
Abstract
Background/Objectives
People with schizophrenia have defective self-assessment of ability (i.e., loss of introspective accuracy [IA]). Although previous studies grouped people according to the degree of IA, the clinical features of these subgroups have not been clarified. Additionally, the determinants of outcomes depending on self-assessment remain unknown. We aimed to identify the clinical features that can help distinguish these subgroups and whether the determinants of vocational outcomes differed between the groups.
Methods
The self-assessment ability of 100 people with schizophrenia was examined and categorized as accurate, over-, or under-estimators. Multiple discriminant analysis was also performed. After demonstrating statistical validity, the relative effects of positive and negative symptoms, cognitive function, and level of IA on vocational outcomes were also examined for each subgroup.
Results
The symptoms that particularly explained the differences between these subgroups were positive and negative (expressing factors) symptoms: p < .001. Using the determinants of vocational outcomes in each subgroup, the over-estimator subgroup was characterized by positive symptoms: p = .025, the under-estimator group, by the underestimation of their own ability: p = .042, and the accurate estimator group, by cognitive function: p = .006.
Conclusion
Reduced IA can be a core mediator of various symptoms. Thus, tailoring the target and strategy of interventions for vocational outcomes according to the accuracy and quality of IA is important in clinical settings.
Keywords
Introduction
A common feature of people with schizophrenia is impaired insight, which is defined as a reduced ability to understand the reality of self or of a situation objectively (Medalia & Thysen, 2010). Perceptions of dysfunction reported by people with schizophrenia are consistently inaccurate, compared to the observations of contact clinicians and interviewers (Durand et al., 2015). The ability to evaluate one’s own cognitive ability is often referred to as “metacognition” and is recognized as an important cognitive ability (Koren et al., 2006). Over-estimating or underestimating one’s abilities indicates a decline in metacognitive function. A newly defined component of metacognition is one’s evaluation of the level of ability and performance. Such self-awareness is called “introspective accuracy” (IA). Poor IA can easily be indexed by the discrepancy between one’s own evaluation of one’s own abilities and outcomes and one’s actual performance/assessment of one’s ability by a contact informant (Silberstein & Harvey, 2019).
Patients with low cognitive function and severe negative symptoms across multiple neuropsychiatric conditions reportedly underestimate their disability (Bowie et al., 2007). Moreover, in the presence of mild depression, patients with schizophrenia overestimate their functions in daily living (Harvey, Deckle et al., 2019). Therefore, poor IA is among the major hallmarks of schizophrenia. Poor IA affects drug therapy compliance, suicidal tendencies, activities of daily living, and social and vocational outcomes; it also has a negative impact on morbidity and mortality (Holshausen et al., 2014; Kim, Ozzoude, et al., 2020).
Consequently, considering the impact of IA on clinical outcomes, studies have been published on intervention methods for people with schizophrenia based on IA features (Harris & Rempfer, 2020). According to a study by Harris and Rempfer (2020), the degree of introspective disability may be associated with the ability to learn new tasks quickly. However, previous studies have not addressed an important issue—is it possible to group individuals based on their IA?
Previous studies have divided individuals into three groups based on the characteristics of IA: those who overestimate their own ability (OE), those who accurately estimate their own ability (AE), and those who underestimate their own ability (UE) (Bowie et al., 2007; Harris & Rempfer, 2020). Moreover, these studies sought to capture the differences in symptom severity in each group. In general, if the IA deteriorates, other related symptoms tend to worsen (Bowie et al., 2007; Harris & Rempfer, 2020). However, few statistical studies have examined whether these three categories can be used to meaningfully divide schizophrenia patients based on their clinical characteristics and symptoms. Similarly, establishing a methodology for subgrouping can help clinicians personalize treatment strategies in busy clinical practices.
Further, it is unclear how schizophrenia relates to functional outcomes depending on the state of insight (i.e., IA). The decline in insight reportedly is the central hub of the symptom network in schizophrenia (Hasson-Ohayon et al., 2018); therefore, depending on the quality and ability of insight, the symptoms that affect functional outcomes may vary.
