
Abstract
Metacognition refers to a spectrum of activities which spans from noticing discrete experiences to synthesizing them into a larger sense of the self and others. Evidence suggesting that deficits in metacognition are broadly present in schizophrenia and represent a potent barrier to recovery from schizophrenia has led to increasing interest in the development of metacognitively oriented treatments. In this article, we will describe the development of one such treatment, metacognitive reflection and insight therapy (MERIT), an integrative form of psychotherapy defined by eight core elements. We will first discuss the concept of metacognition as a means to operationalize the processes which enable persons to have a sense of themselves and others available for reflection and that can then serve as the basis for effective and agentic responses to psychosocial challenges. We will then discuss methods for assessing metacognition, the development of MERIT as a treatment that targets metacognition, and how MERIT compares with other treatments. Next, we will discuss empirical support for MERIT’s role in recovery including its potential to assist persons to develop their own personally meaningful sense of their challenges and then decide how to effectively respond to those challenges and manage their own recovery.
Keywords
Metacognition and recovery in schizophrenia
Metacognition is a core process supporting ongoing self-reflection, adaptation, and cooperation with others across the lifespan. The realization that metacognitive abilities or capacities differ between persons has offered the possibility to explain particular features of schizophrenia spectrum disorders, such as the unawareness of the illogicality of delusional beliefs (Moritz et al., 2014) or the failure to accurately appraise personal limitations (Silberstein, Pinkham, Penn, & Harvey, 2018). Difficulties with metacognitive function likely have even broader deleterious effects on wellness, as they impede persons’ ability to make sense of their own personal psychosocial challenges and then to decide how to manage those challenges and direct their own recovery (Lysaker, Hamm, Hasson-Ohayon, Pattison, & Leonhardt, 2018). This latter possibility has led to increasing interest in the development of recovery-oriented treatments that assist persons to recapture their metacognitive abilities and, therefore, more effectively manage their lives and achieve higher quality of life over time (Lysaker, Glynn, Wilkniss, & Silverstein, 2010).
In this article, we will describe the development of one such treatment, metacognitive reflection and insight therapy (MERIT) (Lysaker & Klion, 2017). We will first discuss the concept of metacognition and its relationship to self-experience and agency. We will then discuss methods for assessing metacognition and the development of MERIT and describe several ways in which MERIT converges with and diverges from other well-established treatments. Next, we will discuss empirical support for how MERIT may promote recovery. Finally, future directions for research and treatment development will be discussed.
The concept of metacognition
Metacognition has been a focus of study by many different areas of psychology over the last 30–40 years. It has been a key variable in research in education (Flavell, 1979), cognition (Bacon, Danion, Kauffmann-Muller, & Bruant, 2001), development (Kurtz & Borkowski, 1987), attachment (Main, 1991), and psychopathology (Dimaggio, Montano, Popolo, & Salvatore, 2015; Lysaker & Klion, 2017). It has been operationalized in many different ways and used for multiple purposes. Metacognition has been used to refer to self-regulated learning (Dinsmore, Alexander, & Loughlin, 2008), attitudes about beliefs (Wells, 2008), awareness of one’s own reasoning processes (Moritz et al., 2014), confidence in cognitive processes (Yeung & Summerfield, 2012), and the development of the shared awareness of oneself and others (Dimaggio et al., 2015; Semerari et al., 2003). Other efforts have sought to distinguish different kinds of metacognition from one another on the basis of the goal of their behaviors, for example, whether they involve planning, self-monitoring, and error detection and knowledge about strategies for responding to challenges (Tarricone, 2011).
In one effort to detangle the rapidly expanding work on metacognition, Moritz and Lysaker (2018) returned to one of the first definitions of metacognition by Flavell (1979). They noted that in Flavell’s paper, metacognition was offered as an umbrella term to describe what is at play when humans continuously think about themselves and their responses to what is transpiring as they act in the world. They also noted that even in the early definitions, metacognition was described as more than a purely cognitive phenomenon; metacognition appeared as a construct that could be readily linked to a long history of philosophical and psychological considerations of what is involved as persons are aware of and reflect upon subjective experience.
