
Abstract
Background: Climate change represents a serious threat to the health of the population. Nurses are the ideal group to act on the health risks posed by climate change. However, their perception of this phenomenon is unknown, as existing studies are very scarce. An in-depth study of nurses’ perceptions of climate change is needed. For this purpose, qualitative research is the best alternative. Objective: To understand nurses’ perceptions of their role as health assets in relation to climate change. Methods: A qualitative study will be carried out. The sample will be selected by means of purposive sampling with a maximum variation approach and will be defined by the data saturation criterion and will include nurses from different health units and regions of Spain. Semistructured interviews will be conducted using a videoconferencing platform. The interviews will be transcribed and analysed by several researchers using the logic of a three-step thematic analysis. Discussion: The results of this study will provide for the first time a clear, in-depth, and representative picture of Spanish nurses’ perceptions of climate change. This is essential for the development of concrete measures through which nurses become real health assets in the face of climate change.
Keywords
Background
According to the sixth report of the Intergovernmental Panel on Climate Change, atmospheric concentrations of greenhouse gases (GHG) have reached unprecedented levels for at least 800,000 years (Lee et al., 2021). As a result, our planet has undergone a series of climatic alterations of increasing intensity, which have ended up constituting climate change due to its speed and anthropological origin, unprecedented (Lee et al., 2021), and which, according to the UCL Lancet Global Health Commission, represents “the greatest global threat to health in the 21st century” (Costello et al., 2009).
In the coming years, continued GHG emissions will continue to cause further warming and further changes in all components of the climate system (Lee et al., 2021). For this reason, it is necessary to develop and implement measures to adapt to the future impacts of climate change, but a substantial and sustained reduction in GHG emissions is also needed to minimise the global warming that leads to climate change (Lee et al., 2021). We could say that climate change, global warming and air pollution from GHG form a triangle in which the three vertices feedback on each other (Intergovernmental Panel on Climate Change [IPCC], 2022; Lee et al., 2021).
Global Warming and Climate Change
Human activities have unequivocally warmed the atmosphere, ocean and land, leading to widespread and rapid changes in the atmosphere, ocean, cryosphere and biosphere (IPCC, 2023). These changes have a major impact on human health (IPCC, 2023), affecting the health of people around the world directly through increased exposure to extreme weather conditions and indirectly through impacts on the physical, natural and social systems on which health depends (Romanello et al., 2022). Thus, for example, secondary to the increased frequency and intensity of extreme weather events, the risk of drowning and injuries, damage to human settlements, the spread of waterborne diseases (due to contamination of drinking water networks, agro-livestock land or shellfish farming areas, following the entrainment of pathogens such as Salmonella or Vibrio cholerae), population displacement and mental health consequences (anxiety, posttraumatic stress or dependence on psychotropic drugs, among others) (IPCC, 2022; Ministry for Ecological Transition and the Demographic Challenge [MITECO], 2020; Romanello et al., 2022; Spanish Society of Public Health and Health Administration [SESPAS], 2022).
Spain will be one of the countries on the European continent most affected by climate change (MITECO, 2020). Variations in traditional weather patterns will result in a series of cascading effects that will threaten the well-being of citizens (MITECO, 2020). Periods of drought will be longer and more frequent, and rising temperatures will lead to increased evaporation from water bodies. In addition, rising sea levels will increase the salinity of groundwater near the coast, and the remaining available water resources could be affected by a higher concentration of particles and microorganisms or by an increase in forest fires. River flows and aquifer recharge will be reduced. Dust storms will become more frequent and intense, as will torrential rains and floods. Extreme events will lead to a decline in agricultural and livestock productivity and affect infrastructure. Changes in biodiversity and climatic conditions will modify the distribution of disease vectors. These are just some of the most salient effects of climate change in Spain (MITECO, 2020; SESPAS, 2022).