Schizophrenia is a debilitating mental disorder associated with disruption of work and academics (Andreasen & Flaum, 1991). Employment is an important aspect of finding a meaningful role in society and subsequently managing schizophrenia (McGurk et al., 2009). Interventions to assist with vocational outcomes are also one of the primary targets for psychiatric occupational therapy. Consequently, it is important to examine the determinants of vocational outcomes and to clarify whether these determinants differ depending on IA to facilitate appropriate employment-based interventions. To date, no studies have shown how different qualitative aspects of IA relate to other clinical symptoms and affect vocational outcomes.
Therefore, two analyses were conducted to clarify these two issues. In the first analysis, the clinical features of patients with schizophrenia were investigated and grouped according to self-estimates of IA and also whether these subgroups could be statistically categorized according to clinical symptoms. In particular, this study investigated which clinical features can be used to distinguish between these three groups. The variables used for discrimination were positive symptoms, negative symptoms (experience and expression), and cognitive function, which are generally considered to be determinants of the effects of schizophrenia (Harvey, Strassnig, et al., 2019). In the second analysis, the results obtained in the first analysis were used to examine the relationship between the IA subgroups and vocational outcomes (Gould et al., 2015; Wright et al., 2019). Thus, this study aimed to evaluate the determinants of vocational outcomes in each IA subgroup (AE, OE, and UE).
Methods
Participants
This study was approved by the institutional review board of the International University of Health and Welfare, and all participants provided written informed consent after a complete description of the study was provided. One hundred patients were recruited from outpatient treatment clinics at the Nasukougen Hospital in Japan to ensure a sufficient sample size, considering that five independent variables were investigated and that there were ≥25 people in each IA subgroup (Vietinghoff and McCulloch, 2007).
The selection was based on the presence of a diagnosis of schizophrenia or schizoaffective disorder as per the International Statistical Classification of Diseases and Related Health Problems–version 10 (WHO, 2016). The participants were excluded from the study if they had the following: substance use disorder; a history of neurological disorders, such as seizure disorder, stroke, head injury, brain surgery, mental retardation, or severe recurrent headaches; or were aged <20 years or >65 years.
All recruited patients had stable schizophrenia (i.e., the patients had not experienced any change in symptomatology during the past year). Antipsychotic drug prescription and dosage were left to the discretion of the treating physicians. Outpatient status was defined as living outside of any institutional setting, including nursing homes. This study occurred in the final phase of the Nasukougen Hospital Psychosocial Determinants Study (Okada et al., 2021). Therefore, we used the part of data set from the past study (Okada et al., 2021).
Subgrouping by IA (self-assessment of abilities)
The patients were divided according to their self-assessment of their own abilities. The accuracy of the evaluation was assessed by comparing the patients’ self-reported score of function with an informant-reported score, using traditional self-assessment techniques of functional status (Bowie et al., 2007) and recent studies (Kim, Jung, et al., 2020). The self-reported score was evaluated by using the Social Functioning Scale (SFS) (Birchwood et al., 1990), and the informant-reported score was evaluated using the Life Assessment Scale for Mental Illness (LASMI) (Iwasaki et al., 1994), which is frequently used in Japan.
The accuracy score, which captures the degree of discrepancy between self-reported cognition and neuropsychological performance, was calculated by evaluating the difference between the SFS and LASMI scores. First, the raw scores of the subjective (SFS) and objective (LASMI) scales were Z-transformed. By standardizing these scores, it was possible to place both subjective and objective variables on the same scale, making it easy to interpret the different scores. When the difference between these scores was 0, it indicated that there was no difference between subjective and objective cognition and function of the patient, representing perfect accuracy. A positive score reflected the patient’s overestimation of his/her own ability, while a negative score reflected underestimation. Consequently, the participants were divided into three groups based on their accuracy scores: AE, OE, and UE. These categories were based on the recommendations of previous studies on this topic (groups that were 0.75 standard deviations above or below the mean) (Bowie et al., 2007).
