
Abstract
Objective
Achieving both the social functioning and personal recovery as treatment outcomes for individuals with schizophrenia remains challenging, despite their recognition as key treatment goals beyond symptom reduction. These interrelated constructs require precise examination to inform effective rehabilitation strategies including occupational therapy. This study explores the relationships between subdomains of social functioning and personal recovery.
Methods
This cross-sectional study included 98 outpatients with schizophrenia. Social functioning was assessed using the Japanese version of the Specific Levels of Functioning Scale (SLOF), and personal recovery with the Japanese version of the Recovery Assessment Scale (RAS). Correlational and hierarchical multiple regression analyses examined their associations.
Results
The Interpersonal Relationships domain of social functioning correlated significantly with the RAS subdomains Trust in Others (r = 0.34, p < .01) and Willingness to Ask for Help (r = 0.26, p < .01). Hierarchical multiple regression analysis identified Interpersonal Relationships as a significant predictor of Trust in Others, but not Willingness to Ask for Help.
Discussion
These findings highlight the crucial role of interpersonal relationships in fostering trust, a key aspect of personal recovery. The results support integrated interventions addressing both social functioning and personal recovery to help reduce loneliness in individuals with schizophrenia.
Introduction
Social functioning and personal recovery are now recognized as key outcomes in schizophrenia (Agarwal et al., 2023). These concepts extend beyond symptom reduction, encompassing broader life aspects. Social functioning involves symptom improvement and the ability to fulfill social roles and daily activities, while personal recovery is a holistic construct emphasizing lifestyle and personal attitudes beyond symptoms, disabilities, housing, and employment (Deegan, 1988). Recovery is classified into three types: clinical recovery, denoting symptom improvement; functional recovery, referring to social and vocational functioning; and personal recovery, which centers on subjective well-being and self-perception (Leendertse et al., 2021; Van Eck et al., 2018). Distinguishing these categories is essential for designing targeted interventions. Both social functioning and personal recovery are multidimensional. Social functioning comprises independent domains such as interpersonal relationships, daily activities, and occupational engagement (Bowie et al., 2012; Harvey et al., 2012). Personal recovery is characterized by five elements—Connectedness, Hope and Optimism, Identity, Meaning in Life, and Empowerment—collectively known as “CHIME” (Shanks et al., 2013). The significance of these constructs is underscored by their low achievement rates. Lambert et al. (2006) reported that 47.2% of individuals with schizophrenia achieved symptom remission, whereas Best et al. (2020) found that only 32.1% and 14.5% attained social functioning recovery and personal recovery, respectively, with just 6.7% achieving both. These findings highlight the substantial challenge of integrating personal recovery with social functioning, emphasizing the need for refined rehabilitation and support strategies. Demographic factors such as age, gender, and education have been identified as influencing personal recovery (Yu et al., 2020). Moreover, meta-analyses by Van Eck et al. (2018) and Leendertse et al. (2021) reported moderate correlations between social functioning and personal recovery (r = 0.21–0.31), suggesting a reciprocal influence. A deeper understanding of their relationship could inform comprehensive intervention strategies. However, this relationship remains insufficiently explored. Inconsistencies across studies may be attributed to variations in assessment methods and sample characteristics, warranting further investigation. Pernice-Duca (2010) reported weak but significant correlations between the total score of the Social Functioning Scale (SFS) (Birchwood et al., 1990) and specific subdimensions of the Recovery Assessment Scale (RAS), such as “Confidence and Hope” and “Goal and Success Orientation.” However, the study did not analyze social functioning by its specific domains, and the total score of the SFS, by conflating distinct functional domains, may lead to misinterpretation of results (Harvey et al., 2012; 2013). Moreover, only 41.4% of the participants were diagnosed with schizophrenia, limiting the generalizability of the findings. Similarly, Roe et al. (2011) investigated 159 participants with schizophrenia-related diagnoses but found no significant correlations between the total score of the Global Assessment of Functioning (GAF) and the RAS subdimensions. However, GAF has been criticized for incorporating symptomatology into its assessment (Brissos et al., 2011). In contrast, Van der Krieke et al. (2019) identified stronger correlations between specific subdomains of the SFS and the total score of the RAS. Nonetheless, the SFS encompasses seven broad functional domains (Birchwood et al., 1990), and personal recovery was assessed in a generalized manner. Additionally, while 84% of the sample had schizophrenia, the heterogeneity of the sample remained a limitation. These inconsistencies suggest that the true relationship between social functioning and personal recovery in schizophrenia may be obscured by differences in assessment tool selection, domain definitions, and sample heterogeneity. To address these issues, this study focuses exclusively on outpatients with schizophrenia, exploring the relationship between specific subdomains of social functioning and personal recovery. This study aims to provide a more detailed understanding of social functioning and personal recovery in schizophrenia, with the goal of enhancing recovery-oriented interventions, including occupational therapy.