Piecing together these early definitions and later psychological research on health and interpersonal wellness, an integrated model of metacognition has been proposed in which metacognition is a spectrum of activities that mutually influence one another. These activities range from the awareness and reflection about specific singular immediate experiences to a larger more complex multifaceted sense of self and others (Lysaker, Zalzala, et al., 2018). In this sense, metacognition includes both noticing an isolated thought or bodily sensation (e.g., “I feel sad” or “I don’t trust a particular person”), as well as a larger sense of oneself (e.g., “I am having a hard time in my life now because of the death of a loved one”). Importantly, the larger sense of self is in part built from the smaller, singular atoms of experience and also serves as a basis for interpreting and integrating these atoms of experience.
Metacognition accordingly consists of processes which are primarily integrative in nature which bring together pre-reflective and reflective, embodied, and cognitive experience in response to what is emerging in the moment (Lysaker et al., 2018). While metacognition is a platform for reflection, it is both automatic and intersubjective, meaning metacognition usually arises naturally rather than effortfully and is tied to others who might hear or respond to the contents that emerge from it (Mascolo, 2016; Stern, 1985). Thus, metacognition is a key aspect of human adaption. It is a basis for agency as it is necessary for an enduring sense of our abilities to respond in a world of complex and changing contingencies (Lysaker & Klion, 2017). Metacognitive processes are also foundational for intimacy, as they allow us to have an immediate sense of ourselves in the moment which is fluid and responsive to the people around us or about to be around us in the moment. This is not to say that interpersonal relationships and first-person experience are not possible with lesser metacognitive capacities, but that with lesser metacognitive capacities the experience of self and others becomes more and more fragmented. For example, with lower levels of self-reflectivity, persons might be aware of individual thoughts but have no sense of how they relate to one another over time or to specific events within the larger environment.
Methods for the quantitative assessment of metacognition in schizophrenia: An iterative relationship between measurement and treatment
While the relationship between metacognition and health is intuitive, the measurement of metacognition poses several dilemmas. In particular, cognitive abilities are generally measured in terms of performance on tasks in which there are correct and incorrect responses. For example, memory can be quantified as the proportion of items correctly recalled or recognized and attention by the frequency of correctly identified targets. Emotion recognition is also often quantified in terms of correct and incorrect responses. However, since metacognition is foremost a process of integration, as it is concerned with how information is organized and fits together and not with the absolute correctness of any given judgment, it cannot be characterized by proportions of correct or incorrect responses. In response to this dilemma, the Metacognition Assessment Scale-Abbreviated (MAS-A) was developed in 2004 (Lysaker et al., 2005) to assess the complexity of the sense of self and others as it appears within spontaneous speech samples. The MAS-A was an advance from the MAS (Semerari et al., 2003) which assessed frequencies of metacognitive acts within a psychotherapy session. The MAS-A specifically quantifies the extent to which an integrated vs. fragmented sense of self and others is formed within a personal narrative of participants’ lives and psychosocial challenges. Following the original structure of the MAS, which allowed for separate assessments of self-reflectivity, awareness of others, awareness of one’s community (decentration), and use of their integrated unique sense of self and others to identify and respond to psychosocial challenges and distress (mastery), the MAS-A similarly generates four separate scores which reflect each of these domains. Within this rubric, mastery notably deviates conceptually from others, more purely cognitive definitions of metacognition as it pertains to action. Mastery, however, is understood as fundamentally metacognitive in nature as it represents enacted metacognitive processes which themselves then become a subject for reflection.