Climate Change and Greenhouse Gas Air Pollution
Air pollution from GHG emissions and climate change are strongly intertwined and feedback on each other. Several air pollutants are also climate forcers, contributing to global warming and consequent changes in climate (Lee et al., 2021; World Health Organization [WHO], 2021). In turn, changes in weather patterns can alter the transport, dispersion, deposition and formation of air pollutants in the atmosphere (IPCC, 2022; MITECO, 2020; SESPAS, 2022). Almost all climate-altering pollutants are harmful to health. However, under current European air quality conditions, particulate matter (PM), ground-level or tropospheric ozone (O3) and nitrogen dioxide (NO2) are the pollutants with the greatest impact on total mortality related to air pollution (European Environment Agency [EEA], 2023).
The latter gas (NO2) is itself toxic and the main source of tropospheric ozone and nitrate aerosols, constituting a significant fraction of the PM mass in ambient air. As a precursor to other pollutants, NO2 concentration is often chosen by agencies such as the World Health Organization (2021) as a guide value for estimating the pollution of an area. NO2 and PM concentrations may be particularly aggravated by the persistence of stable atmospheric conditions favoured by climate change. Similarly, concentrations of ozone and PM precursors increase faster in brighter light and at higher ambient temperatures, so climate change tends to increase them (IPCC, 2022; Lee et al., 2021; MITECO, 2020; SESPAS, 2022; WHO, 2021).
Susceptibility to the health impacts of climate change and air pollution may increase as a result of age, preexisting health conditions or particular behaviours, such as diet, physical activity and smoking (Costello et al., 2009; IPCC, 2022). Air pollution has been linked to an increased risk of respiratory and cardiovascular disease, lung cancer, diabetes, neurological disorders and adverse pregnancy outcomes, among others (EEA, 2023; Romanello et al., 2022). In the European Union in 2020, exposure to PM, NO2 and O3 was responsible for approximately 412,000, 136,000, and 107,000 premature deaths, respectively (EEA, 2023). Spain has the fourth-highest number of NO2-related premature deaths in Europe (EEA, 2023). In absolute numbers, the total mortality from all causes attributable to NO2 concentrations for the country as a whole has been estimated to be 4.800 deaths in 2020 (EEA, 2023) and 60.852 cumulative deaths from 2000 to 2009 (Linares et al., 2018).
The Role of Nursing in the Face of Climate Change
For nurses, protecting the population’s health from environmental hazards is a deontological obligation. This can be seen from the reading of codes of ethics such as the Spanish one, which includes the duties of nurses to know, study, record and disseminate the harmful effects that pollutants may have on human beings to participate in the measures to be adopted and to educate the population about environmental problems (General Council of Nurses, 1973).
Added to this fact, there are specific position statements on the role of nursing in addressing climate change, such as the one adopted by the International Council of Nurses in 2018 under the title Nurses, Climate Change and Health, which calls on all national nursing associations and invidious nurses to empower themselves and be part of national and multisectoral climate change adaptation and mitigation efforts; to incorporate sustainability into nursing curricula and continuing education; and to raise awareness of the health implications of climate change and how to assess and address the health risk of climate change (International Council of Nurses [ICN], 2018).
The UCL Lancet Global Health Commission stated in 2018 that “the voice of health professionals is essential to drive progress on climate change” and highlighted the central role of nurses and other health workers in mitigating and adapting health systems to climate change and in communicating the need for an accelerated response (Watts et al., 2018). Nurses are essential to action on climate change and its effects on health, as they are the largest profession in the health system and have clinical, educational, research, executive and policy-influencing roles (ICN, 2018; WHO, 2016). To design action strategies for nurses in the face of climate change, it is first necessary to understand nurses’ perceptions of this phenomenon (Anåker et al., 2015). By studying nurses’ perceptions of climate and environmental issues and how they can contribute to sustainable development, we can better understand how nurses can participate in mitigating and adapting to climate change to generate better health outcomes (Anåker et al., 2015) and what gaps and difficulties they have in being able to carry out the work they are being asked to do in the face of this challenge. However, although an increasing number of nurses are being encouraged to take an active role in climate change action, previous work studying the perception of nurses as a whole in depth in relation to this phenomenon has not yet been carried out, which is why it is necessary to carry out research in this area (Anåker et al., 2015; Hathaway & Maibach, 2018; ICN, 2018).