Method
Study design and participants
This was a cross-sectional study for outpatients diagnosed with schizophrenia (ICD-10) in a hospital between December 2019 and November 2020. Exclusion criteria comprised cognitive impairment, intellectual disabilities, and cerebrovascular disorders. Based on prior studies (α = 5%, power = 80%, effect size r = 0.31), the required sample size was 79 (Faul et al., 2007). Of 263 eligible outpatients, 171 were deemed suitable by their psychiatrists. Using a non-probabilistic approach, 55 declined, and 18 were unavailable due to hospitalization, transfer, or death. Ultimately, 98 consented and were analyzed.
Assessment items
Demographic characteristics, including age, gender, education duration, illness duration, and antipsychotic dosage (chlorpromazine equivalent), were obtained from medical records.
The brief positive and negative syndrome scale (Brief PANSS)
The Brief PANSS, a six-item version of the PANSS (Yamamoto et al., 2010), assesses positive (“delusions,” “suspiciousness”), negative (“emotional withdrawal,” “passive/apathetic social withdrawal”), and general psychopathology (“tension,” “unusual thought content”) symptoms. Severity is rated from 1 to 7, with higher scores indicating greater severity. Treating psychiatrists conducted the evaluations. The Brief PANSS has strong concurrent validity with the full 30-item PANSS (Yamamoto et al., 2010). This study analyzed positive and negative symptom scores.
Japanese version of the 24-item recovery assessment scale (RAS)
The RAS is a leading quantitative measure of personal recovery in schizophrenia (Chiba et al., 2010; Corrigan et al., 2004). The Japanese version (Chiba et al., 2010), translated from Corrigan et al.'s 24-item scale (2004), has been studied in relation to personal recovery and psychological well-being, concepts associated with the CHIME framework (Salzer & Brusilovskiy, 2014; Van Eck et al., 2018). It consists of five factors: “Goal and Success Orientation/Hope,” “Reliance on Others,” “Personal Confidence,” “No Domination by Symptoms,” and “Willingness to Ask for Help.” Items are rated on a 5-point Likert scale (“strongly disagree” to “strongly agree”), with higher scores indicating greater recovery. Its reliability and validity are well established, with a Cronbach’s α of 0.90 in this study.
Specific levels of functioning scale (SLOF)
The SLOF is widely recognized as the most suitable objective measure of social functioning in community-dwelling outpatients with schizophrenia (Harvey et al., 2011). The Japanese version (Sumiyoshi & Sumiyoshi, 2012) evaluates three domains across 24 items: Interpersonal Functioning (7 items, e.g., “effectively communicating”), Activities (11 items, e.g., “shopping”), and Vocational Functioning (6 items, e.g., “ability to stay on task”). Each item is rated on a 5-point scale from “almost never” to “almost always,” with higher scores indicating better social functioning. In this study, the SLOF subdomains were analyzed as Interpersonal Functioning, Activities, and Vocational Functioning (Harvey, 2013; Sumiyoshi et al., 2016). The Japanese SLOF has shown strong internal consistency (Cronbach’s α = 0.80) and convergent validity, correlating significantly with the UCSD Performance-Based Skills Assessment-B (UPSA-B, r = 0.65), SFS (r = 0.56), and the Brief Assessment of Cognition in Schizophrenia (BACS, r = 0.56) (Sumiyoshi et al., 2016).