Concretely, raters read a transcript and for the scales which pertain to sense of self, others, and decentration determine the first level which participants failed to demonstrate adequate metacognitive capacity. The level below that or the last level in which participants were judged to have adequate metacognitive capacity is the score offered for that scale (e.g., if a participant was not judged to be able to perform the metacognitive activities described by level “5” of the Self-reflectivity scale but were judged to adequately perform levels “1” through “4,” a score of “4” would be offered). For the mastery subscale, each level is conceptualized as requiring a higher level of metacognitive capacity. For this scale, raters identify the maximal level of mastery performed by the participant and that is the score for the mastery subscale (e.g., if the participant was judged to be capable of level “6” of mastery but not levels “7” through “9” then a score of 6 is offered). The scale is freely available from the first author.
The quantification of distinct metacognitive capacities, such as thoughts of self, thoughts of others, decentration, and mastery, has made the development of a metacognitive treatment possible in four key ways. First, it provided a means for establishing the prevalence, character, and significance of metacognitive deficits in schizophrenia. For example, one study found that the MAS-A scores of 166 adults with prolonged schizophrenia were significantly lower than the MAS-A scores of a control group of 51 adults who experienced the significant social and nonpsychiatric medical adversity of HIV (Lysaker et al., 2014). Specifically, the schizophrenia group was found to have significant struggles to form coherent accounts of (i) changing emotions and subjective beliefs, (ii) the distinct emotions of others, (iii) the unique and independent needs of others, and (iv) ways to respond to psychosocial challenges beyond gross avoidance (Lysaker et al., 2014). Similar challenges to metacognitive function have also been found in samples with first episode psychosis as well (Trauelsen et al., 2016; Vohs et al., 2014). In parallel, greater levels of metacognitive deficits in schizophrenia have also been reported cross-culturally in comparison with groups with bipolar disorder (Lysaker, Irarrázaval, et al., 2018; Popolo et al., 2017; Tas, Brown, Aydemir, Brüne, & Lysaker, 2014), depression and anxiety disorders (WeiMing, Yi, Lysaker, & Kai, 2015), posttraumatic stress disorder (PTSD) (Lysaker, Dimaggio, et al., 2015), substance use (Inchausti, Ortuño-Sierra, García-Poveda, & Ballesteros-Prados, 2017), and borderline personality disorder (Lysaker et al., 2017) as well as others without any psychiatric condition (de Jong, van Donkersgoed, Renard, et al., 2017; Hasson-Ohayon et al., 2015). Deficits in metacognition among those with schizophrenia have also been found to potentially influence concurrent function (Bröcker et al., 2017; Buck et al., 2014; Kukla, Lysaker, & Salyers, 2013; Lysaker, McCormick, et al., 2011; Snethen, McCormick, & Lysaker, 2014) and prospective function (Luther et al., 2016; Lysaker, Kukla, et al., 2015; McLeod, Gumley, MacBeth, Schwannauer, & Lysaker, 2014), independent of general levels of psychopathology or neuropsychological function across the majority of these studies.
Second, as research with the MAS-A has detected and characterized how metacognitive deficits affect the experience of the self, others, one’s community, and oneself as an agent in the world, the scales of the MAS-A naturally offered more nuanced conceptualizations of targets for interventions. Accordingly, interventions can be tailored based on the specific deficits. Third, the scales not only described treatment targets, but also offered direction for interventions specific to different levels of metacognitive capacity. Intuitively, any intervention that might seek to target self-reflectivity would need to be sensitive to and not exceed patients’ maximal capacities in the moment. Using the MAS-A, a therapist can concretely assess a unique patient’s maximal capacity for self-reflectivity, awareness of the other, decentration, and mastery and offer interventions or reflections that call for patients to think about themselves or others at a level within, and not beyond, their capability (Lysaker, Buck, et al., 2011). For example, a patient unable to form a nuanced sense of his own emotions would struggle to benefit from a therapist asking him, “how do you feel?,” as this query would be beyond his present metacognitive ability. In essence, a patient with low self-reflectivity would be unable to form or express such a detailed understanding of his own emotion. Instead, the therapist might ask the patient merely to identify fragments of experience which could later be integrated into a larger sense of a nuanced affective state. Fourth, and finally, the MAS-A scales could also provide an opportunity for ongoing evaluation across sessions.