Measures
Positive symptom severity was assessed using a subset of the Brief Psychiatric Rating Scale (BPRS); it is based on factor analysis (Kopelowicz et al., 2008) and includes the following scale items: grandiosity, suspiciousness, hallucinations, unusual thought content, bizarre behavior, disorientation, and conceptual disorganization. Negative symptom severity was assessed using the Brief Negative Symptom Scale (BNSS). Cognitive function was measured using the Schizophrenia Cognition Rating Scale (SCoRS). All symptom assessments interpret higher scores as indicative of severe symptoms.
Brief psychiatric rating scale
The BPRS was created by Overall and Gorham to evaluate a wide range of mental symptoms. In this study, the BPRS was used to evaluate seven items related to positive symptoms. The 7 items were evaluated from 0 to 6 points. The score range was 0–42 points. The higher the score, the more severe the positive symptoms.
Brief negative symptom scale
The BNSS is based on the National Institute of Mental Health consensus statement to precisely detect negative symptoms. Previously, negative symptoms were difficult to distinguish from depressive symptoms and cognitive function, but BNSS is a new scale that solves this problem (Kirkpatrick et al., 2011). Negative symptoms were analyzed by dividing them into two factors based on recent studies (Kirkpatrick et al., 2011), namely, motivation (anhedonia, asociality, avolition: experience factor) and emotional expression (blunted affect, alogia: expression factor) (Kirkpatrick et al., 2011). Anhedonia is rated 0–21, Asociality 0–12, avolition 0–12, blunted affect 0–21, and alogia 0–12. The higher the score, the more severe the disorder of each negative symptom. The BNSS Japanese version total score and score of each subscale showed good convergent and discriminant validity (Hashimoto et al., 2019). The Japanese version of the BNSS translated by Hashimoto et al. (2019) was used.
Schizophrenia cognition rating scale
The SCoRS is a cognitive scale for schizophrenia, based on recommendations of the Measurement and Treatment Research to Improve Cognition of Schizophrenia project. It evaluates seven cognitive domains: vigilance, working memory, processing speed, language learning and memory, visual learning and memory, reasoning and problem solving, and social cognition. The score range is 20–80 points. The higher the score, the more severe the cognitive dysfunction. The Japanese version of the SCoRS translated by Kaneda et al. (2011) was used.
Social functioning scale
The SFS was used as a complete self-reporting measure to assess function. It has seven subitems: (1) withdrawal, (2) interpersonal relationships, (3) social participation, (4) recreation, (5) self-reliance and ability, (6) self-reliance and execution, and (7) employment. In the present study, the subitem of self-reliance and ability was excluded because it was evaluated as the possession of cognitive skills. The score range is 0–222 points. The higher the score, the less severe the outcome. We used the Japanese version of the SFS translated by Nemoto et al. (2008).
Life assessment scale for mental illness
The LASMI is an objective evaluation scale that is frequently used in Japan (Iwasaki et al., 1994). The LASMI does not rely on the subject’s self-evaluation. It measures a patient’s function in five categories of daily life: daily life, social life, vocation, stability, and self-recognition. The daily living outcome, social outcome, and vocation outcome were used to match the self-assessed items with the SFS items. 12 items are scored 0–48 points for daily living, 13 items are scored 0 to 52 points for social, and 10 items are scored 0 to 40 points for vocation. The higher the score, the more severe the disorder of each outcome.
Vocational/roles outcomes
Vocational roles/outcomes were assessed separately, and they did not depend on the SFS and LASMI to avoid bias. Therefore, with reference to the “Time-Use Survey” (Short, 2006) and previous studies using this method (Wright et al., 2019), the vocational role/outcome was assessed using the average weekly hours (×4 weeks = 1 month) of paid work, domestic activities, childcare, and educational activities. Moreover, the time spent at work was evaluated by the care manager in charge, and information regarding the domestic role, childcare, and educational activities at home was collected from the family and the care worker in charge. Finally, the averages daily time spent at work for 1 week was calculated.
