
Abstract
Functional deficits are a hallmark of schizophrenia spectrum disorders, but much debate still exists over why and how they originate. One model suggests that disturbances in social functioning are a result of metacognitive deficits or a failure to integrate information to form more complex ideas of themselves and others. It is unclear if this social dysfunction is present across different symptom presentations. We examined the relationship of metacognition, symptoms, and social functioning among a sample of adults with schizophrenia spectrum disorders (N = 334). A latent class analysis produced a four-class model. Groups were classified as follows: diffuse symptoms/moderately impaired social functioning (Class 1), positive and hostility symptoms/mildly impaired social functioning (Class 2), minimal symptoms/good social functioning (Class 3), and negative and cognitive symptoms/severely impaired social functioning (Class 4). Class 3 demonstrated better overall metacognitive capacity than both Classes 1 and 4 but did not differ significantly from Class 2. Classes 2 and 3 both demonstrated better interpersonal functioning than Classes 1 and 4. Together, these findings provide support for models of poor functioning that stem from fragmentation of an individual’s experience, leading to diminished abilities to form meaningful connections with others. Additional interpretations, limitations, and research implications are discussed.
Introduction
Bleuler (1952 [1911]) proposed that schizophrenia is a heterogenous set of disorders all characterized by the splitting or fragmentation of one’s experience, resulting in an interrupted life course. Specifically, he suggested that disturbances occur in association, affect, and ambivalence which then result in withdrawal from the world, which he characterized as autism. As a consequence of these disturbances, the meanings people make of their experiences, and thus support goal-directed behaviors, disappear. As such, the framework that enables an enduring sense of connection to the social world also disappears (Maatz, Hoff, & Angst, 2015). Bleuler’s view stood in contrast to those of Kraepelin (2002 [1919]), who posited that organic, metabolic processes caused deficits in volition and affect, which in turn caused the loss of adaptive functioning (Noll, 2011).
Researchers have continued to explore the notion that social dysfunction in schizophrenia is a result of fragmentation. One model has proposed that persons with this condition experience disturbance in social functioning as a result of metacognitive deficits or a failure to integrate information into a complex sense of oneself, others, and their place in a larger community (Lysaker, Hamm, Hasson-Ohayon, Pattison, & Leonhardt, 2018). This perspective is based on the integrated model (Lysaker & Dimaggio, 2014; Lysaker et al., this issue), wherein metacognition refers to a spectrum of processes ranging from awareness of discrete thoughts, feelings, and bodily experiences to the synthesis of those experiences into a larger sense of oneself and others as unique beings. Disturbances in these processes could thus potentially explain why individuals with schizophrenia often demonstrate a fragmented sense of themselves and others (Lysaker et al., 2018). As such, it is suggested that metacognitive deficits leave individuals without a coherent understanding of either their own or others’ experiences, needs, and wishes, thus leading to social dysfunction (Bonfils, Luther, Buck, George, & Lysaker, 2016; Lysaker & Klion, 2017).
Several studies have put forth evidence that fragmentation resulting from metacognitive deficits may contribute to social dysfunction. As reviewed elsewhere (Lysaker et al., this issue), evidence suggesting that metacognitive deficits can be commonly observed in schizophrenia and are a barrier to recovery has steadily accumulated. Cross-sectional research has also found that the lower levels of metacognitive abilities predict concurrent deficits in social functioning (Bröcker et al., 2017; Lysaker et al., 2005, 2010a, 2011a; Massé & Lecomte, 2015), independent of other factors thought to contribute to these deficits, including dysfunctional beliefs (James et al., 2016) and social cognition (Lysaker et al., 2013). Other studies have found metacognition predicted social functioning prospectively over a 5-month interval (Lysaker et al., 2011b) and that changes in metacognitive capacity were associated with improvements in social skills (Inchausti et al., 2017a). Support for a link between metacognition and social functioning can also be found in research suggesting that metacognitive deficits predict multiple psychological constructs and biological processes believed to be cornerstones of social functioning, including intrinsic motivation (Luther et al., 2016, 2017), complexity of social schema (Lysaker et al., 2010b), anhedonia (Buck et al., 2014), aggression (de Jong et al., 2018), sense of social connection (Kukla, Lysaker, & Salyers, 2013), empathy (Bonfils, Lysaker, Minor, & Salyers, 2018; WeiMing, Yi, Lysaker, & Kai, 2015), and levels of oxytocin (Aydin, Lysaker, Balıkçı, Ünal-Aydın, & Esen-Danacı, 2018).
