
Abstract
Background
Elderly people frequently experience a decline in hand function, due to ageing or diseases. This leads to decreased independence in activities of daily living (ADL). Assistive technology may enhance independence.
Objectives
The objective of this paper was to explore user acceptance of an affordable wearable soft-robotic glove (ironHand (iH) system), that supports grip and hand opening in ADL. In addition, functional performance with the iH system was explored.
Methods
For this study 28 elderly people used the iH system across two sessions. During these sessions, participants performed six functional tasks with and without the iH system. Outcome measures were System Usability Scale (SUS), Intrinsic Motivation Inventory (IMI) and performance time of the functional tasks.
Results
User acceptance scored highly, with a mean SUS score of at least 63.4 (SD = 19.0) and a mean IMI score of 5.1 points (SD = 0.97 points). Functional task performance improved across repetitions both with and without the glove (p ≤ 0.017), but all functional tasks were performed faster without the glove (p ≤ 0.032).
Conclusion
Participants perceived the iH system as useful, pleasant and meaningful. The learning curve in functional performance time (improvements across repetitions) is promising, since it suggests there is room for improved performance when a longer acquaintance period is applied.
Keywords
Introduction
Hand function often declines with ageing, or due to acute (e.g. stroke) or chronic (e.g. arthritis) diseases.1–3 This results in a decreased ability to grip and manipulate objects. 4 In addition, people with reduced hand function can experience decreased functional performance,5–7 decreased independence in activities of daily living (ADL) and decreased quality of life.8–11
Assistive technology has the potential to improve hand function and independence in daily life. Many different devices are available to assist with or improve hand function. 12 However, most current devices are only used in rehabilitation centres or hospitals because such devices are very expensive, not easy to use (therapist supervision is needed in most cases) and too bulky to use during functional tasks.12–14
Therefore, an easy-to-use and wearable soft-robotic device for the impaired hand of elderly people and patients is being developed in the ongoing ironHand (iH) project. The iH system integrates an assistive system that can support grip strength and hand opening in ADL directly, with a digital training platform to provide specific exercises for the hand at home. The combination of the assistive functionality and therapeutic functionality of the iH system enables hand support during a large variety of functional activities and specific hand training exercises at home.
In order to improve adoption by users, a user-centred process was applied in the development process. As part of this, end-users identified user requirements for the iH concept in an early stage of the project. User-friendly design and ergonomics were identified as major requirements. 15 This study provided the first insight in feasibility, in terms of user acceptance (usability and motivation) and impact on functional task performance, of the assistive functionality of the iH system.
Methods
ironHand system
The iH system (Figure 1) is based on the concept of a soft-robotic glove that can add extra strength to grip for persons with reduced hand function. The glove is portable and can be used to assist the grip during a wide range of ADL (assistive mode of the iH system: iH Assistive System (AS)). In addition, the same glove can be connected to a computer with specialized therapeutic software that allows users to train specific aspects of function such as strength, finger coordination, finger independence or motor memory in a motivating game-like environment (therapeutic mode of the iH system: iH Therapeutic System (TS)).