The development of the elements of MERIT
Using an iterative process, clinicians and researchers, including psychologists, nurse practitioners, and psychiatrists with humanistic existential, rehabilitative, psychoanalytic, and cognitive behavioral backgrounds, have used the research noted earlier as the basis for the design of a treatment that would address metacognitive deficits. An early decision was that this treatment would be in the form of a measurable set of therapist behaviors that should occur within a session. These behaviors were intended to reflect and go beyond the common factor by describing activities which should help patients to engage in metacognitive acts. Within and across sessions, the therapist is expected to provide interventions that match an individual patient’s unique metacognitive capacity and so, with time, promote increasingly greater levels of metacognitive capacity. It was also decided that this should be an integrative form of therapy, and thus, its elements should be ones that could be incorporated by humanistic, cognitive, and dynamic therapists without violating core assumptions of their approaches.
Later named MERIT by colleagues in the Netherlands (Lysaker & Klion, 2017), this treatment was conceptualized as recovery-oriented. MERIT also proposes that the patient herself is required to make sense of her challenges and determine how she might move toward and take charge of her own wellness. The therapy is integrative in the sense that it can be employed by therapists from different backgrounds without needing to adapt a different professional identity. It was believed that these qualities would allow for a holistic treatment that could be flexibly delivered by many different kinds of therapists and in response to patients with many different kinds of needs. In contrast to problem-, symptom-, or technique-focused treatments, MERIT sought to be an internally consistent treatment which could look very different from patient to patient, based on the needs of patients and their phase of recovery. MERIT thus intentionally avoids imposing a curriculum or set of predetermined activities which could hamper reflection and disrupt the development of understanding between patients and therapists.
Through the iterative process described earlier, an operational definition of MERIT was developed which consisted of the presence, within any given session, of sufficient levels of eight elements, which while defined independently, should synergistically influence the growth of metacognitive capacity (Lysaker & Klion, 2017). These elements were divided into three classes: content, process, and superordinate. The first class of elements was linked together by virtue of their focus on content. These elements call for explicit attention to the development of a joint understanding of patients’ agendas or what patients are wishing and seeking during or across sessions (element 1); patients’ experience of therapists’ thoughts and experiences within session (element 2); patients’ narratives or experience within the flow of their life rather than abstractions about experiences (element 3); and recognizable psychological challenges which are confronting the patient (element 4). As a whole, the first four content elements were conceptualized as allowing for a platform for continuous reflection in which patients could seek out and form a sense of their own complex and changing set of needs as unique beings within the flow of their lives and the painful struggles life has and is posing for them. Adequate therapist adherence was defined in terms of either multiple attempts to jointly think about these issues or patients successfully thinking about them on their own in the presence of the therapist (Lysaker & Klion, 2017).
The second class of elements was referred to as the process elements. These elements share a joint focus by therapist and patient on interpersonal and psychological processes within the session, which conceptually support the reflections occurring in the first four elements. The first of these process elements (element 5) requires reflection upon the therapeutic alliance or the qualities of the relationship in which the patient and therapist were jointly thinking about the patient agenda, patient’s reactions to the therapist, and patient narrative and struggles. The second of the process elements (element 6) requires explicit discussion of the effects of the session on the mind and body of the patient. For example, as a result of the session, are there different thoughts in the mind of the patient or different feelings in his or her body? The purpose of the process elements was less to “fix” any problems with the relationship or make sure progress was occurring, but instead to promote awareness and reflection about what was happening and why. Together, the process elements were intended to allow reflections about the larger environment which was supporting or hampering reflection. Adequate therapist adherence was defined in terms of either multiple attempts to think together about these processes or patients successfully thinking about them on their own (Lysaker & Klion, 2017).
