
Abstract
Negative symptoms can be linked to Bleuler’s concept of splitting or fragmentation of thought, affect, and will. Research has shown a link between disturbances in metacognition and negative symptoms, although relatively few studies have examined this relationship longitudinally. The aim of this article is to examine whether metacognitive capacity among patients with first episode psychosis (FEP) predicted negative symptoms after a follow-up period of 3 years. Metacognition was assessed using the Metacognition Assessment Scale abbreviated and symptoms were assessed using Positive and Negative Syndrome Scale among 59 adults with FEP. Symptoms were then reassessed at a 3-year follow-up. Significant correlations were found between baseline metacognitive scores and the expressive component of negative symptoms as well as for individual negative symptoms such as blunted affect, poor rapport, and alogia at 3-year follow-up after controlling for baseline negative symptoms. Self-reflectivity was significantly correlated with the expressive component of negative symptoms at 3-year follow-up. The results are partly consistent with a Bleulerian model which understands the emergence of negative symptoms as a response in part to the experience of fragmentation, particularly in terms of sense of self and others. Future research should clarify the likely role of metacognition in the development and maintenance of negative symptoms.
Introduction
Beginning with the earliest definitions of schizophrenia, disturbances in mental functions known as negative symptoms have been identified as a core source of disability. In case after case, explicitly described the collapse of adaptive function, as a function of the loss of volition and affect. These losses themselves were understood as a kind of progressive dementia which was the direct result of organic processes which at that time were believed to be metabolic in nature. While he believed schizophrenia was the expression of biological as opposed to psychogenic process, offered a different view of the loss of volition and emotional expression which he also saw as a source of disability (Bleuler, n.d.). He suggested that negative symptoms were the result of the fragmentation or splitting of thought, emotion, and volition. As a result of what he called the three primary disturbances of the schizophrenias: alterations in association, affect, and ambivalence, Bleuler (1911/1952) suggested that the meanings that support goal directed behaviors vanished, resulting in a collapse of sense of agency and sense of self (Maatz, Hoff, & Angst, 2015; Noll, 2011).
Contemporary research has continued to document the importance of negative symptoms, including both expressive and experiential symptoms among persons experiencing all phases of schizophrenia (Harvey, Khan, & Keefe, 2017; Lyne et al., 2012; Strauss et al., 2013). Negative symptoms have been associated, for example, with a range of poorer outcomes in psychosis such as lower quality of life (Ho, Nopoulos, Flaum, Arndt, & Andreasen, 1998), poorer social functioning (Hunter & Barry, 2012), and graver challenges attaining meaningful recovery (Austin et al., 2013; Milev, Ho, Arndt, & Andreasen, 2005). Negative symptoms have furthermore come to be regarded as a key area of research as they are generally unresponsive to pharmacological treatment (Erhart, Marder, & Carpenter, 2006).
While research into the neurobiology of negative symptoms continues (Takahashi et al., 2017), it remains unclear whether negative symptoms are best understood themselves as primary facts unto themselves, suggested by constructs such as the deficit syndrome (Ahmed, Strauss, Buchanan, Kirkpatrick, & Carpenter, 2018) or as experience which is a response to the kinds of fragmentation originally described by Bleuler. This issue has far-reaching clinical significance. If negative symptoms are in part a response to fragmentation, then treatments which address fragmentation may impact negative symptoms.
One recently emerging approach addressing the fragmentation related to negative symptoms is concerned with the study of metacognition. Metacognition in this research, following the paradigm of the integrated model (Lysaker & Dimaggio, 2014; Lysaker, Hamm, Hasson-Ohayon, Pattison, & Leonhardt, 2018), refers to a spectrum of activities which range from awareness of discrete mental and bodily experiences to the synthesis of those into a larger integrated sense of self and others. Intact metacognitive processes thus are in part what enables persons to have a sense of themselves and others which is automatically available to them within the flow of life. Operationalized definitions of metacognitive deficits thus share a theoretical link with Bleulers’ concept of splitting of fragmentation of thought, affect, and will. Specifically, persons with metacognitive deficits would be said to experience themselves and others in a fragmented way, with more discrete experiences failing to be integrated into the larger sense of self and others that enables a sense of agency and continuity of action over time.