Importantly, one limitation of the existing research exploring the relationship between metacognition and social function in schizophrenia is that, due to small sample sizes, studies have not explored the way in which metacognitive deficits may be differentially related to social functioning across varying symptom presentations. An example of clinical features that may differentially relate to social functioning is positive and negative symptoms. Positive symptoms have been traditionally thought to affect social functioning when they erode trust in others or lead to anomalous experiences that others cannot understand, contributing to social isolation (Hooker et al., 2011; Yanos, Roe, Markus, & Lysaker, 2008). In contrast, negative symptoms interfere with the detection and expression of emotional experiences. These skills are the basis for intersubjectivity and when they are derailed can impact individuals’ ability to connect with others.
To address the question of whether metacognition is related to social functioning across persons with different symptom presentations, the present study examined the relationships of metacognition, symptoms, and social functioning among a relatively large sample of adults with schizophrenia spectrum disorders. Specifically, we had two aims. First, we sought to identify different configurations of social functioning and symptoms using latent class analysis (LCA). We chose this statistical approach to classification rather than methods that employ a priori predictions to minimize the effects of any preexisting biases regarding which underlying symptom and social functioning profiles exist naturally. The second aim was to explore whether those with impaired social functioning experienced greater metacognitive deficits regardless of symptom profile. We chose not to include metacognition in the LCA because we wished to identify individuals with varying symptom profiles (psychiatric and functioning) and then see how metacognition varied across them. We did not wish to base the classification of the groups on metacognition, as this would have obfuscated the distinct symptom constellations that create these varying groups. We predicted we would identify a group with good, or unimpaired, social functioning and relatively less severe symptoms and groups with impaired social functioning and varying symptoms presentations: primarily positive symptoms, primarily negative symptoms, and a group with diffuse positive and negative symptoms. We predicted all impaired social functioning groups would show greater deficits in metacognition than the good social functioning group, regardless of the symptom presentation.
Method
Participants
Participants were 334 adults receiving outpatient mental health treatment with a diagnosis of schizophrenia (230) or schizoaffective disorder (104) based on the Structured Clinical Interview for DSM-IV (SCID-IV; First, Spitzer, Gibbon, & Williams, 2002). Individuals were participants in studies of the effects of psychosocial rehabilitation; recruitment and study procedures occurred at a Veterans’ Affairs Medical Center in Indiana as well as community mental health centers in Indiana and New Jersey. Inclusion criteria required that individuals were in a non-acute phase of illness, defined by no hospitalizations or changes in housing or medication within 30 days of study enrollment. The mean age of the participants was 43.54 years (range: 18–71; SD = 12.58). The sample was 77.2% male (n = 257) and 22.8% female (n = 76), and the mean years of education were 11.53 years (range: 2–24; SD = 3.23). Additional descriptive statistics for the full sample can be found in Table 1.
Demographic and clinical characteristics of full sample (N = 334).

Note. MAS = Metacognition Assessment Scale; QLS = Quality of Life Scale; PANSS = Positive and Negative Syndrome Scale.
Instruments
Indiana Psychiatric Illness Interview (IPII; Lysaker, Clements, Plascak-Hallberg, Knipscheer, & Wright, 2002): The IPII is a semi-structured interview designed to encourage individuals to provide a sample of how they think about challenges in their life, particularly those related to psychiatric illness. The interview typically lasts 30 to 60 min, during which the interviewer asks participants to talk about: (1) the story of their life thus far; (2) whether they think they have a mental illness and, if so, how that has affected and not affected their thoughts, emotions, and behaviors; (3) the influence the condition has had on their lives as well as their influence on their condition; (4) the influence of their condition on others and other’s influence over their condition; and (5) their thoughts about their future. The IPII elicits a nuanced account of psychiatric challenges that extend beyond the bounds of discussing psychiatric labels, and as such can serve as the basis for the assessments of metacognitive capacity.
