
Abstract
Background/objective
We have been practising the Neuropsychological and Educational Approach to Remediation (NEAR) as cognitive remediation (CR) in a psychiatric hospital and have implemented it in combination with regular interviews based on Motivational Interviewing (MI) approximately 2 years after launching NEAR. In this study, we investigated whether combining MI with CR affected completion of the programme, cognitive functions, global functioning, and personal recovery of patients with schizophrenia by analysing medical records.
Methods
In this retrospective observational study, 14 participants were assigned to the NEAR group and 12 participants were assigned to the NEAR + MI group. Fifteen participants in the NEAR group (n = 6) and NEAR + MI group (n = 9) completed the programme. First, the difference in the completion rate between the groups was examined using the chi-squared test. Second, measures of cognitive functions, global functioning, and personal recovery pre-and post-intervention were examined using the Wilcoxon signed-rank tests for those in each group who completed the programme. Third, therapeutic responses for each group were compared using the Mann–Whitney U tests.
Results
There were no statistically significant differences in completion rates between the groups. In the NEAR group, verbal memory and overall cognition improved after the intervention. On the other hand, not only cognitive functions but also global functioning and personal recovery improved in the NEAR + MI group. Moreover, changes in global functioning and personal recovery were significantly higher in the NEAR + MI group.
Conclusion
Study findings indicated that combining MI with CR improves cognitive functions, global functioning, and personal recovery in patients with schizophrenia.
Keywords
Introduction
It has been shown that approximately 85% of people with schizophrenia have impaired cognitive functions such as attention, memory, and executive function (McCleery et al., 2014). Cognitive impairments in schizophrenia are 1.0–1.5 standard deviations lower than the average for healthy individuals (Heinrichs, 2004; Reichenberg, 2010). Although differences exist depending on the cognitive domains, it has been reported that these impairments persist for 10 or 20 years after the onset of illness (Flaaten et al., 2022; Keefe, 2014). Moreover, it is well-known that cognitive impairments in people with schizophrenia predict deteriorating social functioning in terms of daily activities, work skills, and interpersonal behaviour (Bowie et al., 2010). In addition, these impairments also been shown to make subsequent psychosocial treatments (e.g. social skills training, cognitive-behavioural therapy, and vocational training) less effective (Allott et al., 2013; Kurtz, 2011). Therefore, rehabilitation programmes targeting cognitive impairments in people with schizophrenia and cognitive remediation (CR) programmes have been developed. CR is a behavioural training-based intervention designed to improve cognitive processes, durability and generalisation in global functioning (Wykes & Spaulding, 2011). The effects of CR on cognitive functions have been reported in several meta-analyses (Cella et al., 2020; Vita et al., 2021; Wykes et al., 2011). Recently, the practice of CR by occupational therapists and its effects have been reported (Iwane et al., 2022; Tan & King, 2013).
Various CR programmes have been implemented worldwide (American Psychological Association, 2007). One such programme carried out in Japan is the Neuropsychological and Educational Approach to Remediation (NEAR) for people with mental illness (Medalia et al., 2009). The programme’s theoretical background includes psychiatry, neuropsychology, educational psychology, learning theory, and rehabilitation psychology. One of the features of the NEAR programme is that it includes both computer and language sessions. In the former, participants work on cognitive tasks using a computer prepared for each person, with the aim of improving individually focused cognitive functions. To prevent participants from playing the computer game indifferently, each session is structured to enhance motivation and learning through therapists’ instructional techniques. On the other hand, the language sessions are run with a group composed of clients who are participating in the computer sessions. The contents of the group session include sharing difficulties and effective strategies in computer sessions, discussing the possibility of generalisation to problem-solving in daily life, performing cognitive exercises that are not computer-based, and participating in skill training for problem-solving or planning in daily life. Therapists encourage clients to reflect on their own learning styles, identify their challenges, and develop strategies to overcome them. Through such interventions, therapists aim to improve their clients’ cognitive and general functioning while helping them achieve individual goals.
On the other hand, people with schizophrenia who receive CR, including the NEAR intervention, may drop out from the programme, which is a cause for concern. Although a recent meta-analysis reported that the dropout rate for CR was 16.58% and there was no difference with other interventions, analyses of the moderator effect showed that the dropout rate was higher in studies recruiting only outpatients or both outpatients and inpatients than in studies in only inpatient settings (Vita et al., 2022). In long-term programmes such as CR, interventions may not continue because of changes in outcomes, such as hospitalisation, discharge, or employment. It may become impossible to access the programme due to hospitalisation for acute relapse, discharge far from the institution, or major changes in daily activities such as full-time employment during the intervention period. In addition, even if they are able to access the programme after hospitalisation, discharge or minor changes in daily activities, such as part-time employment, may result in an increased burden, reducing motivation and leading to dropout. Indeed, the dropout rate was 42% in a randomised controlled trial that verified NEAR’s effect on inpatients and outpatients with schizophrenia (Redoblado-Hodge et al., 2010). In the NEAR programme, therapists approach the intrinsic motivations of clients to encourage their active engagement (Medalia et al., 2009). Another study showed that the greater the motivation for the programme, the greater the treatment effect of NEAR (Medalia & Richardson, 2005). Considering the effect of motivation on treatment efficacy, it may be necessary to consider interventions for participants who are likely to have low motivation levels so that they can benefit from the CR programme.