The ironHand system.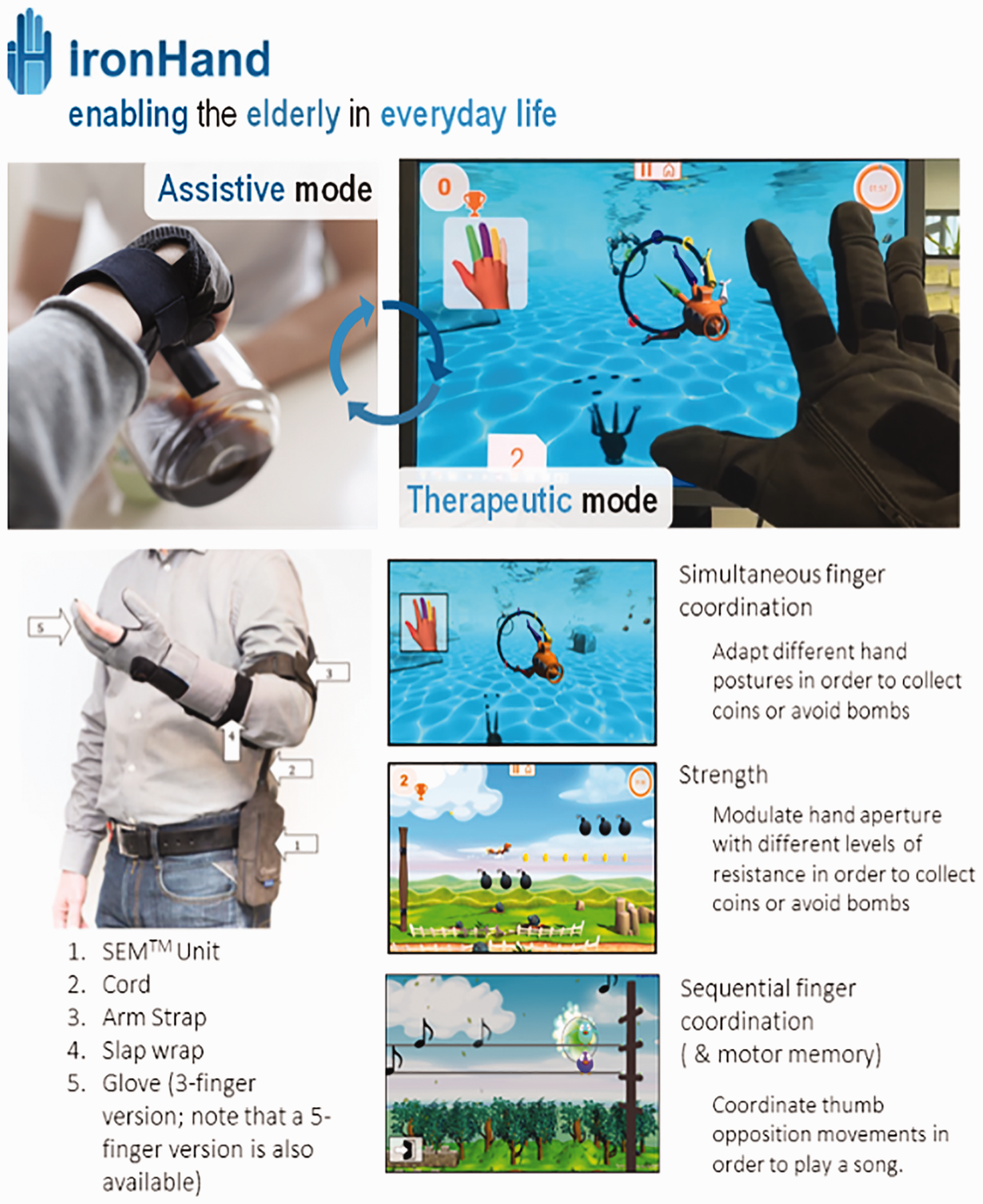
The iH system provides assistive flexion force to the thumb, middle finger and ring finger through a tendon-driven mechanism. The tendon-driven mechanism allows the system to provide active assistance in flexion force. In addition, passive leaf springs (attached to the dorsal side of the glove) are used to support extension of the thumb, middle finger and ring finger. To modulate flexion assistance, the system incorporates pressure sensors (Interlink Electronics) in the finger tips and extension/flexion sensors (Flexpoint) along the fingers. An intention detection logic ensures that the assistive flexion force is only activated in a natural and intuitive way. In addition, the actuators provide support in proportion to the flexion force applied by the user. This ensures that the user maintains an active contribution to the specific movement. The sensitivity level, maximum supported force in flexion and extension (regulated by the amount of leaf springs) of the iH system are customized for the individual user.