To date, there are several reasons to believe that fragmentation reflected by metacognitive deficits could contribute to negative symptoms. As reviewed elsewhere, there is mounting evidence that deficits in metacognition are common in schizophrenia and are a barrier to a broad range of adaptive functions. Cross-sectional research across different international settings has also found correlations between lower levels of metacognitive functioning and a range of negative symptoms (Lysaker et al., 2005, 2018; Lysaker, Vohs, et al., 2015; MacBeth et al., 2016; Nicolò et al., 2012; Popolo et al., 2017; Trauelsen et al., 2016; WeiMing, Lysaker, & Kai, 2015).
A larger study of 163 adults with prolonged schizophrenia reported that a group identified as having anhedonia in the absence of depression had poorer metacognition relative to another group without anhedonia or a third with both anhedonia and depression (Buck et al., 2014). More compelling three studies with follow-up of 6–12 months have found that more severe metacognitive deficits predict more severe levels of negative symptoms after controlling for initial levels measured concurrently with metacognitive function (Hamm et al., 2012; Lysaker, Kukla, Dubreucq, et al., 2015; McLeod, Gumley, MacBeth, Schwannauer, & Lysaker, 2014). Other incidental support for a link between metacognition and negative symptoms can be found in research, suggesting that metacognitive deficits predict concurrent and future deficits in intrinsic motivation, a concept closely related to negative symptoms (Luther et al., 2016, 2017).
To explore this issue further, the current study sought to test whether metacognitive capacity among patients with FEP predicted negative symptoms after a follow-up period of 3 years. We further planned to explore negative symptoms at the level of individual symptoms in the light of recent literature, suggesting that a monolithic account of negative symptoms may not capture the broad range of experiences which comprise the construct (Harvey et al., 2017). Negative symptoms examined were blunted affect, emotional withdrawal, poor rapport, passivity, and alogia. These are seen as the core negative symptoms measured in Positive and Negative Syndrome Scale (PANSS) (VanDerGaag et al., 2006). We predicted that initial levels of metacognition would be related to both concurrent and future levels of negative symptoms.
Methods
Setting
The OPUS treatment for first episode non-affective psychosis has been implemented in Denmark since 2006, building on results from the OPUS project (Nordentoft et al., 2015; Petersen et al., 2005). OPUS treatment in the psychiatric services in Region Zealand is a manualized treatment including an assertive outreach approach, psychoeducation, and family involvement. Age range for inclusion in the program is 18–35 years. The treatment lasts for 2 year includes contact with the OPUS staff at least once a week. The case load of the case managers is limited to around 10 patients.
Subjects
Inclusion criteria: All FEP patients from 18 years to 35 years with an ICD-10 diagnosis F20-29 (except F21) who were admitted to the specialized first episode psychosis (FEP) treatment program (OPUS). Patients were consecutively included, after informed consent was provided. Exclusion criteria: Patients who are not included in the OPUS treatment or who do not speak Danish. Inclusion period: April 1, 2011 to March 31, 2013. Follow-up is 3 years after the start of OPUS treatment. Baseline is defined as the date of the assessment after inclusion in the OPUS treatment.
Assessment
The patients were assessed with a range of instruments and relevant demographic data were collected. Diagnoses were confirmed using operational criteria (OPCRIT) (McGuffin, Farmer, & Harvey, 1991) by a clinical psychologist or psychiatrist.
Premorbid functioning was measured by the Premorbid Adjustment Scale (PAS) (Cannon-Spoor, Potkin, & Wyatt, 1982), covering two areas of functioning—School Adaptation and Socialization—described through initial childhood level and subsequent change (Larsen et al., 2004). Scores ranged from 1 to 6 with higher scores, indicating more impairment. A PAS change score was calculated as the difference between childhood scores and the last score available, to indicate decline or improvement over time.
Symptom levels were measured by the PANSS (Kay, Fiszbein, & Opler, 2012) from which the two-factor model of symptom domain scores was derived (Harvey et al., 2017).
Duration of untreated psychosis (DUP) was measured at inclusion as the time in weeks from emergence of the first positive psychotic symptoms (PANSS score of 4 or more on positive scale items P1, P3, P5, or P6 or General scale item G9) to the start of the first adequate treatment of psychosis, as in the TIPS study (Melle et al., 2004). Level of functioning was assessed using the Global Assessment of Functioning Scale (GAF). GAF scores were split into symptom (GAF-S) and function scores (GAF-F).
