
Abstract
This qualitative study protocol delineates the formulation of a community-based mental health intervention aimed at preventing suicidal behavior among adolescent females in Gorontalo, Indonesia a province noted for its high national rates of suicide attempts. The study seeks to investigate the lived experiences, psychosocial challenges, and contextual factors influencing suicidal ideation among adolescent girls, while integrating the perspectives of government stakeholders, academics, and women entrepreneurs. Employing a qualitative descriptive design, data will be gathered through in-depth interviews and focus group discussions, followed by participatory co-creation and co-design workshops guided by the principles of Participatory Action Research (PAR). The co-creation process entails collaboratively identifying priorities, designing intervention components, and refining culturally grounded strategies for community-based mental health support. The findings will inform the development of an inclusive, context-specific, and sustainable intervention model that bolsters suicide prevention efforts and enhances community engagement in low-resource settings.
Keywords
Background
Mental health is an essential component of human well-being, as defined by the World Health Organization (WHO); yet, mental health disorders continue to be one of the major contributors to the global burden of disease. Globally, approximately one in eight people live with a mental disorder, and the prevalence of anxiety and depression increased by more than 25% during the COVID-19 pandemic. Mental health disorders are often associated with poverty, reduced economic productivity, social inequality, and increased morbidity and mortality risks. Depression, anxiety, and other mental health conditions are important risk factors for suicidal behavior, accounting for more than 703,000 deaths annually (Bastiaansen et al., 2018; Subu et al., 2023; World Health Organization (WHO), 2021a).
Suicide is a serious public health concern, particularly in low- and middle-income countries (LMICs). Females, especially adolescent females, have been found to exhibit higher rates of suicidal ideation and suicide attempts than males. Research across South Asia and Southeast Asia has demonstrated that adolescent girls experience a high psychosocial burden triggered by violence, gender-based discrimination, family problems, social pressures, and limited access to mental health services. These findings align with the Indonesian National Adolescent Mental Health Survey (I-NAHMS), which identified high prevalence rates of anxiety, depression, severe stress, and suicidal ideation among Indonesian adolescents (Kaligis et al., 2023; University of Queensland & Johns Hopkins Bloomberg, 2022).
In Indonesia, variations in suicide rates across provinces indicate differences in social, cultural, religious, and economic contexts that require region-specific preventive approaches. Gorontalo Province has one of the highest rates of suicide attempts. As of October 2023, 31 suicide cases have been recorded in Gorontalo, reflecting a concerning upward trend that has drawn national attention. Investigations by the National Mental Health Center (PKJN) found that this phenomenon is associated with social pressure, family dynamics, limited access to mental health services, and weak community support systems. Previous quantitative research conducted among adolescent females in Gorontalo revealed a high prevalence of suicidal ideation and its association with anxiety, depression, and stress. These findings underscore the need for an in-depth exploration of the lived experiences, sociocultural factors, and barriers to care faced by this population (Infopublik.id, 2023; Onie et al., 2020; Suma, 2023).
A qualitative approach is needed to uncover the contextual and interpersonal dynamics, as well as the perceptions of adolescent girls and local stakeholders regarding suicide prevention, so that the insights obtained can serve as the basis for designing culturally relevant and locally appropriate interventions. The WHO recommends strengthening community-based mental health services as an effective strategy to increase access, reduce stigma, and reinforce social support. Empirical evidence, such as the Roseto Study, shows that communities with strong social cohesion and emotional support have natural protection against stress and adverse health outcomes (Levin, 2020; World Health Organization (WHO), 2021b).
In the Indonesian context, primary healthcare transformation emphasizes promotive and preventive approaches, early detection, peer support, and community-based mental health models involving families, community health workers, teachers, and local stakeholders. To produce interventions that are relevant, acceptable, and sustainable, the intervention design process must actively involve adolescent girls, families, the government, academics, the private sector, and the broader community (Kemenkes RI, 2022).