The final class of elements was referred to as the superordinate elements. These elements offered principles based on the MAS-A for matching interventions to patients’ maximal metacognitive capacity in terms of reflections about the self and others (element 7) and mastery (element 8) or the use of metacognitive knowledge to actively and effectively respond to psychosocial challenges (Lysaker & Klion, 2017). As a whole, the superordinate elements were intended to ensure that reflections about content or process, as defined in the first six elements, were tailored to patients’ unique levels and, therefore, maximally stimulated metacognition while not posing thoughts that were too complex to be useful for patients. Here, the rubric provided by the MAS-A for the assessment of self-reflectivity, awareness of the other, and mastery is recommended as means for assessing patients metacognitive capacity in the moment and tailoring interventions which match that capacity. Adequate therapist adherence was defined in terms of therapists either correctly assessing patients’ metacognitive capacities and offering appropriate interventions across the course of the session or shifting their interventions following inaccurate assessments of patients’ metacognitive capacity (Lysaker & Klion, 2017).
Training in MERIT requires formal training in the basic elements, completion of exercises focused on mastering the intervention framework, followed by several months of consultation around practice with active psychotherapy cases. All of these are available from the MERIT institute (2018).
Overlap and divergence with supportive and manualized cognitive treatments
As noted earlier, MERIT was intended to be integrative in nature and thus something that could be incorporated within other approaches without violating their fundamental assumptions. Indeed, considered alongside supportive therapy and traditional and third-wave cognitive therapies applied to complex mental health conditions, MERIT shares several key commonalities. As summarized in Table 1, MERIT seeks to describe measurable therapist behavior related to content, as well as process, but includes additional requirements that those behaviors be adjusted according to dynamic and in-the-moment assessments of metacognitive capacity. MERIT, similar to supportive and