
Abstract
Objective
To investigate the predictive value of neutrophil-to-lymphocyte ratio (NLR) for early perforation of the appendix in patients with acute appendicitis (AA).
Methods
Two hundred and 80eighty patients with the first episode of AA within 48 hours and not yet treated with antibiotics were included in this study retrospectively; divided into two groups by the presence or absence of perforation. The clinical data, traditional inflammatory indexes, and NLR were compared between the two groups. The predictive value of inflammatory indexes on the early appendiceal perforation was explored.
Results
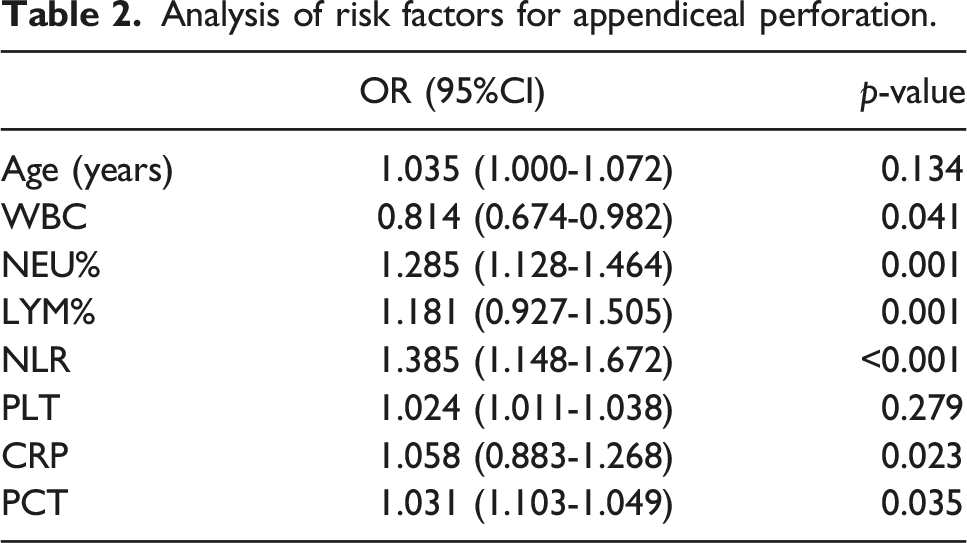
Patients in the perforated group were older, with higher blood WBC, NEU% and NLR, lower LYM% and PLT, higher serum CRP and PCT, and longer hospitalization time. Multivariate regression analysis revealed that high WBC, NEU%, NLR, CRP, PCT, and low LYM% were independent risk factors for early appendiceal perforation. The ROC curves revealed that the predictive value of WBC, CRP, and PCT for early appendiceal perforation was low. NLR, LYM%, and NEU% had a higher predictive value, with AUC values of 0.947, 0.928, and 0.920, respectively. NLR had the highest predictive value. The diagnostic Cut-off value of NLR is 10.83 with a sensitivity of 0.963, and a specificity of 0.850.
Conclusion
NLR can be used as an effective and sensitive predictive maker of early appendiceal perforation in AA patients. It is easy to generate from existing routine clinical laboratory testing for AA and can be included in complete blood count (CBC) as a routine or add-on value.
Introduction
Acute appendicitis (AA), with an individual lifetime incidence of approximately 7%, is the most common surgical emergency in clinical practice. Appendectomy has been the gold standard for the treatment of AA in the past, 1 but in recent years, this traditional treatment paradigm is facing a great challenge. More and more literatures confirm that antibiotic-based conservative treatment is effective and can avoid anesthesia and surgery-related complications. 2 However, in complicated AA, especially perforated AA, despite conservative treatment being proposed, surgery is still the treatment of choice. Most patients with complicated AA treated conservatively still need to undergo appendectomy within a short period. 3 If not treat appropriately, perforated appendix can progress rapidly, leading to spetic shock, multiple organ dysfunction syndrome (MODS), and death. 4 Therefore, it is critical to predict appendiceal perforation effectively and accurately as soon as possible. Neutrophil-to-lymphocyte ratio (NLR) is a recently discovered indicator of inflammation level for grading severity and predicting prognosis in inflammatory diseases such as infections, sepsis, and tumors. NLR is extremely easy to apply and can be simply calculated from the results of a routine complete blood count (CBC) test. It does not cause any extra harm to patients or increase the economic burden of the health care system. Therefore, it has received more and more clinical attention.5–7 A few recent studies explored its clinical use in AA patients with promising results.8–11 The present study is intended to further explore the value of the NLR in the early prediction of perforated AA, to provide more supportive evidence for clinical decision-making.