Statistical analysis
Descriptive statistics of the sample population were calculated, and parametric tests were conducted based on sample size (Kwak & Kim, 2017). Pearson’s correlation coefficients (r) between RAS and SLOF subdomains were then calculated. Following Cohen’s criteria (2013), r values of 0.10, 0.30, and 0.50 were interpreted as small, moderate, and large, respectively. Hierarchical multiple regression analysis was exploratively conducted for variables with significant correlations. In Step 1, confounding variables (age, gender, education duration, positive symptoms, and negative symptoms) linked to personal recovery were entered (Leendertse et al., 2021; Van Eck et al., 2018). In Step 2, SLOF subitems significantly correlated with the dependent variable were added via stepwise regression, and R^2 values were calculated. Cohen’s criteria for R^2 (0.02 = small, 0.13 = moderate, 0.26 = large) were applied (Cohen, 2013). Statistical significance was tested via analysis of variance. Residual normality and multicollinearity were assessed using the Shapiro-Wilk test and Variance Inflation Factor (VIF, threshold = 5). The significance level was set at 5%, and analyses were conducted using IBM SPSS Statistics 27.
Ethical considerations
Ethical approval was obtained from the Institutional Review Board of International University of Health and Welfare (Approval No. 19-lo-99). The study’s purpose and nature were explained verbally and in writing, emphasizing voluntary participation. Participants were informed of their right to refuse or withdraw consent anytime without consequences. Only consenting outpatients were included.
Results
Descriptive statistics of the sample population (n = 98).
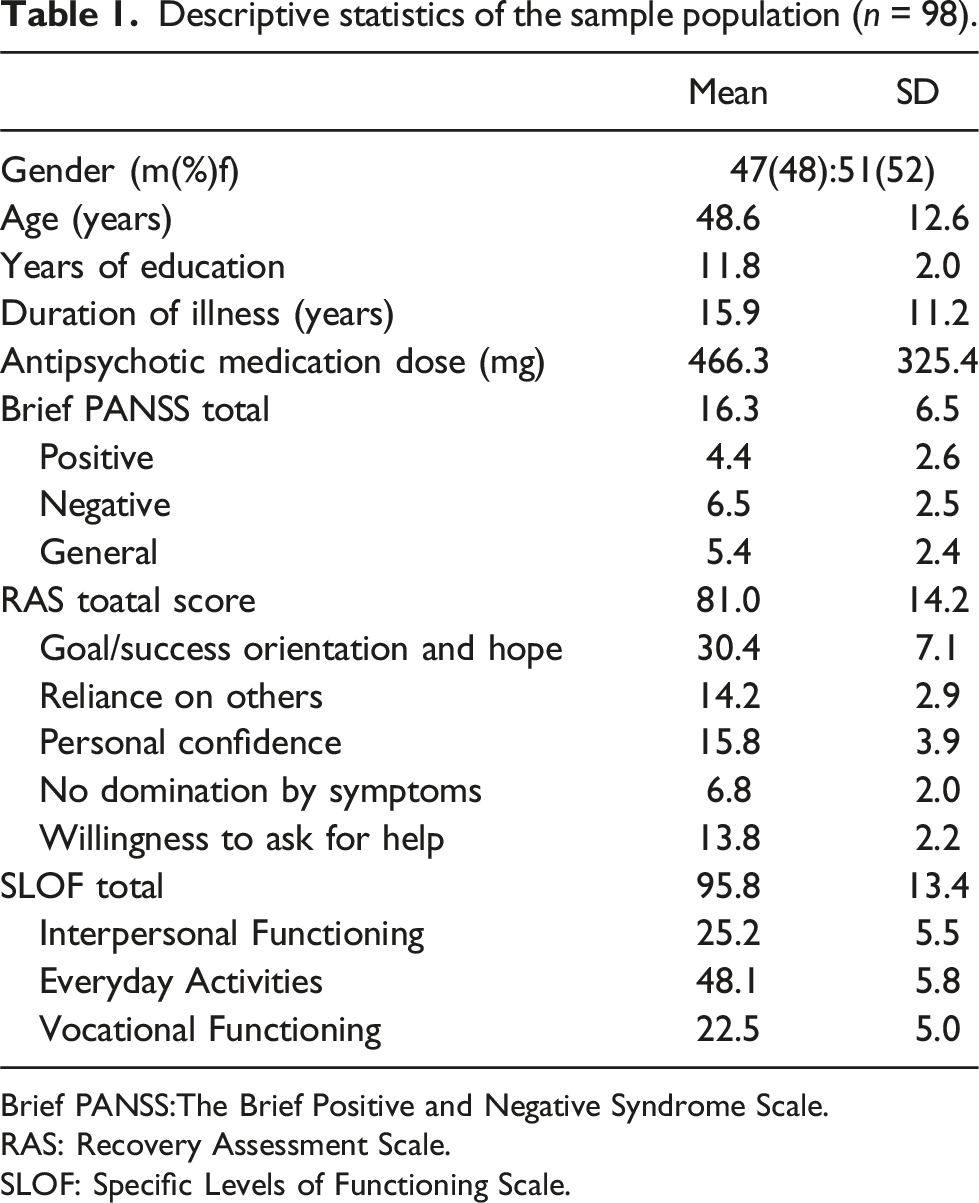
Brief PANSS:The Brief Positive and Negative Syndrome Scale.
RAS: Recovery Assessment Scale.
SLOF: Specific Levels of Functioning Scale.
Correlation between social functioning and conceptual components of recovery.
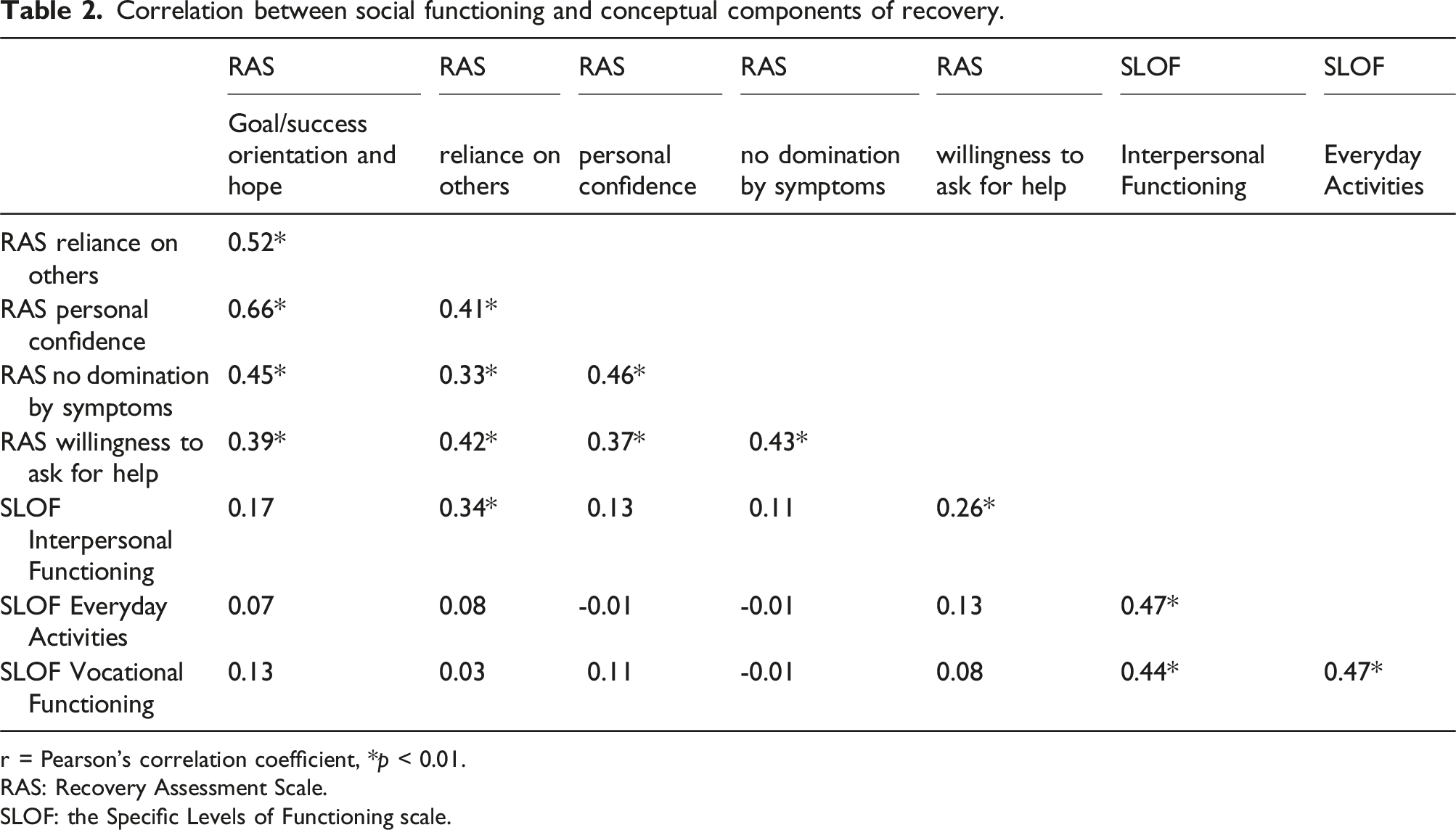
