
Abstract
Background
Meaningful engagement with stakeholders in the provision of healthcare and services is recommended by the World Health Organisation. Culturally specific evaluation may enable deeper exploration of the critical views of people living with advanced long-term conditions, their support people, and healthcare providers.
Aim and design
This article describes how critical theory and Actor-Network theory involved all stakeholders including patients with severe chronic obstructive pulmonary disease as expert voices during the evaluation of end-of-life care services.
Results
We describe how critical theory and Actor-Network theory informed the methodologies for focus groups and how stakeholders spoke as critical experts about and in the system. An analytical sample of the focus group study is presented to demonstrate how the frameworks were applied to identify cohesive themes that were inclusive of all stakeholders.
Conclusions
This paper highlights how the evaluation of health systems can include a critical methodological approach to include the values and perspectives of all stakeholders. The outcomes may be used by those who design health systems to develop high-quality services.
Introduction
Health services have previously been designed according to specific disease groups, with limited capacity to address social, psychological, political, and behavioural factors across illnesses. (Hewa & Hetherington, 1995) Inclusion of biopsychosocial factors has progressively enabled a system with additional resources, co-designed by policymakers, providers, and clinicians. (Timmins & Ham, 2013; World Health Organisation, 2018) A further expansion to include broader socio-political determinants of health during health services evaluation has been enabled by qualitative methodologies that include multiple perspectives from all stakeholders in the health system. (GBD 2015 Chronic Respiratory Disease Collaborators, 2017)
Chronic obstructive pulmonary disease (COPD) is a common long-term condition in all global settings. (GBD 2015 Chronic Respiratory Disease Collaborators, 2017) Patients with COPD frequently experience concurrent conditions such as ischaemic heart disease and anxiety and depression, which further impact well-being and disability. (Carmona-Pírez et al., 2021; Putcha et al., 2013) Those with severe COPD describe a slow physical deterioration and learn to live within their limitations. (Pinnock et al., 2011) Specialist palliative care programmes increasingly aim to provide coordinated services to patients and their supporters and families. (Hyden et al., 2020; Payne et al., 2017; Philip et al., 2018) Qualitative critical analysis evaluating the clinician experience of caring for patients with end-stage respiratory illnesses, and patients with COPD alongside their support people, may inform end-of-life services design. (Philip et al., 2018; Timmins & Ham, 2013; World Health Organisation, 2015)
In our systematic review exploring patient, support people, and clinician experiences of end-of-life care for severe COPD, patients reported little influence on their health services. (World Health Organisation, 2015) Based on the systematic review, the aim of our subsequent study was to include the experiences of all stakeholders involved in end-of-life care of COPD to evaluate healthcare delivery. We used critical theory as the lens for analysis, and the Actor-Network theory (ANT) as the framework for synthesising all stakeholder connections in the healthcare system for people with severe COPD. The purpose of our paper is to report how we navigated positioning the perspectives, experiences, and values of patients with advanced COPD, their support people, and health professionals to record critical perspectives of current end-of-life care service delivery.
Context of Research Into End-of-Life Care
Research in end-of-life care requires considerate construction, from the design of a study, application of ethics, and methodological selection, to the context of ill health, and the burden on patients and support people that impact attrition rates. This section will report how our research team accounted for the context of research into end-of-life care including; defining palliative care, the roles of qualitative methodologies, and critical and Actor-Network theory, that informed the framework for our research. Figure 1. visualises how the qualitative methodology aligned with critical and Actor-Network theory in a palliative care research project. Visual depiction of links between qualitative methodology, critical theory and Actor-Network theory.