Metacognition
Indiana Psychiatric Illness Interview (IPII): The IPII is a semi-structured interview where the interviewees are asked to talk about their life. This includes their life story; the psychiatric problems that they may or may not think they have, and how they have been affected by them; how they control and are controlled by these problems; how they are affected by and affect other people; and how their future will be (Lysaker, Clements, Plascak-Hallberg, Knipscheer, & Wright, 2002). The interview is conversational with minimal amount of direction, although participants are encouraged to answer all questions in the interview and given plenty of time. This allows for a spontaneous narrative. The interview lasts about 30 min, and the responses are audio taped and subsequently transcribed.
The Metacognition Assessment Scale abbreviated (MAS-A): The MAS is a rating scale to assess metacognitive abilities and was originally designed to be used on psychotherapy transcripts in personality disorders (Semerari et al., 2003). This study used a modified version, MAS-A, which was designed for the assessment of metacognitive capacity as a broader integrative process (Lysaker et al., 2005). This abbreviated version contains four scales: “Self-Reflectivity” (the ability to think about one’s own mental states), “Understanding Others” (the ability to think about others’ mental states), “Decentration” (seeing the world as existing with others having independent motives), and “Mastery” (the ability to implement effective strategies in order to cope with psychological problems and related distress). For each scale, higher ratings reflect the capacity to engage in more complex metacognitive acts and the maximum total score is 28. Ratings were made based on participants’ responses to the IPII.
MAS-A has been widely used with schizophrenia patients with acceptable reliability and validity and has been able to predict various psychosocial outcomes independent of symptoms and neurocognition (Lysaker et al., 2010; Lysaker, Gumley, et al., 2011; Lysaker, Erickson, et al., 2011).
Reliability
To establish the reliability of the instruments, 17 cases were randomly drawn from the sample, where the material consisted of video interviews of the PANSS interviews and vignettes. All raters had to score the vignettes concerning diagnosis, substance abuse, DUP, GAF-F, and GAF-S. Agreement was tested for the following ICD-10 diagnoses: schizophrenia, schizoaffective disorder, brief psychotic disorder, delusional disorder, and psychotic disorder Not otherwise specified (NOS). For these five diagnostic categories, we found an overall agreement of 82.4% and a median κ of .52. For the dimensional variables, we found the following Inter class correlation (ICC) (2, k) coefficients: DUP .94, alcohol abuse .91, drug abuse .98, GAF function .62, and GAF symptoms .73. For the PANSS, the ICC (2, k) coefficients were positive component score .81, negative component score .90, depressive component score .86, excitement component score .64, and cognitive component score .81.
Reliability for MAS-A: Thirty-one randomly drawn IPII transcripts were rated by the two raters involved in the baseline ratings (JEJ and AMT). The ICC (2,2) was .944 for the total MAS-A score. For the subscales, the ICC (2,2) was between .795 and .973.
Data analysis
Analyses were made with IBM SPSS for Windows, version 21. The applied methods are reported in parentheses for all group comparisons. All tests were two tailed. Both parametric and nonparametric tests for correlation were used for data without normal distribution. If there were no significant statistical differences between parametric and nonparametric test results, a pragmatic decision to report the parametric results was made for ease of interpretation. Partial correlations were undertaken to control for the impact of baseline negative symptoms when examining the association between metacognition and negative symptoms at 3-year follow-up.
Ethics
All participants received oral and written study information. It was clearly stated that they could withdraw their consent at any time and that participation had no impact on the treatment. The protocol was submitted to the Regional Ethics Committee and pre-approval was found unnecessary. The Data Protection Council, Region Zealand, approved data management (REG-044-2013).
Results
All patients (N = 194) included in the OPUS treatment during the inclusion period were reviewed to participate in the project. A total of 130 patients (67%) agreed to participate in the study. The median time from start of the OPUS treatment to inclusion in the project was 91 days (range 0–456 days, interquartile range 47–154 days). PANSS data from baseline and follow-up and MAS-A data from baseline were available for 59 participants (45.4%) and these patients were included in the current analysis.
Table 1 contains the baseline characteristics of the patients included in the analysis and those not included in the analysis due to missing follow-up data. The two groups did not significantly differ on the majority of characteristics apart from metacognition where the not included group had slightly lower MAS-A total, self-reflectivity, and mastery scores.