r = Pearson’s correlation coefficient, *p < 0.01.
RAS: Recovery Assessment Scale.
SLOF: the Specific Levels of Functioning scale.
Hierarchical multiple regression analysis with reliance on others as the dependent variable.
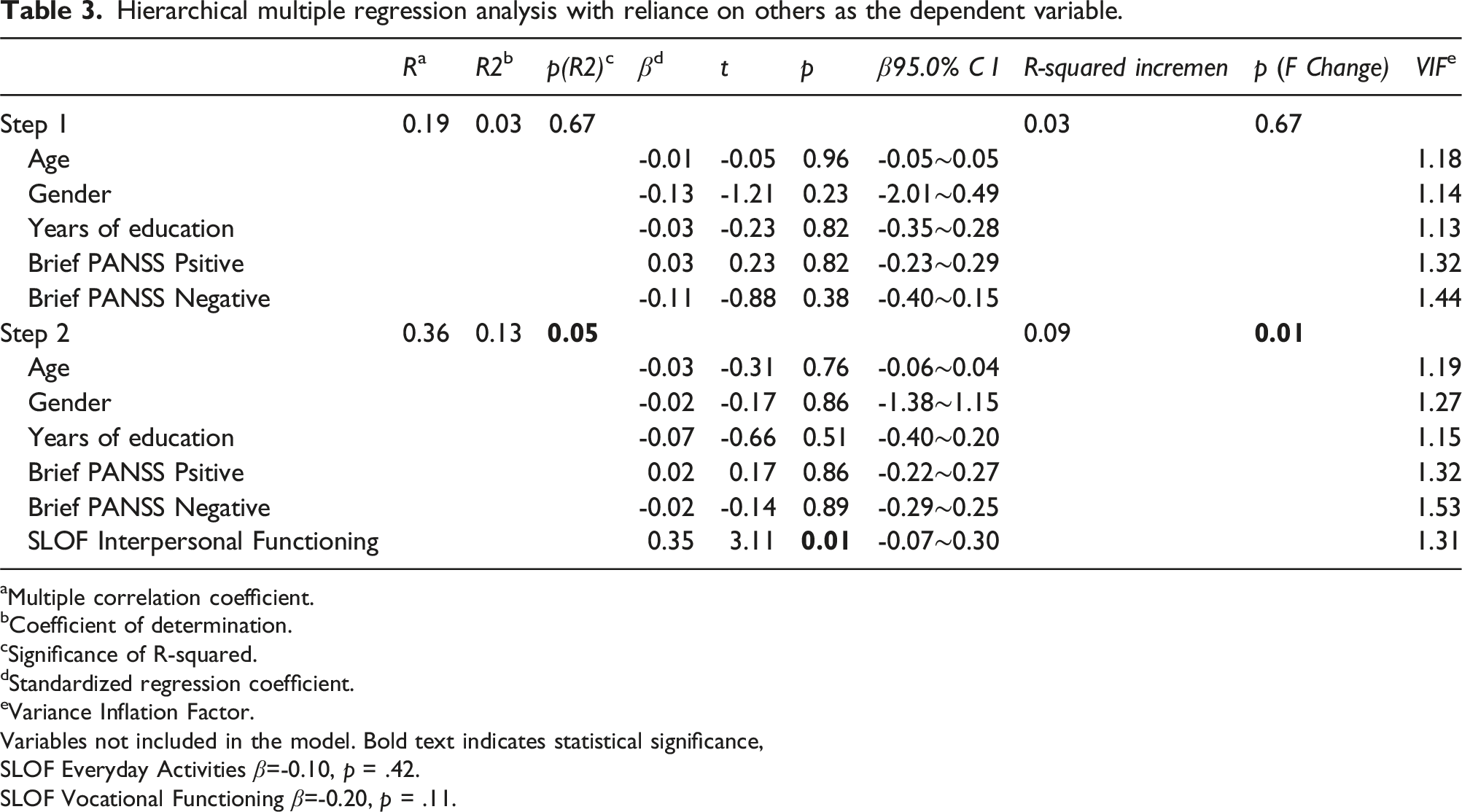
aMultiple correlation coefficient.
bCoefficient of determination.
cSignificance of R-squared.
dStandardized regression coefficient.
eVariance Inflation Factor.
Variables not included in the model. Bold text indicates statistical significance,
SLOF Everyday Activities β=-0.10, p = .42.
SLOF Vocational Functioning β=-0.20, p = .11.
Hierarchical multiple regression analysis with willingness to ask for help as the dependent variable.