Participants
Four sites, National Foundation for the Elderly (NFE), Bunnik and Roessingh Research and Development (RRD), Enschede in the Netherlands, Eskilstuna Kommun Vård- och omsorgsförvaltningen (ESK), Eskilstuna in Sweden and terzStiftung (TERZ), Berlingen in Switzerland, recruited 30 elderly people (≥55 years) who experienced a decline in hand function resulting in difficulties in performing ADL.
Additional inclusion criteria for those participants were: (1) at least 10 degrees of active flexion and extension movement of the fingers; (2) sufficient cognitive status to understand two-step instructions; (3) (corrected to) normal vision; (4) living at home; (5) and signed written informed consent prior to the start of the study.
Exclusion criteria were: (1) severe sensory problems of the hand; (2) severe acute pain of the hand; (3) wounds on their hands that may create problems when wearing the glove; (4) severe contractures limiting passive range of motion; (5) co-morbidities limiting functional use of the arms/hands; (6) insufficient knowledge of the Dutch, Swedish or German language to understand the purpose or methods of the study; (7) and participation in other studies that can affect functional performance of upper limb.
The local Medical Ethical Committees in the Netherlands, Sweden and Switzerland approved the protocol of this feasibility study.
Procedure
Study design
This study was a multicentre cross-sectional study in which the feasibility of the iH AS was tested. Participants performed ADL-like tests in a standardized, simulated ADL environment at NFE, ESK and TERZ supervised by the researchers of NFE, ESK and TERZ, on two separate days (with a minimum of two weekdays between those sessions). Using the iH system for the first time (naive use) was tested on day 1 and a repeated session on day 2 was used to test more experienced use after some repetitions with the iH system. The tests were coordinated and monitored to assure consistent execution across sites by RRD and at each site was supervised by the same researchers.
Experimental protocol
The first evaluation session started with collecting participant characteristics such as age, gender, dominant hand and most-affected hand. At the beginning of both sessions, the amount of support of the iH AS was adjusted to the participants’ needs and experienced comfort. Furthermore, researchers provided the participants with additional information to use the iH system properly. The glove was always worn on the most-affected hand.
Explanation functional tasks.
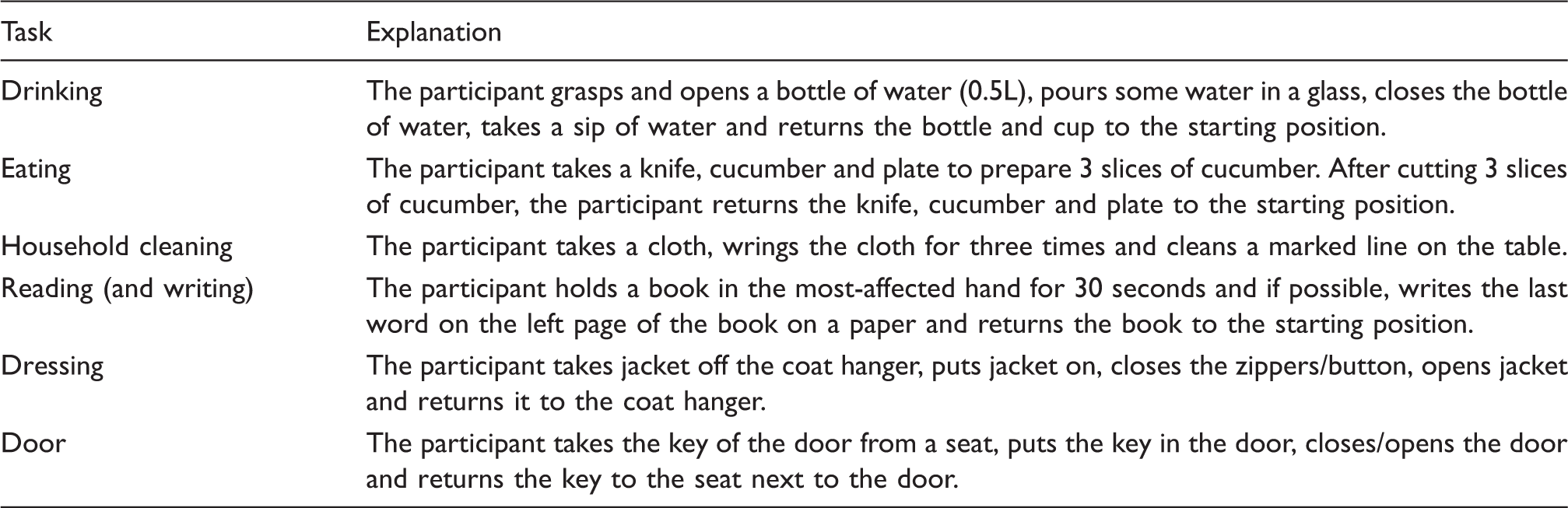
Participants performed each functional task three times with and three times without the iH AS. Sealed envelopes were used to randomize the order of glove use during each session for each individual.