Co-creation and co-design approaches enable the integration of professional knowledge with lived experiences, ensuring that the resulting intervention is aligned with community needs and can be effectively implemented in the Gorontalo context. Co-creation and co-design approaches are essential methodologies in public health that effectively merge professional expertise with community members lived experiences. This integration ensures that health interventions are not merely top-down mandates but are genuinely reflective of and responsive to community needs, leading to more successful implementation and sustained engagement in the long run. Research demonstrates that co-creation fosters a sense of ownership and empowerment among community stakeholders when they are involved in developing health interventions. For example, Morote et al. highlighted how co-creation strategies in school-based programs allow adolescents to become agents of transformation, aligning educational interventions with their emotional and community resilience needs (Morote et al., 2022).
Studies such as those by Josefsson et al. illustrate the substantial benefits of co-creation in healthcare. They found that the collaborative creation of health services allowed for innovative ideas and meaningful exploration of user values, leading to services that were more aligned with patient needs. Engaging communities through co-design not only generates better health outcomes but also plays a critical role in the iteration and refinement of intervention strategies, emphasizing the need for structured approaches in the development and evaluation of co-created interventions. These frameworks highlight stakeholder engagement as a key component, facilitating the translation of complex strategies into actionable health programs (Areskoug-Josefsson et al., 2020; Loisel et al., 2025; O’Cathain et al., 2019). Indicated that active community engagement leads to tailored solutions, underscoring the importance of partnership in crafting interventions that genuinely resonate with public health objectives (McKinnon et al., 2022).
By fostering collaboration and ensuring the active involvement of community members, these approaches lead to interventions that are better aligned with the unique needs and contexts of the populations they serve. Future public health initiatives should adopt these methodologies as standard practices to enhance their effectiveness, sustainability, and community acceptance. Therefore, this study was developed as a qualitative study protocol aimed at exploring the experiences, perspectives, and needs of adolescent females and key stakeholders related to suicide prevention, and using these findings to support the co-creation and co-design of a contextual, inclusive, and sustainable community-based mental health intervention model.
Methods
This qualitative study protocol is an integral component of a larger research initiative focused on the co-creation and co-design of a community-based mental health intervention aimed at preventing suicidal behavior among adolescent females in Gorontalo, Indonesia. This article does not present empirical findings; rather, it delineates the methodological framework, procedures, and planned activities that will inform the implementation of the qualitative phase and subsequent co-creation process. In mental health intervention research, community-based participatory research (CBPR) is a pivotal methodology for fostering effective and culturally relevant interventions. For instance, Giebel et al. described a protocol for co-producing a community-based mental health intervention targeting older adults in Colombia, emphasizing the significance of cross-cultural knowledge exchange and public involvement, particularly in low- and middle-income countries (LMICs), where mental health resources are scarce.
Well-designed qualitative studies enhance the contextual understanding of health disparities, facilitating the development of more robust and locally informed strategies to address community-level health issues. Community engagement in mental health interventions can address various biopsychosocial factors during a crisis. The importance of integrating qualitative research methods within CBPR frameworks is further exemplified by Scott et al., who explore how (Scott & Powell, 2025). Their use of a stepped-wedge design allows for iterative feedback and adaptations based on community input, thereby enhancing overall mental health intervention. Similarly, Haya et al. demonstrated that a mixed-methods approach to community participation in Japan not only identified local health issues but also empowered community stakeholders to actively participate in the planning and execution of interventions (Haya et al., 2020). Furthermore, qualitatively exploring community perspectives is essential for comprehending the nuances of health behaviors in specific cultural contexts. Sheehan et al. employed focus groups to investigate how African Americans with severe mental illness and trauma perceive dietary and physical health challenges, providing valuable insights into the intersection of health behaviors and mental health. This emphasis on community-determined mental health issues is reinforced by Khodyakov et al. ’s study on community engagement outcomes in mental health services, underscoring the importance of participatory methodologies in delivering culturally competent care (Khodyakov et al., 2011; Sheehan et al., 2023).
