
Abstract
Neutrophils are known to play a role in airway inflammation and are activated in inflammatory lung diseases such as asthma. In adult studies the neutrophil/lymphocyte ratio (NLR) was found to be a possible biomarker for both airway and systemic inflammation. However, there is a limited understanding regarding NLR in the pediatric age group. To assess NLR as a biomarker for inflammation in pediatric asthma, 54 children admitted to hospital with exacerbation of asthma between March and October 2013 were enrolled into our study. Complete blood counts were obtained during both exacerbation and an asymptomatic period covering at least 3 months after exacerbation. NLRs of the study group during both exacerbation and the asymptomatic period were compared and these two datasets were then compared with the control group. The study group comprised 27 boys (50%) and 27 girls (50%) with a mean age of 120 ± 36 months. Of the total number of patients, 3.7% had mild, 94.4% had moderate, and 1.9% had severe exacerbation of asthma. The NLRs of the study group were found to be significantly higher during exacerbation compared with both the asymptomatic period and the control group (P = 0.017, P = 0.003). Our study suggests that NLR may be effective and usable measurable biomarker for determining inflammation in cases of pediatric asthma during acute exacerbation period. However, a broad analysis of dependent and independent variables in further prospective studies, is still required.
Introduction
Asthma is the most common chronic inflammatory disease of the airways in the pediatric population. Chronic inflammation caused by mediators released from mast cells, eosinophils, neutrophils, macrophages, lymphocytes, and some other cells has been detected in the airways of asthmatic children. 1 Recent studies have demonstrated that neutrophilic inflammation is related to an increase in the severity of the disease. 2 In addition, the existence of eosinophilic inflammation in asthma has been shown to be related to atopy and symptoms of persistent asthma. 3 A definition of the similar biological indicators that play a role in inflammation in asthma is important since this will open the gate for further developments in diagnosis and treatment. During childhood asthma, in particular, special non-invasive asthma indicators for monitoring and follow-up are of great importance because existing diagnostic techniques cannot be used properly due to their invasiveness or the need for cooperation. Commonly used spirometric measurements require effective cooperation, whereas bronchoalveolar lavage (BAL) is invasive. 4 Therefore, there is a need for non-invasive methods that can be used to monitor asthma. Chronic inflammation is also present in asthma. Cytokines in the pathogenesis of asthma cause an increase in neutrophils, as noted above.1,2 Based on this information, we consider that the NLR is increased in asthmatics. However, our knowledge regarding NLR in asthmatic patients is incomplete.5,6 Although a previous study in adults revealed no relationship between asthma and NLR, 5 NLR was found to be associated with neutrophilic asthma in the second study. 6
In our study, we investigated NLR in asthma patients during exacerbation of asthma and also when their asthma was under control for a period of least 3 months after exacerbation. We compared these results with NLR values from healthy children to assess whether NLR may be used as a biomarker for inflammation in asthma.
Materials and methods
Between March and October 2013, children who were admitted to the Pediatric Allergy Department of Dr Bechet Uz Children’s Research and Training Hospital, Izmir, Turkey were enrolled in our study. We obtained a complete blood count (CBC) for each patient during exacerbation and again at least 3 months after the asthma was shown to be under control according to an Asthma Control Test (ACT). 1 The diagnosis, classification, and classification of exacerbation severity were all performed using the Global Strategy for Asthma Management and Prevention guidelines developed by the Global Initiative for Asthma (GINA). 1 Ninety-four healthy children, who were referred to our hospital during the same time period for a general medical examination, were chosen to be the control group. These subjects had no signs of infection or history of chronic/allergic disease. The CBC values of the study group were compared with the controls. We also investigated the relationships of overall asthma severity, severity of asthma exacerbations, and number of annual exacerbations, pulmonary function, and C-reactive protein (CRP) levels with inflammation. Patients were excluded from the study if their asthma remained exacerbated; they had received systemic steroids within the last month, experienced acute/chronic infection, or had any other systemic disease such as hepatic, renal, or cardiovascular diseases, diabetes mellitus, cancer, sepsis, or systemic inflammatory disorders. This study was approved by the local ethics committee of our hospital (2015/02-05). Informed consents were given by the family of the children.