Definition of Palliative Care
The World Health Organisation (WHO) describes palliative care as a practice that focuses collectively on the physical, emotional, social, and spiritual values of each individual patient, and involves their family and support people. (Sepúlveda et al., 2002) Specialist palliative care services provide complex end-of-life care, including for those with long-term conditions. These services work with the healthcare team to manage symptoms, emotional distress, existential crises, and social problems. Palliative care services were initially designed for the cancer population who may experience a predictable or continuous trajectory of illness. (Fu et al., 2021) Delivering palliative care to patients affected by advanced COPD who may experience fluctuating illness and disability is an emerging priority. (Cramm & Nieboer, 2016; Horton et al., 2013; Philip et al., 2018)
Role of Qualitative Methodology in End-of-Life Research
Many studies have explored the delivery of palliative care services to patients affected by a life-limiting illness. (Carey et al., 2019) These studies have demonstrated the challenges of conducting research in the palliative care setting (Kendall et al., 2007; O'Mara et al., 2009) including defining end-of-life, protecting patients during research (Kendall et al., 2007), and slow recruitment and high attrition rate of participants. (O'Mara et al., 2009). As a consequence, palliative care research is infrequently co-designed with patients and their carers. (Johnson et al., 2021) Qualitative methodologies in end-of-life research can specifically address these challenges. Current qualitative studies of patient experiences at the end-of-life have utilised explorative questions to enhance the understanding by health providers of the barriers and enablers of high-quality care within their systems. (Bailey et al., 2016; Jerpseth et al., 2018; Long et al., 2014)
Qualitative methodologies have also enabled clinicians and researchers to document differences between best practice and the lived consumer experience of healthcare services, communication skills, and cultural safety. (Anne-Mei et al., 2000; Blackhall et al., 1999; Steinhauser et al., 2000) Strengths of a qualitative approach in end-of-life care research include: flexibility to evolve data collection methods according to the needs of participants, creation of safer settings to explore difficult topics, and capacity to hear and incorporate multiple voices. Qualitative approaches such as focus groups have enhanced health services stakeholder collaboration to inform health guidelines and policy. (Hyden et al., 2020; Philip et al., 2018) Qualitative studies that have included experiences of patients, their support people, and health professionals increase the richness of research findings (Burgess et al., 2013), improve researcher commitment to answering research questions, (Fu et al., 2021) and support translation of research findings into practice. (Cooke & Thackray, 2012)
Role of Critical Theory in End-of-Life Care Research
Critical theory can enable stakeholder voices to be translated from research into practice. Specifically, critical theory is an exploration of power in a system; it identifies who holds that power, how it is enabled, how it is resisted, and how power impacts the system. (Oudshoorn et al., 2007) Analysis of the organisation of power and the structures in place can contribute evidence for change that re-orientates systems towards equity, inclusion and justice. Critical theorists are also interested in how social structures have historically been formed, and how they have changed over time. (Meekosha & Shuttleworth, 2009) This historical knowledge, coupled with analysis of the current structures, give context to the health experiences of people with long-term conditions.
In end-of-life COPD care, power has traditionally been located with providers and policymakers, which may be associated with fragmented care, removal of patients and families from decision-making, and low-quality care services. (Anne-Mei et al., 2000; Oudshoorn et al., 2007) Critical theory has been used within palliative care research to highlight that social determinants of health have the highest impact on symptom experiences for patients with cancer. (Salas et al., 2019) A study using critical theory exploring the positioning of palliative care in the management of metastatic melanoma, reported that the health system was confusing for patients to navigate. (Fox et al., 2016) Critical theory has provided insights into how public involvement can inform palliative care policy (Haarsma et al., 2015) showing that health consumers prefer short-term, practical solutions to improve quality of care, while professionals prefer long-term responses.
