
Abstract
There has been interest in using social media for consumer engagement in hospitals, particularly for service design and quality improvement, but services have identified a need for guidance. This article outlines the methods used to involve stakeholders in the development of a guide for the use of social media as a consumer engagement tool for Australian public hospitals, and describes the changes to the guide and implementation findings that resulted from stakeholder involvement. The development of the guide involved cycles of two interrelated methods – (1) small group co-creation involving three hospital consumer representatives, three service provider representatives and three academics gathering and analysing data, and integrating findings into the development of the guide; and (2) a consultation with eighteen hospital stakeholders who provided feedback on versions of the guide throughout its development. Participants were encouraged to use their experience as service providers and consumers to reflect broadly on how the content and design of the guide could support social media-based consumer engagement within their particular setting. The co-creation and consultation methods led to four main feedback themes: (1) Enhancing usability is critical for guidance resources; (2) Executive support and teamwork are essential for implementation; (3) Start small and build experience and knowledge over time; and (4) Thinking about new methods brings up questions around existing practice. Involving stakeholders in the design process through co-creation and consultation methods led to critical changes to the guide, enhancing its usability and creating a focus in the guide on building organisational and individual capacity around service design and improvement. Involving stakeholders in the development of the guide also allowed us to translate existing research knowledge into practical implementation strategies and tools, and may increase the likelihood of the guide being used by hospitals, providers and consumers.
Keywords
Background
Social media are any online applications that allow for users to create or curate their own content, connect with other users, and form social networks (Obar & Wildman, 2015). Social media platforms are used in health for a wide range of functions, including sharing information about hospitals and their services (Househ, 2013; Richter et al., 2014), peer-to-peer contact (Gupta et al., 2020; Patel et al., 2015; Smailhodzic et al., 2016), service data gathering (Bornkessel et al., 2014; Gupta et al., 2020; Househ, 2013) and involving consumers and other stakeholders in the design and improvement of services (Walsh et al., 2021).
Recent research has focused on using social media to engage consumers in the design and quality improvement of public hospital services (Walsh et al., 2021; Walsh et al., in-press; Walsh et al., 2021). Engaging consumers – people who are users, or potential users, of hospitals and health services (Horvat, 2019) – is an established practice in many health systems, including being a legal duty or requirement for hospital accreditation in some jurisdictions (Australian Commission on Safety and Quality in Health Care, 2021; NHS England, 2017; Ontario Hospital Association, 2017). Consumer engagement activities are primarily conducted in-person (e.g., design workshops, consumer membership of committees) or through data gathering exercises such as surveys (Hughes, 2008; Mockford et al., 2011; Nilsen et al., 2006). There has been interest in Australia in adding social media-based engagement to the existing suite of consumer engagement methods (Farmer et al., 2018; Johnson, 2015; Walker et al., 2019), however health services have indicated that further guidance is needed before such activities are undertaken (Hill, 2014).
To meet this need for guidance, we developed a guide for health services, providers and consumers around the use of social media as a consumer engagement tool (Walsh et al., 2022), and involved key service provider and consumer stakeholders throughout the development process. Involving stakeholders in the development of health guidelines, standards and guidance resources can help increase uptake and implementation by increasing their relevance, usability and acceptability in real-world practice (Fretheim et al., 2006; Harrison et al., 2010; Petkovic et al., 2020). The importance of stakeholder involvement in the development of guidelines, guidance and standards is reflected in the increasing expectation from policy makers and funders that service providers and consumers will be involved in development processes through equal partnerships such as through co-production and co-design (NHMRC, 2016; NICE, 2015; WHO, 2014).
Cycles of small-group co-creation, and broader consultation with key stakeholders who represented end-users of the final guide, were used to develop the guide. Co-creation is a method described as “collaborative knowledge generation by academics working alongside other stakeholders … to align research and service development” (Greenhalgh et al., 2016) (p.1). The principles of co-creation are looking at problems and challenges in health from a systems perspective, viewing health design as a creative practice driven by the experience of consumers and providers, and valuing the process of design as much as the outcomes (Greenhalgh et al., 2016). Consultation is a form of engagement where stakeholders are asked for their feedback or experience, and that data is used to inform change and decision making (International Association for Public Participation, 2018; Ocloo & Matthews, 2016; Sarrami Foroushani et al., 2012).
The aim of this study was to use co-creation and consultation methods to develop a guidance resource (‘the guide’) for using social media as a consumer engagement tool for service design and quality improvement in Australian public hospitals. This article outlines the methods of co-creation and consultation we used to develop the guide, and presents the outcomes of stakeholder involvement.
Method
The development of the guide involved two interrelated methods – (1) a co-creation process involving a small group of stakeholders working with the researchers to gather and analyse data, and integrate the findings into the development of the guide; and (2) a consultation conducted with a larger group of stakeholders to provide feedback on the guide throughout its development. As we describe the methods in this section we will distinguish between the methods of co-creation and consultation and how they were used to complement each other.
Recruitment
Co-creation group
The co-creation group consisted of three researchers (LW, NH, SH) and six public hospital stakeholders who were the members of the advisory committee for the research project of which this study was a part (DH, JH, NJ, CL, BM, SR). Three of the stakeholder members of the group identified as public hospital consumer representatives, and three identified as service provider representatives.