Metacognition Assessment Scale–Abbreviated (MAS-A; Lysaker et al., 2005): The MAS-A was used to rate metacognition on the basis of a typed transcript of the IPII. The MAS-A is an adaptation of the MAS which was originally designed to study metacognition within psychotherapy transcripts (Semerari et al., 2003). The MAS-A transformed the original items of the MAS into four ordinal scales. These scales represent the following domains: self-reflectivity (S) or the extent to which individuals have a more fragmented or more integrated sense of self; awareness of others (O) or the degree to which a person has an integrated or fragmented sense of other people; decentration (D), which assesses the degree to which a person has an integrated or fragmented sense of their position within the larger community; and mastery (M), which assesses the degree to which a person can use metacognitive knowledge to respond to psychosocial challenges. The MAS-A frames metacognition as a series of increasingly complex and hierarchical processes, such that once it is determined that an individual did not attain a particular level, it is assumed that no further levels can be meaningfully achieved. Thus, higher scores represent higher levels of metacognitive abilities. Good inter-rater reliability and validity have been presented elsewhere with intraclass correlations ranging from .80 to .92 for the MAS-A subscales (Lysaker et al., 2005, 2011b, 2013; Nicolò et al., 2012).
Positive and Negative Syndrome Scale (PANSS; Kay, Fiszbien, & Opler, 1987): The PANSS is a 30-item rating scale used for measuring symptom severity of patients with schizophrenia and other mental disorders. In this study, we used the Bell, Lysaker, Beam-Goulet, Milstein, and Lindenmayer’s (1994) factor analytically derived model which produces the following five component scores: positive (scores ranging from 6 to 42), negative (ranging from 8 to 56), cognitive (ranging from 7 to 49), emotional discomfort (ranging from 4 to 28), and hostility (ranging from 4 to 28). Good inter-rater reliability was found in prior studies (Kay et al., 1987; Lysaker et al., 2013).
Quality of Life Scale (QLS; Heinrichs, Hanlon, & Carpenter, 1984): The QLS is a 21-item scale completed by a trained rater following a semi-structured interview where the interviewer asks the participant questions about his or her daily life and functioning. It has been widely used as a measure of psychosocial functioning due to its ability to detect strengths and weaknesses in the areas of interpersonal, community, and work functioning (Brekke, Raine, Ansel, Lencz, & Bird, 1997; Lysaker, Bell, Bryson, & Kaplan, 1998). For the purposes of this study, we focused on the interpersonal and intrapsychic subscales; the interpersonal subscale measures the frequency and nature of recent social interactions, and the intrapsychic subscale measures qualitative and foundational aspects of social interactions. Previous studies have found good intraclass correlations (Lysaker et al., 1998). Higher scores are suggestive of better levels of functioning.
Procedure
Procedures were approved by the local Institutional Review Boards. After written informed consent was obtained from participants, clinical psychologists confirmed diagnoses by meeting with participants and using the SCID-IV. Trained master’s-level research assistants subsequently administered the instruments as part of a baseline assessment. All measures were collected prior to randomization into a trial of psychosocial rehabilitation. Raters of the MAS-A were blind to PANSS and QLS scores, and PANSS and QLS raters were blind to IPII content or MAS-A scores.
Analytical strategy
Statistical analyses were conducted using SPSS version 24 and Mplus version 7 (Muthén & Muthén, 2012). First, we conducted an LCA in order to identify the potential presence of homogenous groups of individuals based on symptomatology and QLS intrapsychic foundations. Previous research suggests that the QLS intrapsychic scale is more closely tied to metacognition than is the interpersonal relations scale (Lysaker et al., 2013). In the second phase, we conducted a series of analyses of variance (ANOVAs) to compare demographics and MAS-A scores between groups and utilized the Bonferroni correction for multiple comparisons. In the third phase, we conducted a set of analyses of covariance to control for gender and education level. Finally, we conducted an exploratory ANOVA comparing the four groups on the QLS interpersonal subscale in order to further characterize the sample and confirm that individuals differed on social functioning using a separate index of social skill.
LCA can be employed to statistically identify latent homogenous groups (classes) of individuals from categorical and continuous multivariate data. The approach is based on probabilistic models of subgroup membership rather than arbitrary or theoretical approaches utilized in other clustering methods (Muthén & Muthén, 2012). In the present study, LCA was used to identify latent classes of individuals with schizophrenia spectrum disorders based on PANSS symptom subscales and the QLS intrapsychic subscale. Differences among classes on demographic variables and metacognitive ability were calculated using ANOVA and χ2 tests (significance level of p < .05).