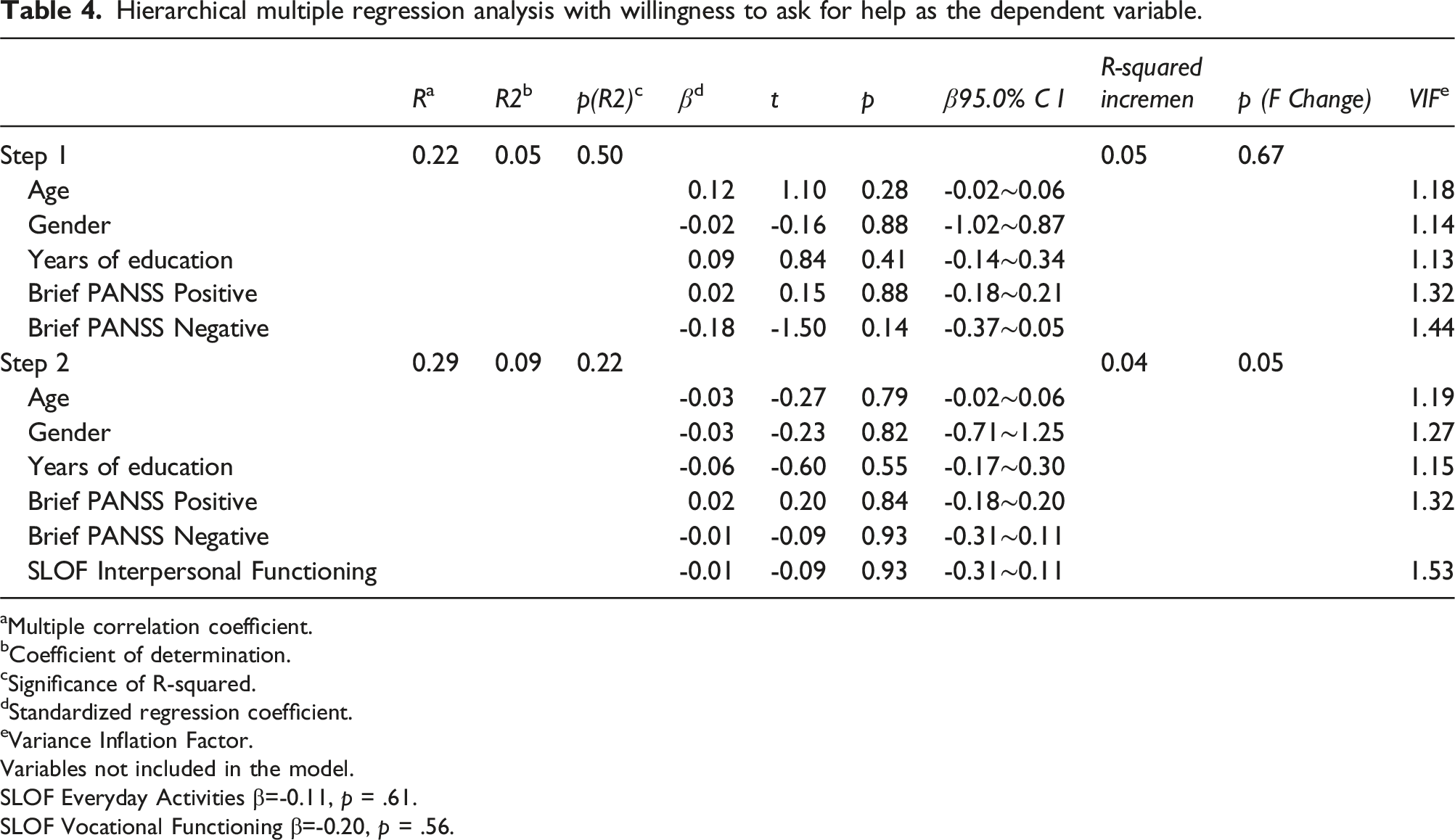
aMultiple correlation coefficient.
bCoefficient of determination.
cSignificance of R-squared.
dStandardized regression coefficient.
eVariance Inflation Factor.
Variables not included in the model.
SLOF Everyday Activities β=-0.11, p = .61.
SLOF Vocational Functioning β=-0.20, p = .56.
Discussion
This study focused on the relationship between personal recovery and social functioning in schizophrenia. Interpersonal Functioning was significantly associated with Reliance on Others and Willingness to Ask for Help. Additional analyses confirmed its significant contribution to Reliance on Others.