Current Status of the Issue to be Addressed
A systematic review by Hathaway and Maibach (2018) that sought to understand how health professionals and the public around the world perceived the health implications of climate change found a high perception among health professionals that climate change was harming health. Nevertheless, the level of knowledge about climate change and how to cope with it was low, and they perceived a need to learn more.
After consulting the existing bibliography, we found only five studies (Anåker et al., 2015; Iira et al., 2021; Kalogirou et al., 2020; Polivka et al., 2012; Xiao et al., 2016) that focused on nurses’ perceptions of climate change, three of which used qualitative methodology. All of them agree with Hathaway and Maibach (2018) that most nurses are aware of the detrimental effects of climate change on health. They also agree with the nurses’ perception that they do not have the knowledge or capacity to carry out this task and their interest in further training in this area (Anåker et al., 2015; Iira et al., 2021; Kalogirou et al., 2020; Polivka et al., 2012; Xiao et al., 2016). There is less agreement on the perceived role of nurses in addressing climate change. According to Polivka et al. (2012) and Anåker et al. (2015), nurses are aware of their own responsibility with regard to climate and environmental problems, despite expressing a lack of knowledge and skills. In contrast, both Kalogirou et al. (2020) and Xiao et al. (2016) found that nurses did not understand the reciprocal influence between the profession and climate change and even doubted that they had any role to play in this phenomenon.
Of these five investigations, only two have been carried out in Europe, specifically in Nordic countries (Anåker et al., 2015; Iira et al., 2021). Both indicate the need for further studies exploring the relationship between climate change and nurses in other countries (Anåker et al., 2015; Iira et al., 2021). It is therefore necessary to carry out this type of research in southern Europe, with the Mediterranean area being the most affected by climate change within the European continent (IPCC, 2022; Lee et al., 2021). In addition, it would be advisable to carry out studies involving professionals from various health services and units to have a more complete view of the phenomenon (Anåker et al., 2015).
Research Question
What knowledge do nurses have about climate change?
How do nurses perceive the relationship between climate change and health?
What is the involvement and empowerment of nurses to be part of climate change action?
Objectives
The main objective of this study will be to understand nurses’ perceptions of their role as health assets in relation to climate change and its effects on health.