Stakeholder members of the co-creation group were invited following purposeful sampling (Palinkas et al., 2015) from the professional networks of the three academic researchers, who were seeking people in roles as service providers or consumer representatives in Australian public hospital settings for their experience using social media as part of their role and/or experience in consumer engagement in hospital quality improvement. Invited stakeholders were given detailed participant information and signed a written consent form. Consumer representative members of the co-creation group were paid AU$75 per meeting. This amount was in line with the rates for consumer involvement in ongoing meetings recommended by organisations who engage consumers in advisory roles (Health Consumers New South Wales, 2021; Safer Care Victoria, 2018). Offering payment for consumer members was in recognition that consumer representative roles may take time away from paid employment, which may be a barrier to participation (Chauhan et al., 2021; McCarron et al., 2020). Provider participants did not receive a payment because it was likely that the project aligned with their paid work.
Six public hospital stakeholders (three who identified as service providers, and three who identified as consumer and community representatives), and three health researchers, participated in the co-creation group. The stakeholders in the co-creation group had experience working and/or as patients, carers or community representatives in a range of public hospital services and settings. These included palliative care, mental health, ICU and critical care, transplantation, chronic disease, consumer engagement and representation, health service governance, and health communications. All participants in the co-creation group are co-authors on this article.
Consultation participants
Eighteen participants were recruited to the consultation. Convenience sampling (Battaglia, 2008) was used to recruit the consultation participants. Participants were recruited by sharing recruitment information through the networks and communication channels of the researchers and co-creation group, and through contacting Australian public hospitals, public health networks and relevant health and consumer peak bodies to share the study information through their own networks and communication channels. Recruitment information was also sent to participants from a previous related study (Walsh et al., 2021; Walsh et al., in-press).
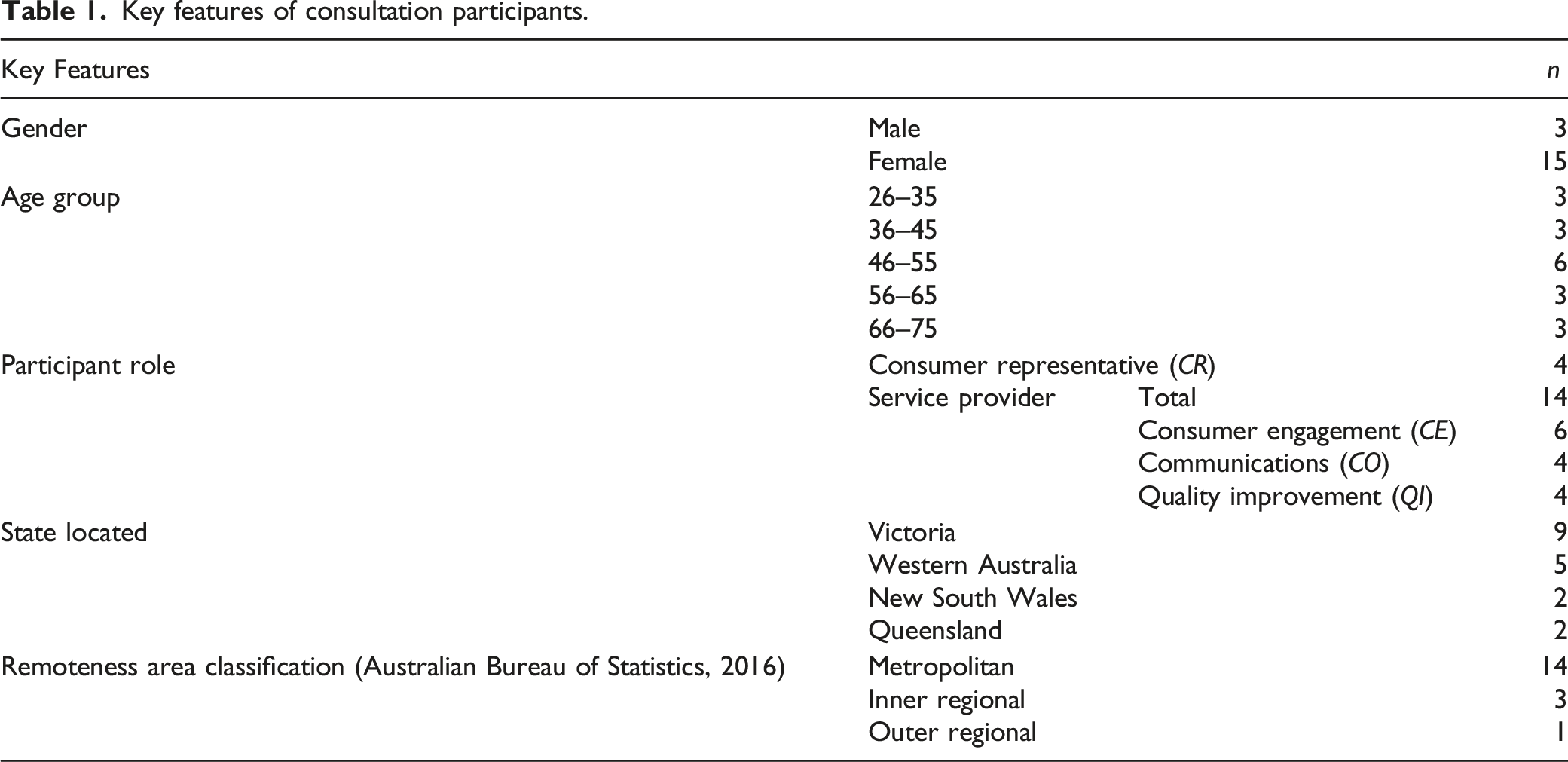
People who were interested in participating contacted LW directly and were screened for eligibility. Eligibility criteria were: aged >18; living in Australia; able to read English; access to email; experience in a consumer representative, quality improvement, consumer engagement/patient experience or communications role in an Australian public hospital; experience in using social media to involve consumers in public hospital service design, patient experience or quality improvement activities; able to participate in a 30-minute interview via telephone or videoconference. People who were eligible for the study were given detailed information and were enrolled once they had completed a written informed consent form. Each participant’s consent was reconfirmed verbally at the start of their consultation interview. Consumer representative participants were given a AU$50 gift voucher for their participation. Again, this was in recognition that participation in the study may take time away from paid work (Chauhan et al., 2021; McCarron et al., 2020).