cognitively oriented treatments, is also focused on beliefs and awareness of cognitive processes as well as the development of the therapeutic alliance. Like compassion focused therapies (Laithwaite et al., 2009), it is deeply concerned with how persons regard themselves and develop a sense of self direction. In contrast, MERIT includes a broader holistic examination of embodied and pre-reflective experiences and their relationship to cognition and the broader patterns of behavior across a lifespan which imbue life circumstance and challenges with their unique meanings. There is also explicit concern with joint reflection as an intersubjective process rather than an objective or subjective process.
Convergence and divergence of MERIT from manualized supportive and cognitive therapies.
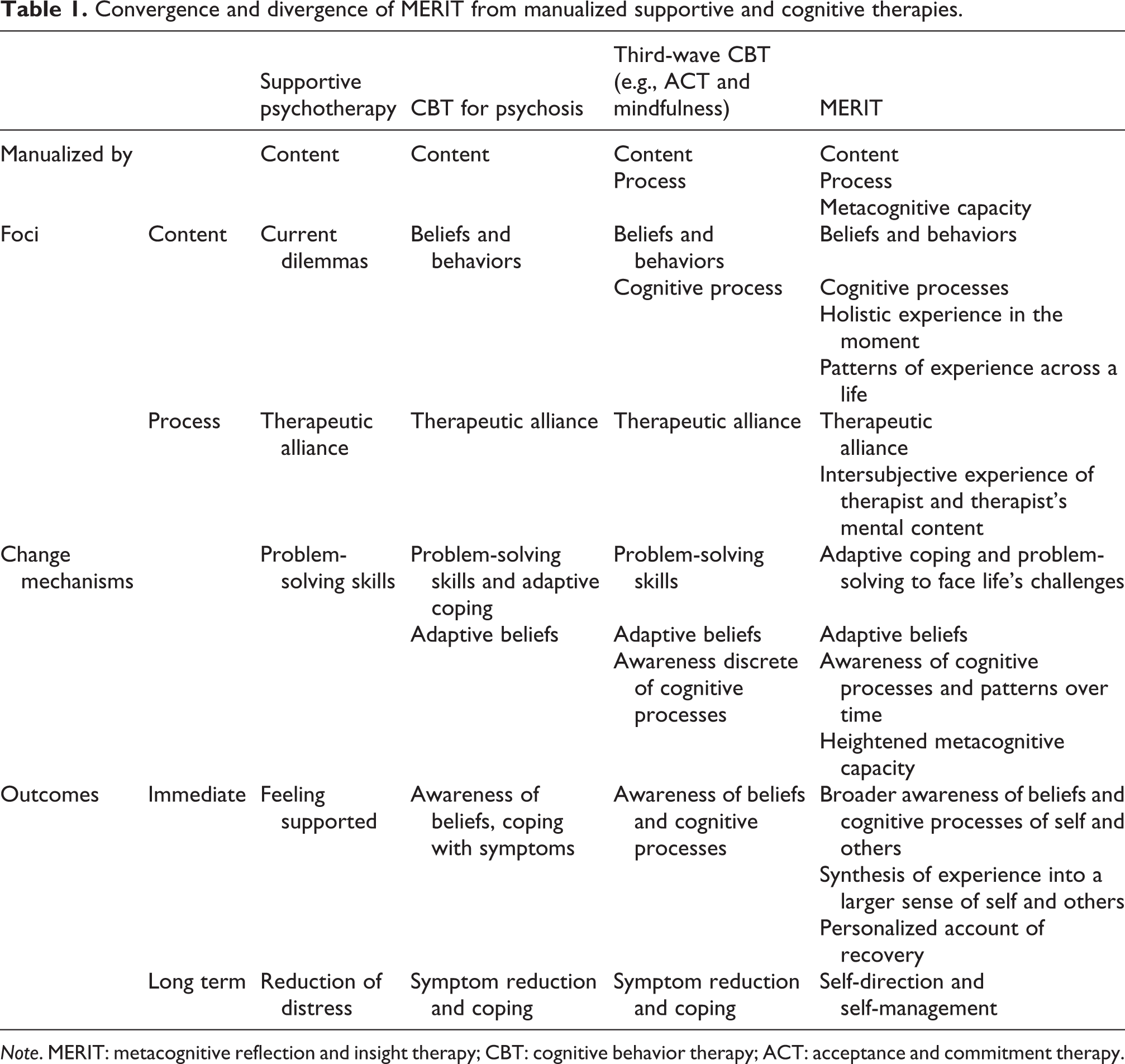
Note. MERIT: metacognitive reflection and insight therapy; CBT: cognitive behavior therapy; ACT: acceptance and commitment therapy.
Concerning mechanisms of action, MERIT is consistent with these treatments in several ways. MERIT focuses on helping patients think differently about themselves and others, as well as increasing awareness of basic cognitive processes. However, MERIT distinguishes itself regarding the aim to facilitate patients being able to form a more integrated sense of self and others and to use that information to adaptively face life’s challenges (Lysaker & Hasson-Ohayon, 2018). Thus, in MERIT, the cognitively oriented therapist needs to see that complexity of any new sense of, or increased awareness of, cognitive processes is as important as cognitive content. In addition, superordinate elements of MERIT indicate that treatment should be tailored to an individual’s measured level of metacognitive capacity; this would also require additional considerations from therapists who are most comfortable with many manualized cognitive behavioral therapy treatments which do not take metacognitive capacity into account. Finally, in terms of outcomes, MERIT can be seen to make demands on therapists that go beyond supportive and cognitive therapies in its explicit focus on the unique construction of a sense of psychosocial challenges and persons’ self-direction and self-management, rather than an emphasis on symptoms or more discrete constructs (e.g., coping skills).