Motivational interviewing (MI) is an intervention that approaches human motivation, especially ambivalent thinking, during a change in unhealthy behaviour or the continuation of healthy behaviour. In MI, therapists guide communication via a style situated between following and directing according to the underlying principle of partnership, acceptance, compassion and evocation. Therapists utilize the fundamental processes of engaging, focusing, evoking, and planning, along with technical skills (i.e. open questions, affirmation, reflections, summarisation, and micro skills) (Miller & Rollnick, 2013). In a previous study of people with schizophrenia, MI-based adherence therapy improved symptoms, insight into illness/treatment, functioning, duration of re-hospitalisations, and medication adherence (Chien et al., 2016). Additionally, MI for drug and alcohol misuse in schizophrenia or psychosis showed beneficial changes in empowerment levels at 12 and 24 month follow-ups (Berry et al., 2014). From these findings about the effectiveness of MI on schizophrenic disorders, combining MI with CR may have a positive effect on the motivation of people with schizophrenia. A study reports greater motivation and adherence to CR programme in people who received MI before the initiation of the program (Fiszdon et al., 2016).
Since 2015, we have been practising NEAR as an occupational therapy programme for inpatients and outpatients at a psychiatric hospital. As with NEAR’s original principles, the programme is aimed not at only improving cognitive functions but also global functioning and the personal recovery of clients. In this context, personal recovery refers to the deeply personal and unique process undertaken by individuals to change their attitudes, values, feelings, goals, abilities, and roles in order to achieve a satisfactory, hopeful, and productive way, despite the possible limitations of their illness (Anthony, 1993). In 2017, the structure of the programme was changed to include regular interviews based on MI during NEAR’s intervention period. Upon reviewing previous research, no study has examined the effect of CR on personal recovery, and two recent meta-analyses are not focused on subjective outcomes (Cella et al., 2020; Vita et al., 2021). Moreover, no reports have indicated whether regular interviews based on MI conducted during CR programmes affected personal recovery in people with schizophrenia. Therefore, the aim of the present study was to investigate whether combining MI with CR affected completion of the CR programme, and promoted cognitive and global functioning as well as personal recovery of patients with schizophrenia. For this purpose, we analysed the medical records of participants in the CR programmes.
Methods
Research design
This study was a retrospective observational study using medical records.
Participants
Study participants were patients referred to the CR programme at the occupational therapy department, Hayashishita Hospital. Although individuals with various psychiatric disorders participated in the programme, this study targeted those who had been diagnosed with schizophrenic disorders (F20-29) according to the criteria of the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10; World Health Organization, 1992). The inclusion criteria were, in addition to a diagnosis of schizophrenia, aged below 65 years old and psychiatrist-referred participation in the programme; the exclusion criteria were complications involving other psychiatric disorders.
Ethical considerations
The research protocol was approved by the Ethics Committee of Hayashishita Hospital (No. 17A). At the start of the programme, we informed all participants that the assessed data could be used for future study, and obtained their written consent. We also explained that they could participate in the programme without the requested consent or withdraw consent at any time without experiencing any disadvantages. This study was conducted in accordance with the Declaration of Helsinki.
Intervention
Neuropsychological and educational approach to remediation
A group-based NEAR programme was initiated in September 2015 as an occupational therapy programme for inpatients and outpatients. It was conducted in the form of a rolling admission with up to eight clients. The clients participated in 90 min NEAR sessions three times per week for 6 months. The first half of each session focused on computer session, and the second half focused on language session. Each session was run by one or two occupational therapists. Programme participants had psychiatric disorders, such as schizophrenia, bipolar disorder, and depression. They had been referred by their doctors because cognitive dysfunction was predicted to interfere with their daily lives. After receiving a referral, pre-intervention assessments were implemented using various assessment scales and an interview about the subjective neuropsychological state and mental health problems, learning style, motivation for the intervention, and goal orientation. During the programme, irregular interviews were conducted when participants requested them or when therapists felt the need for discussions with clients. When participants completed the programme or dropped out, post-intervention assessments were conducted with the same scales used in pre-intervention assessment. Furthermore, an interview was conducted regarding the subjective neuropsychological state and mental health problems, impressions throughout participation in the programme, and the level of achievement of personal goals. However, most participants who dropped out could not receive an evaluation with the assessment scales, or they refused assessments.