The study is grounded in the understanding that adolescent females are a population with elevated vulnerability to suicidal ideation and attempts and that community-based, culturally grounded interventions require the active participation of multiple stakeholders. Therefore, the research design integrates qualitative exploration with participatory approaches to ensure that the intervention model reflects the participants’ lived experiences, contextual needs, and community resources.
Study Design
A qualitative descriptive design will be employed, combining in-depth interviews and focus group discussions (FGDs) to explore the lived experiences, perceptions, and needs related to mental health and suicidal behavior among adolescent girls. This qualitative phase will inform a subsequent co-creation and co-design process involving community stakeholders, including government representatives, academics, private-sector actors, and community members. This study follows the principles of Participatory Action Research (PAR), in which stakeholders are engaged throughout the process to collaboratively define problems, identify priorities, and generate solutions.
Study Setting
The study will be conducted in Gorontalo, Indonesia, one of the provinces with the highest rates of suicide attempts. Gorontalo is located in the eastern part of Indonesia and is geographically distant from the nation’s capital, Jakarta. The province is culturally known as
Participants and Sampling Strategy
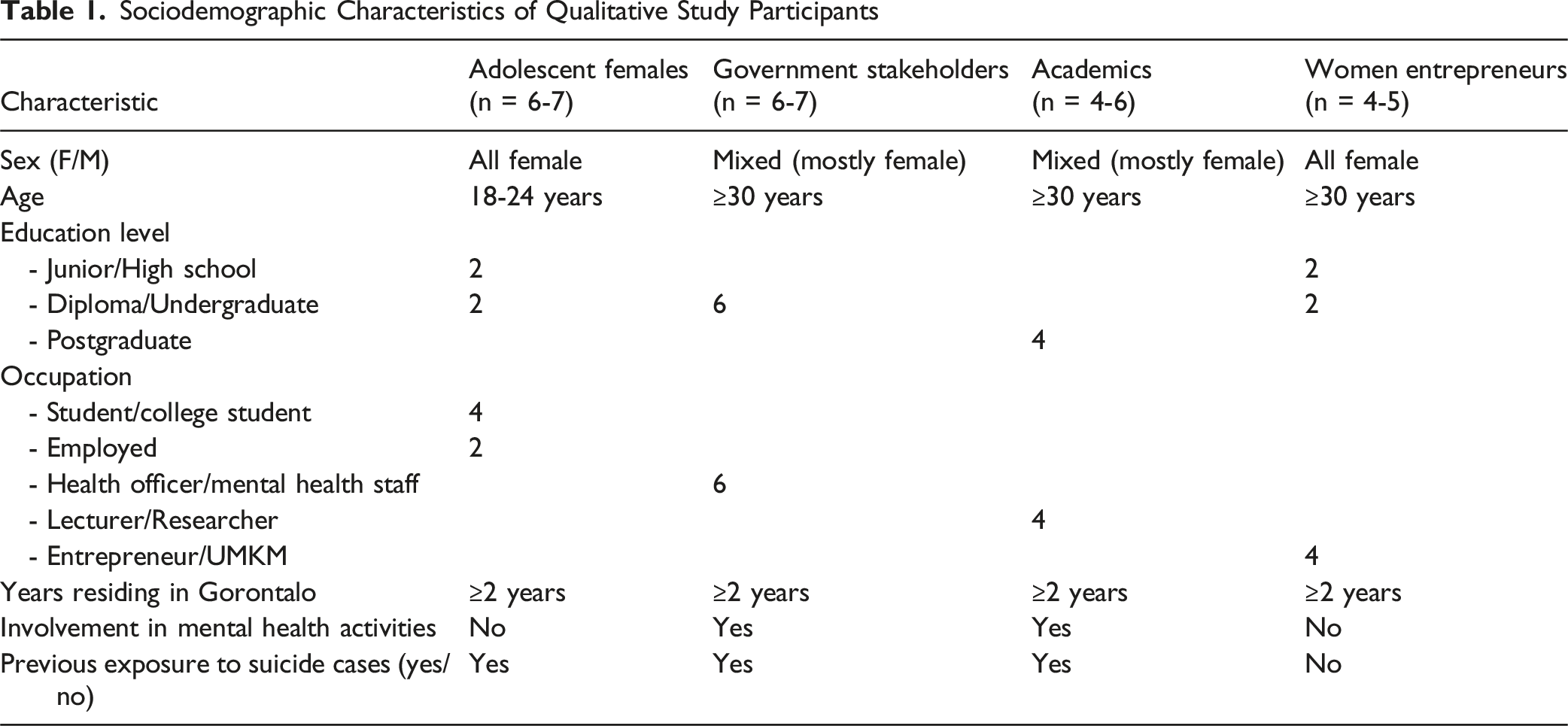
Participants will be selected through purposive sampling based on the quadruple helix framework (Table 1). The eligibility criteria included residing in Gorontalo for ≥2 years, active involvement in mental health initiatives or related service provision, or possessing relevant expertise in community-based mental health (Indrawati, 2018). - Adolescent females (18–24 years), with a history of mental disorders and suicidal ideation among adolescent females (BKKBN, n.d, Sawyer & Patton, 2011; World Health Organization, n.d) - Government stakeholders, particularly the mental health task force (TP-KJM) at the Gorontalo City Health Office, and Mental Health Program Officers at Community Health Centers (Puskesmas) in Gorontalo City (Indrawati, 2018) - Academics (lecturers) and school teachers involved in mental health promotion, youth health, or community empowerment (Indrawati, 2018) - Female entrepreneurs and community actors contribute to local economic resilience and social support structures. (Indrawati, 2018)
Recruitment and Sample Size
Recruitment
Participants will be recruited using purposive sampling to ensure representation across the four stakeholder groups included in the quadruple helix model: adolescent females, local government stakeholders (TP-KJM), academics, and women entrepreneurs. Recruitment will take place in Gorontalo City through collaboration with community health centers, schools, TP-KJM networks, higher education institutions, women’s economic groups, and trusted community organizations.
Sample Size
As a qualitative study, the sample size will be determined by the principles of
The approximate sample size per group was as follows. • Adolescent females: 6–7 participants (in-depth interviews) • TP-KJM stakeholders: 6–7 participants (FGD) • Academics: 4–6 participants (FGD) • Women entrepreneurs: 4–5 participants (FGD)
Total estimated participants: 20–25. (Figure 1) Recruitment Process for Qualitative Participants in the Quadruple-Helix Stakeholder Groups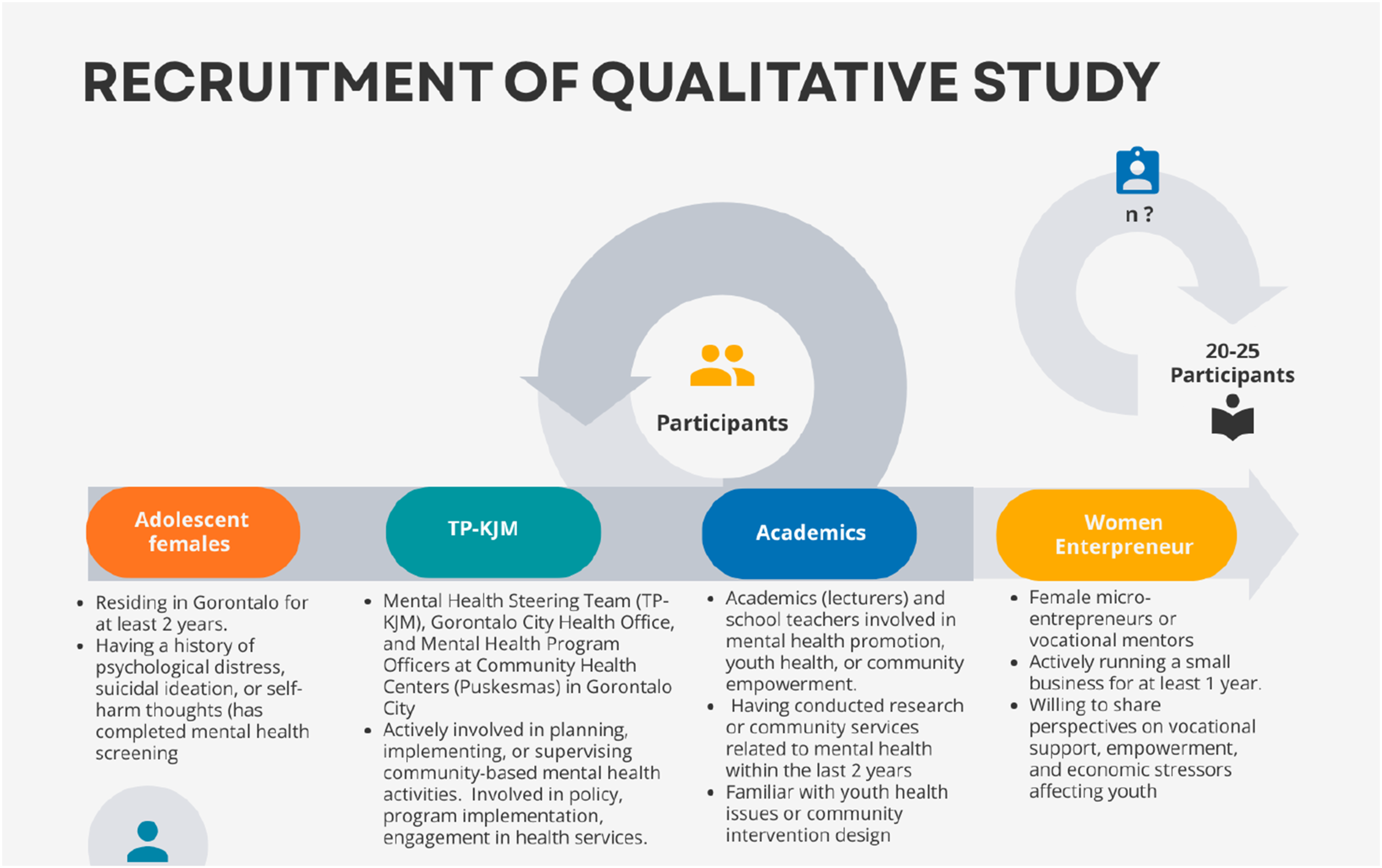
Sociodemographic Characteristics of Qualitative Study Participants
Data Collection Procedures
In-Depth Interviews
