
Abstract
This paper considers the effectiveness of narrative inquiry as a research method in collecting and analyzing stories from a purposive sample of intensive care nurses and doctors, regarding their perceptions of the factors that influence decision-making in relation to the withdrawal of life sustaining treatment. Delaying the withdrawal of treatment when it is clearly indicated, may result in unnecessary patient suffering at the end of life, distress for the family as well as moral distress for staff. In narrative inquiry participants’ first-hand accounts of their experiences are told through story; the focus of analysis is the story, with the story becoming the object of investigation. Initially, participants’ stories were restoried to produce narratives that were co-constructed between researcher and participant. Narrative analysis, employing McCormack’s lenses and the interconnected analytical lenses, facilitated vertical analysis of each narrative. Horizontal analysis through thematic analysis facilitated the derivation of themes that were consistent within or across narratives. We detail here how narrative inquiry methodology was effective in revealing the meaning participants gave to their decision-making experiences through story, offering a broader understanding of the factors that impact on decision-making regarding the withdrawal of life-sustaining treatment. The study’s findings were powerful, derived from narratives rich and thick in description, depicting a multi-dimensional interpretation of the participants’ perceptions of their decision-making experiences. Participants experienced transformative learning through the narrative process, which led to changes in ways of working in the study setting. Recommendations arose to enhance clinical practice and education in this vital area of practice as a result of this study. The application of narrative inquiry enabled the discovery of significant findings as an avenue to challenge legislation and current opinion regarding the autonomy and role of the family in decision-making.
Keywords
Introduction and Background
Critically ill patients are admitted to the intensive care unit (ICU) to alleviate suffering while preserving or restoring quality of life (Holms et al., 2014; Truog et al., 2008). Paradoxically, sustaining life may increase suffering and alleviating suffering may require abandoning efforts to sustain life (Holms et al., 2014; Truog et al., 2008). When it is recognized that the death of an ICU patient is the inevitable outcome, it is a general precept that there should be a transition to comfort care, with the removal of life-sustaining treatments. This process ensures the last minutes, hours, or days of life, are as comfortable as possible for the patient (Curtis, 2005; Lanken et al., 2008). Several factors may inhibit this approach, at times leading to a protracted dying process which may cause unnecessary suffering for the patient (Holms et al., 2014), distress to their family, and moral distress for the staff providing care (Gourgiotis & Aloizos, 2013; McLeod, 2014). There is also potential for professional conflict, as the differing attitudes and beliefs between health professionals in relation to the initiation of end-of-life (EoL) care are revealed during decision making (van der Riet et al., 2009).
Administering non-curative, burdensome treatment to dying patients has been found to dominate ICU nurses’ moral concerns (Cronqvist et al., 2004; Wiegand & Funk, 2012). Decisions relating to the withdrawal of life-sustaining treatment (WLST) precede most deaths in ICU, but this area of practice has been exemplified as one of the most difficult, anxiety-provoking, emotional burdens for an ICU team and is fraught with challenges and conflict (Gourgiotis & Aloizos, 2013; Hamric & Blackhall, 2007). This is of major significance because there is only one opportunity to ensure EoL decisions and care are appropriate for each individual.
The aim of the study was to explore ICU nurses’ and doctors’ experiences of decision making surrounding WLST, with a view to deep exploration of the factors that influence decision making and the process of WLST in the study setting.
The purpose of this paper is to describe and critically evaluate the effectiveness of narrative inquiry, to reveal how practice could change to support staff in making difficult decisions and then implementing the decision to withdraw life-sustaining treatment.
Narrative Inquiry
As death, dying and WLST could be viewed as social constructs, the theoretical foundation for the study was social construction theory. In common with social constructionism, narrative inquiry reveals the meaning of experiences through telling and retelling stories in a continual process of interpretation and construction of those lived experiences; thus, reality is created through language (Riessman, 1990). The underpinning principles of social construction theory are related to the interpretivist paradigm. The qualitative paradigm employed for this study enabled the exploration of experiences, in the form of stories told by nurses and doctors in an Australian ICU. The participant doctors were all senior intensivists i.e. doctors specializing in intensive care medicine. The stories provided the vehicle for consideration of the factors influencing decision-making and the process of WLST in the study setting.
This subjective epistemological perspective (how the phenomenon is known/understood) is congruent with the values of interpretivism (Finlay & Ballinger, 2006). Underpinning this research, the ontological perspective (the nature of knowledge or understanding), was congruent with the conventions of critical realism, which asserts that the world is experienced and construed in subjective and individual ways (Ritchie & Lewis, 2007); hence, “reality” is conceived in a relative manner (Sim & Wright, 2002). Epistemological and ontological principles steer the methodological approach (what knowledge the researcher seeks and how that knowledge is generated) of the researcher (Guba, 1990).
The emphasis of interpretivism and critical realism relates to the understanding of multiple interpretations of the world (Finlay & Ballinger, 2006). The focus of the study therefore aligned with the principles associated with critical realism, in which reality exists independently of subjective values and beliefs. It was considered that the current practice of WLST as a reality and the factors that influence decision-making and the process of WLST required exploration by comparing and contrasting multiple stories told by participants, which could then be considered from a shared lens (Ritchie & Lewis, 2007). Using and correlating multiple theoretical strategies in qualitative research, provides theory triangulation (Denzin, 2009). This theoretical overview is summarized in Figure 1.