Key features of consultation participants.
Development of the guide
The guide was developed through cycles of co-creation and consultation. This section outlines how we alternated between small group co-creation to develop versions of the guide, and consultation with a larger group of stakeholders to gather feedback on each version of the guide. This approach of using a small committee to develop guidance documents, and a larger group of key stakeholders for feedback at different stages of the development process, follows the recommended approach to involving stakeholders in guidance and standards development from the National Institute for Health and Care Excellence (NICE) (NICE, 2015). Figure 1 outlines the three different stages of the guide development process, and the participants involved in each stage. The guide development process.
Pre-consultation
The content in the first draft of the guide was based on findings of research conducted by the members of the co-creation group. The findings from two studies - a scoping review of the international literature examining the use of social media as a tool for stakeholder engagement in health quality improvement (Walsh et al., 2021), and interviews with Australia public hospital stakeholders about their experience and beliefs around using social media as a consumer engagement tool (Walsh et al., 2021; Walsh et al., in-press) - were used by LW to create the first draft of a the guide. This draft was reviewed by the co-creation group at a meeting (held via videoconference), who suggested changes to the draft. These changes were integrated into the guide to create the consultation draft. At the pre-consultation stage the co-creation group also planned the consultation approach, developed the recruitment information, and determined the questions to ask in the consultation interviews.
All meetings of the co-creation group were audio-recorded and transcribed by LW, so that the decisions made could be easily captured and discussions analysed.
First design cycle
The draft of the guide was emailed to the consultation participants. Consultation participants were given time to review the guide (typically between two and 4 weeks) before being involved in a semi-structured interview (DeJonckheere & Vaughn, 2019), by telephone or videoconference, to explore their views on the acceptability, usability, implementation and dissemination of the guide. Participants were asked how the guide could be improved, and how to best support implementation of the guide into practice. The interview questions were based on the following characteristics of guidelines which can affect their implementation (Francke et al., 2008; Harrison et al., 2010): (1) ease of understanding; (2) ease of trying out; (3) resource requirements; (4) relevance to the end user; (5) integration into practice; (6) adaptation to local use; and (7) user awareness of guidelines. See Appendix 1 for the interview guide, which includes how each question related to the seven factors outlined above. LW conducted, audio-recorded and transcribed the interviews.
All 18 consultation participants took part in the interviews during the first round of the consultation. Seventeen interviews were held via videoconference, and one interview was held via telephone.
After the first round of the consultation was complete, LW integrated the minor recommended changes to the guide. Any complex or conflicting recommendations were discussed, and solutions decided upon at a meeting of the co-creation group. After these discussions, the agreed changes were integrated into the guide.
Second design cycle
The guide was sent to the consultation participants via email for a second round of feedback and member checking of the synthesised data (Birt et al., 2016). To support this second round of consultation, participants were also sent a document which summarised how their recommendations for change from the first round of the consultation had been addressed. Consultation participants were given the option of providing their second round of feedback via email, telephone or videoconference, or not providing additional feedback at all if they were satisfied with the changes that had been made. Only four participants (all consumer representatives) provided feedback in the second round of the consultation. All second-round feedback was provided as written feedback via email.
After the second consultation round, LW integrated the final changes, and any complex or conflicting recommendations were discussed within the co-creation group via email. The final content of the guide was then sent to the co-creation group for final review and approval. Once the content was finalised, the guide was professionally designed to ensure the final version was visually appealing and easy to navigate. The co-creation group approved the final design of the guide.
Data analysis
The transcriptions and audio-recordings of the co-creation meetings and the consultations interviews, and any additional written comments received by email, were analysed by LW using qualitative deductive content analysis (Elo & Kyngäs, 2008) with an analysis framework based on the characteristics of guidelines which can affect their implementation as outlined above (Francke et al., 2008; Harrison et al., 2010) and other known implementation factors external to how the guideline is written and developed (Francke et al., 2008). The analysis framework is presented in Appendix 2. NVivo 12 was used for data storage, management, and qualitative coding (QSR International, 2018).