This study was conducted with adolescent females to explore their lived experiences of suicidal ideation, self-harm, emotional distress, perceived triggers, coping mechanisms, and expectations for community-based mental health support (Table 2).
Focus Group Discussions (FGDs)
FGDs will be conducted separately with each stakeholder group to capture a collective understanding of needs, community resources, service gaps and potential intervention components. Discussion guides will be developed using open-ended prompts to promote reflection, dialogue and collaborative meaning-making (Tables 3, 4 and 5).
Co-creation and Co-design Workshops
Following the in-depth interviews and focus group discussions, participatory co-creation and co-design workshops will be conducted involving all stakeholder groups. These workshops aim to synthesize qualitative findings, identify priority issues, and collaboratively develop culturally grounded intervention components, sustainability mechanisms, and monitoring strategies (Table 6).
Data Analysis
Qualitative data will be analyzed using thematic analysis following Creswell’s framework: preparing the data, coding, generating categories, identifying themes, and interpreting findings. (Creswell, 2018). Coding and theme development were supported by NVivo 12 Plus to ensure systematic organization. Reflexivity, peer debriefing, triangulation across participant groups, and maintaining an audit trail were applied to enhance credibility and dependability. Data analysis will follow the iterative process recommended for qualitative inquiries. Initial analysis will begin immediately after the first round of the interviews or FGDs. This enabled the research team to identify emerging insights, refine probing questions, and determine whether additional participants or follow-up interviews were required. The process of collecting, coding, comparing, and refining the data will be repeated until thematic saturation is reached (Sugiyono, 2021).