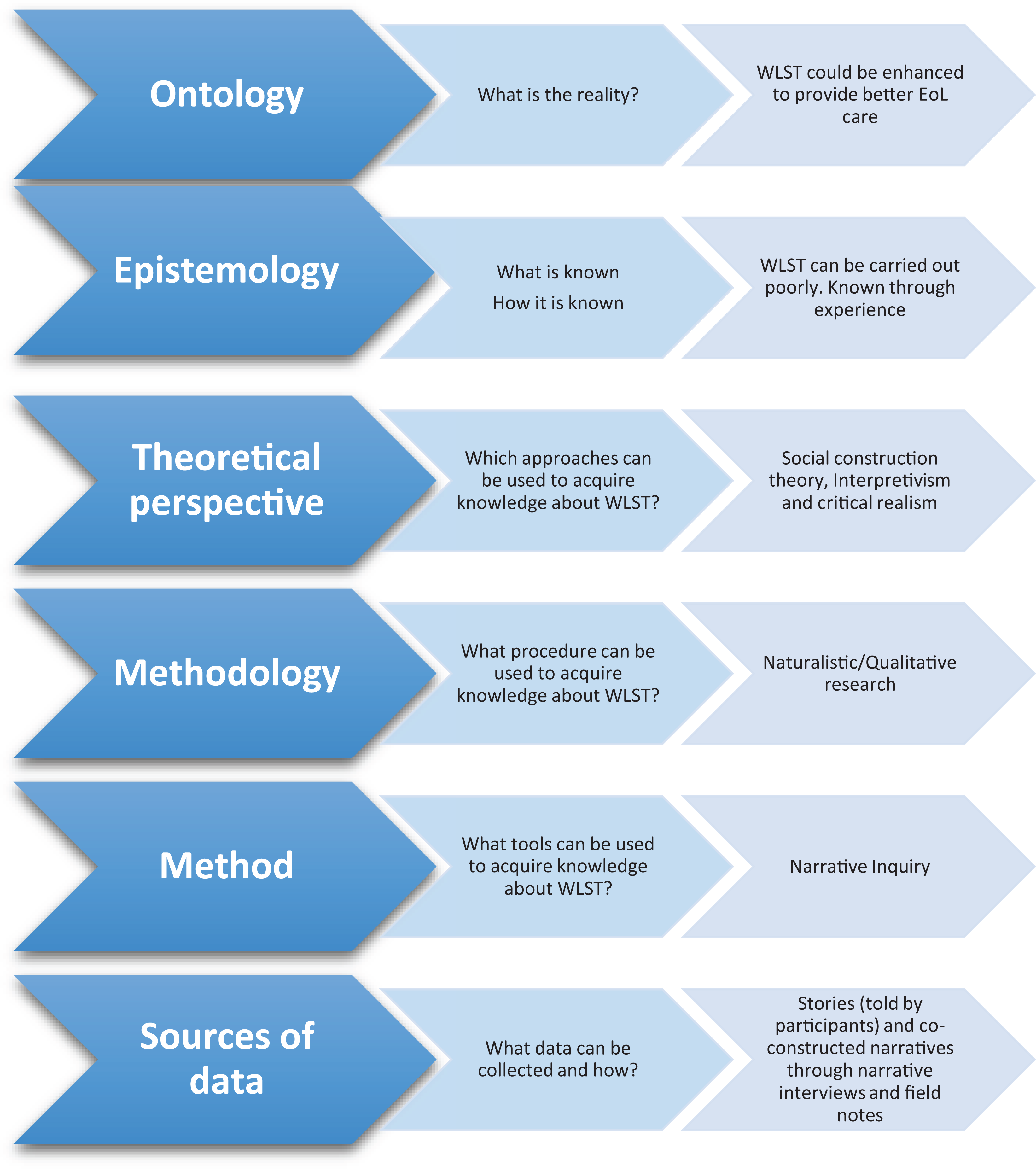
The relationship between the epistemological, ontological and methodological assumptions applied to this study.
The extant research into WLST has taken both quantitative (Mark et al., 2015; McPherson et al., 2019) and qualitative approaches (Adams et al., 2011; Anderson et al., 2019). Little is known about doctors’ experiences related to EoL care in ICU as previous research in this area has focused upon the experience of nurses, particularly within qualitative research (Donnelly & Psirides, 2015). Therefore, in addition to nurses, senior intensivists were included in this study to consider the factors that influence the decision-making process from their perspective, as it is they who can more easily drive change in this area of practice. While nursing research into EoL care in the ICU is more likely to be qualitative in nature (Donnelly & Psirides, 2015; Sibbald et al., 2007; Silén et al., 2008), the use of narrative inquiry within this area of research is rare (Haydon & van der Riet, 2017). It was considered using narrative inquiry may provide a different lens into this area of practice.
Narrative inquiry is a form of qualitative research, grounded in interpretive hermeneutics and phenomenology (Gregory, 2010), and conceptually linked to social construction theory (Bohm, 1996; Galbin, 2014; Gergen, 2005; Santos, 2015) and provides a valuable construct for gaining an in-depth understanding of the complexities of participants’ experiences through reflection (Fontana & Frey, 2008). In narrative inquiry participants’ first-hand accounts of their experiences are told as a story (Connelly & Clandinin, 2006; Holloway & Galvin, 2017), the focus of analysis is the story, with the story becoming the object of investigation (Connelly & Clandinin, 2006; Polit & Beck, 2010; Riessman, 1993). Therefore, narrative inquiry is both the phenomenon and the method of study (Pinnegar & Daynes, 2007).