Assessment
User acceptance
After the tasks were done both with and without the glove in both evaluation sessions, participants completed the System Usability Scale (SUS) and the Intrinsic Motivation Inventory (IMI) to assess system usability and participants’ motivation during use of the iH system.
The SUS is a 10-item scale giving a global subjective view on system usability. Participants scored each item of the SUS on a 5-point Likert scale ranging from ‘strongly disagree’ to ‘strongly agree’. Scores were translated to a total score between 0 and 100. 16 The system has a good probability of acceptance in daily life of potential users if the system receives a total score above 70. A total score between 50 and 70 is promising, but guarantees no high acceptability in the field, and a total score below 50 indicates a high risk of usability difficulties with the system in the field.17,18
The IMI is a questionnaire which measures several dimensions (interest/enjoyment‚ perceived competence‚ effort‚ perceived choice while performing a given activity, felt pressure and tension and value/usefulness) of motivation that patients experience during the performance of a physical activity. 19 For the purpose of this study, ‘activity’ was replaced by ‘using the iH system’ in each item. To capture the concept of motivation when using a new device in the most solid way, the IMI was evaluated only at the end of evaluation session 2. The 34 items are scored on a 7-point Likert scale ranging from ‘not at all true’ to ‘very true’. 19 The level of motivation is higher if the averaged total score on the IMI is closer to 7.
Functional task performance
During the functional tasks, researchers measured the performance time using a stopwatch, observed the execution of the activities (e.g. which hand is used for handling the heavier objects or performing the most difficult movements, speed of movement, fluidity, precision, presence of compensatory movements) and observed the way the participants reacted to the system. This was used to further improve the design of the iH system in next iterations of its development.
From the three repetitions, only the last repetition was used to compare the performance time between the conditions with and without iH AS for each task. In addition, changes over the three repetitions within each evaluation session were assessed to obtain insight in how well participants got acquainted to using the system.
Data analysis
IBM SPSS Statistics version 23.0 for Windows was used to analyse the data. The assumption of normality for the SUS scores and the performance duration of the functional tasks was checked by visual inspection of the q–q plot, the box plot, histogram plot and the Shapiro–Wilks test, prior to the statistical analysis. All outcome measures were described by using descriptive statistics.
A Wilcoxon signed rank test or a paired sample t-test was performed, depending on normal distribution of the outcome measures, to compare the SUS scores for the iH AS between both days and the performance times of the third repetition between both conditions with and without iH AS for each task. In addition, repeated measures analysis of variance (ANOVA) or the Friedman test (the non-parametric variant) was used to compare the performance times between multiple repetitions with and without the iH AS. If a significant difference was found for parametric variables, multiple comparisons were performed with a Bonferroni correction. A Wilcoxon signed rank test for multiple comparisons was performed using an adjusted p-value of 0.017, if a significant difference was found for non-parametric variables.