Analysis method
Primary analysis: profiling of three subgroups
After dividing the patients into the three IA subgroups as described earlier, a one-way multivariate analysis of variance (ANOVA) was performed to examine the differences between the individual scales in each subgroup, and the Tukey test for multiple comparisons. Further, whether the symptom profiles of the three groups could explain the statistical differences and which type of symptoms could be an important variable for separating the three groups by multiple discriminant analysis were investigated. Multiple discriminant analysis was used to determine the degree of isolation based on the severity of a particular symptom among the subgroups.
Secondary analysis
Exploration of determinants of vocation/role outcome in each subgroup
After confirming using ANOVA that the basic attributes were the same for the subgroups that were statistically validated in the primary analysis, the BPRS, BNSS (experience and expression), and cognitive function associated with vocational outcomes were determined using correlation analysis and multiple regression analysis. In addition, IA was considered as the independent variable. IA was the Z-score of each subgroup’s score as described in earlier. Therefore, the proportions of the OE group and UE group were added as independent variables. For the AE group, the deviation from the Z-score of 0 was added to the independent variable.
Results
Analysis 1
Univariate analysis of variance (ANOVA).
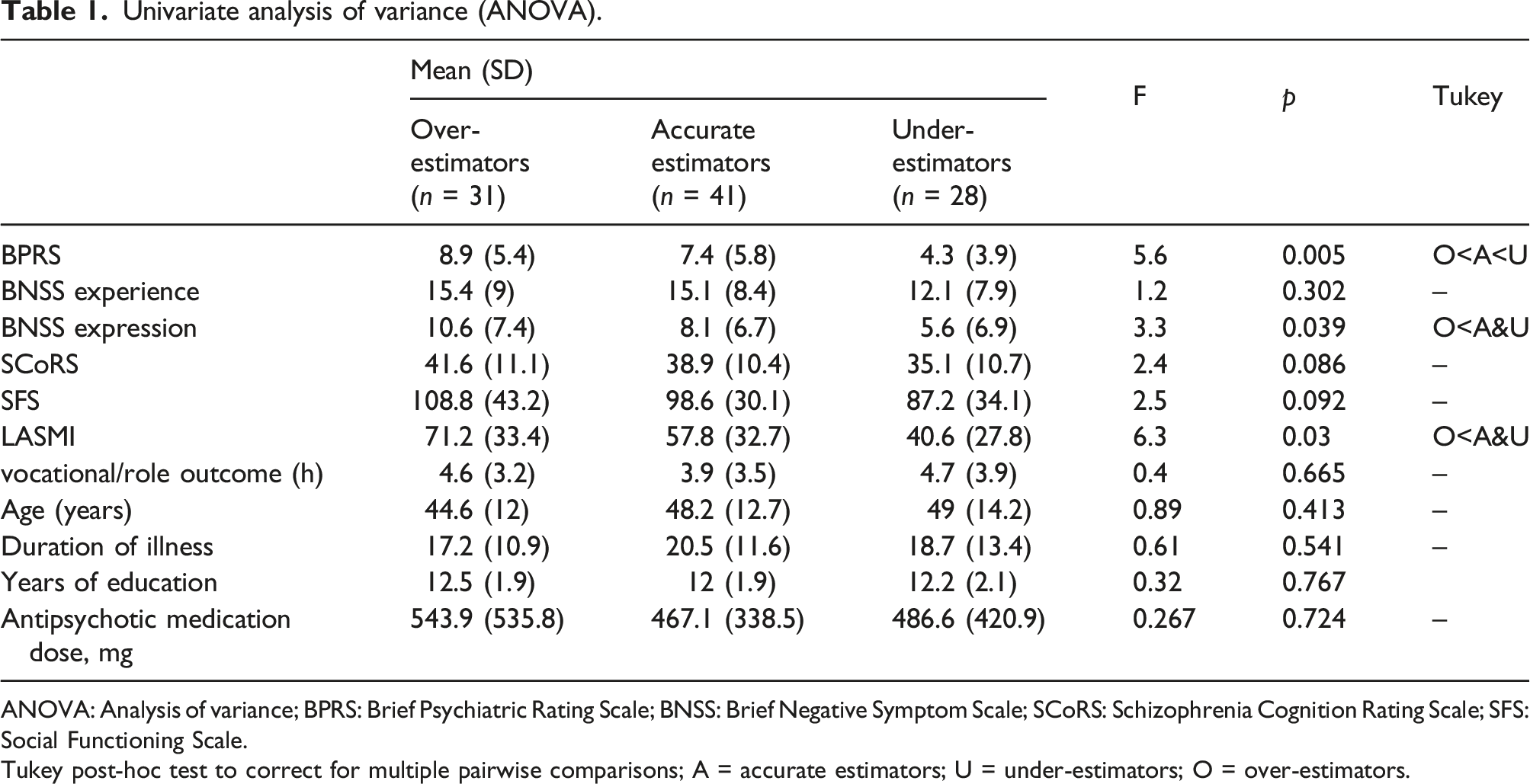
ANOVA: Analysis of variance; BPRS: Brief Psychiatric Rating Scale; BNSS: Brief Negative Symptom Scale; SCoRS: Schizophrenia Cognition Rating Scale; SFS: Social Functioning Scale.
