
Abstract
Rapid and accurate trustworthiness judgments are important during successful day-to-day social interactions because they can influence the decision whether to approach someone and initiate social interaction. The aim of the present study was to analyze associations between these judgments and self-reported and clinician-rated social functioning. The sample consisted of 48 patients with schizophrenia spectrum disorders and 35 healthy controls matched for age, gender, and educational level. A trustworthiness task, subjective, and clinician-rated scales for social functioning were administered to both samples. Trustworthiness judgments did not differ between patients and healthy controls. Both groups were able to discriminate between trustworthy and untrustworthy faces. Trustworthiness ratings were associated with self-reported and clinician-rated measures of interpersonal functioning in patients with schizophrenia. Despite the absence of differences between groups, in patients with schizophrenia, a tendency to mistrust based on facial appearance was related to worse functional outcome, predominantly in the domain of disturbed interpersonal functioning. This study highlights the importance of future research into social–cognitive biases in schizophrenia.
Introduction
Accurate processing of social stimuli (social cognition) is necessary for successful social interactions (Adolphs, 2009) and link between social–cognitive deficits and impaired real-world functioning in patients with schizophrenia has been well established (Fett et al., 2011; Pinkham, Penn, Green, & Harvey, 2016). Buck, Healey, Gagen, Roberts, and Penn (2016) divided social cognition into two factors: social–cognitive skills (e.g., the theory of mind and emotion recognition) and social–cognitive biases (hostile and aggressive attributional style). Empirical research has focused predominantly on social–cognitive skills, and not on the social–cognitive biases. These biases can lead to problems in everyday social interactions, similar to difficulties caused by impaired social skills (Buck, Pinkham, Harvey, & Penn, 2016).
Social–cognitive biases in schizophrenia are usually measured with attributional style tasks, which are based on the interpretation of social scenarios. Based on the locus of attributions, previous studies identified two core attributional processes prominent in patients with persecutory delusions. Patients tend to blame other people rather than situation for experiencing negative outcomes, which is called personalizing bias. Externalizing bias (also known as a self-serving bias) represents tendency to attribute positive rather than negative events to oneself (Bentall, Corcoran, Howard, Blackwood, & Kinderman, 2001; Kinderman & Bentall, 1996). The core bias related to paranoia is a tendency to perceive hostile intentions in behavior of other people. This hostility bias is especially prominent in ambiguous social situations (Combs, Penn, Wicher, & Waldheter, 2007).
Human facial expressions are rich source of social information (Adolphs, 2002) and processing of face physiognomy represents another option for studying social–cognitive biases in schizophrenia. Faces with neutral expression can be evaluated in several dimensions, for example, trustworthy, social, dominant, aggressive, and attractive (Oosterhof & Todorov, 2008; Todorov, Baron, & Oosterhof, 2008). These ratings are often called social trait judgments (Trémeau et al., 2015). Trustworthiness judgments are particularly relevant in day-to-day interactions because they can influence the decision whether to approach someone and initiate social interaction. Studies in healthy participants showed that inferences with regard to trustworthiness from faces are made extremely rapidly and automatically and that the presentation of faces for 100 ms is sufficient to form relatively accurate social judgments (Todorov, Pakrashi, & Oosterhof, 2009).
A large-scale study (Pinkham et al., 2016) using a comprehensive social–cognitive battery did not find relationships between trustworthiness judgments and functional outcome; however, healthy controls and patients with schizophrenia differed in the overall level of trustworthiness they assigned to faces, and the effect size was small (d = 0.27). Couture et al. (2010) compared healthy controls, individuals with high functioning autism, and individuals with schizophrenia. They found similar bias in both clinical groups. Untrustworthy faces were perceived as more trustworthy than in the control group, and no differences between the clinical groups were found. Additional analyses based on the actual symptom severity provide new insights how symptom profile in schizophrenia seems to influence trustworthiness judgments. A subgroup of patients with prominent paranoid symptoms (score ≥4 on the Positive and Negative Syndrome Scale–Suspiciousness item) rated trustworthy faces more negative than controls. This aligns with other studies that found that trustworthiness ratings by patients are negatively associated with the severity of positive symptoms (Haut & MacDonald III, 2010) and with the elevated paranoid ideation in healthy individuals (Kirk, Gilmour, Dudley, & Riby, 2013). The hostile and aggressive attributional biases in schizophrenia are associated with social functioning, predominantly in the domains related to the interpersonal conflict reported by the informants (Buck, Pinkham, et al., 2016).