Relationship between “reliance on others” and “interpersonal relationships”
This study identified a weak-to-moderate correlation between social functioning and personal recovery. However, contrary to existing consensus (Leendertse et al., 2021; Van Eck et al., 2018), their relationship appeared only partial. Correlation analyses showed significant associations only between the SLOF subdomain “Interpersonal Functioning” and the RAS domains “Reliance on Others” and “Willingness to Ask for Help.” Secondary analyses confirmed that interpersonal functioning significantly influenced “Reliance on Others,” explaining 13% of its variance. These findings suggest that interpersonal functioning plays a greater role than sociodemographic factors and psychiatric symptoms. This aligns partially with Van der Krieke et al. (2019), who reported a correlation between RAS total scores and SFS Interpersonal Functioning sub-scores. The association between higher interpersonal functioning and greater reliance on others appears to be opposite to each other, however, the RAS “Reliance on Others” domain includes statements like “Even when I don’t believe in myself, other people do.” This implies that interpersonal functioning fosters trust rather than passive dependence (Chiba et al., 2010). Enhancing interpersonal functioning may thus facilitate recovery in schizophrenia, a condition marked by communication impairments (Adamczyk et al., 2016), high loneliness prevalence (80%) (Suman et al., 2023), and low social motivation (Hajdúk et al., 2024). Unexpectedly, despite moderate correlations among social functioning subdomains, only interpersonal functioning was linked to personal recovery. Partial correlation analyses controlling for Interpersonal Functioning revealed small correlations between Vocational Functioning and Reliance on Others (r = −0.14) and between Activities and Reliance on Others (r = −0.10). This suggests that interpersonal functioning may mediate these relationships or that social functioning domains differ in their associations with personal recovery. Furthermore, our findings align with Strassnig et al. (2015), who reported a significant moderate correlation between social functioning and negative symptoms, as well as a weaker but significant correlation with positive symptoms. While the relationship between social functioning and positive symptoms has received less attention (Rabinowitz et al., 2012), a meta-analysis by Santesteban-Echarri et al. (2017) supported a significant association. However, the mean positive symptom score in our sample was relatively low (mean = 2.2), suggesting a limited impact on social functioning. Additionally, no significant associations were found between RAS total scores and age, education, or clinical symptoms, diverging from Van Eck et al. (2018). While SLOF scores correlated with cumulative time-related factors such as education and illness duration, RAS scores showed no such associations, suggesting that personal recovery may reflect immediate subjective experiences rather than accumulated past experiences.
Clinical implications
This study has several clinical implications. Outpatients with schizophrenia with lower interpersonal functioning may struggle more with trusting others, possibly due to interpersonal impairments. Addressing these challenges requires considering the interplay of symptoms, disabilities (Chen et al., 2020), individual values, and life histories (Kasai & Fukuda, 2017; Slade & Longden, 2015). This underscores the need for evidence-based interventions, including recovery-oriented services (Khanthavudh et al., 2023; Slade et al., 2014), Social Skills Training (SST; Kurtz & Mueser, 2008), and Cognitive-Behavioral Therapy (CBT; Wykes et al., 2008). These approaches may help clinicians foster trust and build therapeutic relationships. Occupational therapists, in particular, can tailor interventions to individual needs to enhance trust (Yilmaz et al., 2008). However, larger samples and advanced methodologies, such as structural equation modeling, are needed to further clarify these relationships.
Limitations
This study has several limitations. First, recruitment from a single facility with non-probability sampling limits generalizability. Second, the causal link between “Reliance on Others” and “Interpersonal Functioning” remains unclear. Despite a moderate model fit, definitive conclusions cannot be drawn. Third, findings may not apply to outpatients with severe psychiatric symptoms, and depressive symptoms were not considered. Lastly, as noted, recovery is shaped by personal values, which vary. Future research should incorporate qualitative assessments to capture these nuances.
Conclusion
This study identified a significant relationship between the social functioning subdomains “Interpersonal Functioning” and “Reliance on Others” in recovery. Despite limitations, the findings highlight the need for interventions targeting interpersonal skills to foster recovery.
Footnotes
Acknowledgements
We express our gratitude to Dr Takano and Dr Nishijima of Nasukougen Hospital and the faculty of the International University of Health and Welfare for their cooperation and support in conducting this study. Finally, we would like to thank Editage (![]() ) for English language editing. We sincerely thank all participants and their families. We also appreciate Director C, the physicians, staff, and mentors at [Hospital Name] for their invaluable support.
) for English language editing. We sincerely thank all participants and their families. We also appreciate Director C, the physicians, staff, and mentors at [Hospital Name] for their invaluable support.
Authors’ contributions
Seiichi Watanabe: Conceptualization, Methodology, Validation, Formal Analysis, Investigation, Data Curation, Visualisation, Project Administration, Writing—Original draft preparation, editing the manuscript, and finalising it. Takamichi Taniguchi: Conceptualization, Methodology, Resources, and Supervision. Motoko Sugihara: Conceptualization, Methodology, Resources, Supervision, and Project Administration.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.