
Abstract
Journey mapping, a participatory arts-based research method, is used to explore experiences, connections and influences by creating graphical depictions that include both time and emotional response dimensions. In health and social sciences research, use of journey mapping can be valuable for participants, researchers, health and social care professionals, and the public. It has been used to explore patient journeys through healthcare systems and student journeys through education. While several researchers have shared their journey mapping instructions, scholars have identified a lack of standardized guidelines and methods for journey mapping in health and social sciences research and reporting. In this article, we introduce a new methodological framework,
Keywords
Introduction
Journey mapping, adapted from marketing and consumer service (Gibbons, 2018) explores experiences over time via various facets of a process (Sperano et al., 2019). However, journey mapping is still an emerging field in health and social sciences research, and thus scholars have identified the need for consistency and standardization with respect to methods, guidelines, and reporting for journey mapping (Cormick et al., 2024; Davies et al., 2023; Joseph et al., 2020). With the increasing use of arts-based activities such as journey mapping within qualitative research, the lack shared guidelines risks inconsistent reporting and limited methodological transparency. Guidelines are needed to support reflexive and context-sensitive use of journey mapping, which can strengthen qualitative rigor while preserving flexibility in methodological and analytic approach. There is particular value in providing opportunities for participants to generate their own journey maps as it encourages self-expression, while avoiding inadvertent transfer of researcher influence or bias in interpreting participant experiences and their intent behind the meanings and messages related to their journey map (Pauwels, 2015). To address this gap we have developed and present “Journey Mapping in Applied Public Health & Social Sciences (J-MAPHS)”, a methodological framework for participant-generated journey mapping in health and social sciences research. Importantly, the J-MAPHS framework is anchored in and built on frameworks that prioritize co-design, patient engagement, and trauma-informed practices. Incorporating these principles differentiates J-MAPHS from regular journey mapping methods that do not address the unique complexities found in public health and social science research.
Background
Arts-Based Methods
Arts-based methodologies/methods (ABM) are used in health and social sciences research as a research tool and stand-alone method to enhance knowledge production and knowledge mobilization to diverse audiences and stakeholders (Boydell, Gladstone, et al., 2012; Fraser & al Sayah, 2011; Moretti et al., 2025; Nathan et al., 2023). ABM are situated within participatory and collaborative social sciences research (Fraser & al Sayah, 2011; Pauwels, 2015) such as participatory action research (PAR). The PAR approach brings together researchers, community members, and others to co-create knowledge and social change to produce new insights and improve the lives and communities of participants. ABM harmonizes well with PAR as both aim to empower participants through involving them as active partners, keeping their voices, experiences, and perspectives central to the research, and fostering a sense of ownership and agency (Chevalier & Buckles, 2019; Kindon et al., 2007; Liebenberg et al., 2020).
The art products emerging from ABM initiatives serve to assist health professionals, the public, and other key partners in learning and understanding art-makers’ lived experiences, and raising awareness of their issues and challenges (Fraser & al Sayah, 2011; Gillibrand et al., 2023), enabling messaging that can elicit empathy, which can lead to social change (Cohen Miller, 2017; Flicker et al., 2013; Fraser & al Sayah, 2011; Woodgate et al., 2017).
Involving participants in self-expression via various art forms, such as drawing, dance, photography, photovoice, poetry, body maps, and theatre, allows for engagement of the whole person bringing meaning-making to the fore within data collection (D'Amico et al., 2016; Leavy, 2020; Murray et al., 2023; Nathan et al., 2023; Woodgate, Isaak, et al., 2024; Woodgate et al., 2020; Woodgate et al., 2016). In this way participatory arts-based research allows participants more control and agency over data generation (Maman et al., 2020), the freedom to determine what they wish to share (Hickey-Moody et al., 2021), along with a greater role in how results are interpreted and disseminated to various stakeholders (Gubrium & Harper, 2013).
The use of creative processes in ABM also facilitates the discovery of non-quantifiable experiences pertaining to life’s social, emotional and relational facets in an inclusive and co-created environment (Chilton & Scotti, 2014; Leavy, 2020; Moretti et al., 2025). This ensures that research remains “responsive to participants’ own meanings and associations” (Bagnoli, 2009, p. 547). Additionally, ABM assist in fostering self-awareness and insight, and facilitate recovery and healing through voicing individuals’ stories in different ways (Bagnoli, 2009; Coholic et al., 2020; Cole et al., 2018; Hidalgo-Padilla et al., 2022; Macpherson et al., 2016; Shukla et al., 2022). Serving as a universal communication tool that can be culturally inclusive, ABM can address complex, layered issues and facilitate self-expression when experiences cannot be described by words alone (Flicker et al., 2013; Gauntlett, 2007). These attributes lend the use of ABM to research with children, young people, and equity-deserving groups (Coholic et al., 2020; Cole et al., 2018; Hidalgo-Padilla et al., 2022; Murray et al., 2023). For example, among children with cancer, the use of a drawing tool “was found to be particularly beneficial in assisting children to express existential challenges that they had previously been unable to articulate in words” (Woodgate et al., 2014, p. 149).
A key tenet of participatory arts-based methods is that they offer accessibility of expression for participants as well as a safe way to share emotions and experiences particularly for topics such as personal health and wellness or for members of vulnerable groups who may have experienced trauma (Alessi & Kahn, 2023). Yet use of ABM with these populations can present additional dilemmas (Fraser & al Sayah, 2011). Considering this, researchers are beginning to address some of these research challenges of ABM including ethical praxis, co-production, and representation. They point out that careful consideration of the ethical processes of informed consent, confidentiality and anonymity is even more critical in arts-based research, given that participant-produced art pieces are a component of the findings presented, including separate participant consents for inclusion of quotes and art pieces with the option of anonymity or credit for their art (Boydell, Gladstone, et al., 2012; Flicker & MacEntee, 2020; Gubrium et al., 2014; Switzer, 2018). Switzer and colleagues also note the added ethical complexity when conducting arts-based research in online community-engaged environments identifying relationality and care, accountability and transparency, and equitable access as key (Switzer et al., 2024).