The specific objectives are as follows: • To explore nurses’ general knowledge of climate change. • To determine their perception of the relationship between climate change and health. • To understand nurses’ perceptions of their role in the face of climate change. • To understand the involvement and empowerment of nurses in taking action on climate change.
Methodology
Design
Study based on the paradigm of constructivism, since we understand that there are different realities and approaches to the phenomenon under study, depending on the participants and their subjectivities (Denzin & Lincoln, 2011). Following this paradigm, a qualitative descriptive study has been designed with a naturalistic and flexible approach (Colorafi & Evans, 2016; Levitt et al., 2018).
The Target Population of the Research
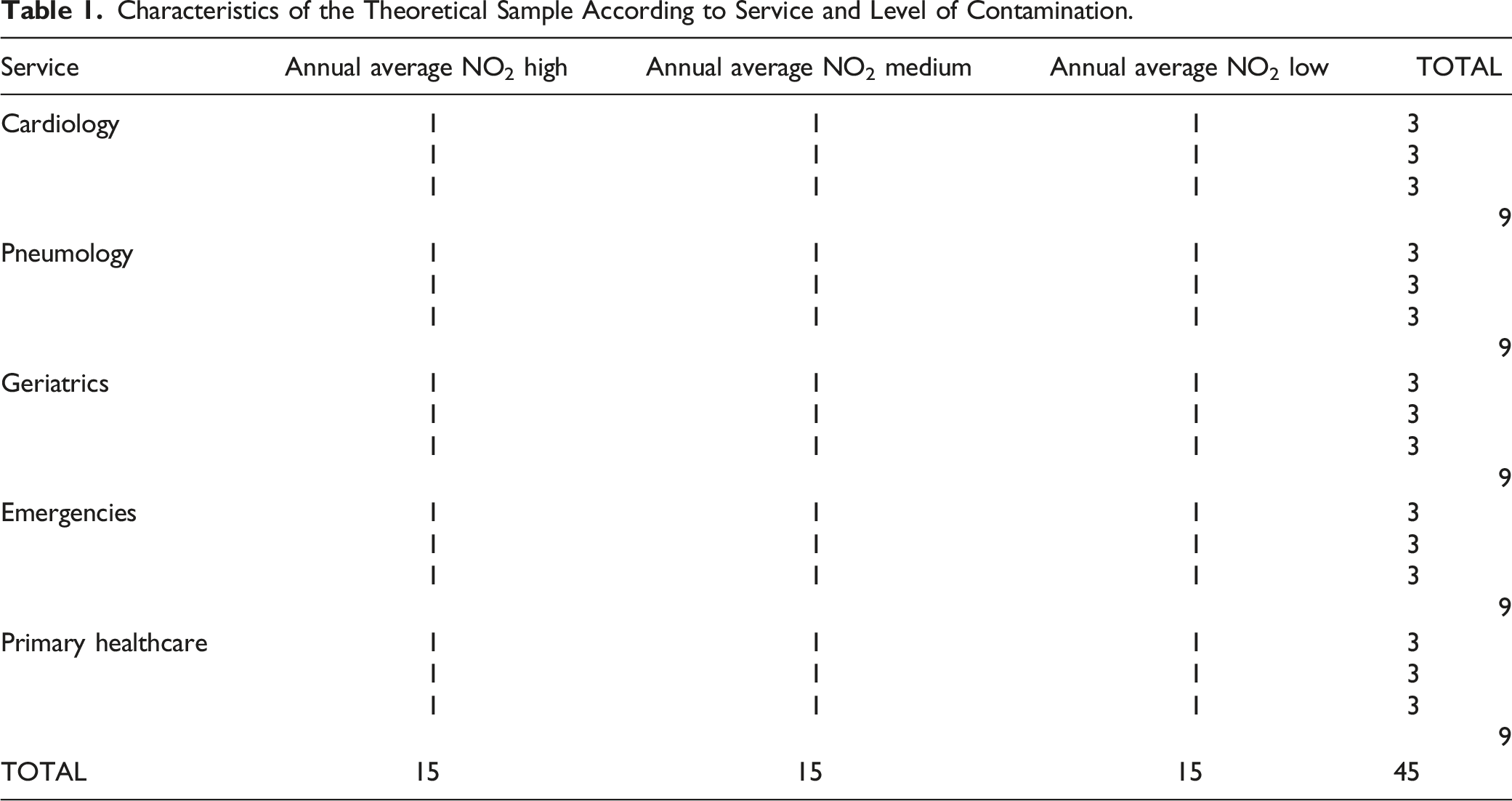
Subjects will be nurses of any gender fluent in Spanish. They will be selected from environments with high, medium and low levels of air pollution (MITECO, 2022; WHO, 2021) and from different units of different health centres of the Spanish National Health System. For the selection of the areas according to their level of pollution, the same zoning used by the Ministry for Ecological Transition and the Demographic Challenge of the Spanish Government and the European Environment Agency has been used. Taking into account the annual average of NO2 recorded during 2021, the three zones with the highest values of pollution by this gas, the 3 with the lowest and the 3 with average values (MITECO, 2022) were selected. NO2 was chosen as an indicator because it is a gas that is representative of air quality because of its effects on health and because it has the highest rates of premature deaths and years of life lost due to exposure per 100,000 inhabitants in southern European countries (EEA, 2023; Linares et al., 2018; WHO, 2021). For the services selected, cardiology, pulmonology, geriatrics, hospital emergency and primary care were chosen because they are considered services that serve groups vulnerable to climate change and/or the access route to the health system (Costello et al., 2009; EEA, 2023; MITECO, 2020; SESPAS, 2022). If these services do not exist in any of the selected areas, the reference health centre for the populations of the selected area will be used.
Finally, and based on the aforementioned criteria, the areas chosen are Prepirineu (Cataluña), North of Gran Canaria (Islas Canarias), Emporda (Cataluña), Turia coastal area (Comunidad Valenciana), Cartagena (Región de Murcia), Albacete (Castilla-La Mancha), Granada and Metropolitan area (Andalucía), Barcelona area (Cataluña) and Madrid (Comunidad de Madrid).
Characteristics of the Theoretical Sample According to Service and Level of Contamination.