Our research team has employed critical theory to highlight the socio-political context of participants and to shift power toward those who are traditionally excluded from active participation in healthcare evaluation. (Hockley & Froggatt, 2006) Critical theory aligns with Indigenous-lead research principles as it affirms the participant voice and validates their experience, while attempting to counteract dominant values and understandings. (Haitana et al., 2020) End-of-life care in a chronic condition such as COPD requires multiple interactions and stakeholders working across numerous settings. Critical theory in qualitative end-of-life care research encourages self-reflection which, in turn, overcomes the focus on self and leads to positive changes in society. (Hockley et al., 2013)
Role of Actor-Network Theory in End-of-Life Care Research
Actor-Network theory was developed in the field of science and technology by Latour and colleagues in the 1980’s. (Latour, 1988) The Actor-Network theory upholds the idea that there is equal agency or ability to influence change conferred on both human and non-human entities (actors). The premise is that actors behave the way they do and produce outcomes because of interactions with each other. Understanding the different actors involved in a network allows better planning for quality improvement in systems, policy and organisations. (Desai et al., 2017)
Research has employed the Actor-Network theory to explore how systems exist and control power in relationships, physical resources, and interactions. (Doolin & Lowe, 2002) The Actor-Network theory allows researchers to explore how relationships among people, objects, and resources are forged, distributed, and sustained. (Callon, 1984; Müller, 2015) McDougall et al. used this approach to analyse team-based, inter-professional services for people with advanced heart failure. (McDougall et al., 2016) Actor-Network theory revealed the concept of ‘collaborative entanglement’, a heterogeneous cognitive adaptation that happens between professions to achieve the goals of patient care. Actor-Network theory has also been used to explore how healthcare reforms have translated into higher quality of care for patients by focusing on information on system-level initiatives. (Ribeiro & Senoo, 2021)
Our research team employed the Actor-Network theory to reveal the actors that contributed to the health system for those with end-stage COPD, and their relationships. (Landers et al., 2022) The theory enabled us to analyse all stakeholder experiences within a system that constantly mobilises people across roles, settings, and organisations. This mobilisation occurs at the local and government level and is influenced by inanimate entities such as policies, resources, knowledge, and information technology. (Montenegro & Bulgacov, 2014) The Actor-Network theory enables the identification of facilitators and mechanisms within a health system that may not otherwise have been considered. (Cresswell, 2019)
End-of-Life Care Research Framework
Reflecting on the differences between best practice and lived experiences for those affected by severe COPD, we selected critical theory to explore the power contexts of stakeholders and Actor-Network theory to reveal which stakeholders held the power in the health care system. This research framework underpinned the methodological decisions that were made about study design, recruitment, participation, and community engagement. The research framework encouraged the role of the research to position and validate all voices in the system including patients, support people, health care professionals, and providers. We planned data analysis using coding frameworks aligned with the research framework. The skills and perspectives of a research advisory group helped confirm stakeholder validity of our analysis by reviewing our coding and critique, providing a non-academic viewpoint, and examining for any cultural nuance.
Applying the End-of-Life Care Framework to This Research
Once the research design, methodology, and framework were decided, we focused on ensuring ethics and governance structures were developed to enable social accountability to the research participants. Based on previous clinical and research experience, we attempted to mitigate negative impacts on participants which could be incurred in the discussion of end-of-life topics about death and dying. This included the refinement of: the research aim, the constitution of the research team, study governance, the ethics review process, and the role of social accountability in end-of-life care research. This section will conclude with a clear outline of the methodological approach developed to meet the research aim of this project.
The Research Aim
The aim of our research study to illustrate the chosen research framework was to investigate the patient, support people, and health professional experiences of end-of-life services for severe COPD. We positioned all participants as experts in the system. A primary goal was to validate multiple voices and highlight opportunities for quality improvement in health care.
The Research Team
To enable the validation and central place of the participants’ voices, we chose frameworks that reduced the potential for research bias and promoted reflexivity. Our research team was multidisciplinary with diverse clinical expertise and experience in research methodologies. AL is a palliative care physician with expertise in providing specialist, community-based healthcare, as well as qualitative methods to develop models of care. SGP is an Indigenous researcher with an extensive background in qualitative methodologies investigating multiple stakeholder voices. SCP is a nephrologist with experience in qualitative research and end-of-life renal care and LB is a respiratory physician, with experience in qualitative research centred on chronic respiratory illnesses. We provided constant challenges to one another, broadening the angle of the lens, and iteratively reframing the research methodologies.