Prior to the implementation of the programme, occupational therapists who ran each session as leaders attended a NEAR training workshop and were qualified as cognitive remediation specialists (CRS). The programme was implemented in accordance with the therapist’s guide for the NEAR programme (Medalia et al., 2009).
Neuropsychological and educational approach to remediation + Motivational interviewing
Approximately 2 years after launching NEAR, all occupational therapists who ran the programme received MI training. As some of the NEAR participants were unable to maintain their motivation during the intervention period, we considered incorporating MI into the CR programme. Moreover, it was difficult to continue visiting the hospital three times per week for 6 months, especially for outpatients and those who were discharged during the intervention period. Therefore, from June 2017, we conducted regular interviews based on MI every month during the intervention period. In the interview, therapists confirmed the clients’ motivation to participate and continue the programme and asked about generalisation in daily life situations. Especially when the motivation of participants was low, an ambivalent background, such as ‘this programme is necessary but troublesome’ was frequently reported. Therapists sympathised with participants’ negative feelings and tried to draw out the motivation in the person by affirming their recognition of the necessity of the programme and clarifying their intention to change or pursue a goal. However, when MI was not recommended (e.g., when the participants showed sufficient motivation), therapists simply listened to clients’ impressions about the programme and achievement of goals.
Some participants achieved their rehabilitation goals early in the 6-months intervention period in a previous programme. Since a previous study reported that a 15 week NEAR improved cognitive functions and global functioning (Redoblado-Hodge et al., 2010), participants who were confirmed to have achieved their goals (via regular interviews) after 4 months were regarded as having completed the programme.
In addition, all occupational therapists completed more than 40 hr of MI training before the introduction of regular interviews, and regular training has continued. Although we were unable to record all regular interview sessions as a practice check, interviews with participants who provided written consent were recorded and supervised. Specifically, to uphold the MI spirit and ensure fidelity, therapists received supervision from a third party with experience as an MI trainer by undergoing the Motivational Interviewing Treatment Integrity Coding (Moyers et al., 2014), which checks whether the interview contents were compliant with MI.
Descriptions of interventions for the NEAR and NEAR + MI groups.
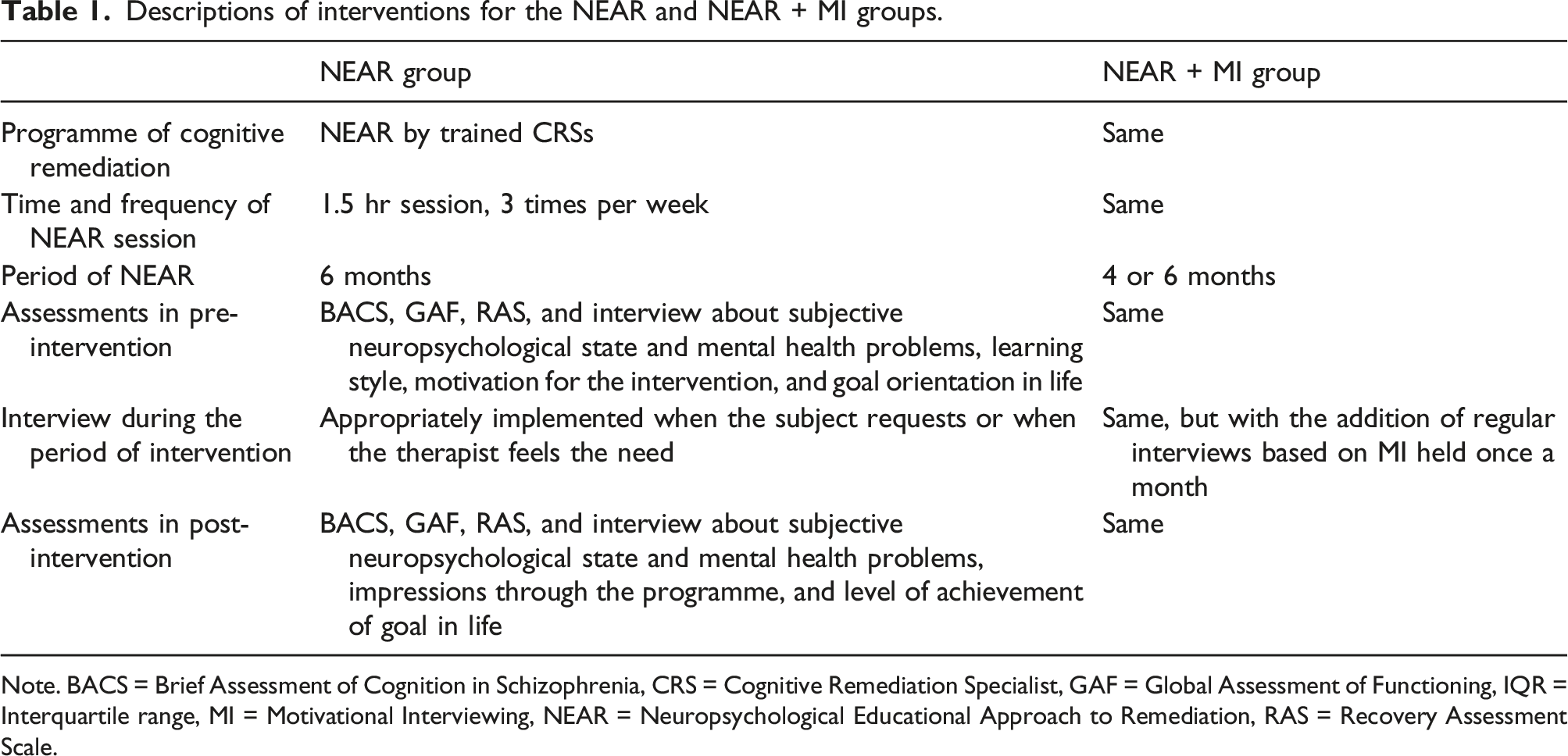
Note. BACS = Brief Assessment of Cognition in Schizophrenia, CRS = Cognitive Remediation Specialist, GAF = Global Assessment of Functioning, IQR = Interquartile range, MI = Motivational Interviewing, NEAR = Neuropsychological Educational Approach to Remediation, RAS = Recovery Assessment Scale.
Measures
In this programme, the following assessment scales were used for all participants before and after the intervention.
Cognitive functions