Tukey post-hoc test to correct for multiple pairwise comparisons; A = accurate estimators; U = under-estimators; O = over-estimators.
Multiple discriminant score and standardization discrimination coefficient.
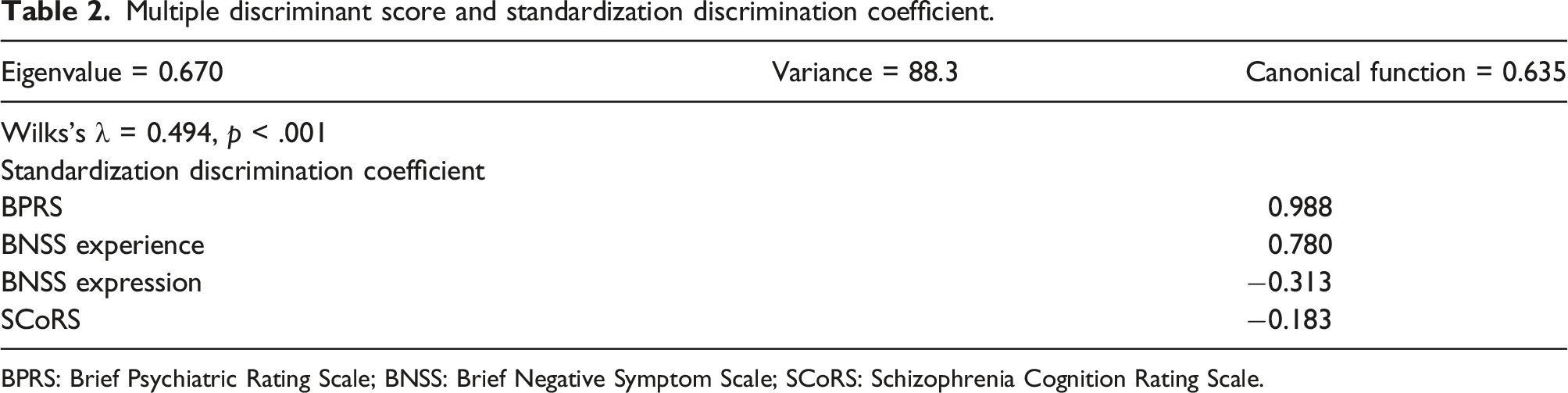
BPRS: Brief Psychiatric Rating Scale; BNSS: Brief Negative Symptom Scale; SCoRS: Schizophrenia Cognition Rating Scale.
Analysis 2
Correlations between vocational/role outcome and symptoms.