Rigor
This study adheres to the four criteria of trustworthiness as proposed by Lincoln annd Guba (1986) credibility, transferability, dependability, and confirmability to ensure methodological rigor and reliability in thequalitative approach, particularly given the sensitivity of topics related to suicidal ideation, self-harm, and emotional distress (Youn et al., 2021).
Credibility
We will ensure credibility in several ways. We will use semi-structured interviews and focus group discussions (FGDs) to gather detailed stories from participants while keeping interviews consistent. We checked with participants by sharing summaries of their stories to make sure they were accurate and true. This helps us see where views on suicidal behavior and community support agree or differ.
Transferability
Semi-Structured Interview Lived Experience of Adolescent Females (In-Depth Interview)

FGD Guide Government Stakeholders

FGD Guide Academics

FGD Guide Women Entrepreneurs

Co-Creation & Co-design Workshops (All Stakeholders)

Dependability
To make the research more reliable, we kept detailed records. We wrote down notes about the setting, feelings, and body language during interviews and group discussions. We also kept a record of our research choices, changes to interview questions, thoughts on analysis, and updates to our coding. We will regularly meet with the research team to talk about coding, analysis choices, and new ideas.
Confirmability
Confirmability was supported through reflexive practices and transparent documentation. Researchers will maintain reflexive journals to identify and bracket their own assumptions, especially given the emotionally charged nature of suicidal behavior.
Discussion
This qualitative study protocol was designed to explore the lived experiences, contextual determinants, and community-level support needs related to suicidal behavior among adolescent females in Gorontalo, Indonesia. By integrating perspectives from adolescents, government stakeholders, academics, and community economic actors, this study seeks to generate a multi-layered understanding of the drivers of suicidal behavior and the structural and sociocultural factors influencing help-seeking and mental health outcomes. These insights will serve as the foundation for developing culturally grounded, community-based mental health interventions. Adolescent females are known to face heightened vulnerability to emotional distress, self-harm, and suicidal ideation due to gendered social pressures, stigma, and inequitable access to mental health care services. Existing suicide prevention efforts in low- and middle-income countries are often fragmented, medicalized, and insufficiently responsive to the lived realities of young women. Thus, an in-depth qualitative exploration of emotional experiences, social environments, and barriers to care is essential for generating the contextual knowledge required to design an intervention that is relevant, acceptable, and implementable in the Gorontalo community. The methodological orientation of this study toward co-creation and co-design deepens its potential contribution. Co-creation, understood within the framework of Participatory Action Research (PAR), extends beyond simple consultation and emphasizes the active involvement of stakeholders throughout all stages, from identifying needs to designing, implementing, and evaluating initiatives. As described by Vargas et al. (2022), co-creation functions as a comprehensive construct that not only integrates diverse expertise but facilitates shared ownership, empowerment, and social inclusion (Vargas et al., 2022). Co-design, as one strategy within co-creation, places participants’ knowledge, lived experience, and priorities at the center of the intervention design process, ensuring that solutions emerge from community-defined realities. Co-production further contributes by supporting collaborative implementation and enabling stakeholders to jointly generate actionable knowledge (Figure 2). Co-Creation and Co-Design Framework used in the development of a community-based mental health intervention for adolescent females in Gorontalo, Indonesia
The co-creation process follows six iterative stages adapted from Vargas et al. (Vargas et al., 2022).
Identify
Mapping relevant structures and stakeholders involved in adolescent mental health and suicide prevention.
Analyse
Examining stakeholder relationships, shared and conflicting values, and interaction patterns to understand the dynamics of decision-making.
Define
Prioritizing key problems and determining collective actions based on insights from the previous stages.
Design
Collaboratively developing intervention goals, strategies, evaluation mechanisms, and resource allocation.
Realise
Testing the proposed strategies, gathering feedback, and refining components through continuous or phased implementation.
Evaluate
Assessing outcomes, reviewing lessons learned, and identifying sustainability needs, such as resources, partnerships, and capacity strengthening.