To synthetize current evidence, it seems that trustworthiness judgments from facial expressions are related to specific subgroups of patients predominantly with high levels of paranoia. Relationships to functional outcome have not been well established and seem to be more strongly related to interpersonal aspect of functional outcome. Using only global functional outcome ratings can obscure specific patterns of relationships between social–cognitive biases and interpersonal aspects of social functioning. Using self-report measures in conjunction with clinician-rated scales, we aimed to find out which domains of functional outcome are associated with social–cognitive biases, especially evaluation of trust. We aimed to test the following hypotheses: (i) patients with schizophrenia judge faces as less trustworthy than controls, (ii) in patients with schizophrenia, lower trustworthiness ratings are associated with more severe problems in interpersonal functioning, and (iii) the severity of positive symptoms is related to lower trustworthiness ratings.
Method
Participants
The sample consisted of 48 participants with schizophrenia spectrum disorders (schizophrenia, schizoaffective disorder, and acute polymorphic psychotic disorder with symptoms of schizophrenia). Diagnoses were established by trained psychiatrists according to the International Classification of Diseases version 10 criteria (World Health Organization, 1992). Patients were assessed either before discharge (N = 18) from inpatient treatment or during attendance at an outpatient care center (N = 30). Patients with other types of psychotic disorder and those unable or not willing to provide informed consent form were not eligible to participate in the study. The healthy control group consisted of 35 participants without self-reported history of mental illness or other health conditions that might influence the performance of study assessments. All participants with schizophrenia were recruited from Psychiatric department of University Hospital of Bratislava. Healthy controls were recruited from the local community in Bratislava. Samples were matched on age, gender, and educational level. Demographic and clinical variables are presented in Table 1. The study was approved by the Institutional Ethics Committee of the University Hospital of Bratislava, Slovakia. All participants gave informed consent before participation in the study.
Demographic and clinical characteristics.

Note. N = frequency. M = mean. U = Mann–Whitney U test. χ2 = chi-square test. CGI-SCH = Clinical Global Impression-Schizophrenia. PSP = Personal and Social Performance Scale. SFQ = Social Functioning Questionnaire. SD = standard deviation.
*p = 0.05; ***p < 0.001.
Measures
Trustworthiness task
This task consists of 40 images from the Todorov Lab Database (Oosterhof & Todorov, 2008; Todorov et al., 2008), containing images of Caucasian male faces digitally morphed to different trustworthiness levels by changing the face physiognomy. Each person in the database can be morphed to look trustworthy or untrustworthy based on the model of face perception. Model represents faces using two broad dimensions (trustworthiness and dominance). Authors proposed that facial cues are used for evaluation of faces along these dimensions. Faces were used to measure the following trustworthiness levels: −3 SD, −1 SD, +1 SD, and +3 SD. SD represents standard deviation from neutral face in terms of trustworthiness. The mean ratings for untrustworthy faces were calculated as mean for −1 SD and −3 SD faces and those for trustworthy faces as mean for +1 SD and +3 SD. Participants were asked to rate the face on the scale from 1 = not at all trustworthy to 9 = extremely trustworthy. The following instruction was used: This experiment tests your ability to judge how trustworthy a person’s face looks. We are interested in the “first impressions” so we want you to just go with your “gut feeling” and don’t spend too much time studying the faces. Every face was used only in one expression (trustworthiness level) when presented. Response time was not restricted but we encouraged participants to use “gut feeling.” The task novelty lies in using digitally morphed pictures instead of photographs. The majority of studies of trustworthiness judgments in schizophrenia have used Adolphs’ version of trustworthiness task (Adolphs, Tranel, & Damasio, 1998) which consists of older Black and White stimuli of unfamiliar people.