The level of significance was set at α ≤ 0.05 for all statistical tests.
Results
Characteristics of participants at baseline.

Mean ± standard deviation (range)
User acceptance
SUS
Twenty-seven participants completed the SUS for the iH AS after session 1. One participant missed some values resulting in an incomplete SUS. The mean SUS score was 70.1 (SD = 14.1).
A subset of the participants (data only available from 17 participants of NFE and ESK) completed the SUS for the iH AS after session 2 as well (see Figure 2). The SUS score after session 2 was not different (p = 0.073) compared with session 1, with a mean of 63.4 (SD = 19.0).
Individual System Usability Scale scores for the iH AS after evaluation session 1 and 2.
IMI
The scores for each dimension of the IMI were positively rated by all participants (n = 28), resulting in a mean score on the IMI of 5.1 points (SD = 0.97 points) out of 7 points (see Figure 3).
Individual Intrinsic Motivation Inventory scores after evaluation session 2.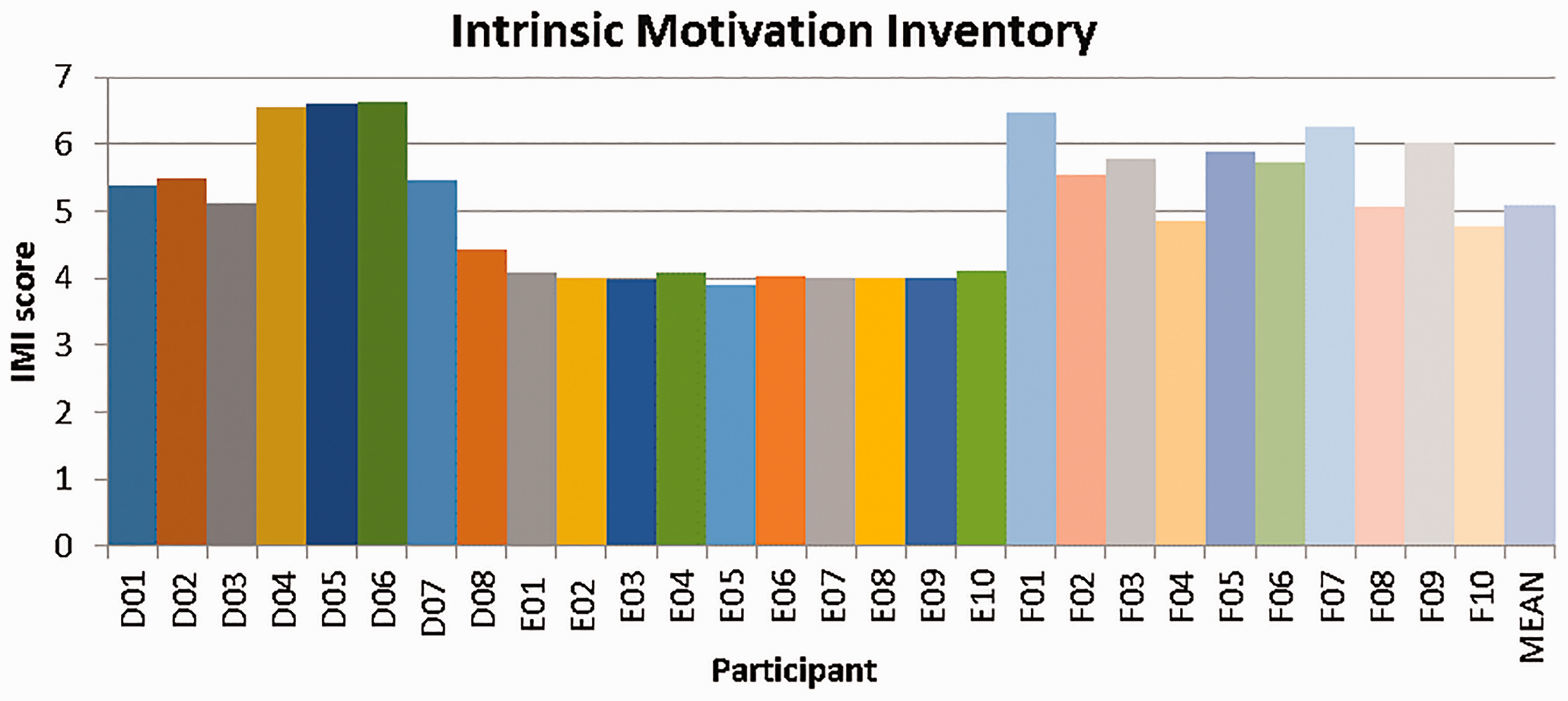
Functional task performance test
During both evaluation sessions, participants had difficulties with performing the dressing task due to the iH system not being slender enough to wear underneath a jacket. Therefore, the dressing task was excluded from statistical analyses. Furthermore, data of the reading task were missing for one participant, data of the door task of session 1 were missing for two participants and data of the door task of session 2 were missing for one participant due to erroneous reporting of the data values and unintentional omission of some values from the scoring sheet.