Ethics approval
Ethics approvals for this study were given by the La Trobe University Human Research Ethics Committee via two separate but linked applications, Application IDs HEC19075 (co-creation group) and HEC21068 (consultation).
Results
In this section we outline the key activities and outcomes of each stage of the development process, and the recurrent themes which were discussed throughout the development of the guide by both the consultation participants and co-creation group.
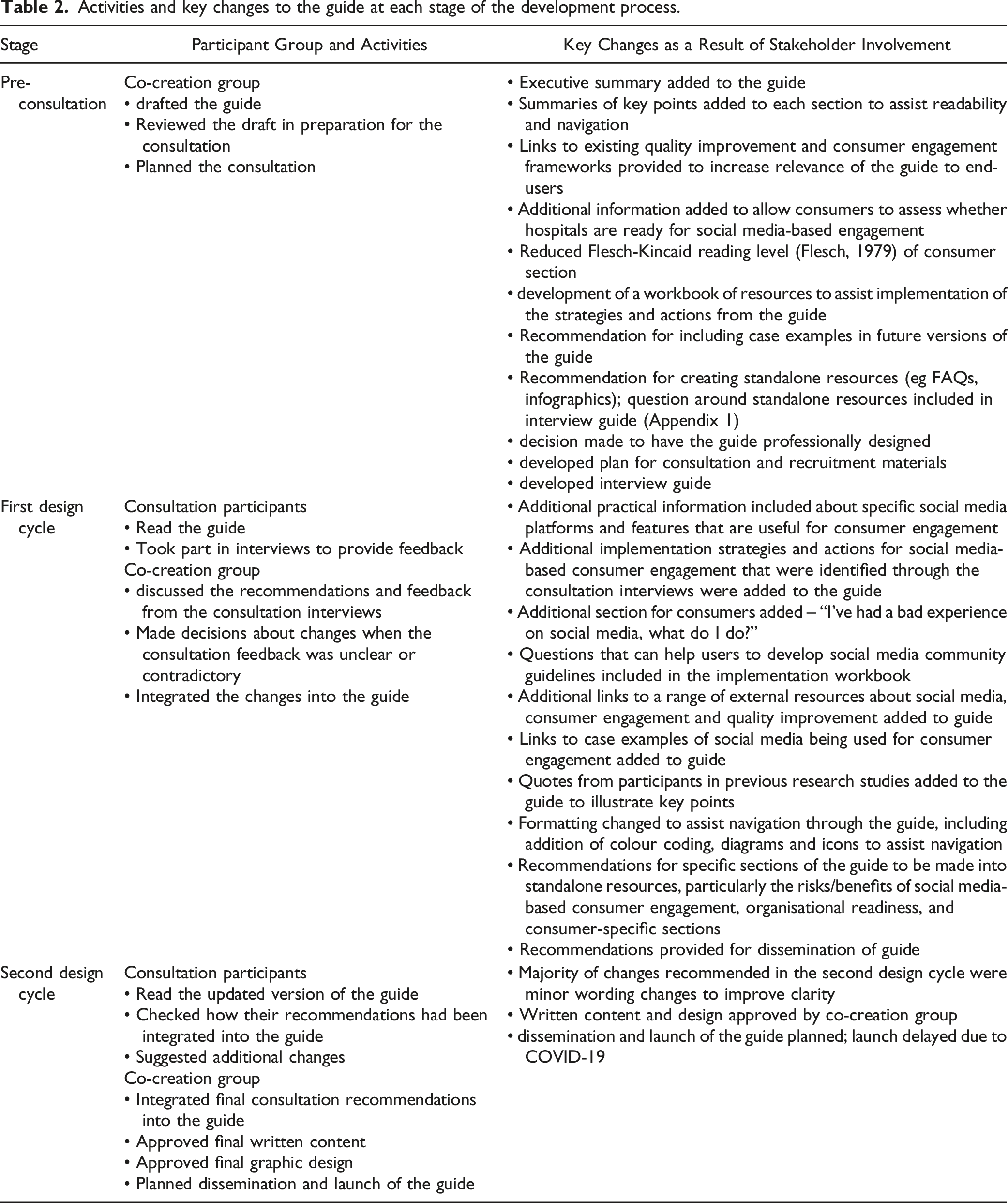
Activities and outcomes of each stage of the guide development process
Activities and key changes to the guide at each stage of the development process.
Recurrent themes throughout the development of the guide
During the cycles of co-creation and consultation there were recurrent themes discussed across both groups. These themes highlighted not only what was important in terms of the guide under development, but also demonstrated how development of a resource can cause people to reflect more broadly on improving consumer engagement within their hospital and implementing new methods of communication and engagement. We identified four key themes, which were: (1) Enhancing usability is critical for guidance resources; (2) Executive support and teamwork are essential for implementation; (3) Start small and build experience and knowledge over time; and (4) Thinking about new methods brings up questions around existing practice. The first theme reflects the need for the guide to be useable by stakeholders, while the other three themes reflect feedback with a focus on enhancing adoption and implementation of the guide.