Materials and methods
General data
Retrospective analysis of 568 patients with AA admitted to the Trauma Emergency Center of Shuguang Hospital, Shanghai University of Traditional Chinese Medicine, from January 2022 to January 2023 were performed. Confidentiality of all patients´ information was maintained and permission from the hospital ethical committee for the use of medical data and publishing of the study results was obtained. Inclusion criteria: (1) definitive diagnosis of AA (confirmed by histopathology); (2) onset of disease to surgical consultation time ≤48 h; (3) surgical treatment without prior conservative treatment; (4) first onset of disease; (5) age of 18-70 years old; (6) complete clinical, laboratory and pathological data. Exclusion criteria: (1) onset to surgical consultation time >48 h; (2) chronic appendicitis with or without acute episode; (3) conservative treatment; (4) with other infectious diseases, autoimmune disease, tumor, or other diseases, or long-term use of immunomodulatory drugs; (5) incomplete clinical, laboratory or pathological data; (6) antibiotics had been applied before obtaining blood specimens.
Methods
The clinical, laboratory and pathological data were reviewed. From the clinical notes and operative records, the results of routine complete blood count (CBC) and differential test, C-reactive protein (CRP), procalcitonin (PCT), liver and kidney function, blood coagulation, electrocardiogram, image studies were obtained. Perforation and gangrene of the appendix were observed and documented by surgeons during laparoscopic appendectomy. The pathologic reports were reviewed for macroscopic and microscopic perforation. Patients who had appendiceal perforation identified by surgeons and/or pathological confirmation of perforation were classified as perforated patients, while the rest of them were included in the group of non-perforated patients. The duration of the patient’s illness (from the symptom to the time of blood sampling), the duration of hospitalization, and other clinical data were recorded.
Statistical methods
All data were analyzed by IBM SPSS 22.0 statistical software, and p < .05 was interpreted as statistically significant. For data description, mean ± standard deviation was used for quantitative variables. Normal distribution of quantitative variables was confirmed by the Kolmogorov–Smirnov normality test. Categorical variables were presented as frequencies and percentages. t test, Fisher’ exact test and chi-square test were used for the statistical analysis between the groups. Multivariate logistic regression analysis was performed. The ROC curve was used to determine the optimal diagnostic cut-off value of the observed indexes, and calculate the sensitivity and specificity.
Result
According to the criteria in methods, a total of 280 cases of AA patients enrolled in the study period. 154 were males and 126 were females. The ages range from 18 to 70 years old with the mean age of 38.56 ± 15.34 years old. The duration of the disease was 2–46 h with the mean duration of 26.89 ± 19.45 h 54 cases were identified as perforated patients and 226 cases were non-perforated patients.
Comparison of general clinical data between the two groups
Comparison of general clinical data between the two groups.

Analysis of risk factors for early appendiceal perforation
Analysis of risk factors for appendiceal perforation.
ROC curve
The diagnostic value of each inflammatory index for early appendiceal perforation in patients with AA has analyzed. ROC curve suggested that traditional inflammatory indexes WBC, CRP, and PCT had low predictive value for early appendiceal perforation, with AUCs of 0.620, 0.700 and 0.757, respectively, while NLR, NEU%, and LYM% had high predictive value for early appendiceal perforation, with AUCs of 0.947, 0.920 and 0.928, respectively. Among all, NLR had the highest predictive value for early perforation in patients with AA. When the Cut-off value of 10.83 was used, the sensitivity and specificity of NRL were 0.963 and 0.850, respectively. See Figure 1 and table 3. ROC curves of each inflammatory index for the prediction of appendiceal perforation in patients with AA. Analysis of the diagnostic value of each inflammatory index for appendiceal perforation in AA patients.

Discussion
During inflammation, bone marrow releases a large number of neutrophils, prolongs the time of their regeneration, and then exerts its phagocytosis, resulting in a significant increase in the proportion of peripheral blood neutrophils and the release of a large number of active substances to increase their pathogen clearance capacity. 12 The cytokines released by the inflammatory response directly induce the acceleration of lymphocyte death, leading to a significant decrease in the proportion of peripheral blood lymphocytes, which in turn causes a significant increase in the NLR value of the patient. At the same time, a further increase in the NLR exacerbates the level of inflammation, resulting in a vicious circle. 13
NLR is a simple inexpensive marker of inflammation. It can be easily calculated from the differential WBC counts. NLR has shown important clinical value in many inflammatory diseases. 14 Studies have found that it not only serves as an independent risk factor for the prognosis of tumor patients but also has an important predictive value for the toxic side effects of radiotherapy in tumor patients. 15 In addition, it is an independent predictor of death in patients with sepsis. 7 NLR is also a marker of subclinical inflammation. As an inflammation index, it can be commonly used in the clinical diagnosis and grading the severity of infectious diseases.