During session 1, the last repetition of all functional tasks was performed faster without the glove (p ≤ 0.032) than with the glove. Additional analysis of the NFE and ESK participants showed that the performance time improved over the three repeated attempts either with or without the glove (p ≤ 0.017), except for the reading and household tasks without the glove (see Figure 4).
Performance time functional tasks evaluation session 1.
Data of the functional performance times of the NFE and ESK participants of session 2 showed that all functional tasks were again performed faster without the glove (p ≤ 0.007) than with the glove. In addition, participants showed improvements in performance time over the three attempts only with the glove during the drinking and eating tasks (p ≤ 0.003) (see Figure 5). Furthermore, Figures 4 and 5 show that the first attempt of the functional tasks was performed faster in session 2 compared with session 1, supporting the observation of a learning curve between session 1 and 2.
Performance time functional tasks evaluation session 2.
In addition to the data of the functional performance test, participants reported that their performance with the iH AS improved after using the system for a longer time period. They also indicated that they felt the support of the iH AS during the functional tasks. On the other hand, researchers observed that participants experienced some usability issues when using the iH AS. They especially encountered difficulties with grasping the cap of the bottle, opening and closing the bottle, writing, grabbing the plate, grasping the pen and picking up the key.
Discussion
The present feasibility tests focused on user acceptance. The results showed that the concept of the iH system was well accepted by the majority of the participants, as reflected by the positive SUS and IMI scores. However, all functional tasks were performed significantly faster without the glove, even after repeated use of the glove across two sessions. The results of functional task performance within both sessions showed that performance either with or without the glove improved during three repetitions. Although improvements across three repetitions were less predominant during session 2, performance with the glove of the drinking and eating tasks still improved across repetitions.
This feasibility study, a first stage of user testing, focused on user acceptance including ease of use, usability and motivation, since these are early-stage tests during the ongoing iterative development process of the iH system. As described by the framework of DeChant et al., 20 it is important that the evaluation suits the stage of the development process. Subsequent stages of user testing should focus increasingly on the effect of the iH system after a longer period of use and a larger maturity of the technology.
Participants reported that they appreciated the main components of the iH AS prototype: the support of grip strength and hand opening during ADL. This is confirmed by the positive SUS and IMI scores. The mean SUS scores of 70.1 and 63.4 for the iH AS indicate good probability for acceptance of the iH AS in the field.17,18 Although not significant, this slight change might indicate higher expectations in terms of usability when using the system for a second time. Studies that investigated system usability of other types of technology showed similar or higher SUS scores.21-23 The study of Nijenhuis et al. 22 also investigated the actual use of a robotic hand device for training purposes at home by stroke patients. This study showed that stroke patients, who had SUS scores comparable with the participants of this study, were able to independently use such training device at home for on average 15 min/day over 6 weeks.