Narrative inquiry was chosen because life experience is complex and contradictory, and as a method is well suited to laying bare that complexity and contradiction (Clandinin & Connelly, 2000; Creswell, 2013). Narrative inquiry is based firmly in the premise that as human beings we come to understand and give meaning to our lives through story. So narrative inquiry is the study of the activities involved in generating and analyzing stories of life experiences and reporting the results (Creswell, 2013). East et al. (2010) suggest that as health care professionals, nurses and doctors are often exposed to tragedy and human adversity and for this reason, using storytelling within a narrative inquiry framework can be valuable in developing greater understanding of human experience. East et al. (2010) suggested that values and emotions are articulated in personal stories and differences and similarities between people’s experiences can therefore be illuminated.
It was anticipated that encouraging the free flow of participants’ stories and analyzing those stories would be more informative than asking a set of pre-determined questions. Hence, the study was grounded in narrative inquiry to elicit stories that would represent the experiences of senior ICU nurses and senior intensivists relating to WLST. Narrative inquiry facilitated an exploration and deep understanding of the factors that influenced decision-making and the process of WLST. During the interviews, participants were encouraged to detail their stories of WLST while considering the factors that influenced their own decision-making, or those also involved in the process, including a description of the sequence of events leading to the withdrawal of treatment from a patient in their care, to create a whole story.
The Research Puzzle
According to Clandinin and Connelly (2000), when using narrative inquiry, a research puzzle should be framed to enable the inquirer to think narratively about the phenomena under study. Each study using narrative inquiry considers what Clandinin and Connelly (2000) describe as a particular wonder, therefore there can be no precise definition, single expectation of an answer, or single truth (Clandinin, 2013).
In reporting their research, narrative researchers may interlace their own subjective experiences or story along with the stories that they tell of their participants’ experiences (Creswell, 2013). In this study, the lead researcher provided a personal framing of the “particular wonder” to be investigated, which in this instance formed the basis of the research puzzle (Clandinin & Connelly, 2000). The researchers drew on their many years of experience in ICU nursing to frame the research puzzle. The issues contributing to this puzzle were: Critically ill patients are admitted to ICU to receive life-sustaining treatment but, lives cannot always be saved. When it is inevitable that a patient is dying, there should be a transition to comfort care, with the removal of all non-comfort treatments, to ensure the last hours of life are as comfortable as possible. Several factors may inhibit this approach at times, for example, family dissent, conflict between medical teams, failing to recognize dying, leading to a protracted dying process, potentially causing unnecessary suffering. This can cause unnecessary distress to the patient’s family and the staff caring for the patient may also suffer moral distress, potentially leading to professional conflict, which may result from differing ethical perspectives between nurses and doctors. Such a situation is incongruous with quality end-of-life care, so how can it be tolerated?
In considering this research puzzle, one overriding research question arose: what are the factors that influence decision-making relating to WLST in ICU? To answer this question and solve the puzzle about the factors that influence decision-making relating to WLST in ICU, it was necessary to consider WLST and the issues it raises from various perspectives. It was anticipated that this would reveal the factors that influence decision-making and the process of WLST, providing enlightenment about what inhibits the transition to comfort care, when it is clearly appropriate. This study sought to treat the narratives in the manner suggested by Polkinghorne (1988), by describing and explaining individual narratives of life episodes (relating to WLST) and consider the relationships between stories and thus, how such events prevailed over, cohered with, or conflicted with other storylines. This would emphasize the temporal, social and spatial experiences of participants, important in narrative inquiry (Haydon & van der Riet, 2017).
Sampling and Recruitment
A purposive sample of five senior registered nurses and five senior intensivists was recruited in 2018, from an ICU at a tertiary public-sector hospital in a metropolitan area of Australia. All participants had significant experience in caring for patients from whom life-sustaining treatment had been withdrawn.
Ethical Considerations
Ethical approval was granted from the participating hospital and university human research ethics committees (HREC approval number: 2015-127) and all participants provided informed written consent.
Data Collection
Triangulation of data is the use of multiple sources of evidence to determine the credibility of a study’s findings, themes, or perspectives (Creswell, 2008; Stavros & Westberg, 2009). Qualitative data can be considered from an emic (insider’s) and/or etic (outsider’s) perspective (Polit & Beck, 2010). A variety of data were collected for the study, including participants’ narratives developed from narrative interviews, conversations, email correspondence and field notes (emic perspective). Further interpretive stories were written to gain a deeper understanding of the narratives (etic perspective) from the researchers’ perspective, as well as a reflective journal. A summary of each narrative and interpretive story was tabulated, highlighting the significant issues within each narrative.
Narrative Interviews
Each interview commenced with a preamble to determine demographic data and to allow the participant to settle in to the interview and to be at ease with the researcher. Each participant was then requested to recount a story (or stories) about a situation related to WLST in ICU in which they had been involved. Participants were invited to tell stories that were meaningful for them and to describe the events that led to the de-escalation or withdrawal of treatment. They were also asked to reveal how the process of WLST was implemented and how, in view of their ethical values, they were affected on both a personal and professional level throughout the event. It was anticipated this would create understanding of the factors that influence their own decision-making, or those involved in the decision-making process.
Each participant was interviewed once by the lead researcher, with the offer of further face-to-face interviews being declined. Follow-up conversations occurred by telephone and/or email, to ensure participants had sufficient time to reflect upon, add to or alter their stories.
Each participant was encouraged to talk freely; the interviewer only intervened to summarize as stories unfolded and, where appropriate to probe with further questions appropriate to the story being told. Several participants stated that the interview afforded an opportunity to debrief and was at times, cathartic. Indeed, Bruce et al. (2018, p. 560) highlighted the therapeutic benefits of storytelling, including “enriched meaning-making, emotional conveyance, and therapeutic connections between storytellers and listeners.” Some participants also stated that the opportunity to reflect on the situations discussed had prompted them to consider enhancements to practice, and that their reflection provided the impetus to potentially drive change in EoL care in the study ICU.