An aim of ABM is to develop an equal researcher-participant relationship where art products co-produced and the interpretation of them are owned by the participant (Flicker et al., 2014; Huss, 2005). Yet these co-relationships can become complicated due to socio-structural issues (e.g. racism, stigma), which may impact inclusion and accessibility (Switzer et al., 2018), power dynamics (Switzer & Flicker, 2021) and structured versus flexible ways that researchers may work with participants and communities (Boydell et al., 2016).
Researchers have also highlighted the challenge of balancing participant agency in representation while also doing no harm (Boydell, Volpe, et al., 2012). Several point out that truth in representation and interpretation of images is paramount to ensure inadvertent stigmatization, stereotyping or misinterpretation of intended messages of arts-based products by various audiences including researchers (Boydell, Volpe, et al., 2012; Switzer, 2018, 2019).
Journey Maps
Journey mapping, an example of participatory ABM, incorporates principles of participatory action research, integrated knowledge mobilization (iKM), and visual methodologies in social sciences through collaborative, participant-focused co-production of art products using visual methodologies to interpret and understand the maps, and generate discussion and new knowledge (Chevalier & Buckles, 2019; Glaw et al., 2017; Kothari et al., 2025; Pauwels, 2015). Rooted in human-centred design (Annamma, 2023; Stickdorn & Schneider, 2010), journey maps are graphical depictions of individual or organizational lived experience that include both time and emotional response dimensions to create visual narratives (Gibbons, 2018; Joseph et al., 2020; Kalbach, 2016). Journey maps explore meaningful experiences, connections and influences over time, documenting diverse and complex social realities using an integrated visual and text-based approach (Bagnoli, 2009; Govender et al., 2024; Guillemin, 2004; Nielsen & Bruselius-Jensen, 2021; Pauwels, 2015). Common elements of journey maps include touchpoints, transitions, turning points or milestones at pre-, during- and post-event/experience periods (Rosenbaum et al., 2017).
Use of journey mapping can be valuable in health and social sciences research for a variety of key partners. For research participants (e.g., map creators) journey maps serve as a form of visual feedback, allowing for longitudinal, three-dimensional and chronological representations of self without personalization (Futch & Fine, 2013; Pauwels, 2015), while having their knowledge, voices, and connections honoured (Paris, 2011). Scholars also contend that visual narratives enable their creators “to express complex identities, extreme contradiction and vacillating contestation because maps do not insist upon a resolved and coherent narrative” (Futch & Fine, 2013, p. 45). The combination of journey maps and interviews can help to address the contradictions. In this way, like other participatory ABM, journey mapping creates a safe and supportive space for participants to share their stories, including those involving trauma. It also offers an opportunity for reflection, which is a vital step in the healing process. The use of visual narratives, such as journey maps, can move beyond normative boundaries contributing to social justice by elevating the voices of participants’ trauma experiences and ensuring they feel seen and heard (Stetz, 2025). For researchers, use of journey maps are beneficial as a means of answering research questions and improving processes and practice (Haltom & Kamdar, 2024). The accessible and versatile nature of journey maps also makes them a valuable communication tool that can assist in providing health and social care professionals with understanding and empathy for their patients and clients (Haltom & Kamdar, 2024; McCarthy et al., 2016). For the public, the approachable nature of journey maps can act as powerful knowledge translation instruments for the public, potentially mitigating or reducing stigma that is often associated with illnesses or mental health challenges, for example (Moretti et al., 2025).
A common journey mapping approach is where experience managers, or researchers create personas or avatars with attributes built on known or observed experiences of the population being explored, and then create the journey map to reflect customer or patient experiences (McCarthy et al., 2016; Park et al., 2020; Qualtrics XM, 2022). Within health and social services research, journey mapping and process mapping have mainly been used to explore patient experience journeys through health systems and services with the goal of improving care or identifying service delivery bottlenecks (Davies et al., 2023; Joseph et al., 2023; Ly et al., 2021; Trebble et al., 2010), using primarily researcher-generated journey maps or templates created by researchers given to patients. There has been some utilization of journey maps in participatory research to document connections, impacts and social realities (Bagnoli, 2009), and with and for Indigenous populations to co-design culturally safe healthcare (Cormick et al., 2024) and to develop a decolonizing research framework (Star et al., 2025). Within the realm of qualitative research with youth, journey mapping has been used to encourage reflection to create narrative timelines (Ly et al., 2021; Nielsen & Bruselius-Jensen, 2021), and has been employed to elicit experiences of care leavers of the child welfare system (Clarkin et al., 2021; Layton et al., 2021). Of these, only the Nielsen, Clarkin and Layton studies employed participant-generated journey mapping, which better aligns with PAR, although Clarkin and Layton used a facilitated group approach within which participants created journey maps (Clarkin et al., 2021; Layton et al., 2021; Nielsen & Bruselius-Jensen, 2021).
Regarding publication of researchers’ journey mapping strategies and processes used, recently, Haltom and Kamdar (2024) contributed to the methodological development and design of journey maps in healthcare settings by sharing their process and design recommendations for journey map matrices. These researchers created a journey map themselves as a data visualization tool based on qualitative interviews with veterans experiencing food insecurity (Haltom & Kamdar, 2024). Kalbach (2016) identified five common journey map approaches: (1) Mental (Cognitive) Model Diagram, (2) Experience Map, (3) Customer Journey, (4) Service Blueprint, and (5) Spatial Map, and Joseph et al. (2022) published an evaluation guide and decision support tool to facilitate patient journey map selection among these five approaches. Several other socially-focused research articles provide aspects of the journey mapping processes, such as participant instructions used in research with systems-involved youth in the U.S. (Layton et al., 2021), prompts employed in educational research with students (Annamma, 2023; Futch & Fine, 2013), and general journey mapping instructions and follow-up questions with at-risk youth in Denmark (Nielsen & Bruselius-Jensen, 2021).