The Research Governance
Strategies to mitigate the imposition of previously held beliefs about end-of-life care in COPD by our research team and strategies to enhance social accountability were built into the methodology. This included the provision of a research advisory group as well as clear roles and responsibilities of our research team to support appropriate research governance. The role of the research advisory group was to ensure community stakeholder engagement, participation, and analysis in the research. The research advisory group consisted of a public health physician with a position in hospital funding governance, a respiratory service manager, a Pacific nurse researcher, a Māori (Indigenous) General Practitioner, and a non-Māori academic General Practitioner. The advisory group had input at the project design stage, into the ethics application, and during the recruitment of participants. We followed institutional policies on research consultation with Māori and Pacific engagement and the code of conduct which guides researchers in responsible research practice. These policies prompted the research team to ensure that each member worked to their strengths and to clarify roles within the research. Our research team had discussions on the ethics of studying a population at end-of-life in accordance with University and National guidelines
The Ethics Review Process
Ethical approval was sought from the New Zealand Health and Disability Ethics Committee (HDEC). It is well-documented in the literature that researchers experience challenges in obtaining ethical approval for studies involving populations with life-limiting illness and their support networks. (Kendall et al., 2007; O'Mara et al., 2009; Gardiner et al., 2010) The ethics committee raised concerns for the safety of patients with COPD as the focus was on end-of-life care. The ethics committee felt group discussion about sensitive topics such as death and dying could be harmful to the participants. In response to the ethics committee feedback, we made changes to the patient consent forms to ensure the participants were aware that death and dying may be discussed in the focus groups. The consent process emphasised that we were exploring the experience of health services, rather than personal experiences. The consent form indicated opportunities for participants to include support people, or health workers during participation. Information to participants about the study indicated that the sovereignty of Indigenous information would be upheld and belonged to the participants. A psychologist was engaged to be available to participants following participation. Ethical approval was granted by HDEC after areas of concern were addressed by changes to the research governance and design.
The Role of Social Accountability in End-of-Life Research
The systematic literature review highlighted the main actors in the healthcare network for people with severe COPD. We actively worked to create meaningful engagement and relationships with the relevant healthcare and social communities. We felt there were missing actors in the healthcare network such as aged residential care and cultural providers, so these groups were included. A strategy to connect with a clinician or manager in each of the relevant groups was developed and invites were sent for face-to-face meetings. The lead investigator built and sustained relationships with people in these groups through visits to community organisations, hospital departments, and patient support groups. The research question and findings of the systematic literature review were discussed with health providers, and their managers in each relevant department or organisation. AL also participated in six community COPD support groups and discussed with attendees the study and aims of the research.
These relationships promoted social accountability to participants and identified who would be appropriate facilitators, including ensuring cultural concordance with the Māori and Pacific focus groups. The process of accountability led to the adoption of recruitment methods with layers of support for each focus group, with awareness of cultural expectations and inequities in health service delivery and outcomes. As focus groups asked participants to discuss sensitive topics with people they did not know, we used strategies informed by healthcare networks to create a potentially safer environment for the participants to provide critical perspectives. These strategies included offering participants a choice of venue, inviting participants to bring support people, and providing free counselling if required. Medical support was available at each patient focus group to assist with any medical issues present during the research conduct.
Participants reported they felt safe during the focus group to share their experiences and perspectives on end-of-life care. The data gained from the focus groups identified a rich exchange of information and the development of new relationships between participants. The facilitator summarising the general themes from the focus group and seeking ratification from the participants at the end of each focus group was identified as a strength of the process by co-facilitators.
The process of engagement with the healthcare network also influenced the way data were collected and analysed. The participants themselves advocated for the importance of the stakeholder’s voices as the centre of the narrative. This provided a framework by which we actively reviewed their analysis and critiqued the integrity of their processes. This analysis was then presented to the research advisory group for further feedback.
The Research Methodology
We sought a framework by which to construct and shape the research design that would build on previous qualitative research. The Interactive Model of Research Design had previously aided researchers to reflect on five components of study design; the research question, goals, methods, validity, and conceptual framework (Figure 2). (Maxwell, 2012) An interactive model of research design adapted from Maxwell et al. with permission.
Maxwell et al. expanded the elements further by looking at the environment within which each of the components is framed. The model guided our research team to consider whether all components of our proposed study were interconnected in a flexible and meaningful way. The lead investigator (AL) systematically looked at each element of the model of research design and applied it to the qualitative study design and implementation of this proposed research (Figure 3). The framework assisted us to focus on the central role of the research question and its relationship to the overall goal, the method chosen, research validity, and the conceptual frameworks already in existence. The researchers were unable to find any examples of the Maxwell model being utilised in palliative care research. The result of the amended Maxwell model was the development of the ‘interactive model‘, which formed the framework for the design, development, recruitment, implementation, analysis, and dissemination of this research. An interactive design of qualitative research in the experience of end-of-life care in COPD adapted from Maxwell (The new model also provided us with confidence that the research would provide the context and sensitivity to address the study aim of exploring stakeholder experiences of end-of-life care in COPD.