Trained occupational therapists assessed cognitive functions using the Japanese version of the Brief Assessment of Cognition in Schizophrenia (BACS: Kaneda et al., 2007). The BACS was originally designed to measure cognitive impairment in patients with schizophrenia and establish reliability and validity in the Japanese population (Kaneda et al., 2007; Keefe et al., 2004). This neuropsychological battery includes the following six tests: list learning (verbal memory), digit sequencing task (working memory), token motor task (motor speed), category and letter fluency task (verbal fluency), symbol coding (attention), and the Tower of London test (executive function). For each test, the z-score was calculated using standardised data (Kaneda et al., 2013).
Global functioning
The Global Assessment of Functioning (GAF: American Psychiatric Association, 2000) was used to assess participants’ global functioning. To enhance the reliability of the assessment, an evaluation of the GAF score was performed by an occupational therapist, and the evaluation was confirmed by another occupational therapist who observed the daily behaviours of the subjects.
Personal recovery
The Japanese version of the Recovery Assessment Scale (RAS: Chiba et al., 2010) was used to measure the personal recovery process. The RAS is a self-reported scale that was originally developed to assess the recovery process in people with mental illness and has been validated in Japan (Chiba et al., 2010; Corrigan et al., 2004). This scale contains 24 items with the following five-factor structures: goal/success orientation and hope, reliance on others, personal confidence, no domination by symptoms, and the willingness to ask for help. Participants rated the items using a five-point scale (1–5), and the mean score of each factor was used as an index of personal recovery (with higher scores indicating a higher orientation towards personal recovery).
Statistical analysis
Prior to performing the statistical analysis, we extracted data of patients who participated in the programme from September 2015 to December 2020 and met the inclusion criteria as study participants. Those who participated in the programme before May 2017 were assigned to the NEAR group and those who participated after June 2017 (when regular interviews based on MI began) were assigned to the NEAR + MI group.
First, demographic variables (i.e. age, sex, educational years, and estimated IQ), clinical data (i.e. outpatient/inpatient, diagnosis, duration of illness, total number of hospital stays, total length of hospital stays, GAF score, and antipsychotics dosage), and completed/dropout status were extracted from the medical records. Then, the differences in demographic variables, clinical data, and the programme completion rate of both groups were compared using the Mann-Whitney U test or chi-square test. Second, assessment scales (BACS, GAF, RAS) scores before and after intervention were extracted for participants who completed the programme. To verify the effect of each type of intervention, differences in scale scores before and after the intervention were examined using the Wilcoxon signed-rank tests for each group. Moreover, to compare the effect of the intervention, changes in these scores (post-intervention minus pre-intervention) in both groups were compared using the Mann-Whitney U tests.
All statistical analyses were performed using IBM SPSS Statistics for Windows (version 25.0; IBM Corp, Armonk, N.Y., USA) with the significance level set at 0.05. In addition, the effect size corresponding to the nonparametric test (Cramer’s V or r) was calculated.
Results
Of those recruited for participation in the programme from September 2015 to December 2020, 26 met the study’s inclusion criteria. Of these, 14 were in the NEAR group and 12 were in the NEAR + MI group.