As outlined above, journey mapping research is being done in the health and social services field, and participatory ABM including journey mapping, together with their respective and common benefits and barriers have been documented in the literature. Yet, in doing work with journey mapping, we found that, unlike for example the structured SHOWeD method for questioning photovoice participants about their selected photos (Wang, 1999), a structured guideline geared specifically for use with participant-generated journey mapping in health and social sciences research has not been developed and published. As journey maps are increasingly used within qualitative research, the absence of shared guidance risks inconsistent reporting and limited methodological transparency. Rather than imposing a universal template, guidelines are needed to support reflexive and context-sensitive use of journey mapping by making analytic choices and interpretive assumptions explicit. Such guidelines strengthen qualitative rigor while preserving flexibility in epistemological stance, data collection, and analytic approach.
To address this gap and take journey mapping methodology work one step further, we have developed and present “Journey
The goals of the J-MAPHS methodological framework in health and social sciences research are, 1) to enable research participants to play a role in addressing and improving health and social challenges, 2) to guide researchers in the use of journey mapping during the interview and analysis processes, 3) to advance and integrate ‘pathways of meaning’, the conceptual routes and processes of how individuals make sense of their lives and experiences and 4) to influence practice and policy.
Ethical Considerations
Ethics approval was obtained from the University of Manitoba, Human Research Ethics Board 1 (REB1) at the Fort Garry campus for the studies presented in this paper. All studies were conducted in line with the principles of the Declaration of Helsinki. All participants provided written and verbal informed consent including informed consent for publication of their interview quotes and journey map images. All participants’ names were anonymized to ensure participant privacy and safety. Participants were compensated with an honorarium that was distributed as an e-gift card based on the participants’ preference.
Development of the J-MAPHS Methodological Framework
The J-MAPHS methodological framework was developed within the IN•GAUGE research program. This research focuses on diverse populations (e.g., newcomer youth, young carers, youth transitioning through the pandemic, child-rearing families, and youth with mental health needs). These IN•GAUGE (https://www.ingauge.ca/) research program studies are designed to understand and address health and social issues experienced by young people (i.e., children and youth) as individuals, within families and relationships, and within socio-ecological systems with the aim to improve their health and well-being.
According to scoping and systematic reviews there is no formal guidance on developing methodological frameworks, hence various approaches are used (Cruz Rivera et al., 2017; McMeekin et al., 2020). To advance the development of robust guidance for methodological frameworks, McMeekin and colleagues (2020) summarized the steps used in development of published methodological frameworks into three phases: identify evidence to inform the methodological framework, develop the methodological framework, and evaluate and refine (McMeekin et al., 2020). Cruz Rivera and colleagues’ (2017) systematic review summarized development of methodological frameworks included literature reviews, stakeholder involvement, methods to incorporate stakeholder views (e.g., interviews, thematic analysis), and a pilot phase (testing applicability and modifying) (Cruz Rivera et al., 2017).
Similarly, the inception of the J-MAPHS methodological framework, also referred to herein as J-MAPHS, was informed by evidence in the literature, including existing participatory ABM and journey map methods literature (Davies et al., 2023; Joseph et al., 2023; Pauwels & Mannay, 2020; Wang, 1999) and research team experience, expertise and observation. J-MAPHS uses participant-generated journey mapping, which refers to visual representations created by participants themselves with minimal researcher influence. We acknowledge that a few others (Clarkin et al., 2021; Layton et al., 2021; Nielsen & Bruselius-Jensen, 2021) have similarly used participant-generated journey mapping in their research, which helped guide the development of J-MAPHS.
IN•GAUGE Research Program Studies Using the J-MAPHS Methodological Framework

*This study began in 2021 and journey mapping was only introduced near the end of the study.
**These studies are currently ongoing.

Participant Journey Mapping Instructions

Journey Map Interview Questions
Guiding Frameworks
The J-MAPHS methodological framework is informed and guided by four frameworks: Co-design (Sanders & Stappers, 2008), the Strategy for Patient-Oriented Research (SPOR): Patient Engagement Framework (Canadian Institutes of Health Research [CIHR], 2023), the Youth Engagement in Research Framework (Woodgate, 2022; Woodgate, Moser, et al., 2022), and Trauma-Informed Socially Just Research Framework (Voith et al., 2020, 2021). Together, these frameworks champion an inclusive, people-centred, trauma-informed, action-oriented approach, that is applicable specifically to health and social science research. Each of these frameworks and how they shaped development of J-MAPHS are explained in more detail below.