Overlap and divergence with humanistic and dynamic treatments
Considering the integration of MERIT with humanistic and psychodynamic treatments, like most humanistic and psychodynamic treatments, MERIT rejects the prescription of predetermined exercises or therapeutic activities beyond merely relating to and conversing with patients in the moment. Also like these therapies, it is interested in holistic self-experience and patterns across the lifespan, as well as reflection as an intersubjective process. MERIT further shares a lack of concern with symptoms and an emphasis on meaning, focusing on the ability to form a more integrated sense of self and others in order to become better able to make sense of and respond to distress.
In contrast, MERIT may stretch the work of humanistic and psychodynamic therapists as it requires that the approach to the issues of meaning and experience be sensitive and titrated to patients’ metacognitive capacities (Lysaker, Zalzala, et al., 2018). MERIT requires a step beyond these treatments as usually practiced, in that it conceptualizes metacognitive deficits as limiting the degree of complexity with which a person can find meaning. MERIT imposes a rubric of assessment and intervention meant to help persons maximally make sense of what they face, but then also to promote growth in metacognitive capacity. There is nothing in MERIT that would be inconsistent with the possibility that wellness can proceed from self-actualization or coming to terms with emotional and psychological conflicts; however, in MERIT, it is the complexity of any new emergent sense of self and others that is again as important as the content of those new ideas of the self or others.
Evidence supporting MERIT
Given dropout rates in trials of dynamic psychotherapies for psychosis decades ago (Gunderson, 1980), any potentially long-term treatment has lived under the shadow of questions about its acceptability and feasibility. To date, two randomized controlled trials of 6 and 8 months of MERIT, respectively, have demonstrated that between two-third and three-fifth of patients randomized to receive MERIT completed treatment (de Jong, van Donkersgoed, Timmerman, et al., 2018; Vohs et al., 2018). Similar rates of treatment acceptance were also reported in an open trial of a metacognitively oriented psychotherapy that conformed to the elements of MERIT, lasting between 11 months and 26 months offered to 11 persons with schizophrenia (Bargenquast & Schweitzer, 2014) and in another open trial of a shorter 12-week course of MERIT offered to 12 adults with schizophrenia (de Jong, van Donkersgoed, Pijnenborg, & Lysaker, 2016).
Beyond controlled trials, case studies conducted under routine clinical conditions have also reported that a broad range of patients with very different clinical presentations, as well as profiles of strengths and needs, including heightened levels of negative symptoms, comorbid substance misuse, cognitive disorganization, depression, and lack of insight can benefit from MERIT (Arnon-Ribenfeld, Bloom, et al., 2017; de Jong, van Donkersgoed, Aleman, et al., 2016; Dubreucq, Delorme, & Roure, 2016; Hamm & Firmin, 2016; Hasson-Ohayon, Kravetz, & Lysaker, 2017; James, Leonhardt, & Buck, in press; Leonhardt et al., 2016; Leonhardt, Ratliff, & Buck, 2018; Van Donkersgoed, De Jong, & Pijnenborg, 2016). In contrast to other more supportive therapy experiences, patients who received MERIT, whether via routine care (Lysaker, Kukla, et al., 2015) or within a clinical trial (de Jong et al., 2017), reported the development of a sense of personal agency, connections with one’s own unique history, and a greater capacity to tolerate and manage painful affects and emotion.
Concerning treatment outcomes, the case work reported earlier indicates that patients receiving MERIT can develop and meaningfully attain individualized recovery-oriented goals as they make sense of their psychosocial challenges and then decide how they want to respond to and manage those challenges across different phases of recovery (Hamm & Firmin, 2016; Hasson-Ohayon et al., 2017; Hillis et al., 2015; James et al., in press; Leonhardt et al., 2016; Leonhardt et al., 2018; Van Donkersgoed et al., 2016). This case work has also reported evidence of significant improvements in metacognition across treatment, as assessed with the MAS-A (Arnon-Ribenfeld, Hasson-Ohayon, Lavidor, Atzil-Slonim, & Lysaker, 2017; Hamm & Firmin, 2016; Hasson-Ohayon et al., 2017; Hillis, Bidlack, & Macobin, In Press; Hillis et al., 2015; James et al., in press; Leonhardt et al., 2016; Leonhardt et al., 2018; Lysaker, Buck, & Ringer, 2007; Van Donkersgoed et al., 2016). To date, one study has also suggested that the clinical, psychosocial, and metacognitive gains in MERIT persist for follow-up periods of several years (Schweitzer, Greben, & Bargenquast, 2017).