Where quotes from consultation participants are reported in this section, their participant code has been used to indicate the speaker. The letters in their participant code (CR, CE, CO, QI) correspond to their role (see Table 1). Quotes from co-creation group members use the generic term ‘co-creation group member’ for quotes from any member.
Theme 1: Enhancing usability is critical for guidance resources
In both the co-creation and the consultation groups, most recommended changes to the content of the guide were easily integrated, and were generally highly specific recommendations for social media-based engagement based on their own experiences with social media that had not been captured through previous research (Walsh, Hyett, Howley, et al., 2021; Walsh et al., in-press; Walsh, Hyett, Juniper, et al., 2021). For example, one participant in a communications role (CO4) shared how they had asked one of the hospital speech pathologists to give their team an education session on developing social media posts for people with low English literacy. Another participant, who worked in a consumer engagement role (CE3), talked about how running a highly targeted social media-based consultation caused some “tension” with the communications team at the hospital because it was not meeting their key performance indicators for individual reach of social media posts. Although experiences like these were very specific, they could be integrated into the guide by including advice around connecting with other teams with experience and knowledge around social media, and understanding the priorities and evaluation metrics that are relevant to social media managers.
Most recommended changes were around the usability of the guide. This included recommendations to include colour or pictures to assist navigation through the guide, strategies for reducing its length, consideration of alternative modes of presenting the information, and suggestions for editing the writing to make the guide easier to read. The focus of these discussions was often around increasing accessibility and usability of the guide for a range of audiences.
Usability considerations for consumer audiences were often around simplifying the language in the guide and including colours and pictures to break up the text and improve navigation through the document.
I don’t know if you’re looking at including colour and graphics, especially for the consumer section? … We do a consumer consultative committee, and … we changed how we present the agenda and minutes to our consumers. It’s easier to have graphics, especially considering different levels of health literacy. (CE2, Consultation participant)
I did have a look to see what its readability level was and … it’s still sitting around the twenty mark, and government still works on the low high school range. (Co-creation group member)
Usability considerations for service providers were primarily about the document being long, and the service providers having limited time.
The thing for me about the guide was just how lengthy it was … it raised concerns for me about its usability. I needed to find myself an hour or two to sit down and read it, and … if it takes me that long … no one’s going to pick it up off the shelf. (QI1, Consultation participant)
Feedback on the usability led to a range of solutions, including getting the guide professionally designed with a focus on breaking up the text and using colour to aid navigation, editing the guide to reduce the Flesch-Kincade reading level (Flesch, 1979) and improve the clarity of the writing, and consideration of alternative formats to present the information in the guide alongside the main document (e.g., standalone resources created from different sections of the guide, website).
Theme 2: Executive support and teamwork are essential for implementation
Participants in the consultation were asked questions about what would help them to try out the strategies in the guide or implement social media-based consumer engagement in their organisation. The most frequent responses centred around organisational culture, particularly the attitude of organisational leaders and the interaction between key teams involved in consumer engagement, quality improvement and social media.
The leadership of the hospital was seen as essential for creating a culture where consumer engagement was prioritised and new methods were supported, and for providing the resourcing for consumer engagement.
We’re lucky that our organisation has a CEO that really values consumer engagement, we have a very active CAC [Community Advisory Committee], board members, so I think we’ve been very lucky in terms of the leadership. (CE4, Consultation participant)
A secondary obstacle may be some reluctance at the executive and/or board to really consider this as valid a communication channel as some of our other channels. (CO1, Consultation participant)
I think … you need to make it clearer about executive buy-in. Because any hospital staff reading this, even if they agree with all of it, they know in their hearts that they can’t do any of it without approval from the top. (CR2, Consultation participant)
The other factor that participants saw as key to implementation was creating effective communication pathways between the relevant teams. Some participants talked about feeling isolated from other teams involved in communications, consumer engagement and quality improvement, and this was a barrier to the use of social media as a consumer engagement tool. [The guide] highlights that you need those internal relationships to really function as a fully functioning machine rather than in your own silos. (CO4, Consultation participant)
I think the organisation … needs to have the policies and procedures in place that talk to the issues of de-siloing. … It’s a cross-boundary issue, and that will require executive support to breakdown some of that siloing. (QI1, Consultation participant)
Finally, some participants saw potential in using the guide as a tool to advocate within their organisation for changes to consumer engagement and social media practices, particularly when speaking to hospital leadership.
Everything … in the guide, I would actually like to … really pull it apart and take it to the key stakeholders and say “look, this is definitely an area that we can consider utilising to improve our consumer engagement”. (QI3, Consultation participant)
The emphasis placed on executive support, organisational culture and team building, enabled confident decision-making for inclusion in the guide. Additional perspectives on building effective relationships and organisational readiness for social media-based engagement, alongside internal team communications, illustrated this was important for inclusion in the guide. We also provided details about the risks and benefits of social media-based engagement (Walsh et al., 2021), and gave recommendations around minimising or mitigating known risks to aid decision making around adoption and implementation of social media as a consumer engagement tool.