Co-design, with its roots in action research and design thinking, is a participatory method increasingly used in health research and public service (Moll et al., 2020; Trischler et al., 2019). The goal of co-design is to address a problem or challenge by creating innovation or change in service delivery that is useful and meaningful to potential end-users (Bolster et al., 2021; Reid et al., 2024). Key principles of co-design are lived experience and collaboration (Greenhalgh et al., 2016) and acknowledging service users as part of the team and as experts of their experience (Sanders & Stappers, 2008). This approach prioritizes voices from equity-deserving groups, who are included and empowered in the co-design and decision-making processes (Harrison et al., 2022; Moll et al., 2020). Co-design is operationalized through direct engagement with the communities or individuals impacted by the problem, together with those who are in directly involved in the process or have the capacity to influence change, such as health and social care providers, researchers, and/or policymakers (Bammer, 2013). Use of co-design principles can be seen in Cormick et al. (2024), who employed this approach to develop a journey map resource for culturally safe healthcare for and with First Nations people in Australia. In the development of J-MAPHS, co-design was key, as it shaped how we wrote the instructions and encouragement to participants to create their map in the way that worked best for them (Box 1), and for the creation components of the best practice guidelines (Figure 1) to encourage unhindered independent creation of participant journey maps. Co-design was also integrated into J-MAPHS through active inclusion of participants as experts by incorporating their feedback on their experiences with the process of creating their journey maps via the concluding journey map interview questions (Box 2). Best practices of journey mapping in applied public health & social sciences (J-MAPHS) creation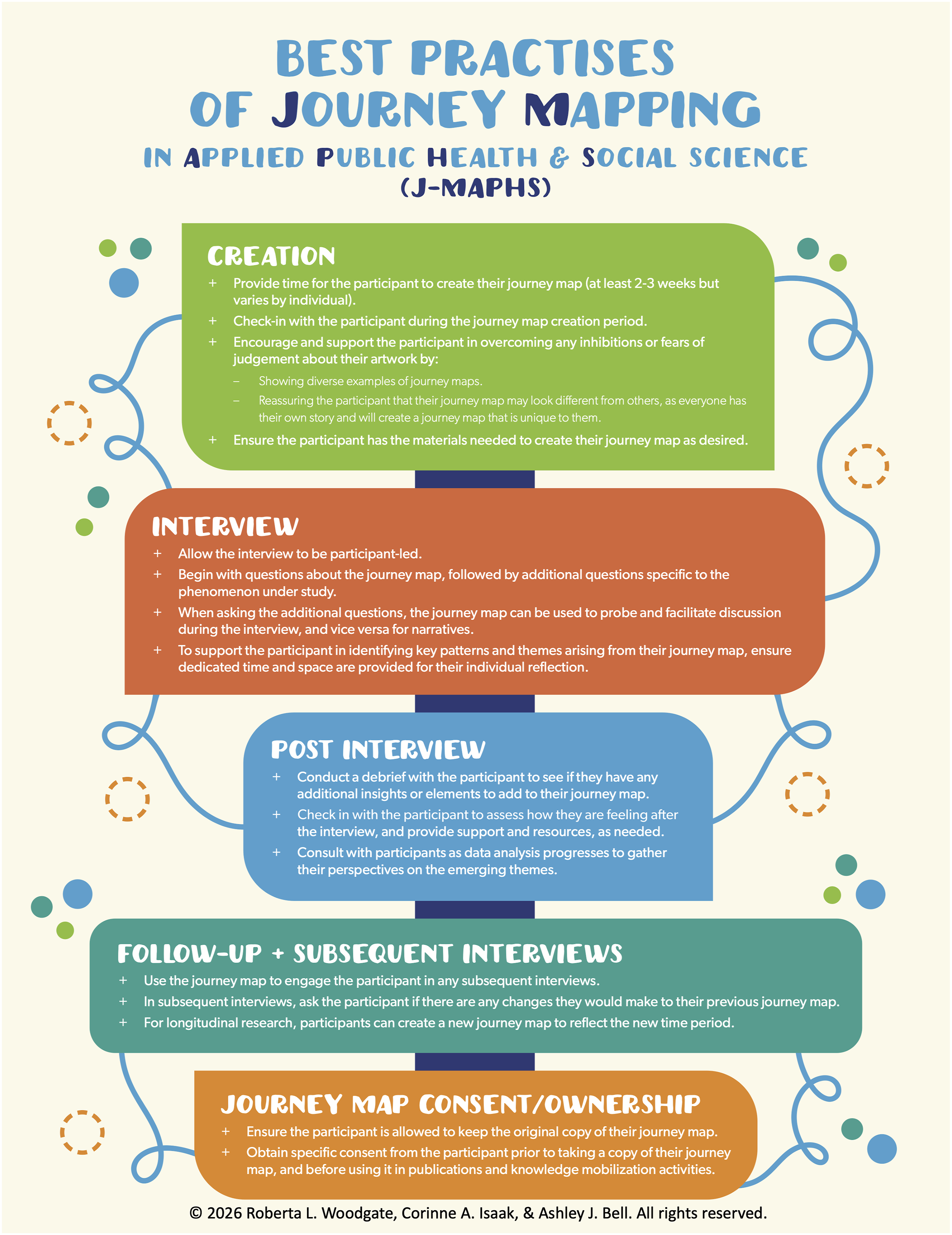
The guiding principles of the Strategy for Patient Oriented Research (SPOR): Patient Engagement Framework, developed by the CIHR (2023), are inclusiveness, support, mutual respect and co-building. These principles are implemented in research to meaningfully engage patients as partners with researchers in active collaboration, focussing on their priorities in conducting research to improve their health outcomes and disseminate and translate knowledge (CIHR, 2023). Alternate terms used internationally for patient engagement include patient involvement, consumer involvement, community involvement, and stakeholder engagement (Chudyk et al., 2022). A recent study by Chudyk et al. (2024) used this framework to conduct a qualitative study to determine the future of Canadian patient engagement in research. The SPOR Patient Engagement Framework supported our desire to centre the participants’ voices throughout their journeys, to reflect on and speak to their own needs and priorities. This facilitated mindful development of the J-MAPHS instructions reflection questions (Box 1), initial interview question prompts (Box 2), and the best practice to allow the interview to be participant-led (Figure 1).
Key principles of the Youth Engagement in Research Framework further support the J-MAHPS methodological framework. The Youth Engagement in Research Framework provides guidance on strategies to facilitate full and active engagement of participants as partners in research (Woodgate, 2022; Woodgate, Moser, et al., 2022). Three key principles from the Youth Engagement in Research Framework informed procedural decisions during J-MAPHS development: (1) Respect for different forms of knowledge. Using multiple forms of data gathering (journey maps and interviews), with flexible, dynamic, and evolving options to engage research participants, embracing imagination and creativity promotes participation. J-MAPHS utilizes flexibility and openness with respect to how participants create their journey maps, providing opportunity for participant to be creative and express themselves in a way that feel authentic to themselves (Box 1). (2) Build trusting relationships. We felt it vital to share leadership in research to empower participants. With J-MAPHS, we wanted to ensure participants are understood to be the expert of their experience and are provided the space to feel heard and acknowledged. These principles led us to include post, follow-up and subsequent interview opportunities (Figure 1). (3) Support diverse expressions of identity. Respecting participants’ unique identities and diversity helps create a safe space for sharing their experiences, which is reflected in the initial journey map interview question asking about materials and colour choice of participant maps and their story behind the meanings of the symbols etc. on their map (Box 2).