Demographic and clinical data of all participants.
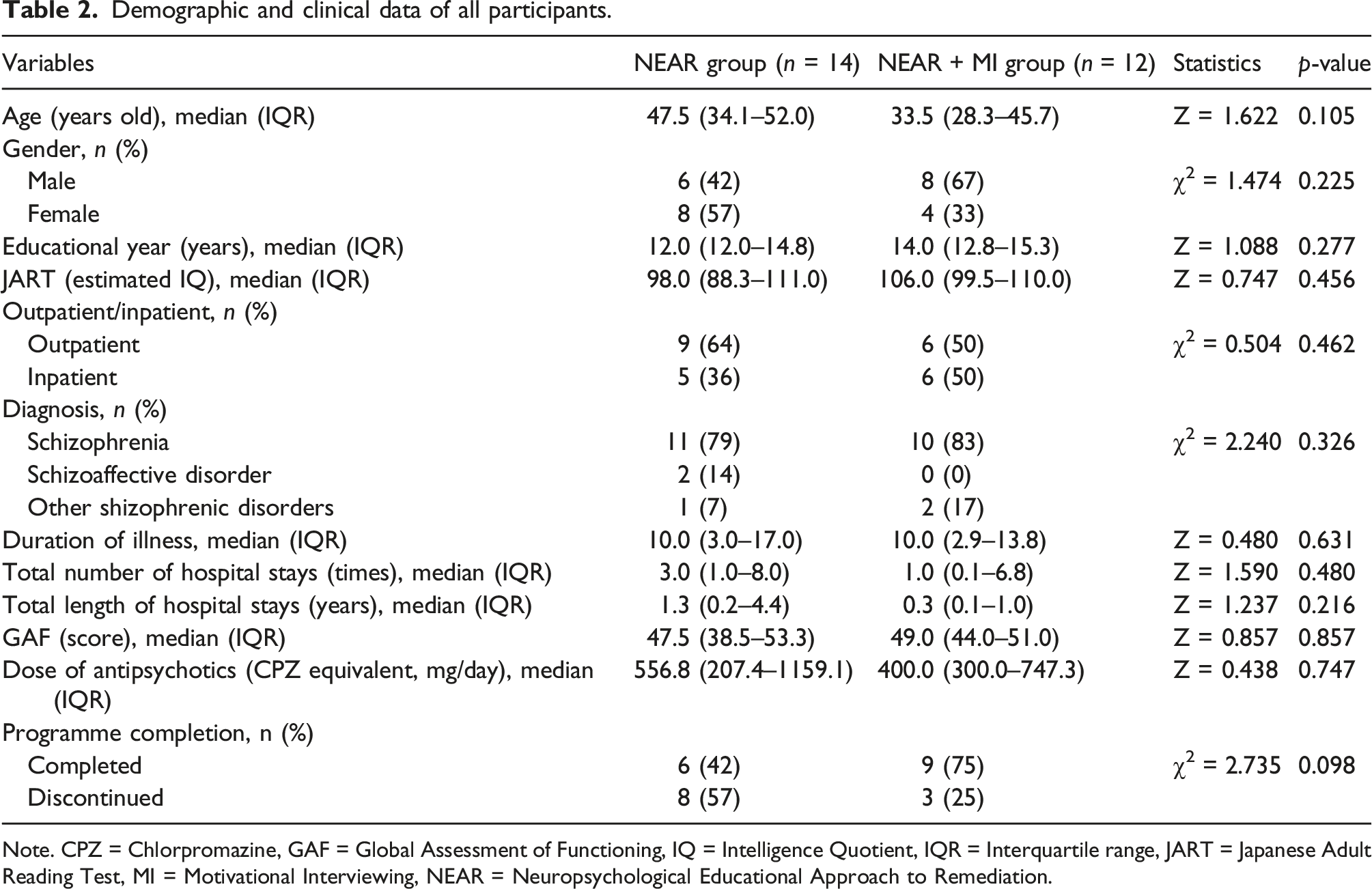
Note. CPZ = Chlorpromazine, GAF = Global Assessment of Functioning, IQ = Intelligence Quotient, IQR = Interquartile range, JART = Japanese Adult Reading Test, MI = Motivational Interviewing, NEAR = Neuropsychological Educational Approach to Remediation.
Comparison of the outcome scores between pre- and post-intervention in each group.