Theme 3: Start small and build experience and knowledge over time
In discussions about adopting and implementing social media-based consumer engagement methods, consultation participants talked about their experience of starting with small, achievable tasks, and building their experience, knowledge and skills over time.
I think starting off small … and linking to a closed group, … would be a great way to trial the guide. Then start identifying ‘what are the issues, what are risks’ for our health service, then build a policy and procedure from that. (CE2, Consultation participant)
Learning from the experience of others was also seen as important. “Someone else has to be the guinea pig. And then if they’re successful, then it’s like ‘oh, maybe we’ll follow now!’ (CR2, Consultation participant)”
In the guide we encourage users to start with small projects or tasks, and increase their use of social media-based methods as they gain experience in social media-based engagement. We linked the guide to existing resources for engagement, and some case studies of using social media for consumer engagement. We also structured the guide to take readers through the steps of building capacity for social media-based engagement – such as establishing organisational readiness, building a social media community, using social media for information gathering to inform quality improvement projects, and finally using social media for consultation or co-creation activities. We based this approach on the IAP2 spectrum of participation (International Association for Public Participation, 2018), which views consumer engagement as occurring along a spectrum of increasing consumer involvement in, and control over, design and decision making. Using the spectrum to frame the guide reinforced the idea that starting small and building skills and experience over time was an acceptable approach to social media-based engagement, rather than there being a ‘right’ or ‘wrong’ way to do engagement.
Theme 4: Thinking about new methods brings up questions around existing practice
Having the opportunity to consider a new method of using social media to engage consumers in service design and quality improvement activities led to participants in the consultation and the co-creation group examining existing consumer engagement and social media practices in their hospitals.
Some participants in the consultation talked about consumer renumeration for social media activities and the challenge of paying hospital consumer representatives.
We have parts of the service that remunerate, whereas the rest of us don’t, and that in itself is an exclusion. … I don’t necessarily want that perception to be out there that by moving your consultation to online … you don’t remunerate, because that’s not the case at all. (CE1, Consultation participant)
We have a reimbursement policy as well, I know … best practice is that consumers should be paid for their feedback and their time. I don’t know how that works with social media, I think that’s something I’d probably have to think about a bit more. (CE2, Consultation participant)
Reviewing the guide caused some people to reflect on their existing social media policies and practices, and how they could better support consumer engagement.
The conversation earlier got me thinking about our social media policy which is very much … telling staff what to do in a HR [human resources]-based approach. So maybe before we think about doing anything too adventurous in this space we need to start off there and shift our focus to what is possible [for supporting consumer engagement]. (Co-creation group member)
In response to these discussions, we included advice in the guide around updating social media and consumer engagement policies to cover the use of social media for consumer engagement. We also advised users of the guide to update their consumer remuneration policies to include social media-based engagement activities.
Discussion
This article presented the methods and findings of the development of a guide for using social media as a tool for consumer engagement in hospital service design and quality improvement activities. The guide was developed by drawing on findings of previous research (Walsh et al., 2021; Walsh et al., in-press; Walsh et al., 2021) to create a draft version of the guide which was then refined through cycles of small-group co-creation, and broader consultation with key stakeholders who represented end-users of the final guide.
Key to the development of the guide was the co-creation method which encourages design groups to take a health system perspective of problems, views design as a creative practice that has the lived experience of consumers and providers at its core, and values the design process as much as the outcomes (Greenhalgh et al., 2016). By using a consultation method to inform our co-creation method we aimed to gather perspectives on the problem from a broad group of stakeholders to complement the knowledge and experiences of the co-creation group members and inform and aid decision-making. Using this combination of methods, lived experience of consumers and providers informed every stage of the research and led to a number of valuable changes to the guide, ranging from the layout and content, to changes addressing broader and more critical challenges around the use of social media, and hospital practices of consumer engagement and quality improvement. This reinforces the importance of incorporating participatory methods in health services research where the research outcome has a direct impact on consumers and consumers have a right and purpose for being involved (NHMRC, 2016; Ocloo et al., 2017; Ocloo & Matthews, 2016; Shippee et al., 2015).
Three key themes were identified that led to critical changes to the guide which could inform health service implementation strategies for consumer engagement. The key themes revealed the importance of hospital leadership in influencing consumer engagement and quality improvement practices in hospitals, the effectiveness of staged implementation to build skills and confidence in innovative methods of consumer engagement over time, and the need for examination of existing policies and processes around hospital communications, consumer engagement, and consumer renumeration. Use of co-creation with consultation enabled understanding of these challenges and allowed us to address them directly in the guide, enhancing knowledge translation and closing the research to practice gap which can be a major challenge for researchers (Banner et al., 2019; Minogue et al., 2018; Shippee et al., 2015). Without stakeholder involvement, it is likely that many of these real-world implementation considerations would have been missed.