Field Notes and Reflective Journal
Field notes were used to capture additional information during data collection and were invaluable during the data analysis process. During the interviews scant notes were made but as soon after each interview as possible, detailed information was entered into field notes. These related to thoughts and impressions of the participants’ stories, the discussion, the level of interaction, language use, expressiveness, body language, non-verbal cues, evident emotions and attitudes.
A journal was maintained to capture the researcher’s thoughts, feelings, and reflections throughout the research journey, which increased consciousness of subjective perspectives, and how to avoid such perspectives affecting the research process. The field notes and the reflective journal both aided triangulation of data, adding context and richness to the data that may not have been captured in an audio-recording and interview transcription and thus, the credibility of the project findings was enhanced.
Data Analysis
The method of analysis adopted to analyze data collected from narrative interviews must enhance the ability to capture the truthful essence of the experience and the data analysis technique must render the data accessible to the reader while retaining the original intent of the story (Dibley, 2011). Clandinin and Connelly (2000) highlighted that narrative is viewed as a whole and does not therefore require theming or categorization, rather, they discuss threads within narratives. However, Jones (2004) emphasizes that narrative approaches paradoxically, uncover common ground by expressing individual differences, and this occurred during this study. Perhaps as a result of participant nurses and doctors being asked to narrate stories of the same phenomenon perceived from individual perspectives; themes inevitably arose. Additionally, “narrative researchers treat stories as data and use analysis to arrive at themes that illuminate the content and hold within or across stories” (Ellis, 2004, p. 196).
Narrative interviews generate stories which Muylaert et al. (2014) suggested can be analyzed in different ways, although they state that the interpretation of narratives remains a challenge to researchers, as there are many different methods for analyzing narratives. Kim (2015) asserted that “flirting” with data allows data analysis methods to be adapted and modified to address individual research designs and purposes. Flirtation, in this context, refers to the consideration of new ideas without being influenced by our wishes (Phillips, 1994). It is therefore incumbent on the researcher to present the data analysis methods in detail.
There were four stages of data analysis (Figure 2). Of note, a conscious decision was made to manually analyze the data rather than using a data management system, in order to experience data immersion and to further develop analytical expertise.

Stages of data analysis.
Vertical Analysis
Vertical analysis involves the in-depth analysis of individual stories (Reid et al., 2014), although significant commonalities and insight across stories may begin to appear at this stage.
Stage One of the Data Analysis Process—Restorying
When analyzing narratives, “subject positions, social locations, interpretations, and personal experiences” are examined “through the refracted medium of narrators’ voices” (Chase, 2005, p. 666). This process entails rewriting, reorganizing and retelling the stories such that key elements are analyzed and chronologically sequenced, into a coherent whole (Ollerenshaw & Creswell, 2002; Polkinghorne, 1988). Restorying also enables the reader to understand what happened and why (Kim, 2015, p. 197).
Narrative smoothing is a method used to convert raw data into a coherent, engaging, and interesting story (Kim, 2015). Spence (1986) highlighted that such smoothing can lead to the provision of a good story but that it may be quite different to the original story and therefore not a faithful account. Co-constructing the narratives with participants negated this possibility and ensured faithful representations of participants’ stories.
Restorying comprised replaying the audiotaped interviews, verbatim transcription and note-taking, enabling a deeper understanding of the stories. This ensured that the meaning or emotional context of the participants’ words were discerned; for example, laughter, sarcasm, emphasis, hesitancy, humor, sadness, frustration, passion and even anger laced the spoken word.
The transcriptions were then rewritten and edited where necessary to form written narratives (Kim, 2015; Ollerenshaw & Creswell, 2002). Many elements of the participants’ experiences and the factors influencing decision-making were intertwined throughout the transcriptions, e.g. stories of specific patients, emotional effects of the WLST event and their consequences, practical issues, ethical issues, with each element rearranged to create a chronological and logical format. All participants, patients and family members mentioned in the stories were allotted a pseudonym to facilitate ease of understanding and a smooth flow within the narrative.
As restorying occurred, care was taken to maintain the participant’s voice and the same words as those spoken in the interview were used as far as possible within each narrative. The process of co-constructing the narrative ensured each participant agreed that the narrative produced was a true reflection of the discussion, minimizing misinterpretation or misunderstanding. The narratives provided the participants’ (emic) perspectives of the factors influencing decision-making surrounding WLST.
Stage Two of the Data Analysis Process—Narrative Analysis
Interpretive stories were then composed from each narrative, using narrative analysis through McCormack’s Lenses (McCormack, 2000) and the interconnected, analytical lenses, identified by Chase (2005). These interpretive stories considered the researchers’ (etic) perspective of the participants’ narratives.
McCormack’s Lenses
McCormack’s lenses provide a flexible framework to assist the process of revealing core themes within a story by encouraging the researcher to consider each part, as well as the whole story, from differing perspectives Dibley (2011). The four lenses guide the researcher to consider all parts of a story from four differing viewpoints. Dibley (2011, p. 15) states that “each viewing reveals a different aspect of understanding, and when this is ultimately combined into a final interpretive story, a contextual, rounded perception of the story’s message is revealed.”