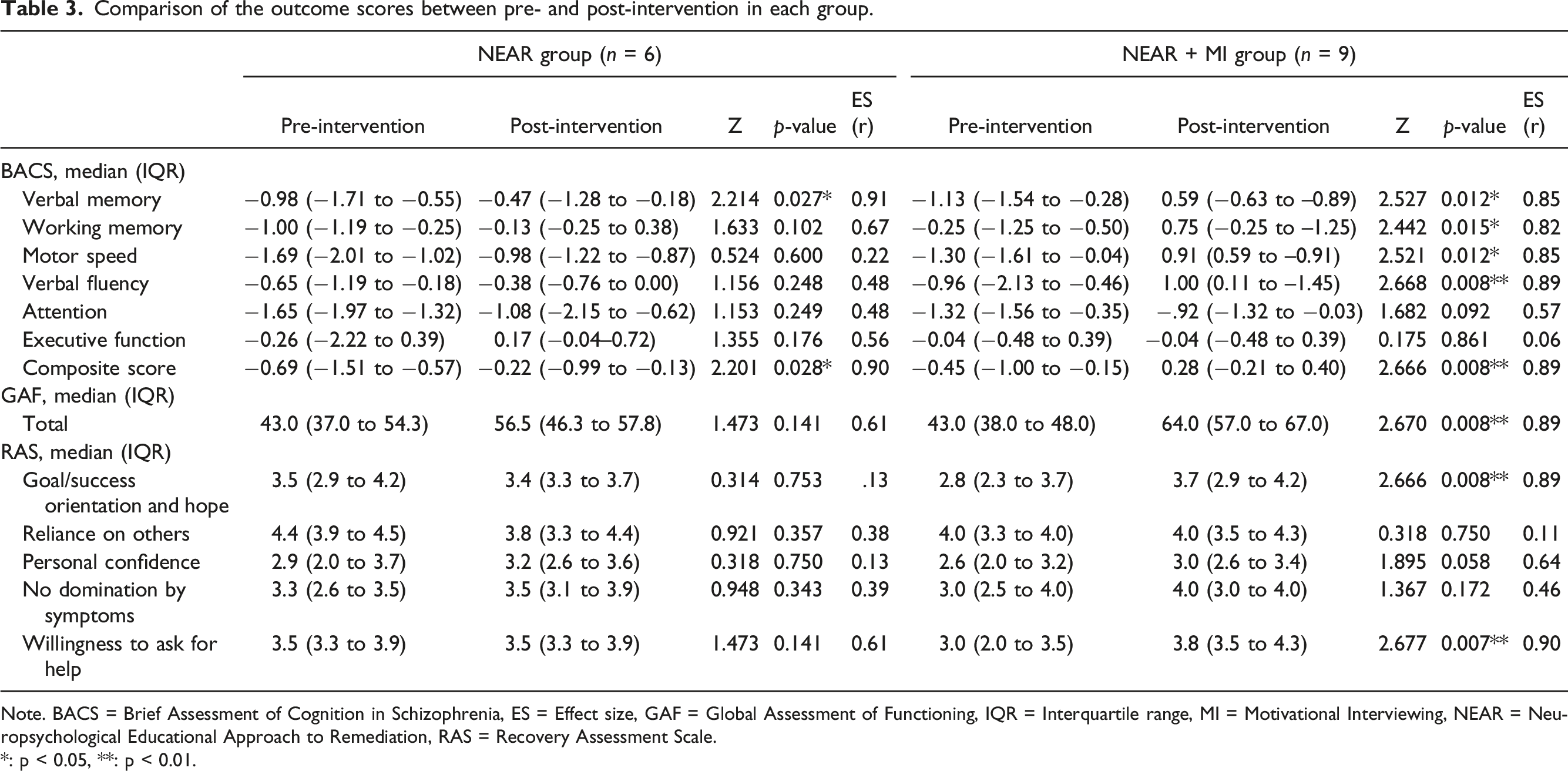
Note. BACS = Brief Assessment of Cognition in Schizophrenia, ES = Effect size, GAF = Global Assessment of Functioning, IQR = Interquartile range, MI = Motivational Interviewing, NEAR = Neuropsychological Educational Approach to Remediation, RAS = Recovery Assessment Scale.
*: p < 0.05, **: p < 0.01.
Comparison of changes in score on each scale pre- and post-intervention between groups.
