkpoint pathway and releasing immunosuppressive factors, can effectively dampen both innate and adaptive immune responses in the host. 44 Furthermore, research has established a correlation between Type 2 diabetes and an increased susceptibility to various forms of cancer.44–46 The immune system dysfunction shared by tumors and sepsis is associated with decreased survival rates in elderly patients with sepsis. 47
The qSOFA score was not included in our study. While qSOFA is extensively utilized in emergency and general wards due to its simplicity and convenience, the SOFA score offers multiple advantages. Primarily, the SOFA score provides superior multi-organ function assessment, evaluating six major organ systems—respiratory, cardiovascular, hepatic, coagulation, renal, and neurological—thereby delivering a comprehensive overview of a patient’s condition. This detailed scoring of each system’s functional impairment results in a more thorough evaluation of the patient’s health status. Conversely, the qSOFA score assesses only three parameters: respiratory rate, altered mental status, and systolic blood pressure, which, though straightforward, do not fully capture the status of multiple organ functions. Additionally, in ICU and dynamic monitoring contexts, the SOFA score proves more effective.48–50 Initially designed for ICU environments to monitor multi-organ failure, the SOFA score is both more suitable and clinically valuable for managing ICU patients. 51 The qSOFA score, primarily a rapid screening tool for non-ICU settings, shows limited effectiveness in the ICU. Given that this study focuses on ICU patient evaluation, the SOFA score holds greater relevance. Furthermore, the SOFA score enables dynamic monitoring of organ function changes during treatment, aiding physicians in adjusting treatment plans and enhancing outcomes. The qSOFA score, typically used for initial screening, lacks the capability for continuous monitoring.
Several limitations of this study must be acknowledged. Firstly, the diverse diagnostic criteria for sepsis, such as the Martin criteria, necessitate further validation of our model’s effectiveness using these different benchmarks. Additionally, the study’s retrospective observational design inherently limits the ability to establish causal relationships between the identified predictors and patient outcomes. The use of the MIMIC-IV database, with its specific inclusion criteria, resulted in the exclusion of certain populations, potentially limiting the generalizability of our model. While the MIMIC-IV database provides a wealth of high-quality clinical data, it also presents potential selection biases and demographic limitations, as the data primarily originate from a single large academic medical center in Boston, USA, which may restrict the applicability of our findings to other regions or healthcare settings. Consequently, our results may not be fully generalizable to broader populations. Future studies should utilize multicenter data to validate the generalizability and robustness of our model. Furthermore, data limitations prevented the inclusion of certain conventional factors known to influence sepsis outcomes, such as ventilation status, neurological symptoms, cardiac injury biomarkers, procalcitonin levels, neutropenia, and inappropriate empirical antibiotic therapy. The absence of these variables may affect the comprehensiveness and precision of our nomogram. Future research should aim to integrate these additional factors to enhance the model’s accuracy and comprehensiveness. LASSO regression and logistic regression models were selected for prediction analysis due to their high interpretability in clinical settings. Although more advanced machine learning techniques might offer improved predictive performance, they often lack the transparency and interpretability crucial for clinical decision-making. Therefore, the choice of models balances predictive performance with clinical interpretability. The study demonstrated the model’s robustness through internal validation. However, to comprehensively evaluate the robustness and effectiveness of the nomogram, future investigations should include external validation with independent datasets from various medical institutions and regions. This approach will ensure the model’s effectiveness in a wider range of clinical settings. Lastly, our nomogram prediction model is a valuable tool for assessing the 28-days mortality risk among ICU elderly patients with sepsis and T2DM. Clinicians can utilize this model for more accurate patient prognosis evaluations and personalized treatment plans, including initial risk assessment upon ICU admission, identifying high-risk patients for timely intervention, and dynamically adjusting treatment strategies to improve outcomes. Additionally, this model can aid in the efficient allocation of medical resources and optimize ICU management. By acknowledging these limitations and areas for future research, caution is emphasized when interpreting our results, and further studies are recommended to address these issues and validate our model in diverse clinical settings.
Conclusion
The newly developed nomogram, which includes age, length of stay in the intensive care unit (LOS ICU), metastatic solid tumor, Sequential Organ Failure Assessment (SOFA), blood urea nitrogen (BUN), Logistic Organ Dysfunction System (LODS), mean blood pressure (MBP), and vasopressor usage, effectively predicts 28-days mortality in elderly ICU patients with sepsis and Type 2 Diabetes Mellitus. Tailoring treatment strategies to address the identified factors within the model has the potential to improve the 28-days survival rates for this specific cohort of ICU patients.
Footnotes
Acknowledgement
We thank Bullet Edits Limited for the linguistic editing and proofreading of the manuscript. This research was supported by National Natural Science Foundation of China (81672526, 81802560, 82403182), and Special Program for Clinical Research of Shanghai Municipal Health Commission (2018470263, 20184Y0105) and Key Discipline of Tongji Hospital in Shanghai (ZD24-MN) and A nucleotide targeting lncRNA ZNF518A for AR-V7-mediated castration-resistant prostate cancer (ZLZH2202). This data used in this study are available at the database: ![]()
Author contributions
H.L.; Y.Z.: Designed the protocol, write the manuscript. X.W.; Q.W.; T.Z.; X.Q.; Y.Z.; W.J.; C.X.: Collected and analyzed the data. X.C.; G.W.: reviewed and edit the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by National Natural Science Foundation of China (81672526, 81802560, 82403182), and Special Program for Clinical Research of Shanghai Municipal Health Commission (2018470263, 20184Y0105) and Key Discipline of Tongji Hospital in Shanghai (ZD24-MN) and A nucleotide targeting lncRNA ZNF518A for AR-V7-mediated castration-resistant prostate cancer (ZLZH2202).