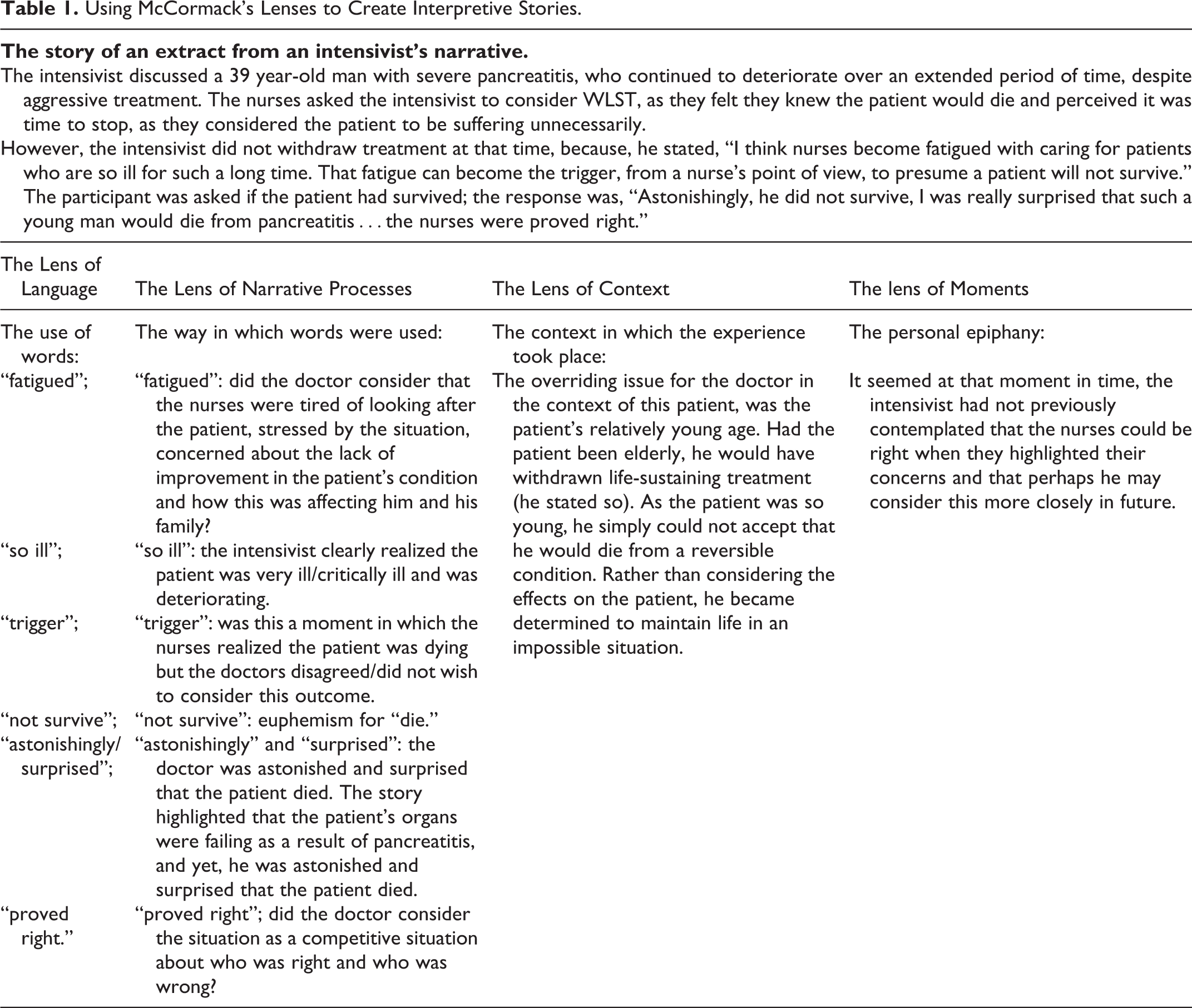
The lens of language focuses on the words people use; the lens of narrative processes focuses on the way in which the words are used; the lens of context focuses on the context in which that experience took place and the lens of moments refers to the point at which the storyteller comes to a previously unrecognized understanding of a fundamental issue in the related experience, or a personal epiphany (Dibley, 2011). Figure 3 outlines the manner in which the lenses can be used and Table 1 outlines in more detail how the lenses were used in the context of a narrative extract when creating an interpretive story.

Using McCormack’s Lenses to create interpretive stories.
Using McCormack’s Lenses to Create Interpretive Stories.