Data Collection
The semistructured interview was considered the most appropriate technique for collecting information. On the one hand, this technique allows the interviewer to focus the conversation on the topics he/she considers important in relation to the research project, following a script of questions (Appendix A) with questions considered essential to achieve the set objective. On the other hand, it gives interviewees the flexibility to go into greater or lesser depth on the issues they consider of greatest interest (Leavy et al., 2014; Malterud et al., 2016). The script of questions was developed based on a literature review of similar studies and was subsequently validated by means of a pilot test with volunteer nurses who were independent of the study (Creswell, 2013).
Interviews will be one-on-one, as this will allow the interviewer to more easily guide the conversation in a direction that is successful in relation to the research interests (Leavy et al., 2014). The meetings will be conducted via video calls using the Microsoft Teams platform and will be led by two team members who will act as interviewer and observer. Video calls will allow us to reduce or eliminate limitations of conventional interviews, such as time and financial constraints or geographical dispersion (Creswell, 2013; Janghorban et al., 2014; Leavy et al., 2014). Moreover, thanks to video calls, the interviews will take place in a more comfortable environment for the participants, which will encourage a more open attitude toward the expression of their perceptions (Creswell, 2013; Janghorban et al., 2014). The duration of the interviews will be between 45 and 60 min. The initial number of semistructured interviews will be 45, although the final number will depend on the achievement of data saturation. At that point, the research team will terminate the data collection.
The interviews will be videotaped, with the prior written and verbal consent of the interviewees, and then transcribed verbatim. In addition, a field notebook will be used in which the interviewer will make notes during the interviews and the preliminary analysis to later incorporate them into the analysis of the transcripts.
Data Analysis
Once the interviews have been transcribed verbatim, inductive content analysis will be carried out, in which the researchers will immerse themselves in the data to make sense of the whole through reading and rereading (Vaismoradi et al., 2013). The software ATLAS. TI 8.3 will be used.
The data analysis will be carried out in three steps by three expert researchers following the logic of thematic analysis (Leavy et al., 2014). First, sentences or paragraphs from the transcripts will be divided into meaning units, which are text segments containing a single idea (Colorafi & Evans, 2016). For each meaning unit, one or more codes will be applied during first-level coding, which will be highly descriptive in nature (Colorafi & Evans, 2016). In the second step of data analysis, conceptually similar codes will be organised into emergent categories (Colorafi & Evans, 2016; Levitt et al., 2018; Vaismoradi et al., 2013). Finally, a cross-analysis of the emerged categories in relation to the whole dataset will be performed, and from these categories, themes will be interpreted and identified that will show the meaning attributed to climate change and its relation to health from the nurses’ point of view (Leavy et al., 2014; Vaismoradi et al., 2013). The process will be an ongoing comparative method in which codes, categories and themes will be discussed with the research team until all members are in agreement (Leavy et al., 2014).
Rigour
A strength of this study is the use of a qualitative methodology to understand nurses’ perceptions of their role as health assets in relation to climate change and its effects on health, from their own perspective. However, conducting a qualitative study carries risks of bias focused on the rigour of the results obtained. To this end, several strategies were used to guarantee a rigorous analytical approach.
The credibility and reliability of the findings are enhanced through the selection of the participants: an initial sample of 45 subjects with heterogeneous characteristics in terms of work environment and exposure to levels of air pollution (Giacomini & Cook, 2000). Although, a possible bias is the participation of subjects with a prior predisposition and interest in the subjects studied, which could lead to results that are not representative of the entire population, it has been considered that this condition may, paradoxically, represent a strength, since a sample previously interested in the subject of the study may also provide a greater wealth of data (Creswell, 2013).
As mentioned previously, semistructured interviews are the most appropriate tool to achieve our objective (Leavy et al., 2014; Malterud et al., 2016). Precisely the use of a script of questions for the interview reinforces the reliability of the study (Colorafi & Evans, 2016). Furthermore, to avoid the influence of the interviewer on the interview script, it was developed based on the literature and validated by piloting it with nurses independent of the study (Creswell, 2013). All interviews will be conducted by the same researcher and with the same question script. A field notebook will also be used to analyse the consistency between the results from the analysis of the transcripts and those extracted from the notebook itself (Colorafi & Evans, 2016; Levitt et al., 2018; Vaismoradi et al., 2013).