Summary and future directions
Metacognition refers to a range of processes which enable human beings to have a sense of themselves and others which is available to them within the flow of life. With mounting evidence that deficits in these processes are common in schizophrenia and are a barrier to persons defining and managing their own path to recovery, interest has arisen in developing forms of psychotherapy that might enhance metacognition.
In this article, we have reviewed the development and early exploration of one such therapy, MERIT. This therapy seeks to stimulate metacognition at optimal levels in light of individual patients’ metacognitive capacity in a given moment, leading to the eventual development of greater metacognitive capacities. These enhanced metacognitive capacities are presumed to allow patients to develop their own coherent and personally meaningful accounts of the challenges they face and how they want to respond to them to move toward recovery. Preliminary evidence supports its acceptability and potential to lead to meaningful clinical change among unique patients with no formal or anecdotal reports of adverse side effects.
Importantly, there are limitations. Larger randomized controlled trials are needed in more diverse settings with wider ranges of patients. For example, while case work suggests MERIT may be applied to address the needs of adults with borderline personality disorder (Buck, Vertinski, & Kukla, 2018; Vohs & Leonhardt, 2016), rigorous trials are needed in persons diagnosed with these and other forms of significantly disabling mental illness. Some metacognitive deficits may be secondary to cognitive deficits and it is unclear whether there is a basic level of neurocognitive functioning required for MERIT to be acceptable and potentially helpful to patients with more profound limitations forms of cognitive impairment. Additionally, the general psychometric properties of the MAS-A have not been reported in general clinical settings though several studies are currently underway exploring this issue.
Work is also needed to explore a range of more nuanced issues related to the practice of MERIT. First, more work is needed to examine the integrative nature of MERIT and its utilization by therapists from different perspectives. For example, it is unknown in what ways MERIT offered by a cognitive behavioral therapist would differ from the therapy of a humanistic or psychodynamic psychotherapist. A second issue concerns the need to develop more explicit models which describe how and when effortful and automatic processes and cognitive and embodied experiences come together to form a sense of self or the other. Self-experience is necessarily a reflection of the interaction of multiple facets (Lysaker & Lysaker, 2008). More research is needed to explore the ways in which MERIT may promote this with a consideration of what kinds of different needs different kinds of patients have. Furthermore, once one has a sense of self available as a result of this, research is needed to examine what enables or blocks its flexible evolution and emergence over time. For example, what are the pathways by which persons gain a more robust and stable sense of themselves that can withstand contradiction and conflict and meaningfully respond to the complex realities present in all of our biological, social, and political environments? Regarding other forms of symptoms, including distress and positive symptoms, it is assumed that with the emergence of meaning persons become better able to tolerate pain and are less likely to rely on idiosyncratic explanations of distress and challenge but this remains to be formally tested in clinical settings. Research is currently underway examining whether metacognition is in fact a moderator of the link between distress and positive symptoms.
Finally, while we have focused on outcome in terms of patients’ recovery, it is also relevant how this therapy affects therapists and contributes to or complicates their long-term practice. This may not be a therapy for all therapists. For some, responding to the meanings being formed in disorganized discourse may be threatening and overwhelming. It may require that therapists are able to think in the moment, accept their own confusion and vulnerability, and to use their creativity to understand the profound suffering of the patient. However, for many therapists, this process unlocks creativity and may help to prevent career burnout. In research, we are now analyzing and exploring how MERIT may play a role in the professional well-being of psychotherapists, acting as another means to promote better patient outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article