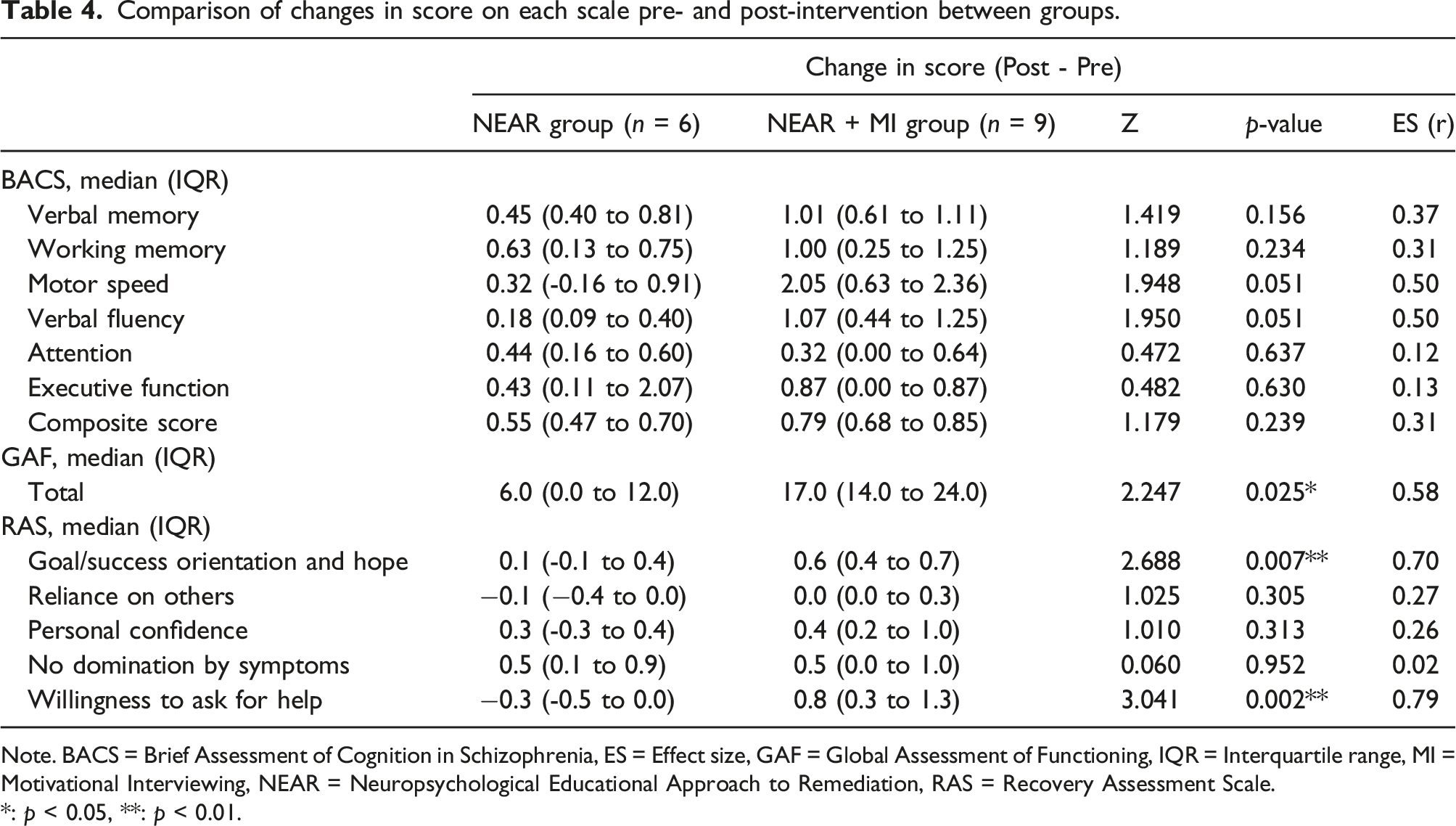
Note. BACS = Brief Assessment of Cognition in Schizophrenia, ES = Effect size, GAF = Global Assessment of Functioning, IQR = Interquartile range, MI = Motivational Interviewing, NEAR = Neuropsychological Educational Approach to Remediation, RAS = Recovery Assessment Scale.
*: p < 0.05, **: p < 0.01.
Discussion
In this study, although the implementation of the NEAR programme improved verbal memory and overall cognitive functions, adding regular interviews based on MI and making the intervention period flexible improved not only cognitive functions, but also global functioning and personal recovery. There was no statistically significant difference in the completion rate of the programme between the two forms; however, analyses of participants who completed the programme showed that global functioning and personal recovery improved more in those who received regular interviews based on MI than in those who did not.