As qualitative research is often conducted with participants who have experienced trauma, oppression and marginalization (Alessi & Kahn, 2023), J-MAPHS is guided by a trauma-informed research lens to support participant empowerment and healing (Alessi & Kahn, 2023; Voith et al., 2020, 2021). Trauma-informed qualitative research should actively employ strategies that prevent the re-traumatization of participants, while also promoting participants’ resilience (Alessi & Kahn, 2023). This approach ensures safety for all participants, regardless of their past experiences (Alessi & Kahn, 2023). Interviewers should be well versed on the impacts historical and current traumas at the individual and community level (Alessi & Kahn, 2023; Voith et al., 2020). Safety is established by supporting participant choices and boundaries within the research process (Alessi & Kahn, 2023; Voith et al., 2020). If a participant needs additional emotional support during or after the J-MAPHS process, appropriate community resources should be provided (Alessi & Kahn, 2023; Voith et al., 2020). These key components helped us to shift the research process of J-MAPHS into one of empowerment by including ethical safeguards into J-MAPHS best practices (Figure 1 Journey Map consent/ownership), and debriefing with participants post-interview and providing supports if/as needed (Figure 1 Post Interview). Self-reflection on the interviewer’s part is essential to further delve into their own biases and emotions and how this impacts the research being done (Alessi & Kahn, 2023). This aspect of trauma-informed research reminded us of the importance of completion of field notes post interview, which is done by all IN•GAUGE interviewers.
The J-MAPHS Methodological Framework
To addresses the second goal of the J-MAPHS framework, which is to guide researchers in the use of journey mapping during the interview and analysis processes, we present detailed guidance for researchers on how to use the J-MAPHS framework in health and social sciences research. We do this by explaining and providing rationale for the three key steps described below. Also refer to Figure 1, which depicts best practices for the J-MAPHS methodological framework.
Step 1: Participant Journey Mapping Instructions
Guidelines, instructions and questions are given to participants in advance of their journey map generating, giving them time to consider and reflect (see Box 1). If the participant needs guidance or requires any type of assistance, they are helped as needed by the research personnel. The reflection questions provided to participants while generating their journey maps align with the intent of qualitative research and scientific inquiry more generally. Firstly, qualitative research methodology seeks to answer the ‘what’, ‘how’, and ‘why’ focusing on subjective experiences to understand reasons and motivations. Further, ‘what, why, when, where, who, and how’ (“5W1H” or Kipling method) questions are often used as a creative problem-solving approach (Cook, 1998), which encourages approaching a question or problem from multiple angles to obtain the full story, a comprehensive account of the situation (Zhang et al., 2013).
Step 2: Journey Map Creation
The participant creates a journey map independently, on their own time (as opposed to in a facilitated or group session) and then sends it to research personnel when completed. Research personnel will check-in with participants during this time.
The diversity and uniqueness of participant-generated journey maps in Figures 2–6 substantiate the template-free and independent (non-facilitated, non-group, non-completion-time-limited) intent of the J-MAPHS method, which allows for design freedom and fosters unhindered expressions of experiences. For participants, using this engaging framework gives ownership of the process and opportunity for further reflection during the interview(s). It is integral to recognize that the journey map created will be unique to each participant. Each will approach it in their own way, through different mediums and forms of expression. For instance, some maps have more text and fewer symbols. Yet regardless of the style, the maps provide the environment for participants to better express themselves. Every journey map will be helpful in eliciting a dialogue and understanding a participant’s experience. Journey map of a 17-year-old’s experience of the COVID-19 pandemic Journey map of a 19-year-old’s experience of the COVID-19 pandemic Journey map of an 18-year-old’s experience of the COVID-19 pandemic Journey map of a 23-year-old’s experience of of the COVID-19 pandemic Journey map of a family’s experience with COVID-19 and vaccination



Step 3: Conducting the Journey Map Interview
The interview is scheduled. In addition to questions specific to the phenomenon under study, questions specific to the journey map are asked (See Box 2). The interview begins with the journey map questions where the participant is asked to talk about and describe their journey map with the interviewer who uses interview guide questions to probe and prompt. After the participant is finished describing their journey map, additional questions specific to the phenomenon under study are asked. When asking the additional questions, the journey map can also be used to probe and facilitate discussion during the interview and vice versa for narratives.
Asking specific questions during the journey map interview regarding materials, medium and colours used by participants on their maps (e.g. question A. 2. from Box 2) provides additional layers of meaning on their own. For example, within IN•GAUGE research studies, when asked this question, some participants spoke of their preference to draw their journey map by hand “I prefer drawing over like digitally making things any day” (Female, 15 Y) (Woodgate, Kirk, et al., 2022). Others opted to create theirs digitally (e.g., Canva, Freeform) due to familiarity with the application, ease of use, and accessibility. As one young person noted, these digital tools were “easier than getting paper, pencil, and markers” (Female, 17 Y) (Woodgate, Kirk, et al., 2022). Giving participants freedom to select their own medium for their journey map provides choice, a sense of ownership. It also reduces the risk of participants feeling uncertain or hesitant about embarking on the activity, as has been noted in some photovoice research where some participants expressed anxiety due to perceived researcher expectations of a ‘proper’ photograph (Ronzi et al., 2016).
The use and role of colour and colour choice in art is significant as it is said to act as a type of psychological transference for the artist, wherein the art piece embodies the artist’s emotions (Dalley et al., 2013). In this way, colour in art can be an “emotional signifier” (Hussain, 2021, p. 302) for the artist as a means of connecting to or processing emotions and translating them into meanings, which are then further interpreted by art viewers. Describing their journey map (see Figure 2) of COVID-era experiences (Woodgate, Kirk, et al., 2022), the following quote exemplifies the emotions, connections and meanings related to colour choice by the participant: PARTICIPANT: The yellow is like the start of it but, I don’t know, yellow to me is like an uncertain colour. INTERVIEWER: When you look at your Freeform picture here, you’re moving from left to right and you’ve chosen grey as your background colours. Any specific reason why you chose that colour? PARTICIPANT: Because it’s kind of like a dark colour, like it was shaded, it’s not a happy colour. It kind of feels like my life has changed as a result of COVID because, I don’t know, the fear of it happening again and I still feel like I’m 15 but I’m actually 17. It feels like I just lost a bunch of time in-between that… the bottom of the map, which is like scribbled with a red, that was the low point where there was like nothing going on specifically. And it was just like really depressing. (Female, 17Y)
Having the participant describe their journey map avoids the researcher from making the assumption that ”the picture is the person” (Futch & Fine, 2013, p. 46), which allows the participant to provide their own interpretation of their journey map. It also mitigates a common journey map challenge where researchers may feel urged to create a one-size-fits-all journey map that incorporates all encounters and interactions (McCarthy et al., 2016; Rosenbaum et al., 2017).