We will rely on consensus-based qualitative research (Colorafi & Evans, 2016; Leavy et al., 2014). Three researchers will independently read the data collected through the interviews and discuss any discrepancies that arise until consensus is reached (Leavy et al., 2014). Researchers will use reflexivity, especially in the inductive part of the analysis, trying to control how prior knowledge about the phenomenon could influence the interpretation of the data (Giacomini & Cook, 2000). The process of coding and derivation and identification of themes will be made explicit by conducting preliminary analyses during data collection. Researchers will document their thoughts and reactions as a way of tracking emerging impressions of what the data mean and how they relate to each other (Colorafi & Evans, 2016; Tong et al., 2007).
Data saturation will also be discussed among three researchers. In addition, each interviewee will be sent a copy of the transcript of his/her interview and the results obtained after data analysis to ensure that their perceptions are correctly represented and that there are no biases (Tong et al., 2007).
Discussion
The results of this study will provide for the first time a clear, in depth, and representative picture of Spanish nurses’ perceptions of climate change.
As a result of this work, the strengths and needs of nurses will be mapped to become true health assets in the face of the climate challenge. Only with this reliable mapping will it be possible to efficiently define concrete measures with which nurses will be able to develop their maximum potential as drivers of the population’s well-being, even under the adverse conditions that climate change poses for society as a whole.
Given the cross-cutting nature of nurses within social and health care, the development of studies such as this one, which through qualitative research provide a solid knowledge base on which to develop further measures, is the first stepping stone on the road to the resilience of the welfare state and the development of quality social and health care, even under the worst possible conditions.
Ethical and Legal Aspects
This protocol was approved by the Research Ethics Committee of the Cuenca Health Area (registration 2021/PI3721). Prior to the interviews and after sending the information sheet to the participants, written and verbal consent will be requested from the participants, and they will be informed of the possibility of withdrawing from the study at any time. In the information sheet, participants will be informed of the video recording of the interviews. For the transcription of the interviews, an identification code will be assigned to each interviewee, and his/her name will be omitted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the HEALTH, GENDER AND SOCIAL DETERMINANTS RESEARCH GROUP, which is funded by the Council of Education and Science of the Regional Government of Castille-La Mancha and the FEDER Funds (grant number 2022-GRIN-34439).
Appendix
Interview script
Reminder introduction
Study theme: Nurses’ perceptions of climate change and its effects on health.
Objective: To understand nurses’ perceptions of their role as health assets in relation to climate change and its effects on health. To explore their knowledge, opinion, interest and involvement in climate change.
Repetition of ethical issues: This research has been approved by the Research Ethics Committee the Cuenca Health Area (registration 2021/PI3721). Prior to the start of this interview, the interviewee must have signed the informed consent form. The interview will be recorded and only the research team will have access to the recordings. With the transcription of the interview, the personal data of the interviewees will be omitted. The interviewee has the right to leave the interview at any time. The interviewee has the right to have the transcript of his/her interview removed from the study. A copy of the transcript of each interview will be sent to each interviewee so that he/she can corroborate its veracity.
Corroboration of secondary data: (Geographical area, health service, years of experience in the service).
Questions
General knowledge about climate change
• What is the first thing you think of when you hear the term “climate change”?
• What is climate change?
• What is happening, what is causing it, what or who is causing it?
• What can we do about climate change?
Climate change and health
• How might climate change affect us humans?
• How do you think climate change might affect health?
• What signs of climate change effects on health have you observed in your environment (either private or professional)?
Climate change and nursing
• Does nursing have an impact on climate change? Does climate change have an impact on the daily work of nurses?
• What can nurses do about climate change?
• What do you do about climate change in your private life (recycling, food, travel)?
• What do you do about climate change in your workplace?
• How do you act on climate change in your work environment (at service, management level) (both mitigation and adaptation measures)?
• What barriers exist to taking action on climate change in your work environment?
• How do you know so much about climate change?
• Where did you determine about climate change? Official media?
Comments and questions that have not been covered and the respondent wishes to add.