Personal and social performance scale
Assessed in a structured interview format, this scale measures four domains of social functioning: social activities, social relationships, self-care, and disturbing and aggressive behavior. The total score (0–100) is calculated from each subscale scores based on a validated algorithm (Morosini, Magliano, Brambilla, Ugolini, & Pioli, 2000). The total score and subscale scores were used in the statistical analyses. A higher total score indicates better overall functioning; lower domain scores indicate better functioning, coded 1 as “absence of problems,” up to 6 as “presence of very severe problems.”
Social Functioning Questionnaire
The Social Functioning Questionnaire (SFQ; Tyrer, 2005) is an 8-item self-report measure of social functioning. The scale is based on the social functioning schedule (Remington & Tyrer, 1979). Items measure different domains of social functioning from interpersonal relationships, social isolation, work, satisfaction with the spare time, and so on. The mean score is considered as a global level of social functioning, with higher scores indicating poorer social functioning.
Clinical Global Impression–Schizophrenia
The Clinical Global Impression–Schizophrenia (CGI-SCH) scale is based on the clinical impression during the week before assessment. The Scale consists of 5 items, the severity of symptoms (positive, negative, cognitive, and depressive), and overall severity is measured on a 7-point Likert-type scale from 1 = normal, not ill to 7 = among the most severely ill (Haro et al., 2003). The scale was administered by trained psychiatrists.
Statistical analysis
The SPSS v. 20 was used for statistical analyses. Repeated-measures analysis of variance (ANOVA) with trustworthiness as a within factor (trustworthy vs. untrustworthy faces) and group as a between factor (healthy control vs. schizophrenia) was used for evaluation of group differences in the trustworthiness task. We used only trustworthy versus untrustworthy faces, not all 4-level due to following correlation analysis with symptom severity and functional outcome. Our aim was to reduce the total number of pair correlations and to make interpretation of trustworthiness levels more straightforward. Comparison of trustworthy and untrustworthy faces was used in previous studies (Couture et al., 2010; Pinkham, Hopfinger, Ruparel, & Penn, 2008). The Spearman rank coefficient was used for the assessment of strength of the relationships between trustworthiness judgments, social functioning, and symptoms. A nonparametric correlation coefficient was used due to the ordinal character of the data and violations of normality assumptions for the Personal and Social Performance (PSP) scale and CGI-SCH. Post hoc analyses on the individual item level of SFQ were conducted to explore which domains of functional outcome are related to trustworthiness judgments.
Results
Groups were matched on gender, χ2(1) = 1.452, p = 0.228; age, U = 808.5, p = 0.771; and total years of education, U = 665.5, p = 0.100. Significant group differences were found in employment status, χ2 (2) = 6.712, p = 0.035, and family status, χ2 (4) = 44.728, p < 0.001, with patients being significantly less likely to be employed and married. Table 1 presents means and SDs for social functioning measures and the severity of symptoms.
Group differences in trustworthiness ratings
A significant main effect of face type emerged, F(1, 81) = 184.894, p < 0.001, η2 = 0.695, 1−β = 1. Group × Face type interaction, F(1, 81) = 1.707, p = 0.195, η2 = 0.021, 1−β = 0.252, and main effect of group, F(1, 81) = 0.707, p = 0.403, η2 = 0.009, 1−β = 0.132, were not detected. The mean ratings of trustworthy faces (M HC = 5.22 and SD HC = 1.16 vs. M SCZ = 4.86 and SD SCZ = 1.46) were higher than those for untrustworthy faces (M HC = 3.37 and SD HC = 0.75 and M SCZ = 3.33 and SD SCZ = 1.24) in both groups. Mean values and 95% confidence intervals are presented in Figure 1. We utilized second repeated-measures ANOVA with four levels of face type (−3 SD, −1 SD, +1 SD, +3 SD trustworthiness levels as described in the “Trustworthiness task” section). Results were comparable with previous analysis. We found significant effect of face type and nonsignificant between groups differences and interaction.

Results of ANOVA for group comparison in trustworthiness task. ANOVA = analysis of variance.