The participant-created journey map can also be used throughout the interview to facilitate the conversation. If a series of interviews are to be conducted, the journey map can be used during each of these interviews to engage with the participant. For longitudinal research, participants can create a new journey map to reflect the new period. In these instances, asking about how participants’ journeys have changed provides further opportunity for participant reflection and researcher understanding.
J-MAPHS Analysis
Qualitative analysis takes place alongside data collection, where it is not just the researchers who interpret the data during and after methods like interviews, but also the participants themselves as they engage in the data collection process. All data is imported into NVivo 12 (2018). The graphical data (drawings/symbols from journey maps) serve as visual representations of the textual data (interviews, field notes, words/statements from journey maps) and help to inform themes emerging from the participants’ data. Formally linking the graphical data to the corresponding textual data (visuo-textual analysis) results in a deeper understanding of participants’ perspectives and experiences (Brown & Collins, 2021). Analysis is a co-creation process during the interviews. For example, interview questions about colours used evokes emotions which adds insight and provides further information for researchers. This information is incorporated into the interview, field notes and analysis.
In J-MAPHS, data analysis is iterative in nature. Full immersion in the data occurs by reading and re-reading the data for significant statements. The inductive approach of thematic analysis is employed, which involves identifying recurrent themes across participants and data sources (transcripts, journey maps and field notes), as well as delineating units of meaning from the data, clustering units of meaning to form thematic statements, and extracting themes (Barbour, 2008; Morse & Field, 1995; Patton, 2014). Open codes are discussed, collated, and examined for significant broader patterns of meaning (potential themes).
During analysis, the coded textual data are revisited with the related graphical (i.e. journey map) data by asking the following questions: (1) What is in the visual representations (i.e. drawings/symbols) that supports or reinforces what was learned from the textual data?; (2) What is in the images that challenges what was learned from the textual data?; (3) What is in the images that is not in the interviews?; and (4) What is in the interviews that is not in the images? (Trombeta & Cox, 2022). These questions help to facilitate comparison between different sources of data, considering the possibilities for congruence or divergence between the content of textual and graphical data (Trombeta & Cox, 2022). Notes and memos are detailed to identify and examine overlaps between these data sources, assessing whether they complement, challenge, or reveal different aspects of the experience under study.
The integration of textual and graphical data helps to enhance the depth and clarity of analysis by affording a visualization of the participants’ experiences, while grounding interpretations in direct quotes and narratives. Integration also assists in identifying patterns, inconsistencies, and unique insights that might not be apparent when analyzing each data type in isolation. By simultaneously collecting and analyzing data, any inconsistencies or new insights are further examined through ongoing interviews. This process helps deepen the analysis, providing a more comprehensive understanding of participants’ experiences through J-MAPHS.
J-MAPHS: Advancing Pathways of Meaning in Health and Social Sciences Research
To demonstrate the operationalization and value of the J-MAPHS methodological framework, a selection of uniquely created journey maps and participant quotes reflecting their experiences with the journey map creation process were drawn from six IN•GAUGE research program studies (see Table 1) and are presented here. All participants in these studies provided written informed consent to have their quotes and journey maps published.
Use of J-MAPHS methodological framework, as supported by participant journey maps and quotes can assist in meeting the four goals of J-MAPHS: to enable research participants to play a role in addressing and improving health and social challenges, to guide researchers in the use of journey mapping during the interview and analysis processes, to advance and integrate ‘pathways of meaning’ - the conceptual routes and processes of how individuals make sense of their lives and experiences, and to influence practice and policy. In applying the J-MAPHS framework, in which participant instructions include diverse examples of journey maps and encouragement to “create it in the way that works best for you” (Box 1), we show that the J-MAPHS framework allows for great diversity and uniqueness in the journey maps created by participants, which aligns with one of our guiding frameworks, the Youth Engagement in Research Framework (Woodgate, 2022; Woodgate, Moser, et al., 2022). Based on this work and participant feedback, we contend that use of the J-MAPHS framework in research enables autonomy and inclusion of participants, and facilitates participant agency in representation as per ABM principles (Boydell, Volpe, et al., 2012), allowing their maps to be relatable and accessible to a broad range audiences. This in turn can open the door for creative conversation with health and social care providers and policymakers to propel change and challenge current health and social services norms to shape change (Bammer, 2013).
We establish this by presenting varied and distinct journey maps examples (see Figures 2–6). The first four are from a study exploring youth’s journeys through COVID-19 and how the pandemic impacted their mental health and well-being (Woodgate, Kirk, et al., 2022).
Figure 2 is a non-scripted digital freeform iPhone image. A white looping line moving from left to right on a shaded grey background and vertical lines of shades of grey moving from light to dark left to right depict the shifting flow of the participant’s journey through COVID-19. In describing her journey, the participant shared many emotions experienced along the way with the emotion of sadness as being the most prominent emotion (black mass with red dot at the bottom right corner).