Interconnected, Analytical Lenses (Chase, 2005)
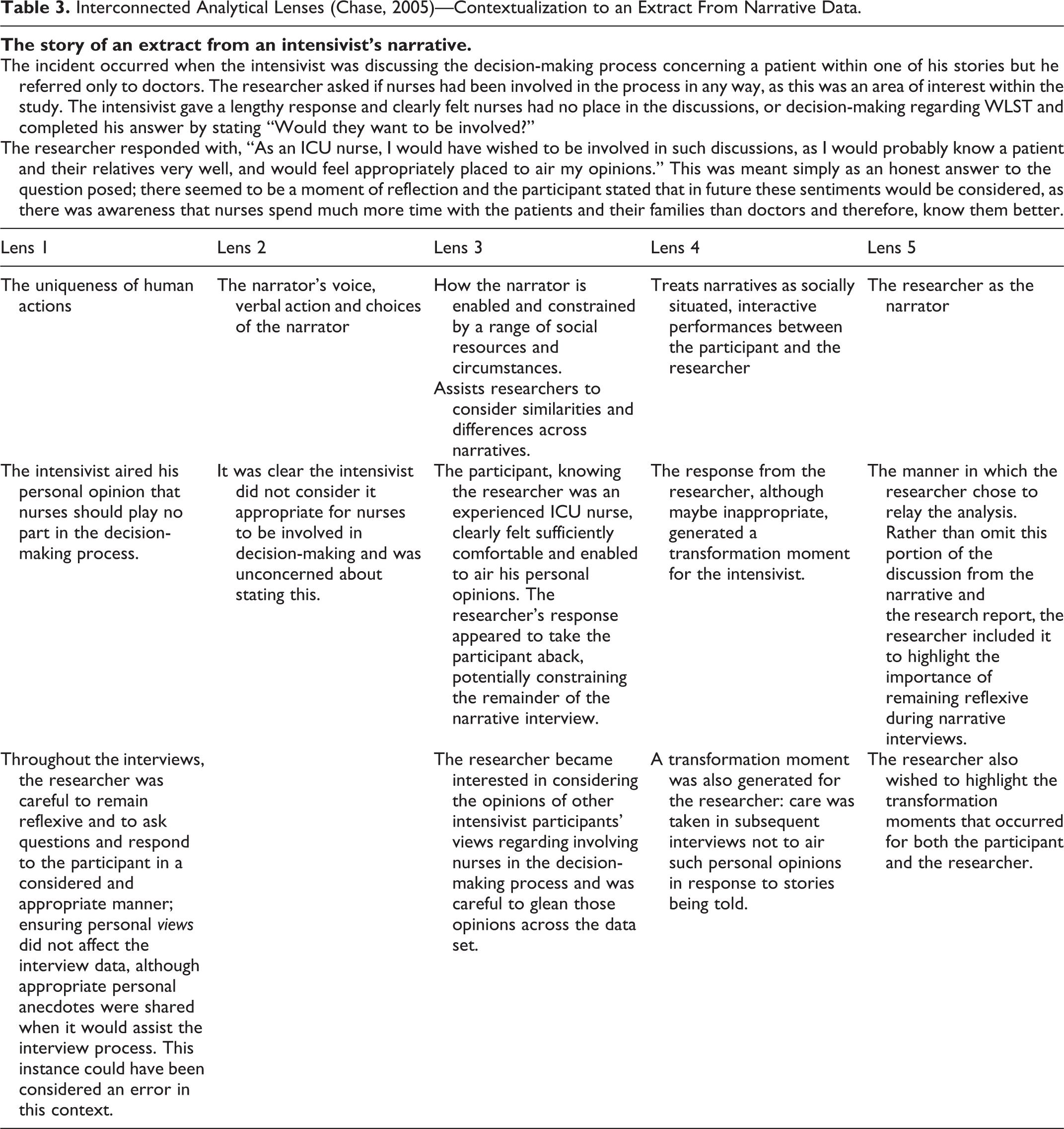
There are five interconnected, analytical lenses, identified by Chase (2005) that assist in narrative analysis; each lens focusses on a different aspect of the narrative process. The first lens considers the uniqueness of human actions; the second lens emphasizes the narrator’s voice, verbal action and choices of the narrator; the third lens considers how the narrator is enabled and constrained by a range of social resources and circumstances (Chase, 2005). Chase (2005) acknowledged that every narrative is particular to the narrator, but this lens assists researchers to consider similarities and differences across narratives. The fourth lens treats narratives as socially situated, interactive performances between the participant and the researcher. The fifth lens focusses upon the researcher as the narrator (Chase, 2005).
Using these lenses was very useful, as they helped to highlight a “how and why” perspective during each stage of analysis. Particularly, in relation to these analytical lenses, the “how and why” of specific actions (first lens) arising during decision-making were considered. The process of WLST was considered in relation to the factors that influenced these actions for each participant, initially, individually and then, collectively, through comparing and contrasting narratives (third lens) and was therefore also useful during horizontal analysis. Also considered was the “how and why” of the manner in which issues were discussed by each participant (second lens); enablers and constraints when considering WLST for a dying patient (third lens) and the manner in which the participant interacted during the interview (fourth lens). These aspects were recorded in the reflective journal and/or field notes and were further reflected upon. Also reflected upon was the way in which the narratives were interpreted and how the data were presented (fifth lens). Table 2 demonstrates the way in which these lenses were applied and Table 3 demonstrates the contextualization to an extract from narrative data.
Interconnected Analytical Lenses (Chase, 2005)—Putting Them Into Practice.

Interconnected Analytical Lenses (Chase, 2005)—Contextualization to an Extract From Narrative Data.
Using both McCormack’s Lenses (McCormack, 2000) and the interconnected lenses described by Chase (2005) ensured triangulation of data analysis methods and therefore contributed to the credibility of the study.
Stage 3 of the Data Analysis Process—Summarizing
This stage encompassed the final stage of vertical analysis, with each narrative and interpretive story being further analyzed to highlight emerging issues. Tabulated summaries of significant issues within each participants’ narrative were created.
Stage 4 of the Data Analysis Process—Horizontal Analysis
Horizontal analysis is the stage at which themes emerge across the entire data set (Reid et al., 2014) and is an in-depth analysis to consider all of the narratives for similarities.
According to Riessman (2008), narrative analysis is concerned with analyzing a whole story. In this study, it was necessary to determine themes across all stories to provide a full picture of how participants’ experiences of WLST shaped the factors that influenced decision-making in this area of practice. Analysis commenced by using the paradigmatic mode of analysis described by Polkinghorne (1995), as it can be used in narrative data analysis to consider common elements from experience that appear frequently and can be categorized into themes. However, as the narratives generated a huge data set, to handle such cumbersome data, the phases of thematic analysis outlined by Braun and Clarke (2006) were followed. Braun and Clarke (2006) emphasized that an accessible and theoretically flexible approach to analyzing qualitative data is offered through this approach. Therefore, this mode of analysis was selected, as it provided a more systematic approach to the horizontal analysis (Table 4).
Phases of Thematic Analysis (Braun & Clarke, 2006).