End-of-Life Care Methods Utilised in This Research
Recruitment of participants posed some challenges and the difficulties encountered will be outlined in this section. The role of focus groups in this research is described, as well as the approach to data collection. The methods of data analysis are summarised including each cycle of coding and an example of outcomes has been included.
Participant Recruitment
For several months prior to the focus groups, the lead investigator (AL) built relationships with key stakeholders involved in caring for people with end-stage COPD including primary and secondary care services, patient support groups, organisations, Indigenous providers, and representatives of various medical specialties. Recruitment of participants also occurred through Māori and Pacific health researchers and service providers. Driven by community requests, the planned support people focus group transformed into a bereavement group. This had not previously been considered but it allowed the exploration of a post-system critique.
Health professionals in secondary care had numerous colleagues and friends in their focus groups. A co-facilitator not known to the participants enabled frank discussion about organisations and services, without pressure to be positive. Health professionals working in the community were recruited to include participants with a wide range of qualifications, roles, and services.
People with severe COPD were recruited along with their family, friends, and support network. At the beginning of the study, the international GOLD guidelines defined severe COPD as having a forced expiratory volume (FEV1) of less than 40%. An updated version defined severe COPD defined it as having an FEV1 of less than 50% predicted. We adjusted the inclusion criteria to the new guidelines (Landers et al., 2022).
We needed to access clinical information before the focus groups to check eligibility. At times it was not possible to gain verbal consent for this prior to recruitment. That was particularly relevant in the community group and when participants bought others with COPD on the day. This led to a small number of people participating without severe COPD as defined by the GOLD criteria, including one in the Māori focus group who was from the Cook Islands.
Electronic versions of the consent forms and a demographic questionnaire were sent to those who supplied an email address. People with COPD were also asked to complete a COPD Assessment Tool survey as a routine test to quantify the severity of their current symptoms. (Jones, 2013) Those without access to devices were sent these forms through the post. The Pacific group requested for the consent forms be completed on the day. This allowed for the interpretation of the consent and questionnaires by the Pacific nurse researcher who co-facilitated the focus group. It also allowed ample time for questions and enhanced the rapport with this focus group. Refreshments and a gift voucher ($40NZD) were given to all the participants to acknowledge the value we placed on their time and expertise.
The Role of Focus Groups in End-of-Life Care Research
Focus groups assist, “group discussions exploring a set of specific issues that are focused because the process involves some collective activity”. (Kitzinger, 1994) In this research, the collective activity was debating a set of three questions about a model of healthcare. Focus group conversation considers both the similarities of individual experiences and their differences. The discussion gives priority to their language, their perceptions, and the way they view the care of people with severe COPD.
The focus group lead facilitator (AL) was trained by SGP. Each focus group was led by the most appropriate member of the research team or associate to increase the cultural safety of the discussion. The Māori group was led by SGP, an Indigenous researcher. A senior Pacific nurse facilitated the Pacific focus group with the lead researcher co-facilitating both sessions. A primary care clinician and member of the research advisory group co-facilitated the community health professional group.
A semi-structured interview schedule (Supplement One) was informed by a systematic literature review of the research question and discussed with Māori researchers. As the topic of end-of-life care is potentially sensitive, patients were encouraged to invite family members and key health workers to the focus group sessions. This layer of support increased familiarity and camaraderie between patients and their supporters which strengthened the interaction of the participants. All sessions were started with instructions and the message that the research question placed them as the experts in the model of care. A brief 3-min presentation (Supplement Two) was delivered by the same researcher (AL) in each session outlining the systematic literature review findings that led to the researchers understanding of the current healthcare network model of care (Supplement Three). Any questions raised by the presentation were answered and then the recording began. Sessions were conducted informally with minimal intervention from the facilitators.
The Data Collection
Characteristics of Participants Across the Seven Focus Groups n = 74.