The number of classes were not hypothesized a priori but were determined from an examination of model fit statistics, including entropy values, Akaike’s information criteria (AIC; Akaike, 1987), Bayesian information criteria (BIC; Schwarz, 1978), and sample size-adjusted BIC (ssaBIC; Sclove, 1987) (lower AIC, BIC, ssaBIC, and higher entropy values indicating better fit). Bootstrapped likelihood ratio tests (BLRT; McLachlan, 1987; Nylund, Asparouhov, & Muthén, 2007) and Lo–Mendell–Rubin (LMR; Lo, Mendell, & Rubin, 2001) tests, where n and n − 1 number of classes are compared, were also conducted.
Results
Five LCA models were estimated specifying between 1 and 5 latent classes. The AIC and ssaBIC values decreased with each successive class addition and thus did not readily discriminate a model of best fit. BIC values decreased for k = 2–4 classes, but increased for the k = 5 model, suggesting the five-class model is a poorer fit to the data. Entropy values were adequate and increased in value for most models (k = 3–5), but decreased for k = 5 class, again suggesting the five-class model was a poorer fit. BLRTs remained significant (p < .0001) with each successive class addition to the model, thus not clearly discriminating a model of best fit. LMR likelihood ratio tests were significant for k = 2–4 classes, suggesting that each successive addition of a class was a significant improvement to the fit of the model; the LMR test for k = 5 was nonsignificant. Taken together with relationship to the extant literature and model interpretability, it was determined the four-class model was the best fit to the data.
Correlations between the PANSS subscale, QLS, and MAS-A scores for the entire sample are found in Table 2. Descriptive statistics for each of the classes, including demographics, PANSS subscale, QLS scores, and MAS-A scores, are found in Table 3. Groups were classified as follows: diffuse symptoms/moderately impaired social function (Class 1), positive and hostility symptoms/mildly impaired social function (Class 2), minimal symptoms/good social functioning (Class 3), and negative and cognitive symptoms/severely impaired social functioning (Class 4). Groups did not differ by age. Class 4 had lower levels of education than other groups and Class 2 had a higher proportion of women.
Correlations among MAS-A, PANSS, and QLS subscales for full sample (N = 334).
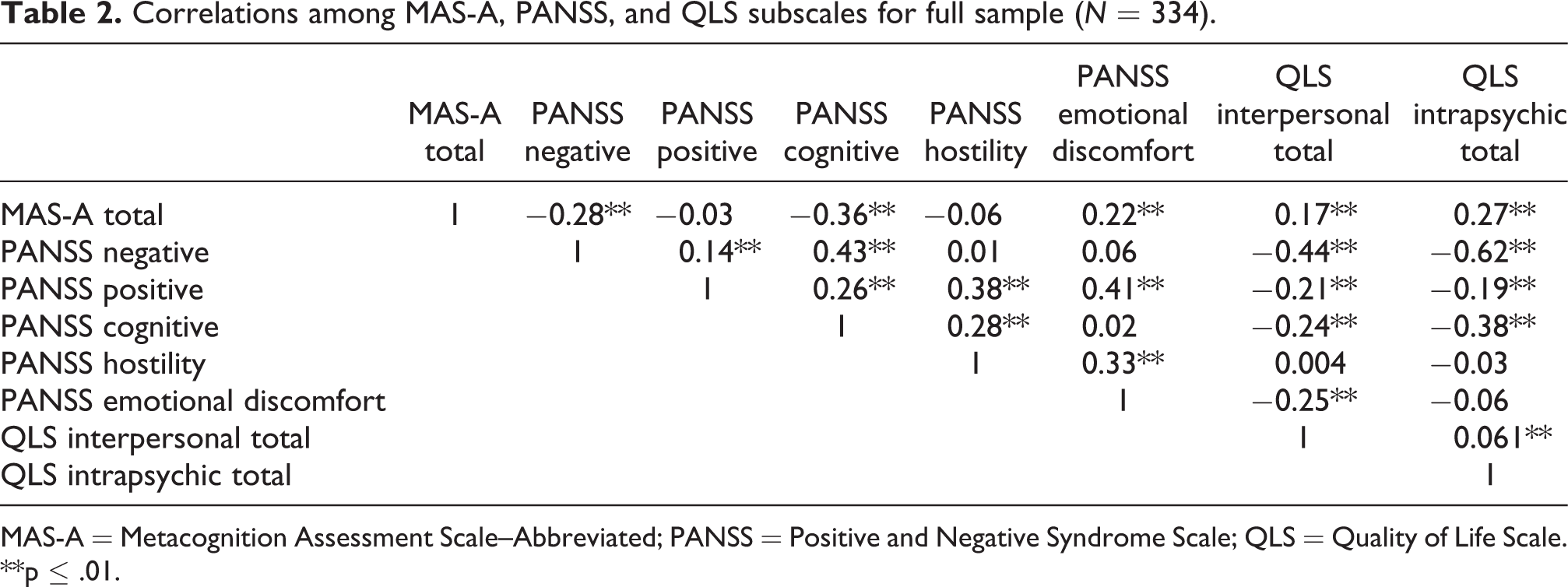
MAS-A = Metacognition Assessment Scale–Abbreviated; PANSS = Positive and Negative Syndrome Scale; QLS = Quality of Life Scale.