The Process of Thematic Analysis
Phase One
The data were handled during this initial stage by reading each narrative, interpretive story, tabulated summary, field notes and reflections and noting preliminary and potential themes on post-it notes, which were pasted to a single sheet of paper with the participant’s pseudonym written at the top.
Phase Two
The content of each narrative was further examined to ensure no ideas had been overlooked. Following this, initial ideas were coded independently and then reviewed and discussed among the research team. Initial ideas were again reviewed, to ensure no information had been misinterpreted, or overlooked.
Phase Three
As more narratives were analyzed, post-it notes were transferred to other sheets of paper with the potential theme codes written at the top. As narratives were re-read, similarities in the themes became more transparent and as a deeper understanding developed, the post-it notes were manually placed onto larger sheets of paper and theme codes altered as appropriate. This process initially uncovered over 70 theme codes, which were rapidly conflated because of their close associations. This process was the foundation of the horizontal analysis, which derived the themes that elucidated content consistent across stories (Ellis, 2004).
Phase Four—Level One
During this phase of analysis, it became clear that several of the emerging themes raised issues that were inherently associated within broader themes, enabling themes to be conflated further. At this point, clean copies of the narratives were printed and each one was re-read and while doing so, sections of the narratives were physically cut and pasted to large sheets of flip-chart paper under theme headings.
Phase Four—Level Two
Once the story sections had been manually placed into themes, the sections were again re-read, with several sections being moved, either because there was a deeper understanding of the stories, or because there was a closer relation to a different theme than was originally assumed. There were clearly some sections of the narratives that could have related to two, or in some cases three of the themes, so the best fit was chosen but these sections were highlighted, as a reminder to consider this issue when writing up the analysis.
Phase Five
The final part of the theming process was placing all themes with their corresponding sub-themes into physical piles of the large sheets of paper that contained sections of stories that held related themes. Detailed description and analysis of the findings are reported elsewhere (Foxall, 2019). Six major themes, each with sub-themes emerged from this iterative analysis: theme one alluded to the drivers that prompted the deliberation of WLST for a given patient; theme two alluded to the discussions that took place between all concerned, including medical teams, nursing staff, patients and their families, during decision-making. theme three outlined differences in the decision-making process and who made final decisions. theme four considered the reasons leading to delays in decision-making or in initiating WLST. theme five highlighted potential moral distress and professional conflict as a result of patient suffering and the emotional burden experienced by the ICU team in relation to WLST. theme six considered a number of dilemmas and difficulties that could arise during the decision-making process and the subsequent process of WLST.
Phase Six
The research report was produced after the selection of the most vivid and compelling extract examples from the participants’ narratives and using the interpretive stories to comprise the discussion. The research question and literature were continuously considered during this final stage of analysis. Figure 4 provides an overview of the horizontal (thematic) analysis process.
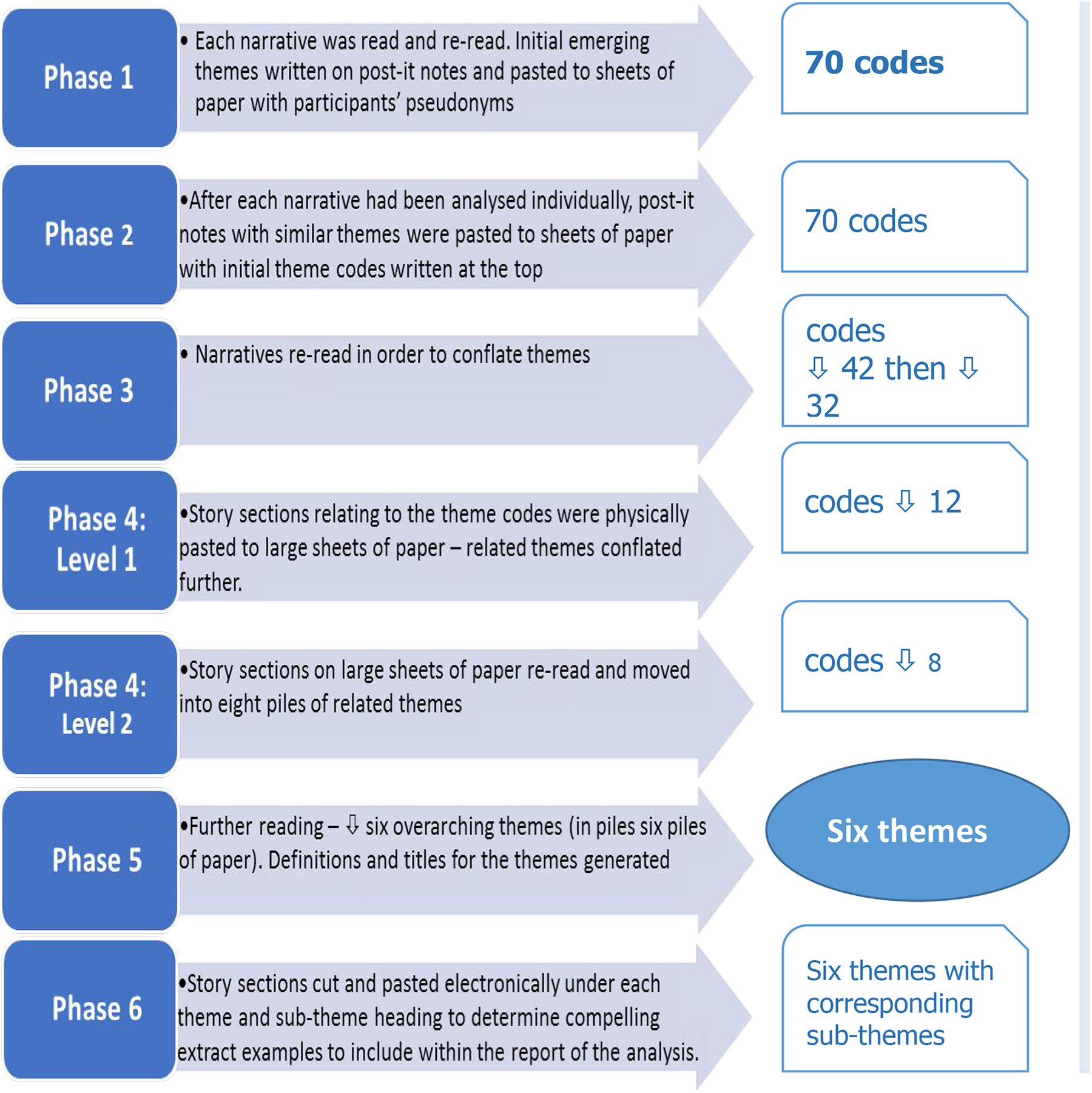
Overview of horizontal (thematic) data analysis.