Trustworthiness rating, psychopathology, and psychosocial functioning
Trustworthiness ratings in patients with schizophrenia were not associated with any symptom domain nor with the overall severity of the illness (all p values > .247). Judgments of trustworthy faces were negatively associated with the severity of impairments in the useful social activities (r s = −.316, p = .029) and self-care domains (r s = −.328, p = .023). Mean ratings of trustworthy (r s = −.293, p = .043) and untrustworthy faces (r s = −.322, p = .026) were negatively associated with the severity of disturbing and aggressive behavior. The overall PSP total score was associated with the ratings of untrustworthy faces on a trend level (r s = .260, p = .075). The total score for the SFQ was not related to the trustworthiness ratings. Based on the post hoc analysis of SFQ items, only the item ‘I get on well with my family and other relatives significantly correlated with the rating for trustworthy faces (r s = −.378, p = .008). Table 2 presents a correlation matrix for patient sample. In the healthy controls, trustworthiness ratings were not significantly correlated with PSP or SFQ.
Correlation analysis (patients sample).
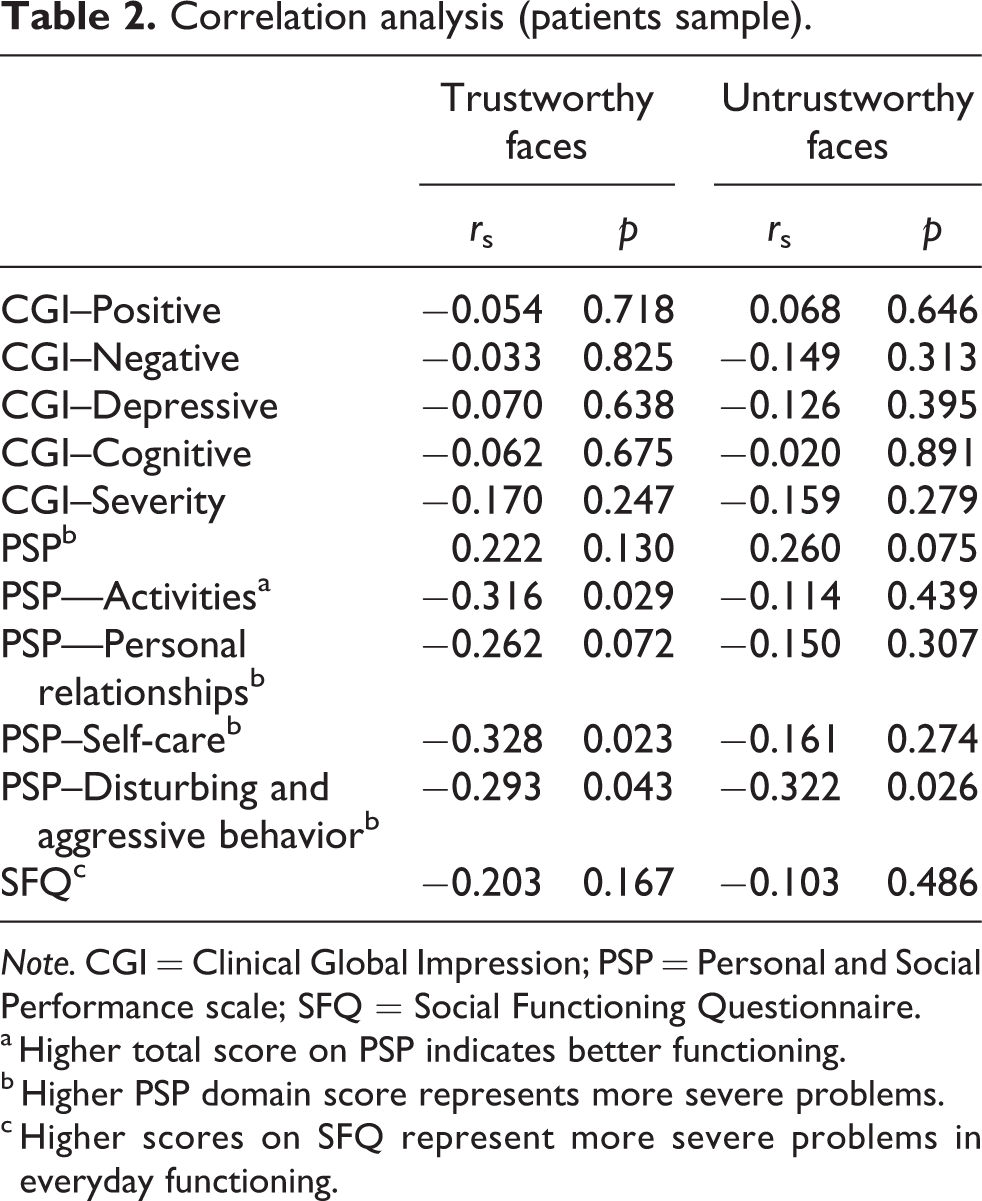
Note. CGI = Clinical Global Impression; PSP = Personal and Social Performance scale; SFQ = Social Functioning Questionnaire.