Co-design has increasingly been recognized as a key participatory approach in public health because it enables stakeholders including communities, practitioners, and researchers to collaboratively shape health interventions that reflect real needs and lived experiences. Through intentional, iterative, and dialogic processes, co-design supports the creation of culturally grounded and context-sensitive solutions, while strengthening engagement and shared ownership among participants. This collaborative ethos emphasizes inclusive decision-making and values the experiential knowledge of those directly affected by design outcomes (Zeivots et al., 2025). Research in various health contexts further demonstrates that co-designed interventions enhance relevance, acceptability, and sustainability by aligning program strategies with local priorities and social dynamics) (Longworth et al., 2024; Okop et al., 2023; Slattery et al., 2020).
The multi-informant design of this study is another strength. Government stakeholders (TP-KJM) will provide insights into structural and system-level gaps; academics will contribute theoretical and evidence-based perspectives; and women entrepreneurs will highlight the relevance of economic empowerment and social participation as protective factors for youth mental health. This diversity enhances the ecological validity of the findings and offers a uniquely comprehensive foundation for designing an intervention model suited to Gorontalo’s sociocultural context. Nevertheless, this study has some limitations. As a qualitative protocol, it did not measure intervention effectiveness or allow generalization beyond the study population. Self-reported accounts of suicidal ideation may be influenced by emotional discomfort, recall bias, or social desirability.
Despite these limitations, this study is expected to make meaningful contributions by generating context-sensitive evidence for suicide prevention and empowering multiple sectors to participate in designing community-based mental health interventions. By embedding co-creation and co-design processes within a qualitative exploration of lived experiences, this study provides a robust pathway for producing an intervention that is culturally rooted, community-owned, and sustainable. The findings will also offer valuable insights for future quantitative evaluations, policy development, and broader health promotion strategies targeting adolescent mental health in low-resource settings.
Conclusion
This qualitative study protocol outlines a systematic approach for exploring the lived experiences, contextual determinants, and community support needs related to suicidal behavior among adolescent girls in Gorontalo, Indonesia. By integrating perspectives from adolescents, government stakeholders, academics, and community economic actors, this study will produce a comprehensive understanding of the multi-level influences shaping mental health vulnerability. Through the use of in-depth interviews, focus group discussions, and participatory co-creation and co-design workshops, the study aims to design a culturally grounded and community-owned mental health intervention. The adoption of a Participatory Action Research (PAR) framework ensures that the resulting model reflects both lived experiences and structural realities, enhancing feasibility, acceptability, and long-term sustainability. The findings of this study will contribute to strengthening community-based suicide prevention strategies in low-resource settings. This study will provide foundational evidence for developing, refining, and eventually evaluating an intervention model that is responsive to the unique sociocultural context of adolescent females in Gorontalo. Ultimately, this protocol establishes a pathway toward multisectoral collaboration, empowerment, and inclusive mental health promotion within the community.
Footnotes
Acknowledgment
All authors of this manuscript have disclosed any potential financial or personal conflicts of interest with organizations or individuals that may have influenced their work. The authors have also disclosed any financial support received for the preparation of this review. The authors explicitly declare that there are no relevant conflicts of interest that could affect the objectivity of this study.
Ethical Approval
Ethical approval for this project was obtained from the Research Ethics Committee of the Faculty of Public Health, Hasanuddin University (approval number: 1608/UN4.14.1/TP.01.02/2024). Participants received detailed oral and written information before providing informed consent. They were informed about the aims of the study, guaranteed anonymity and confidentiality, and notified that participation was voluntary, with the option to withdraw at any time. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Author Contribution
Conceptualization: YAA., AZA., SN., and DAP.; methodology: YAA., AZA., SN.; validation: AZA., SN. DAP.: Formal analysis, YAA.; investigation, AR., IFI. and SS.; data curation, YAA., AZA., and SN.; writing the original draft preparation, YAA.; supervision, AZA., SN., DAP., AR., IFI., and SS. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Center Of Higher Education Funding And Assessment (PPAT) Ministry Of Higher Education Indonesia Endowment Fund (LPDP); Grant Number, 202209090498.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors of this manuscript have disclosed any potential financial or personal conflicts of interest with organizations or individuals that may have influenced their work.