Research Rigor
Trustworthiness was ensured throughout the study by using Guba and Lincoln’s model for trustworthiness (1994). Credibility was achieved as the research team, all nurses, have considerable ICU experience and have cared for many patients undergoing WLST. The research team were cognizant of the fact that as nurses, their perceptions may differ from those of doctors and hence, through reflexivity, remained as objective as possible. Also, through prolonged engagement with participants, co-construction of narratives and triangulation of data collection and analysis methods. Transferability was achieved by providing a dense description of the research methods and sample. Dependability was demonstrated by enabling future investigators to replicate the study in different ICU settings, by providing a detailed description of the research methodology. Confirmability of the study’s findings is possible from electronic recordings of the interviews, field notes, reflective journal, interview transcriptions, narratives and interpretive stories.
The Strengths of Narrative Inquiry as a Methodology
Narrative inquiry was an invaluable methodology as it facilitated the exploration of the meaning participants gave to their experiences through their stories (Clandinin & Connelly, 2000; Moen, 2006). Exploring diverse experiences of WLST through individual narratives and comparing and contrasting those narratives was illuminating and facilitated understanding of how such experiences are socially constructed, “narratively composed, embodied in people and expressed in practice” (Clandinin & Connelly, 2000, p. 124).
Haydon et al. (2018, p. 125) described narrative inquiry as a “gentle relational methodology” that assists the researcher “to uncover what is important to the person in their situation.” This study sought to treat narratives in the manner suggested by Polkinghorne (1988), by describing and explaining individual narratives of life episodes (relating to decision-making regarding WLST) and consider the relationships between stories and thus, how such events prevailed over, cohered with or conflicted with other storylines. This emphasized the temporal, social and spatial experiences of participants, as described by Haydon and van der Riet (2017). The study provides an example of the application of narrative inquiry within interdisciplinary research and can be replicated.
The Limitations and Challenges of Narrative Inquiry as a Methodology
The findings reflect the subjective thoughts and feelings about participants’ experiences and their perceptions of the factors that influence decision-making. All participants were from one ICU; thus, relevance to others may not be apparent and transferability to the wider population is not possible. These issues, however, prove to be limitations with most qualitative studies. As argued by Sinuff et al. (2007), qualitative results cannot be presumed to be generalizable or to predict, but they potentially provide enlightenment.
There may be a level of artfulness in stories (Freeman, 2007) and human memory is selective, therefore, over time, memories may change (Kitzinger, 2004). Since human memory is fallible, individuals remember experiences in the way they wish to remember them (Kitzinger, 2004). It has been argued that while such autobiographical accounts may not be considered legitimate knowledge, it is mitigated by a poetic dimension, opening a fuller conception of the human condition (Freeman, 2007). However, understanding and giving meaning to events often occurs in retrospect (Polkinghorne, 1995) and “it is grounded in what is tellable” (Atkinson & Coffey, 2003, p118). The narratives are representations of the world through social constructivism and therefore, are not judged as true or false, they express the truth of the point of view of the participant (Muylaert et al., 2014).
Conclusion
Narrative inquiry provided the vehicle to explore and describe a unique view of the personal experiences of ICU nurses and doctors through the analysis of personal narratives. The research puzzle and research question are unique in the incorporation of these concepts, providing a comprehensive, qualitative view of the factors that influence decision-making regarding WLST from the perspectives of both ICU nurses and doctors. There are no identified studies relating to nurses’ and doctors’ perspectives of the factors that influence decision-making regarding WLST that employ narrative inquiry as the research method.
The findings from this study further contributed to the available evidence related to the perceptions of EoL care in ICU. We have facilitated the interpretation of participants’ experiences of decision-making regarding WLST and arrived at powerful conclusions that serve as an avenue to challenge legislation and current opinion regarding the autonomy and role of the family in decision-making.
A window into participants’ experiences of WLST has been developed providing an opportunity to consider the factors that may influence decision-making in this important aspect of nursing and medical practice. Ultimately, using narrative inquiry as the methodology in this study has enabled us to shed light on the reasons WLST may be delayed, potentially increasing patient suffering at the end of life, which should be unacceptable. The findings may trigger new ways of working to ensure EoL care and WLST in ICU are optimized to ensure we use the only opportunity afforded to ensure EoL care is appropriate for each individual.
The research material related to this paper is available from Research Online at https://ro.ecu.edu.au/theses/ 2256 and will be available for download on November 15, 2022.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.Edith Cowan University (Open Access Fund) provided the article publication charge.