Statistical analyses
Statistical Package for Social Sciences (SPSS for Windows 15.0, Chicago, IL, USA) program was used to analyze the data. Results were given as either mean ± standard deviation (SD) or median (min–max) according to the distribution. The Chi-squared test was used to compare grouped data. The paired t-test was used to compare group-specific measurements, and the independent Student’s t-test to compare measurements among independent groups. Kruskal–Wallis test and Mann–Whitney U tests were used for non-normally distributed variables. Pearson’s correlation analysis was used to explore correlations between the measurements. P values <0.05 were considered statistically significant.
Results
The study group consisted of 54 children with asthma, while the control group consisted of 94 healthy children with a similar age and gender distribution. The study group comprised 27 boys (50%) and 27 girls (50%) with a mean age of 120 ± 36 months. The median age on hospital admission was 75 ± 37 months (range, 12–168 months) and the median age at the onset of symptoms was 40 ± 39 months (range, 1–144 months). Cases were classified according to the severity of asthma, as follows: mild intermittent (1.9%), mild persistent (33.3%), moderate persistent (61.1%), and severe persistent (3.7%). Of the total number of patients, 3.7% had mild, 94.4% had moderate, and 1.9% had severe exacerbation of asthma. The medians of the eosinophil count and immunoglobulin E (IgE) levels were 300/ mm3 and 355 IU/mL, respectively. According to skin tests, 35 (64.8%) of the patients were atopic and 19 (35.2%) were non-atopic. The mean age and gender ratio were similar between the control and study groups (P = 0.71, P = 0.901). The NLR was calculated to be 4.9 ± 8.1 during the exacerbation period and 2.4 ± 0.3 during the asymptomatic period. The ratio in the control group was calculated as 1.5 ± 1.2. The NLR was significantly higher during the period of exacerbation compared with both the asymptomatic period and the control group (P = 0.017, P = 0.003). On the other hand, the NLR during the asymptomatic period was not significantly different compared with the control group (P = 0.08) (Table 1). No significant correlation was identified between the NLR and overall asthma severity, severity of asthma exacerbation, number of annual asthma exacerbations, respiratory function test, or CRP value (P >0.05).
Comparison of the study group’s CBC values obtained both during exacerbation and the asymptomatic period with those of the control group.
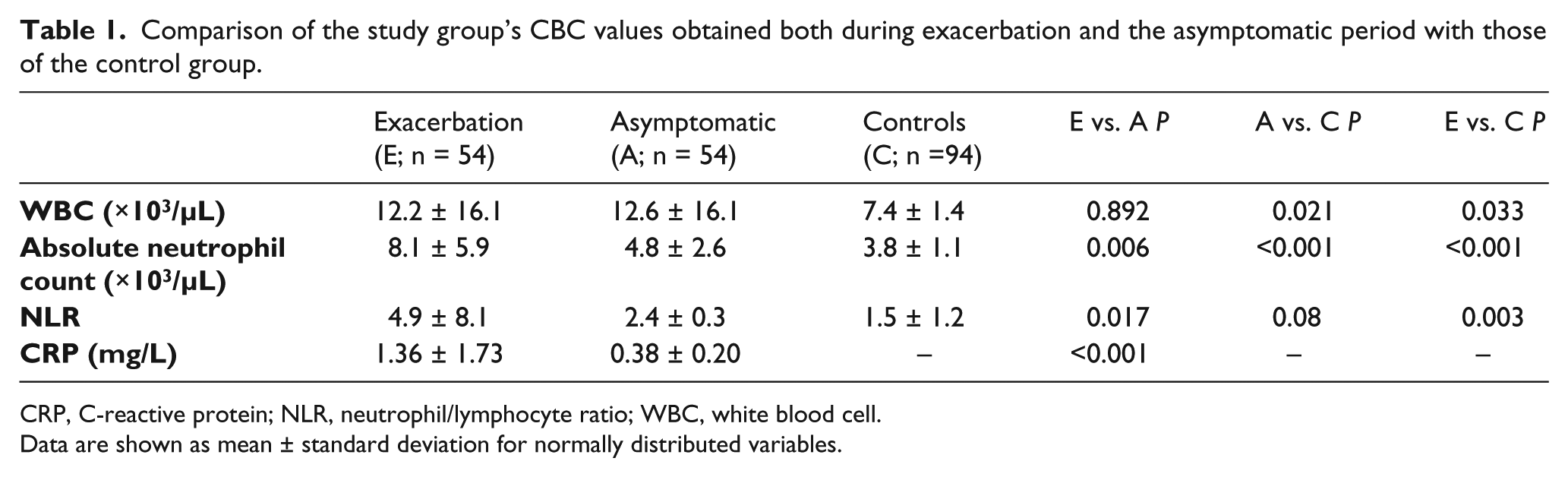
CRP, C-reactive protein; NLR, neutrophil/lymphocyte ratio; WBC, white blood cell.
Data are shown as mean ± standard deviation for normally distributed variables.