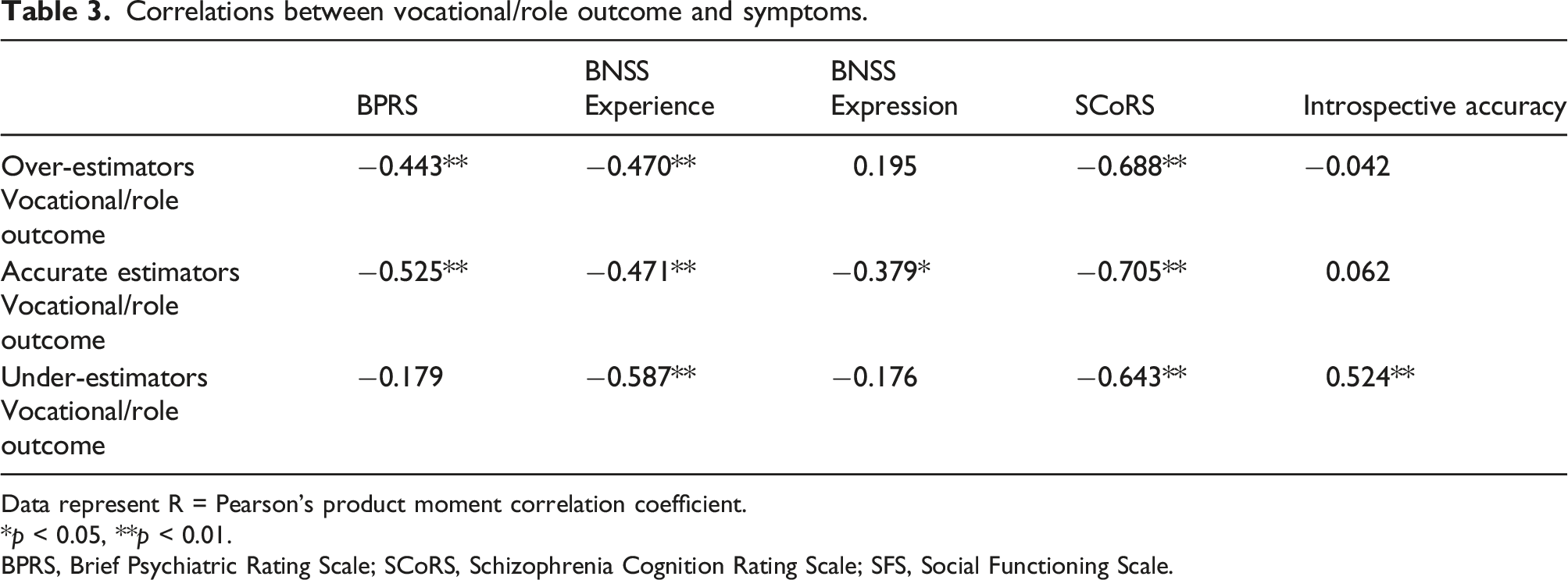
Data represent R = Pearson’s product moment correlation coefficient.
*p < 0.05, **p < 0.01.
BPRS, Brief Psychiatric Rating Scale; SCoRS, Schizophrenia Cognition Rating Scale; SFS, Social Functioning Scale.
Multiple regression analysis with vocational/role outcome as the dependent variable.
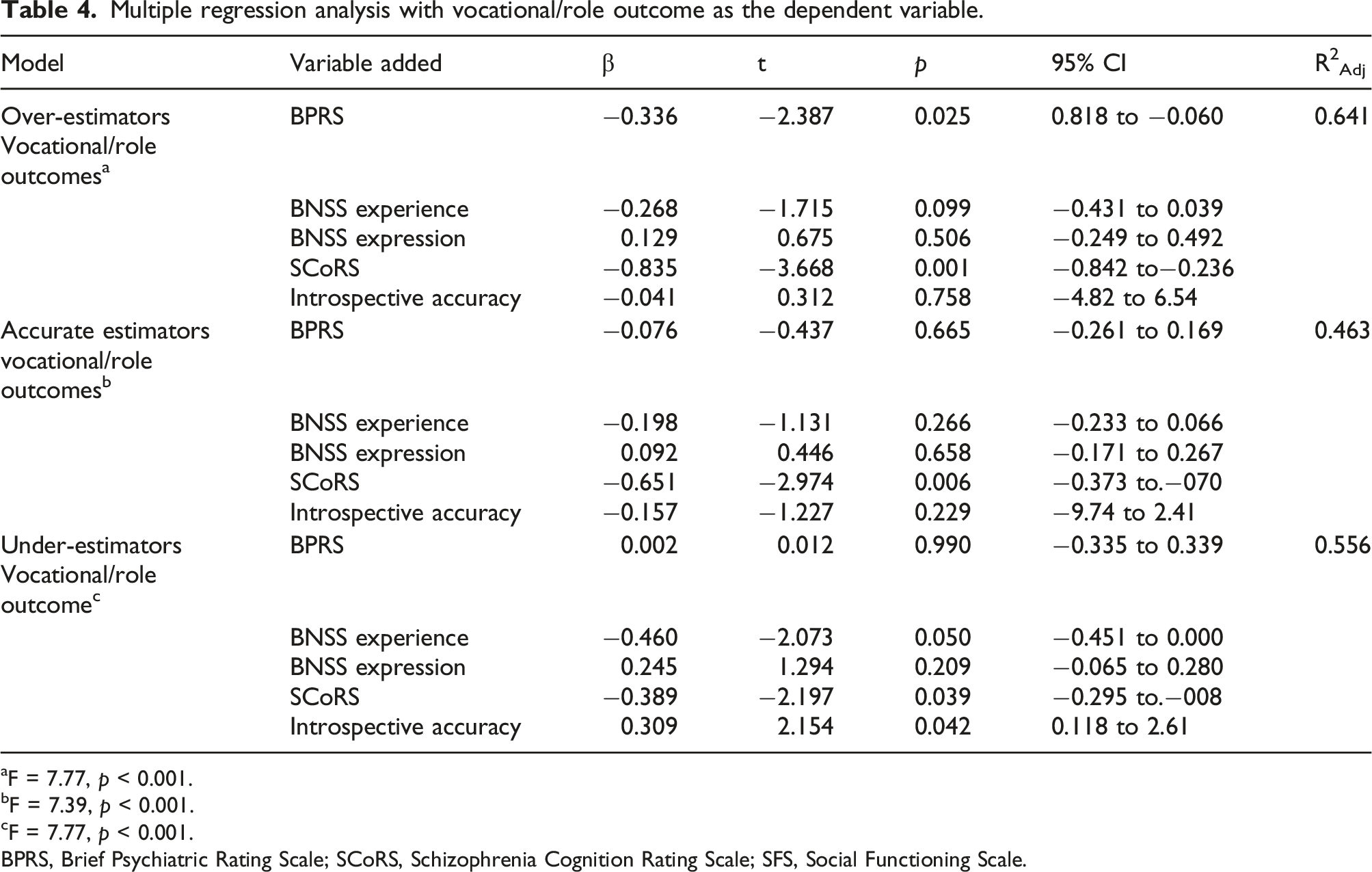
aF = 7.77, p < 0.001.
bF = 7.39, p < 0.001.
cF = 7.77, p < 0.001.
BPRS, Brief Psychiatric Rating Scale; SCoRS, Schizophrenia Cognition Rating Scale; SFS, Social Functioning Scale.
Discussion
This study examined whether IA subgroups could be significantly discriminated based on differences in positive and negative symptoms and cognitive function as well as the symptoms that could be useful for distinguishing between subgroups. Hence, the subgroups that were defined in previous studies (OE, AE, and UE subgroups) could be statistically discriminated using the symptoms characteristic of schizophrenia.
The most influential factor in the discrimination of the subgroups was positive symptoms. The OE subgroup had the highest positive symptoms. Positive symptoms reflect the discrepancy between the actual condition and the person’s perception (Garety et al., 2001). Overestimation of actual and self-perceived ability suggests that positive symptoms may worsen. The determinants of self-assessment by persons with schizophrenia are unknown; however, they may include neurological problems, and mood states may be a factor in combination (Orfei et al., 2017; Moritz et al., 2015). Additionally, increased self-confidence in patients with schizophrenia may be due to difficulty in self-monitoring. This is said to increase positive symptoms (Moritz et al., 2015). Considering the results of previous studies and the results of this study, positive symptoms could indicate subgroup differences. A particularly interesting finding was that after positive symptoms, negative symptoms best discriminated the subgroups. Among the negative symptoms, only motivational disorders (experience factors) not associated with impaired self-awareness of abilities (Harvey et al., Deckler, 2019) have been reported. Emotional factors are defined as linguistic and nonverbal losses of expressiveness. As shown in Table 1, it is predicted that the persons in the OE subgroup will have poor expressiveness.