In this study, the majority of recommended changes focused on improving usability elements targeting the various audiences or communities of practice who are all needed to put social media into practice for design or quality improvement purposes. Visual design, language and other usability elements are key components of health information and guidance resources which can reduce health access barriers by making resources easier to read and understand (Chinn, 2017; Nilsen et al., 2006; Office of Disease Prevention and Health Promotion, 2016; Walsh et al., 2019). Although the changes suggested for increasing usability were consistent (increased use of graphics and colour, simplifying language, considering alternative formats for presentation of key sections) the reasons given for the changes were different depending on the audience the participants were considering. Participants believed that consumers who had lower English literacy proficiency would benefit from the changes they were recommending, while service providers would primarily benefit because it would reduce the time needed to engage with the resources. Using co-creation and consultation methods with a range of different stakeholder groups allowed us to better understand the particular access needs of different audiences, which guided changes to content and design to better support accessibility and usability of the guide for all users. In addition, a focus on making information and other health resources more accessible often delivers better user experiences across a broad range of stakeholders – including and beyond groups with known access barriers (Schmutz et al., 2018).
Alongside the importance of executive support, key feedback on the guide from the co-creation and consultation focused on starting small and building skills and experience in social media over time. Involving stakeholders in the development of the guide allowed us to understand their level of knowledge and key concerns around social media, consumer engagement and quality improvement. Their feedback also demonstrated that different individuals and services are at different levels of understanding and implementation related to social media, consumer engagement and quality improvement. These findings reinforced previous research demonstrating that quality improvement and consumer engagement practices can be difficult for service providers and consumers to understand and put into practice (Ayton et al., 2021; Batalden, 2018; Hamilton et al., 2020), and consumers and providers can lack confidence in using social media and technology for engagement activities (Walsh et al., in-press). To address this wide range of understanding and experience, the findings provide support for a capacity building approach to change implementation. A stepped process of smaller changes, for example establishing organisational readiness and creating policies and procedures, building to more complex activities, such as conducting quality improvement by co-design.
The link between executive support and implementation of social media-based consumer engagement described by participants in the consultation, and the need for policies and processes reinforced findings around organisational-level barriers and enablers of social media-based consumer engagement from previous research (Walsh et al., in-press). The consultation also prompted discussions around consumer renumeration, which is an important issue for participatory researchers (Ayton et al., 2021; Cullen & Walsh, 2019; Wilson et al., 2017). For health service researchers, planners and evaluators who consider that consumers are paid to reimburse expenses related to consumer engagement activities (such as travel and parking costs), social media-based engagement may be looked at as a way to reduce costs of engagement because consumers might not have obvious out-of-pocket costs. However, the consultation participants recommended that consumers should not simply be reimbursed for their out-of-pocket costs, but instead renumeration should be associated with consumers sharing their lived experience and expertise, both assets to a health service and for health service research. This is supported by previous research, which recognises remuneration of consumers as one way of demonstrating that consumer input and expertise is valued (Chauhan et al., 2021; McCarron et al., 2020). Through changing the nature of the potentially reimbursable costs of consumer engagement (such as travel and parking) to other costs (such as purchasing devices or internet access), or shifting organisational focus from ‘reimbursement’ of consumers to ‘renumeration’, social media-based engagement may lead to new understandings about why consumers need to be paid for involvement.
Limitations
There were two main limitations of this study. The first was that the sampling methods used did not purposively include people from communities who are known to be under-represented in stakeholder involvement in the development of health guidelines, standards and guidance or health research more broadly (Chauhan et al., 2021; Davis & Farmer, 2017; O'Neill et al., 2014; Ocloo & Matthews, 2016; Wallace et al., 2019) and, while we did collect data on job role and geographic remoteness, we did not collect comprehensive socio-demographic data on race, ethnicity, and indigeneity. While participants did discuss the experiences and needs of some under-represented communities, and some changes to the guide were based on these discussions, it is important to acknowledge that this guide has not been specifically reviewed by or targeted towards people from under-represented groups. Given that stakeholder involvement in developing guidelines, standards and guidance is a potential way to address issues of equity in access and delivery of healthcare (Petkovic et al., 2020; Shi et al., 2014), future research is recommended to gather this data with group representation in the research team.
The second limitation was the small number of participants (n = 4) in the second consultation cycle, and a lack of a mechanism within the study to gauge whether non-tparticipation was due to participants being satisfied with how their feedback had been applied and having no additional feedback, disengagement from the study, or other factors. Low levels of participation in member checking or feedback processes after an initial research interview is common (Thomas, 2017), and even more likely in participatory research such as this which involves ongoing contact with participants (Birt et al., 2016; Thomas, 2017). Additionally, the benefits of these types of feedback processes on the quality of research outcomes remains unclear (Morse, 2015; Thomas, 2017). While understanding the reasons for non-participation beyond the first feedback cycle may help with the design of future consultation, any mechanisms for collecting this data would need to be balanced against ethical issues associated with member checking, such as respecting a participant’s choice to disengage from the research (Thomas, 2017).
Opportunities for research and practice
We believe that this model of small group co-creation informed by a wider consultation with key stakeholders provides a model that other researchers or health services can use when designing guidance resources to support service design or quality improvement.
Now that the guide has been developed opportunities exist for hospitals, service providers and consumers to trial the guide and see how the advice and strategies aid implementation of social media-based consumer engagement in their health services. Alongside this, there are opportunities for researchers to partner with hospitals to examine the experiences and outcomes of social media-based consumer engagement on service design and quality improvement projects. Research examining the outcomes of social media-based consumer engagement activities for hospitals, providers and consumers are particularly important to fill a gap in existing literature (Lloyd et al., 2021; Lowe et al., 2021; Walsh et al., 2021). Research which focuses on the experiences and outcomes of service design and quality improvement activities involving people from communities known to be under-represented in consumer engagement activities (Chauhan et al., 2021; Davis & Farmer, 2017; O'Neill et al., 2014; Ocloo & Matthews, 2016; Wallace et al., 2019) is also warranted.