We investigated the potential of NLR as a biomarker for inflammation in asthma and found that leukocyte count, absolute neutrophil count, and NLR correlated with inflammation in asthma. However, only NLR or absolute neutrophil count are feasible as biomarkers for showing the inflammation during acute exacerbation of asthma. Previous studies focusing on NLR have found that the level of inflammatory response in various inflammatory pulmonary diseases due to harmful particles infiltrating the lungs leads to many other effects such as systemic oxidative stress, activation of circulating inflammatory cells, increased plasma cytokines and acute phase reactants, weight loss, and skeletal muscle dysfunction.7–11 Studies in adult chronic obstructive pulmonary disease (COPD) patients have demonstrated that plasma CRP levels and leukocyte counts are both significantly higher during acute exacerbation of COPD.7,8 Drews et al. 9 observed a high ratio of neutrophils in the sputum of children with non-atopic asthma, whereas eosinophils were found to be most abundant in the sputum of children with atopic asthma. Zhang et al. 6 compared blood count neutrophil and eosinophil ratios in sputum cytology. They found that NLR was high in patients with neutrophilic asthma. In addition, Fu et al. 10 studied 50 adult asthma patients and found that patients with detected systemic inflammation exhibited an increased sputum neutrophil count. In our study, in agreement with the literature, we found that leukocyte count, absolute neutrophil count, NLR, and CRP were significantly higher compared to the control group during acute asthma exacerbation. For this reason, we consider that NLR may be effective and usable biomarker for determining systemic inflammation during exacerbation period in cases of asthma.
No statistically significant correlation has yet been identified between NLR and overall asthma severity, severity of asthma exacerbations, number of annual exacerbations, pulmonary function tests, or CRP values. However, Furukawa et al. 12 found that asthmatic children have increased sputum neutrophil counts, and identified a small but positive correlation between NLR and hospital admission. Günay et al. 13 found that stable COPD patients had a higher NLR compared to the control group in their study of 269 adult patients, and found a positive relation between CRP and NLR.
Our study had some limitations. First, we used a small study population. Second, we were not able to examine sputum cytology or the correlation between NLR and other systemic or airway inflammatory marker, which have been shown in previous studies to act in systemic inflammation.
This study is one of a small number of studies to investigate NLR in pediatric asthma patients. Our study suggests that NLR may be effective and usable biomarker for determining systemic inflammation in pediatric asthma cases during acute exacerbation period. However, a broad analysis of dependent and independent variables in further prospective studies is still required.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.