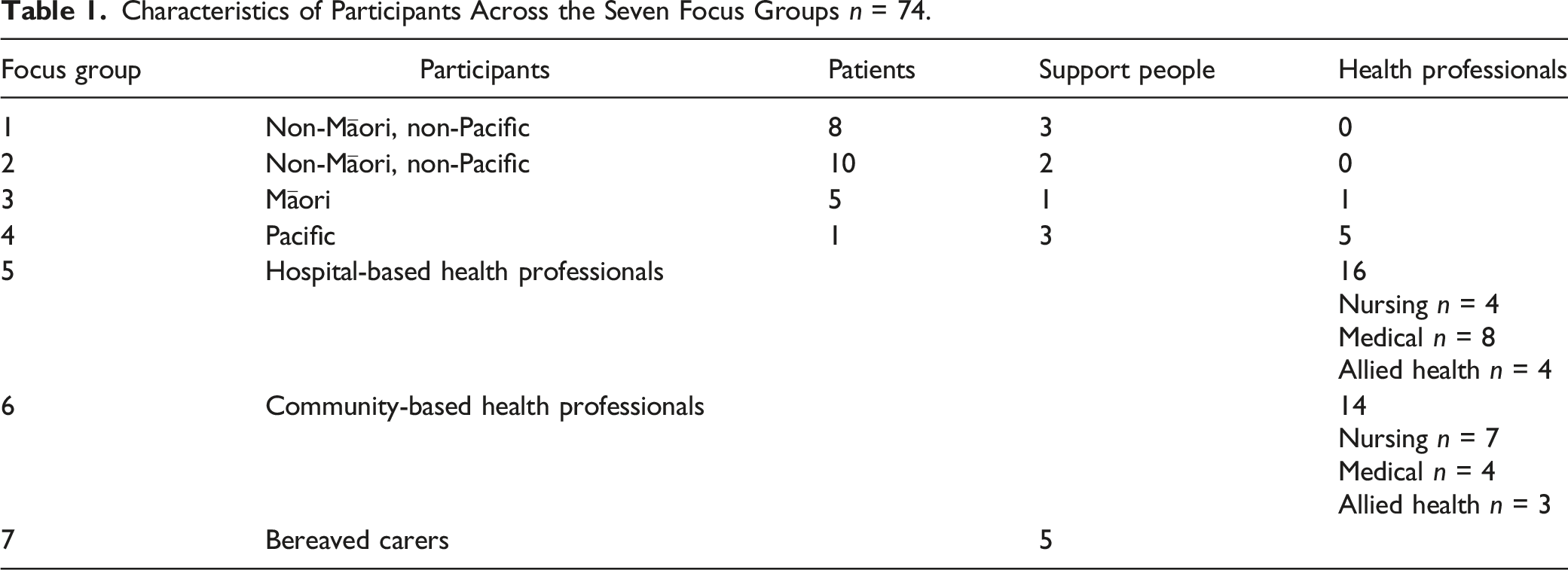
Participants within focus groups (except the bereaved group) were identified to have previously met each other through health system interactions (including support groups). Previous interactions had built trust within the group prior to the focus group questions. Although the bereaved carers had never met one another before the session, the retelling of shared experiences built rapport between members of the group. Field notes documented laughter, joking, banter, and tears.
The Research Analysis
Audio recordings of each focus group were transcribed by a professional agency and checked for accuracy by the lead investigator (AL). The process of reviewing the transcripts also supported the lead investigator to review tone and pace that assisted in identifying key points participants were highlighting as of importance to them, which was not necessarily obvious within the scripts alone. Further notes were then added to enhanced field notes.
Our research team utilised coding procedures outlined in Saldaña (Cresswell, 2019) to analyse the transcripts. Saldana offers a variety of lenses with which to approach the data, each with a potentially different outcome. We employed Critical Theory and Actor-Network theory to guide analysis. These frameworks informed coding methods that focused on how participants talked about systems and structures.
Coding categorised the transcripts using a word, phrase, or paragraph. Codes were then clustered together into categories to illustrate patterns and relationships. We agreed on inclusion and exclusion criteria for each code to ensure they were reproducible. Categories were then merged into themes, with clear definitions and inclusion criteria to centre and align participant voices with the analytical framework. An example of these themes is ‘compassion’ defined as being aware of, and responding to the suffering and distress of others. The inclusion criteria included aspects of compassion which strengthened the healthcare network such as listening, and those aspects which disrupted the network such as the undermining of trust. Further examples are available in our publication exploring the aspects of care delivery that lead to high-quality services. (Landers et al., 2023)
The first cycle of coding involved structural and descriptive coding informed by critical theory and Actor-Network theory. We used structural coding to categorise and catalogue relevant data in response to the research question. Our five structural codes were thus aligned to critical theory and Actor-Network theory: the context of participants, disconnection in the network, healthcare environment, integration, and the expert voice.