Recent meta-analyses have shown that CR, such as the NEAR programme, is effective for improving cognitive functions in people with schizophrenia (Cella et al., 2020; Vita et al., 2021). In particular, it has been reported that the degree of improvement in verbal memory is higher than that in other cognitive domains (Vita et al., 2021). Findings of this study also revealed improvement in verbal memory for both groups. Moreover, improvements in multiple cognitive domains were observed when MI was added to the NEAR programme; further improvements in global functioning and personal recovery were also observed. Therapeutic alliance is one of the treatment response predictors of CR in people with schizophrenia (Barlati et al., 2019). It is possible that the therapeutic alliance was strengthened for participants who underwent regular interviews based on MI, leading to better cognitive outcomes and global functioning. However, regular interviews showed no improvement in attention and executive function. Since the effect size of attention in the NEAR + MI group was medium (0.57), smaller than other domains such as verbal memory, working memory, motor speed and verbal fluency, the insignificant result seems to be due to insufficient power. Regarding the reason for no improvement in executive function, it might due to the fact that ‘executive function’ scores at baseline were higher than the other BACS scores. It is also possible that participants might have been less motivated to improve their executive functions, which led to fewer problems in this domain than that of other cognitive domains. Furthermore, it is considered that opportunities of verbalisation by clients how the NEAR programme could be useful for them in regular interviews promoted goal orientation and hope and willingness to ask for help. In addition, therapists whose behaviours were consistent with those fostered in MI training showed empathy and faithfulness to the MI principles of partnership, acceptance, compassion, and evocation (Pace et al., 2017). Although therapists were involved in a collaborative manner in achievement of clients’ life goals, even during the regular NEAR session, the regular MI session increased opportunities to demonstrate willingness to cooperate in a formal interview format. This may have promoted the clients’ personal recovery process. However, among the elements of personal recovery considered, reliance on others, personal confidence, and no domination by symptoms did not improve through these interventions. In consideration of the high scores for reliance on others at pre-intervention, it might be difficult to significantly improve the state of having a certain degree of reliance. Although there was some improvement in personal confidence because its effect size was large (r = .64), it was also possible that some participants lost their confidence through facing difficulties in achieving goals as they became more goal-oriented. Regarding the no domination by symptoms, it is considered that the lack of effect was due to the fact that the main theme of CR did not address psychiatric symptoms.
On the other hand, although it was hypothesised that combining MI with NEAR would improve the programme completion rate, no statistically significant improvement was noted, possibly because of the small sample size. In fact, the completion rate improved by approximately 30% compared to that before adding MI; however, it is highly possible that it remained at the trend level owing to the small power. In addition, the dropout rate in the NEAR group (57%) was higher than that reported in a recent meta-analysis (16.58%: Vita et al., 2022) or previous randomised controlled trial (42%: Redoblado-Hodge et al., 2010). This meta-analysis (Vita et al., 2022) showed that studies that included both inpatients and outpatients, similar to our study, had higher dropout rates than studies that included only inpatients. In addition, our programme did not set stringent client selection criteria. Specifically, those who met the criteria recommended by the therapists’ guide for the NEAR (Medalia et al., 2009), such as those aged between 13 and 65 years, with a premorbid intelligence level estimated at above 70 and no active substance or alcohol dependency, were eligible, even if their symptoms or functional status were not stable. In fact, the median GAF score in this study was less than 50 in both groups, indicating that some participants had severe symptoms or functional impairments. In a recent review article (Barlati et al., 2019), baseline psychiatric symptoms, cognitive dysfunction, and functional impairments have been shown to be predictive factors influencing CR response. Perhaps patients with lower global functioning may have more difficulty perceiving treatment effects and are more likely to discontinue CR. As described above, this study did not examine the effects of the novel CR programme by limiting the participants, but, rather, verified the data from a practice of NEAR for a variety of clients in a clinical setting (e.g., those with lower and higher cognitive and global functioning levels). This may explain the high dropout rate.
In addition, as there are individual differences in the improvement of cognitive functions in people with schizophrenia (Medalia et al., 2019), it may be useful to flexibly change the intervention period according to individual characteristics and goals. Although the duration of the original NEAR intervention was 6 months (Medalia et al., 2001, 2003), a 15 week intervention has also been reported to improve cognitive and global functioning (Redoblado-Hodge et al., 2010). Furthermore, a study of first-episode outpatients reported that 10 weeks of intervention improved cognitive and global functioning (Lee et al., 2013). Although only 11.1% shortened the intervention period in this study, flexibility in its duration may be useful for improving the completion rate, even minimally.
A limitation of the present study is that it was a retrospective study with a small number of samples from a single institution. In particular, in this study, which utilised data from daily clinical practice, intentionally increasing the number of samples before combining MI with NEAR was not possible. Moreover, since the therapists had accumulated NEAR experience when MI was introduced, it is possible that they were able to implement the NEAR programme more effectively. Furthermore, the data of the individuals who discontinued participation (NEAR group: n = 8, 57.1%; NEAR + MI group: n = 3, 26.0%) could not be included in the comparison before and after the programme because almost all such individuals were not assessed by the scales post-intervention. Given that combining MI with NEAR was effective despite these limitations, conducting prospective and controlled studies based on the findings of the present study is recommended.
Conclusion
The present study showed that combining MI with CR and inserting flexibility into the intervention period according to the goal achievement status of participants may improve cognitive functions, global functioning, and personal recovery in patients with schizophrenia. In the clinical setting, if occupational therapists use MI when there is a concern about clients dropping out of the programme, clients may participate in the treatment more proactively, and as a result, receive more benefits from occupational therapy.
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.