AA is the most common cause of acute abdomen. The appendix used to be considered as a degenerative and useless organ so traditional appendectomy has always been the main treatment for AA. However, modern medicine has confirmed that the appendix plays an important role in intestinal immunity. In recent years, with the continuous discussion and research on the conservative treatment of AA, the traditional surgical model is challenged and questioned. 16 However, in patients with perforated AA, surgery is inevitable, because the rapid progression of perforated AA may easily lead to septic shock or even death. 17 Therefore, how to predict perforation in AA patients and how to diagnose a perforated appendix at an early stage are crucial.
A few recent studies have explored clinical use of NLR in AA patients with promising results.8–11 In pediatric AA, using NLR alone or combined NLR with other biomarkers8,18 have been shown to aid the diagnosis of AA and complications. In adult AA, the role of NLR in diagnosing and predicting complicated AA has also been investigated.9–11 However, no consensus has been reached on the cut-off value, sensitivity and specificity.
The aim of this study was to investigate the predictive and diagnostic value of NLR for early perforation in AA patients. Firstly, univariate and multivariate regression analyses were performed to determine whether high WBC, NEU%, NLR, CRP, PCT, and low LYM% were independent risk factors for early perforation of the appendix in patients with AA. Subsequently, further ROC curve analyses revealed that the NLR was of the highest predictive value for appendiceal perforation in patients with AA. With a diagnostic cut-off value of 10.83, the sensitivity and specificity were 0.963 and 0.850, respectively. Kelly et al. reviewed 663 patients over a 4-year period and found that NLR >6.35 or CRP >55.6 mg/L could be used as the diagnostic cut-off value for grading the severity of the disease in patients with AA and that the hospitalization time was longer in patients with a high NLR. 19 Mori et al. found that high NLR was an independent risk factor for increased complications after appendectomy. 20 Yardimci et alfound that the mean NLR values of simple AA, AA combined with restrictive peritonitis, and complicated AA were 8.36 ± 5.6, 9.1 ± 6.2, and 10.6 ± 6.4, respectively, suggesting that the NLR could be used as a parameter for grading the severity of disease in patients with AA. 21 In addition to NLR, lymphocyte-to-monocyte ratio (LMR) has also been found to be useful in assessing the severity of AA patients. 22
The results of our study combined with the results reported in literature suggest that, as an emerging inflammatory index, NLR can reflect the degree of lymphocyte demobilization and neutrophil activation in the inflammatory state at an early stage. It is similar to or better than the traditional biomarkers, such as CRP and PCT, and can be helpful for grading the severity of the disease.
Although images such as ultrasound, CT and MRI are almost always used in acute appendicitis in developed countries, NLR is an accurate and low-cost marker in selected populations and settings. For example, NLR can be used in underserved areas where immediate access to image studies is limited or in pregnant patients where the use of CT scan is contraindicated. Image remains gold standard for diagnosis of appendiceal perforation preoperatively. However, no image can predict future perforation. 9 This study demonstrated that NLR has the potential to predict perforation in the cases with clinically or radiologically confirmed uncomplicated appendicitis. It can be used to triage patients and aid in decision making for surgical versus conservative management; patients with higher NLR can be operated earlier while patients with lower NLR can start with conservative therapy. NLR may also be used to monitor treatment response for patients on conservative management.
However, the present study has limitations. It is a retrospective observational study with small sample size in a single-center and the selection criteria are relatively strict. Our future study will include patients with longer duration of illness, use of antibiotics, and chronic appendicitis. We plan to also conduct a prospective study to use NLR as one of the criteria to guide management plan. A larger prospective and multicenter study is our future direction.
Conclusion
NLR derived from simple routine blood tests is closely associated with early appendiceal perforation in patients with AA. It is very simple to obtain the results and does not add extra burden to patients. High NLR is an independent risk factor for early appendiceal perforation and has a higher diagnostic value than that of the traditional inflammatory markers. Implementing the use of NLR in emergency room is promising and recommended.
Footnotes
Author contributions
Chen Q, Bao JF, and Chen F contributed equally to this work; Chen L and Zhu T designed the research study; Chen Q, Bao JF, and Chen F performed the research; Chen L, Zhu T, Chen Q, Zhu T, Ding J and Bao JF analyzed the data and wrote the manuscript; All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
The data that support the findings of this study are available on request from the corresponding author.