Descriptive codes then summarised related data into topics for further enquiry. After reviewing the five structural code transcripts, we grouped the data into three descriptive codes. Three descriptive codes were: the health system, patients’/support landscape, and health providers’ landscape. Each code contained data from the structural codes.
Example of Coding Cycles.

Discussion
Key Findings
This paper outlines a methodology that positioned those with severe COPD, their support people, and health professionals as experts in the evaluation of end-of-life healthcare services. The research paradigms of critical theory and Actor-Network theory were utilised to explore the network of healthcare as experienced by stakeholders. The critical theory paradigm created a shared language among groups and enabled a high-level view of systems and structures by stakeholders within the system.
The use of qualitative methodologies was successfully employed to explore the experiences of end-of-life care services for patients, support people, and health professionals. The research paradigms of critical theory and Actor-Network theory offered a framework to investigate these services in a large region of New Zealand. The stakeholder perspectives were weighted equally during the analysis, enabling the exploration of a complex healthcare system. This qualitative approach is aligned with the WHO palliative care indicators through the empowerment of individuals, families, and communities to partner with health and social services in decision-making about health needs. Our research begins the process for people with severe COPD in New Zealand and may guide health planners with a vision for future services.
The application of Maxwell’s interactive model of research design allowed us to ensure study design was relevant, focused, and answered the question at the heart of the model. The research model also provided a framework to check every aspect of decision-making. Adapting the model to our research question helped us conceptualise how our findings may fit in the broad landscape of non-malignant palliative care and service provision.
Limitations and Recommendations
Limitations include a lack of empirical data about how participants experienced this research, including the lack of ethnicity inclusivity in research participation.
Conclusion
Qualitiative research is a valuable methodology when prioritising the voices of patients, their support people and health professionals in designing end-of-life care service delivery. The use of a framework such as Maxwell’s interactive model of research design is beneficial in crystallising all aspects of investigating a research question in palliative care. The stakeholder perspectives of end-of-life for those with COPD challenges those in health care design to look outside of the biomedical model and reframes the value placed on all elements of the wider network. Together, it may be possible to strengthen the healthcare network for those with severe COPD, their carers and those who help care for them across the health and social network.
Supplemental Material
Supplemental Material - Positioning Stakeholder Perspectives in COPD End-of-Life Care Using Critical Theory and Actor-Network Theory: A Methodological Approach
Supplemental Material for Positioning Stakeholder Perspectives in COPD End-of-Life Care Using Critical Theory and Actor-Network Theory: A Methodological Approach by Amanda Landers, Suzanne G. Pitama, Suetonia C. Palmer, and Lutz Beckert in International Journal of Qualitative Methods.
Supplemental Material
Supplemental Material - Positioning Stakeholder Perspectives in COPD End-of-Life Care Using Critical Theory and Actor-Network Theory: A Methodological Approach
Supplemental Material for Positioning Stakeholder Perspectives in COPD End-of-Life Care Using Critical Theory and Actor-Network Theory: A Methodological Approach by Amanda Landers, Suzanne G. Pitama, Suetonia C. Palmer, and Lutz Beckert in International Journal of Qualitative Methods.
Supplemental Material
Supplemental Material - Positioning Stakeholder Perspectives in COPD End-of-Life Care Using Critical Theory and Actor-Network Theory: A Methodological Approach
Supplemental Material for Positioning Stakeholder Perspectives in COPD End-of-Life Care Using Critical Theory and Actor-Network Theory: A Methodological Approach by Amanda Landers, Suzanne G. Pitama, Suetonia C. Palmer, and Lutz Beckert in International Journal of Qualitative Methods.
Footnotes
Acknowledgements
The authors acknowledge the time and energy of all participants in this study. The team thanks Dr Margot De Koning Gans, Suli Tuitaupe and Dr Ben Hudson for assisting with participant recruitment and focus group facilitation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been funded by the Health Research Council of New Zealand (20/023).
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.