a Higher total score on PSP indicates better functioning.
b Higher PSP domain score represents more severe problems.
c Higher scores on SFQ represent more severe problems in everyday functioning.
Discussion
Contrary to previous findings (Pinkham, Hopfinger, Pelphrey, Piven, & Penn, 2008; Pinkham et al., 2016), we detected no differences between healthy controls and patients with schizophrenia in their ratings of trustworthiness of the faces. Although patients rated the faces as numerically less trustworthy than the controls did, this was not statistically significant, possibly due to insufficient power associated with the current sample size because the magnitude of differences between groups was similar to results previously reported by Pinkham, Penn, Green, and Harvey (2016) using different trustworthiness judgments task. Based on these findings, it is necessary to design future studies with larger samples with sufficient power to detect small differences. Another implication is that biases are present in both types of trustworthiness task, real faces, and computer-generated pictures. Previous study (Buck, Pinkham, et al., 2016) used photographs of real people instead of computer-generated images of faces. This difference can at least partially explain the absence of differences between groups in our study. Our version of the trustworthiness task was designed to measure how changes in physiognomy influence ratings. Both groups were equally able to discriminate between trustworthy and untrustworthy faces. Real faces seem to be more ambiguous (not solely based on changes of parameters from face perception model) and can be considered as better stimuli to evaluate biases than computer-generated pictures. Direct comparison of real and computer-generated faces in assessment of trustworthiness is needed to test this hypothesis.
We confirmed our hypothesis that the trustworthiness ratings would be associated with everyday interpersonal functioning. Associations were found predominantly with the severity of disturbing and aggressive behavior toward other people measured by the clinician-rated PSP. This domain reflects such behavior as extensive arguing with others, verbal aggression, physical aggression, and inappropriate behavior. The global subjective rating of functioning was not related to social judgments. Nevertheless, on the item level, we found that patients with more severe deficits in interactions with their close family and relatives tended to rate faces as less trustworthy. Aggressive and disturbing behavior can more frequently occur in the close family context. Home environment of patients is characterized with high level of expressed emotions, extensive criticism, hostility, and overprotection (Kavanagh, 1992). Another interpretation might be that family members, due to their own impairments in mentalizing, can be role models with insufficient social skills (Lavoie et al., 2014).
Buck, Healey, et al. (2016) reported similar findings showing that social–cognitive biases predict only specific interpersonal aspects of social functioning, predominantly the severity of interpersonal problems and conflicts. Trémeau et al. (2015) found that social judgments also predict social skills in schizophrenia. In their research, where authors let patients to evaluate faces on the several dimensions such as social, weird, intelligent, and so on. Trustworthiness ratings were not predictor of social skills. Clinician assessments are an important source of information about the patient functioning and are related to the patient performance. In our study, both self-reported and clinical-rated measures of interpersonal functioning were related to social judgments. Social–cognitive biases seem to be more closely related to interpersonal functioning than to instrumental activities such as self-care. Absence of other association on item level of SFQ can also be partially explained by lack of insight in problems with introspective accuracy (Harvey, Pinkham, & Penn, 2017). For this reason, combination of different sources of information about patients’ functioning is necessary.