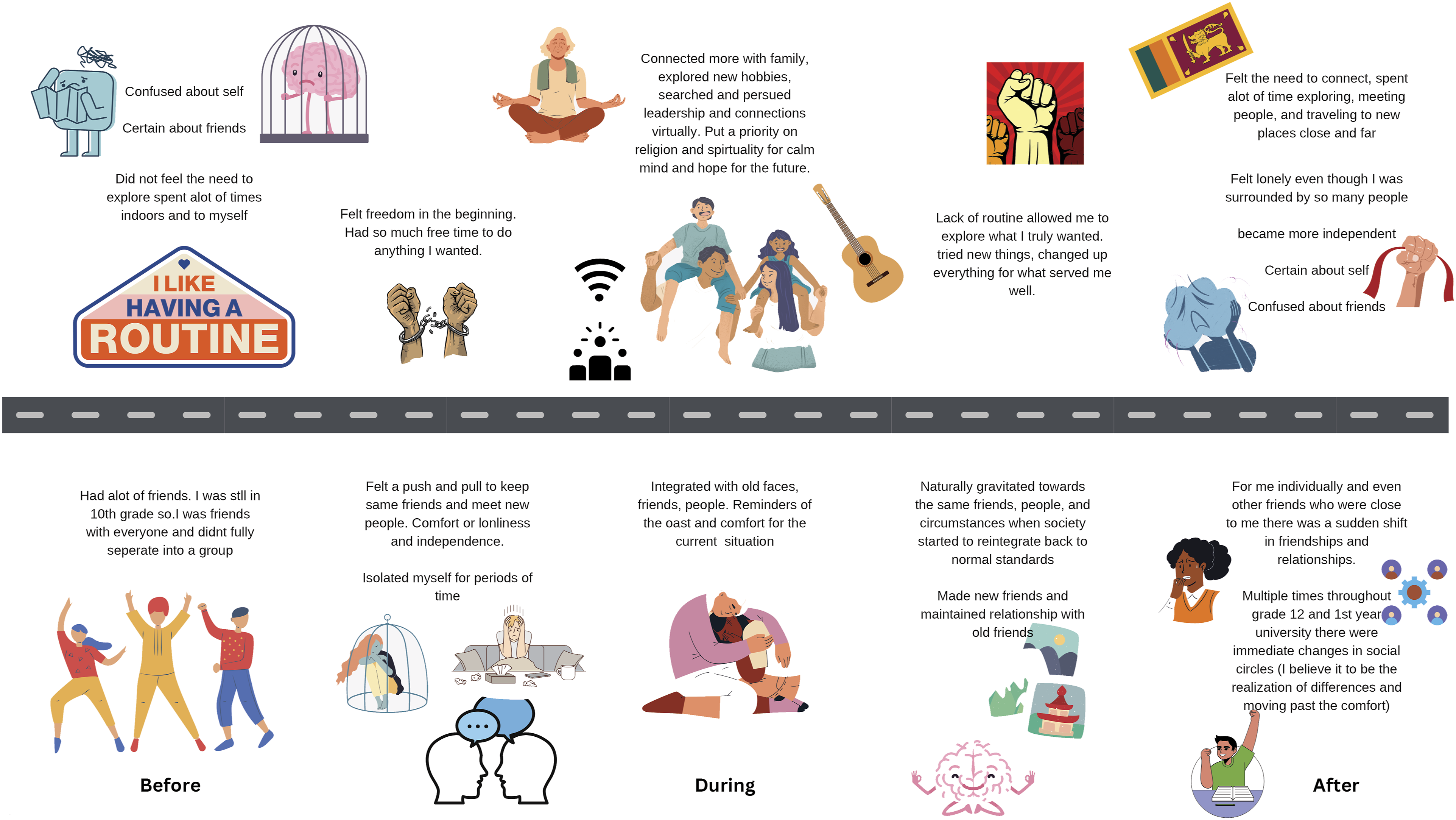
Figure 3, a scripted, and landscaped digital image created by the participant using Canva, shows ‘Before’, ‘During’ and ‘After’ time periods of COVID-19 and a straight grey road across the middle of the entire full image with individual and grouped images with text above and below it. While each image represented key moments experienced by the participant during the pandemic, the most meaningful to the participant was the image of the Sri Lankan flag (right upper corner). Images such as these in a participant’s journey map can serve to anchor meaning across time, which serves to connect the text with the visual (Boden et al., 2018), allowing the two data sources to work together to bring balanced meaning in arts-based research (Drew & Guillemin, 2014), as reinforced by the following, “The first image that I actually put was the Sri Lankan flag…And that’s because the most important part of like the after journey I guess was like visiting Sri Lanka, being able to like visit that place was so important…. the pivotal point where my life truly changed.” (Male, 19 Y)
Figure 4 is a journey map with 24 digital-colored images of people, places, activities or objects placed on white background according to time periods identified in black text between April 2020 to September 2023, with no other text. Each picture depicted an event experienced by the participant during the pandemic, which the participant reflected on during the interview. In creating his journey map, he expressed the following, “I had to really think and you know, I was like doing things that and revealing things at the same time at the same time so it was mentally challenging, but now I’m not like that, it is less mentally challenging…I remember everything that happened to me in these pictures, so it’s been helpful for me to look back at what I did.” (Male, 18 Y)
Figure 5 is by a 23 year-old female who created a hand drawn map with text, symbols, and pictures in black on a white background moving left to right, bordered by a black line across the bottom of the page with Pre-pandemic, COVID-19, and After COVID-19 equally spaced below; images and text are located above correlating time periods (a total of four columns with two occurring in the COVID-19 period) and arrows representing connection to, creating, or resulting found throughout the map. She chose this medium as it afforded her the opportunity to convey important meaningful messages from her interview that go beyond words. She noted that “there’s a lot of repetitive stuff you’ve heard already but it just looks different here” (Female, 23 Y). It afforded her the opportunity of communicating key memories through drawing and text.
In addition to youth, the J-MAPHS methodological framework is relevant for other groups. For example, we used J-MAPHS in a study related to families’ decision-making regarding vaccinating children for COVID-19 and influenza (Woodgate et al., 2023). Using the journey map (Figure 6), a mother conveyed the many frustrations she experienced while waiting for a COVID-19 vaccine she felt was safe for her children. For instance, the section titled ‘Who is Steering the Ship’ captured her confusion and frustration with the inconsistent messaging and lack of reliable information and expressed “everyone had a different answer”. This type of feedback can be utilized to create change in service delivery that is meaningful to end-users and to improve patient health outcomes as per co-design and SPOR Patient Engagement frameworks (Bolster et al., 2021; CIHR, 2023; Reid et al., 2024).