**p ≤ .01.
Latent class analysis based on symptom and functioning scores.

Note. Class 1 = diffuse symptoms/moderately impaired social functioning; Class 2 = positive and hostility symptoms/mildly impaired social functioning; Class 3 = minimal symptoms/good social functioning; Class 4 = negative and cognitive symptoms/severely impaired social functioning; LCA = latent class analysis; QLS = Quality of Life Scale; PANSS = Positive and Negative Syndrome Scale; MAS-A = Metacognition Assessment Scale–Abbreviated. Analyses were repeated for the MAS-A subscales and QLS interpersonal total controlling for gender and education; all group comparisons remained significant at the p ≤ .01 level.
*p ≤ .05; **p ≤ .01; ***p ≤ .001; +p = .057.
ANOVAs and post hoc analyses using the Bonferroni correction for multiple comparisons were performed to compare classes on MAS-A scores. Class 3 had better overall metacognitive functioning than both Classes 1 and 4. When comparisons were repeated at the subscale level, these differences appeared to be accounted for by the self-reflectivity and mastery subscales. Class 3 did not differ in terms of overall metacognitive capacity than Class 2. Given the significant gender and education differences between classes, we repeated these analyses controlling for both variables. All group differences on the MAS-A scores remained significant at the p < .01 level.
Finally, to further characterize the sample, classes were compared on the QLS interpersonal subscale using ANOVA and post hoc analyses using the Bonferroni correction for multiple comparisons. This analysis revealed that Classes 2 and 3 both demonstrated better interpersonal functioning than Classes 1 and 4.
Discussion
In this study, we empirically derived four classes of individuals with schizophrenia spectrum disorders on the basis of their social functioning and symptomatology, and we sought to determine whether deficits in metacognitive function were found in groups with poorer social functioning. As predicted, we found four groups: one with generally good social functioning and three groups with differing levels of impaired social functioning. As anticipated, the three groups had distinct symptom presentations: one with predominantly negative symptoms, one with predominantly positive symptoms, and one with diffuse levels of both positive and negative symptoms. Surprisingly, the group with negative symptoms also had pronounced cognitive symptoms, and the group with positive symptoms had concurrently higher levels of hostility symptoms.
When we compared metacognitive capacity across groups, our predictions were only partially confirmed: the groups with poorest social functioning, those with predominately negative/cognitive symptoms and those with diffuse symptoms, had lower levels of overall metacognition and greater impairment in domains of self-reflectivity and mastery than the group with good social functioning. Therefore, these findings are consistent with models of poor functioning dating back to Bleuler that suggested fragmentation of an individual’s experience may result in some form of social dysfunction.