Participants also scored positive on the IMI with a mean score of 5.1, indicating that participants perceived the iH system as an interesting, pleasant and enjoyable system to improve their hand function in daily life. Comparable IMI scores were found by other studies that investigated motivation of an intervention with rehabilitation technology in a clinical setting.24,25 Nijenhuis et al. 25 showed that user acceptance of such technology appears to be equal with independent practice with conventional exercises at home. This suggests that the chances for actual use and adoption of the iH system in daily life are promising.
Functional task performance duration without the current prototype was better compared with task performance with the glove, despite the positive reactions of participants on usability and motivation. The slower performance times with the iH AS have probably been affected by several usability issues. This may have hindered participants’ ability to experience the full potential of the iH AS. For instance, participants experienced less sensation of the fingertips during the performance of functional tasks with the glove due to the fabric of the glove. In addition, the position of the sensors was not always optimal, and sometimes participants had difficulties in obtaining a good grip on an object due to a reduced friction between the object and the surface of the glove.
Furthermore, the participating elderly performed the functional tasks with the glove worn on the hand they perceived as most affected, which was, in most cases, their dominant hand. This might have caused difficulties with performing fine motoric functional tasks, because these activities are difficult to support with a robotic glove. Therefore, it is important to focus on the gross motor activities. Indeed, many participants mentioned that they liked the assistive function of the iH system during gross motor activities such as lifting and opening a bottle, holding a book, cutting food and turning a key. In other populations, for example stroke patients, the most-affected hand is mainly used to support the healthy hand instead of using the most-affected hand as primary hand to perform functional tasks. 26 Therefore, the role of the gloved, more affected hand in (bi-manual) functional tasks should be taken into account more specifically in subsequent studies with elderly participants. In addition, it is also important to take into account the content of the functional tasks. The selected functional tasks were probably too easy to perform for the current sample of participants. Ultimately, this can result in reduced performance with the iH AS because the glove is sometimes more obstructive than helpful.
In addition, participants have used the iH AS actively only for approximately 20 minutes during the functional task performance test in both sessions to assess feasibility and usability. The learning curves of both sessions with and without the glove show that participants can improve their performance after multiple repetitions. Figures 4 and 5 show that, in general, the first repetition in session 2 was faster than that in session 1. This indicates that participants learned to perform the task rather quickly with and without the glove. On one hand this implies that the glove is easy to use; on the other hand, that a learning curve in glove use is still present during some of the functional tasks. 27 Therefore, in future studies a longer acquaintance period with the iH system should be applied to examine if more progression in performance is possible.
Since soft-robotics to assist upper extremity function is a very young field of research, only one other comparable study was found. The present findings are in line with the study of Polygerinos et al., 28 which showed that a healthy subject completed functional tasks of the Jebsen–Taylor Hand Function Test slower with assistance from a soft-robotic glove as compared with performing those tasks without assistance from a glove. Their conclusion was that such an assistive system might make a difference when participants need to perform multiple functional tasks in a row and are losing handgrip strength during prolonged activity. 28
Conclusion
The current feasibility study showed that participants with a perceived decline in hand function were positive about the usability of the assistive functionality of the iH system. However, the participants performed functional tasks faster without the soft-robotic glove than with the glove. The participants especially appreciated support of the iH AS during gross motor activities. The performance time of the functional tasks was improved after multiple attempts with the iH AS. Therefore, a longer time to get used to new assistive technology may be needed to further improve performance with the iH system. Furthermore, design adaptations are needed to improve performance with the iH system, based on the user input collected during this study. In future studies, a new version of the iH AS will be tested in daily life situations. Additionally, the iH TS will be evaluated as well.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is partly funded by the Active and Assisted Living joint programme (grant AAL-2013-6-134) via ZonMw (the Netherlands), Vinnova (Sweden) and the State Secretariat for Education, Research and Innovation (Switzerland).