At the end of the journey map interview, participants are asked to provide feedback on their thoughts and experiences during the journey map creation process. As a component of the J-MAPHS framework (see Box 2) this step provides an opportunity for participants to reflect on and process experiences, events or emotions they had not previously engaged with which further helps to validate the framework. Some examples of questions to elicit this feedback include: o How did the journey map activity impact your understanding of [experience/event]? o How did the journey map activity impact your ability to share your experiences with [experience/event]?
In asking these questions, participants noted several benefits that occurred during or after journey map completion, yet they also spoke to potential challenges for participants when embarking on the journey map creation. For one participant in the COVID-19 study (Woodgate, Kirk, et al., 2022), they discussed overall enjoyment in creating their journey map, though they initially had some hesitations: “I actually really liked making this [journey map] just because I felt like it was kind of like a, I don’t know like a spectrum kind of, it wasn’t really just like here are like four things that happened, it was just kind of like how things progressed over time. So yeah, I definitely enjoyed making it… At first, I was kind of hesitant if like my pictures would really like express anything, but I feel like it worked well because I don’t know it’s not really answering a specific question, it’s just kind of like highlighting some stuff that happened to me in the past few years, so I feel like this is a good exercise.” (Female, 23Y)
Likewise, the ability to reflect on their experience was a benefit for another participant in a study on young carers (Woodgate, Bennett, et al., 2024), who commented, “...thank to you and your team for putting it out there as a prompt, it was definitely a reflective experience and kind of helpful making sense of the milestones, the snakes, the ladders” (Female, 30Y).
Engaging in the reflective processes inherent in J-MAPHS was emotionally challenging for a participant in the young carers study (Woodgate, Bennett, et al., 2024), but by doing so, they found catharsis through journey mapping their experiences: “...this was an interesting and hard process like there was a lot of like memories and emotions tied to doing this and to try to go back through the years…I don’t think about these things and...once I finish this experience I am going to ask [my brother] if he’s willing to do it as well ‘cause I think it might also be cathartic for him… this is the most I think I’ve ever told anyone about like my journey outside of my brother, like no one else kind of really knows what I’ve experienced.” (Female, 29Y)
Further, the following excerpts demonstrate how working through the J-MAPHS process was empowering for some participants, which supports the trauma-informed approach used by the J-MAPHS methodological framework (Alessi & Kahn, 2023; Voith et al., 2020, 2021): “I think it was a unique exercise to kind of like put it in like a visual manner, so I am familiar with some of the journaling, but it’s nice to have like a, a concise visualization or even some of like those mental health practices that I have, like it’s nice to have like a one-stop shop where it’s like, oh yeah look at all the projects I’ve made, like look how far I’ve come.” (Female, 23Y) “Like my brain feels occupied when I’m doing it and then like after that it’s like, you kind of feel like a sense of accomplishment after you’re done with them.” (Female, 14Y)
Future Research
The next steps for future pilot testing of the J-MAPHS methodological framework would be to gather feedback on usability, clarity, and relevance to determine if the instructions elicit the intended outcome and purpose with different populations and in different contexts. We also hope to use J-MAPHS in studies in practice settings where the framework processes of participant journey map creation and reflection are visible, for example, to clinicians or teachers. This would help to promote better understanding of patient or student experiences and promote communication. We acknowledge this may require adapting J-MAPHS to different cultures. In the spirit of collaboration, we also invite other researchers to join us in applying the J-MAPHS framework to their work and welcome their input to further evaluate and refine J-MAPHS. This would enhance the validity of the proposed instructions following rigorous methodological and theoretical steps. Given the reflective power of journey maps in helping individuals explore significant periods in their lives, they hold strong potential as an intervention tool for facilitating change. Thus, there is promise for use of the J-MAPHS methodological framework in intervention studies addressing health and social challenges.
Conclusions
This work presented the Journey Mapping in Applied Public Health and Social Sciences (J-MAPHS) methodological framework and demonstrated how the four goals of J-MAPHS are achieved. Use of journey maps within the J-MAPHS methodological framework are an accessible participatory tool that can be utilized in health and social research to engage the whole person, to uncover participant lived experiences, and to share their stories, thus enabling them to play a role in addressing and improving health and social challenges. Yet, standardized methods and guidelines for using participant-generated journey mapping in health and social sciences research were lacking. We have addressed this research gap by providing J-MAPHS as a guide for researchers’ use of journey mapping during the interview and analysis processes, along with supporting rationale of using J-MAPHS to advance and integrate pathways of meaning in health and social sciences research. Journey map examples using J-MAPHS from studies with youth and families that are part of the IN•GAUGE research program showcases diverse and meaningful art pieces facilitated through use of J-MAPHS. The exercise of journey mapping is essential to assist participants in thinking through their experiences and talking about their map in the interview. The journey maps themselves are windows into participants’ experiences, which can be used by participants to process their own emotions and experiences and enhance meaning-making for participants, as well as to inform policy and decision makers and community members, thus assisting in understanding and improving the lives of youth and families. With additional use, refinement and validation, the J-MAPHS methodological framework has potential to standardize and enhance use of journey mapping in health and social sciences research.
Footnotes
Acknowledgements
The authors are grateful and thank youth and family participants for sharing their time, perspectives, and journey maps for these projects.
Ethical Considerations
Ethical approval for projects cited in this article are listed below.
Consent to Participate
All participants provided written informed consent to participate prior to enrolment in the studies.
Consent for Publication
Informed consent was also provided by participants for publication of their interview quotes and journey map images.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the New Frontiers in Research Fund; Grant # NFRFR-2021-00296, Canadian Institutes of Health Research; CIHR -Canadian Research Chair - 950-231845, Grant # PJT 174997, Grant # PJT 186112, Grant # PJT 191729, Grant # PPE 190335, Grant # YN1 191661. The funders had no role in study design, data collection and analysis, decision to publish, or manuscript preparation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to the nature of the research, supporting data are not available for ethical reasons. The participants of this study did not give written consent for their data to be shared publicly.