While the cross-sectional nature of this study precludes drawing any causal conclusions, results may suggest several hypotheses for future research. For one, it is possible that relative inabilities to form a complex and integrated sense of self and use that information to respond to challenges results in the presence of fewer resources for social relationships. For example, it may be that the basic building blocks for intimacy are compromised when persons cannot synthesize discrete information into more complex ideas that could guide behavior. Examination of mean MAS-A scores suggests that the ability to understand one’s own mental and emotional states as changing and subjective is associated with greater levels of social functioning, while the tendency to address psychosocial challenges simply by gross avoidance (rather than changing one’s behaviors or thoughts) is associated with poorer social functioning. Of note, alternative hypotheses cannot be ruled out, including that with poorer social function, metacognitive capacity is degraded, or that the link between these variables is the result of the presence of other phenomenon such as attachment style (Gumley et al., 2014) or trauma history (Pec, Bob, & Lysaker, 2015). Future research should explore these possible relationships.
There were unexpected findings. The group with predominantly positive and hostility symptoms contained a higher proportion of women, and their metacognitive capacity did not differ from the group with good social function, though their metacognitive capacity was superior to the group with prominent negative symptoms. One possibility may be that positive symptoms (and perhaps hostility) may represent a path to social dysfunction that is qualitatively different than others linked with negative or diffuse symptoms and in which metacognitive deficits do not play a major contributory role. A potential speculation is that higher levels of arousal and positive symptoms may be related to traumatic experiences, which may uniquely impact social functioning (Bell, Robinson, Katona, Fett, & Shergill, in press). Additionally, affective symptoms are more commonly present in women with schizophrenia (Goldstein & Link, 1988). Women also generally demonstrate better social functioning than men in schizophrenia (Usall et al., 2002) and the course of illness is often more favorable in women as well (DeLisi, 2011). Men generally have poorer premorbid social adjustment and as such, greater social disability (e.g., Addington, van Mastrigt, & Addington, 2003). As with all unexpected findings, future research is needed before any weight is afforded to their interpretation.
There are limitations to the current study. Individuals in the study were currently enrolled in outpatient mental health treatment. As such, it is unclear whether individuals in the community not seeking or refusing treatment would demonstrate similar patterns of functioning. We also only included persons with schizophrenia spectrum disorders. It is consequently unknown if the relationships found here are specific to schizophrenia or whether they may also apply to other disorders where metacognitive deficits have been observed to be linked to social functioning, including Posttraumatic Stress Disorder (Davis et al., 2016; Leonhardt, Lysaker, Vohs, James, & Davis, 2018), affective disorders (Ladegaard, Lysaker, Larsen, & Videbach, 2014; Lysaker, Hamm, et al., 2018), substance abuse (Inchausti, Ortuño-Sierra, García-Poveda, & Ballesteros-Prados, 2017b), and borderline personality disorder (Lysaker et al., 2017). Assessment of social functioning was completed by a trained rater, and metacognition was assessed using a single paradigm. As such, future research with different and broader methodology is needed (e.g., self-report, observation). Additionally, there may be conceptual overlap between PANSS items (e.g., passive social withdrawal) and our measures of social functioning (e.g., QLS interpersonal functioning) that may have impacted the pattern of results. Research is also needed that examines other factors that may influence social functioning, including social cognition, trauma, stigma, and neurocognition, particularly in longitudinal designs. Finally, we did not assess medication dosage or adherence so it is unknown to what extent pharmacological treatment may have influenced results.
With replication, results may have clinical implications. Interventions that target metacognition may lead to the recovery of building blocks for healthy and sustained social functioning (Lysaker, Gagen, Moritz, & Schweitzer, 2018). Indeed, recovery from serious mental illness has been conceptualized as a social process (Schön, Denjoy, & Topor, 2009; Tew et al., 2012). If the framework that underlies an individual’s ability to connect with others is disrupted, this can in turn jeopardize attainment of recovery. As such, it is critical that emphasis be placed on these constructs in order to more fully support an individual’s recovery. Potential candidates for this type of intervention include metacognitive training (Moritz et al., 2014), which promotes reflection upon reasoning processes within the flow of life, and metacognitive reflection and insight therapy (Lysaker & Klion, 2017), which assists persons in forming and using more complex understandings of themselves and others. These findings, coupled with an analysis of a broad group of case reports (Hamm & Lysaker, 2018; Hillis, Bidlack, & Macobin, 2018; James, Leonhardt, & Buck, 2018; Leonhardt, Ratliff, & Vohs, 2018), suggest that it may be useful to include treatments such as these in larger batteries which flexibly respond to the recovery needs of patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.