Conclusion
This article presented the methods and key findings from the development of a guide for hospitals, service providers and consumers seeking to use social media as a consumer engagement tool in service design and quality improvement activities. The development of the guide followed a stakeholder involvement approach from NICE (NICE, 2015). The co-creation and consultation methods led to a wide range of critical changes to the initial draft of the guide, with a focus on changes which would enhance usability and implementation of the guide by hospitals, service providers and consumers. Critical changes included the provision of risk mitigation strategies and additional supporting resources; a focus on relationship building within and between key hospital teams involved in consumer engagement, social media and quality improvement; structuring the guide to support a capacity building approach to social media-based engagement, and making changes to format, layout and writing style. These changes were a direct result of involving stakeholders in the development of the guide through co-creation and consultation methods, which encouraged the participants to use their experience as service providers and consumers to reflect broadly on the content and implementation of the guide, how the guide might impact their health service, and how it could be improved to better support social media-based engagement within their particular setting. This method of involving stakeholders in the development of the guide, may bridge the research to practice gap by increasing the relevance and usability of the guide for end-users (Banner et al., 2019; Minogue et al., 2018; Shippee et al., 2015), which could also increase the likelihood of it being used by health services, providers and consumers (Fretheim et al., 2006; Harrison et al., 2010; Petkovic et al., 2020). Opportunities now exist for the guide to be used in practice by hospitals, service providers and consumers, and for the social media-based engagement activities undertaken using the guide to be evaluated by researchers.
Footnotes
Acknowledgements
The authors wish to thank the participants in the consultation for their contributions to developing the guide.
Authors contributions
All authors were involved in the conception and design of the study, analysed and interpretated the data, and provided feedback on and approved the final version of the manuscript. LW conducted and transcribed the consultation interviews, chaired and transcribed the co-creation group meetings, and drafted the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study forms part of a PhD project funded through the National Health and Medical Research Council Postgraduate Scholarship GNT1168409.
Ethics approval
Ethics approvals for this study were given by the La Trobe University Human Research Ethics Committee via two separate but linked applications, Application IDs HEC19075 (co-creation group) and HEC21068 (consultation).
Interview guide showing how the questions correspond to known factors which affect implementation of clinical guidelines
Implementation Factor (from Franke et al., 2008; Harrison et al. 2010)
Question
Participant profile
What is your gender?
What is your age?
Which hospital do you work in (provider)/act as a consumer representative in (consumer)? Where is the hospital located?
Provider: What is your job title, and can you describe your role?
Consumer: What do you do as part of your representative role(s)?
How have you used social media as a tool for consumer engagement in hospital service design and quality improvement activities? Are these activities taking place at your current hospital?
Ease of understanding
Is the guide easy to understand?
What could be improved?
How could we present this information to make it easier for people to find and use?
Are there any parts of the guide that you think would be useful if made into a brief factsheet or 'how to' guide?
Is there any information missing from the guide that you think would be useful?
Ease of trying out
Which areas or departments of your hospital are currently responsible for consumer engagement activities that happen on social media?
Which strategies or actions in the guide are currently used by you, or your hospital, as part of consumer engagement activities?
Which parts of the guide are different from what you, or your hospital, does now?
Which aspects of the guide could be useful for you, or your hospital, in the future?
Resource requirements
What resources would be required to be able to implement the aspects of the guide you feel would be most useful for your hospital?
Relevance to the end user and integration into practice
How would you use this guide?
Consumer: How do you think that people in a quality improvement/consumer engagement/communications role at your hospital would use this guide?
Provider: How do you think that consumers at your hospital would use this guide? How about someone in quality improvement/consumer engagement/communications role <pick one that is not the provider’s role>?
Adaptation for local use
Are there any other changes that might be needed to make this guide more suitable for your health service?
What would have to happen for your health service to increase their use of social media for consumer engagement?
User awareness of guidelines
Once it’s finalised, how should we promote or share this guide to reach people in other health services?
Theme
Subtheme
Code
Guideline characteristics
Ease of understanding
Formatting
Additional resources
Usability and accessibility
Content changes – new experiences, missing information
Content changes - other
Ease of trying out
Catalysts for trying out
Ways of trying out, implementation strategies
Resource requirements
Time
Staff
Money
Other
Relevance to the end user
Strategies from the guide currently in use
Integration into practice
How consumer representatives would use this guide
How consumer engagement staff would use this guide
How QI staff would use this guide
How communications staff would use this guide
Adaptation to local use
Teams involved in consumer engagement
Opportunities for use at their hospital
Use awareness of guidelines
Dissemination strategies
External factors
Characteristics of organisation/environment
Characteristics of service providers
Characteristics of consumers
General experiences of use
How social media has been used for consumer engagement in QI
Risks, benefits, barriers, enablers