Trustworthiness judgments are typically not made in isolation. In the everyday life, the use of information from the social context is crucial for the generation of accurate evaluations of people. Successful interactions require holding a quantity of relevant information in mind, and using this information or suppressing it at appropriate times (Cohen, Barch, Carter, & Servan-Schreiber, 1999). A study specifically analyzing the role of context processing in social–cognitive abilities (Chung, Mathews, & Barch, 2011) found that the deficit in context processing was associated with a more severe impairment in higher level of social–cognitive inference (e.g., theory of mind/mentalizing).
We did not find any association between trustworthiness ratings and symptom severity. Previous studies have found associations between trustworthiness judgments and, especially, paranoid symptoms (Haut & MacDonald III, 2010). The context in which judgments are made can trigger more distrustful judgments of other people. Pinkham, Hopfinger, and Penn (2012) found that paranoid patients rated faces as more untrustworthy using fMRI scanning but not in standard assessment that were used in the present study. Social traits judgments vary dynamically according to the context and patient symptom severity. Negative or threat-evoking situations can elicit more negative judgments (Hooker et al., 2011).
Recent studies have advocated for inclusion of various situational contexts in social–cognitive bias research because appropriate processing of ambiguous and accidental social situations is predictor of functional outcome (Buck et al., 2017). Buck et al. (2018) found that bias toward intentionality is elevated in schizophrenia. Patients tend to perceive intentions in situations which healthy people perceived as accidental. They also found that patients had problems in controlling their automatic judgments especially under the time pressure, which can resemble negative or stressful situation occurring in real life. Inability to control judgments, including trustworthiness, due to cognitive impairment (Fioravanti, Bianchi, & Cinti, 2012) might explain how these judgments are related to the problems in interpersonal relationships. Another mechanism which also explains this relationship is aberrant perception of social threat (Pinkham et al., 2014). Future studies should model these complex relationships between different biases and impairments present in patients with schizophrenia.
The current findings should be interpreted with due consideration of the limitations of the study. Firstly, only the information about patient symptom severity was limited to clinical assessments with CGI-SCH. Using broad symptom severity measures like CGI-SCH may obscure the role of individual symptoms. Using self-report measures of paranoia or complex objective rating scales for paranoia will be necessary for future research because different aspects of paranoia predict social functioning across continuum from healthy to pathological (Hajdúk, Klein, Harvey, Penn, & Pinkham, 2018). Future studies should also test mediation model in which paranoia mediates relationships between social–cognitive biases and interpersonal functioning and the stability of these judgments (acute vs. stable phases of the illness). Direct comparison of schizophrenia, high functioning autism, and social anxiety can be very useful for identification of share and unique aspect of this bias across diagnostic boundaries. Currently we do not know whether this bias predicts interpersonal functioning in all groups. Another limitation of the study was low power to detect between-group differences. Strength of association between trustworthiness judgments and functioning was small to moderate. Replication of findings with well-powered study with larger sample is warranted.
In sum, our results did not support our predictions of differences in trustworthiness judgments between patients and controls. Patients were able to distinguish between trustworthy and untrustworthy faces. Importantly, the positive associations between trustworthiness findings and self-reported as well as clinician-rated social functioning of the patients detected in this study suggest that social–cognitive bias associated with trust has meaningful implications for everyday interpersonal functioning. In clinical practice, the application of specific training that targets and improves social–cognitive biases such as metacognitive training (Moritz & Woodward, 2007; Woodward, Balzan, Menon, & Moritz, 2014) may be useful in enhancing interpersonal functioning of patients, thus improving their quality of life.
Footnotes
Acknowledgement
The authors would like to thank Dr. Stephen Z. Rapcsak for providing us with the trustworthiness task. The authors would also like to thank Dr Zuzana Kasanova for her comments on the earlier version of this manuscript.
Author contribution
Michal Hajdúk, Ján Pečeňák, Viera Kořínková, and Anton Heretik designed the study. Michal Hajdúk, Dana Krajčovičová, and Miroslava Zimányiová participated on the data collection. Miroslava Zimányiová conducted initial analysis and wrote the initial draft. All authors critically reviewed the article. All authors contributed to and have approved the final manuscript. Data will be made available upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Slovak Psychiatric Association SMA under grant no 01/2015, publication grant of Slovak Psychiatric Association SMA.