Based on these results, the determinants of vocational outcomes for each subgroup were examined; they differed among subgroups. In terms of vocational outcomes, the OE subgroup was associated with positive symptoms and cognitive function, the AE subgroup was associated with cognitive function, and the UE subgroup was associated with cognitive function, the degree to which they underestimated their ability (IA), and motivational experience factors.
First, the OE subgroup showed poor cognitive function and positive symptoms. Cognitive function has a marked influence on vocational function (Cowman et al., 2021), which was expected. However, the association between positive symptoms and vocational outcomes remains unclear. For example, positive symptoms have previously been associated with vocational outcomes (Harrow et al., 2017; Luther et al., 2020); but, some studies showed that these factors were weakly related (Llerena et al. 2018; Galderisi et al., 2020). If positive symptoms are strong, the behavior is likely to be aggressive, which can deteriorate the relationships with colleagues (Lincoln and Hodgins, 2008). It has long been pointed out that aggressive behavior was more strongly associated with high scores for psychopathy traits and positive symptoms than with lack of insight (Lincoln and Hodgins, 2008). Therefore, positive symptoms affect work outcomes. Many of these previous studies did not classify people with schizophrenia according to their degree of self-awareness. The OE subgroup had unrealistic perceptions, which promotes positive symptoms and significantly impacts vocational outcomes.
For the UE subgroup, the degree of underestimating their abilities (IA), as well as cognitive function and motivational factors, affected the vocational outcomes. IA affected only the UE group; while in the OE group, the degree of overestimation of capacity was irrelevant. In the UE subgroup, the lower the self-evaluation, the worse the vocational outcomes. This is interesting given that the experiential symptomatology factors that reflect motivation are equally influential (Grant and Beck, 2010). Low IA can be associated with motivation and can worsen vocational outcomes (Grant and Beck, 2010).
Conversely, in the AE subgroup, cognitive function played a role in vocational outcomes, similar to that in the other groups (Harvey, Khan et al., 2107). Cognitive function is linked to potential work ability. Therefore, the participants in the AE subgroup may adjust the amount of work according to their abilities because they have an objective grasp of their abilities.
Therefore, these results suggest that interventions in occupational settings should use different strategies for each characteristic of the IA. Particularly, for those who underestimate themselves, training to regain objective IA such as cognitive behavioral therapy that facilitates objective self-awareness may be necessary as vocational support. Likewise, for those in the OE subgroup, interventions that reduce positive symptoms such as hallucinations and delusions and help them to manage themselves may improve vocational outcomes.
This study had some limitations. First, this study did not evaluate all the components of insight. The indicators used in this study reflect only awareness of one’s abilities (Moritz & Lysaker, 2018). Knowledge recognition is the basis of insight, but by using specialized methods of measuring insight or complex insights, the relevance thereof to vocational outcomes may become apparent. Additionally, in this study, the sample size of each subgroup was small because of stratification. This study was designed to prevent statistical errors in regression analysis, but studies with large sample sizes should be considered in the future.
In conclusion, this study showed the importance of considering metacognition in psychiatric occupational therapy and rehabilitation on schizophrenia. The three subgroups could be statistically discriminated by differences in the degree and quality of IA. Moreover, positive symptoms are most likely to explain the differences between these groups. Furthermore, by examining the determinants of vocational outcomes in each subgroup, vocational outcomes are affected by positive symptoms in the OE subgroup, by cognitive function in the AE subgroup, and by the degree of underestimation of one’s own ability and motivational deficit in the UE subgroup. These results strongly support the importance of changing the target and strategy of interventions in vocational support according to differences in the IA of people with schizophrenia.
Footnotes
Author contributions
The corresponding author collected, analyzed, and wrote the treatise.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The data used to support the findings of this study are restricted by the Institutional Review Board of the International University of Health and Welfare to protect patient privacy. Data are available from the corresponding author for researchers who meet the criteria for access to confidential data.