Characteristics of participants.
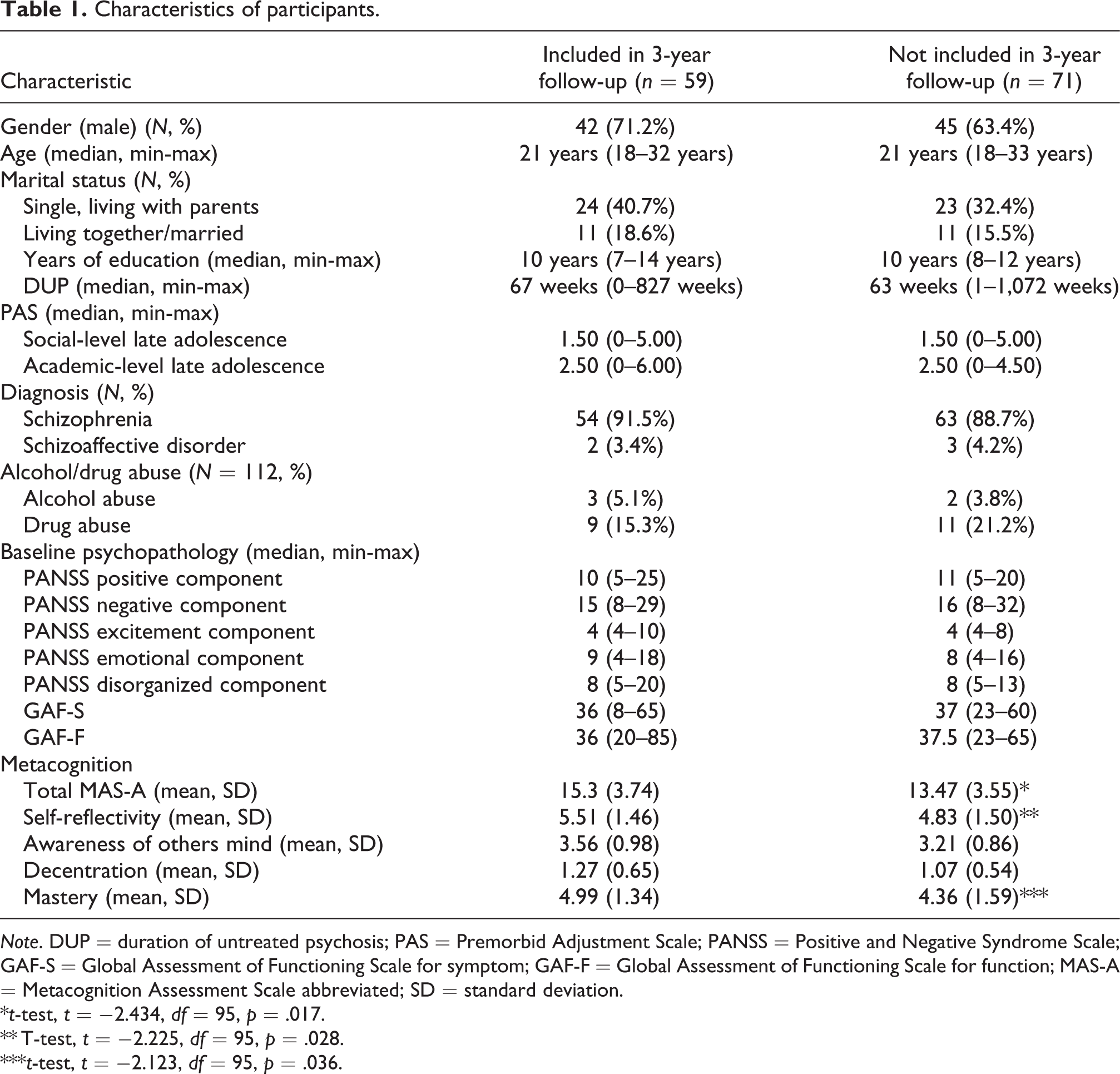
Note. DUP = duration of untreated psychosis; PAS = Premorbid Adjustment Scale; PANSS = Positive and Negative Syndrome Scale; GAF-S = Global Assessment of Functioning Scale for symptom; GAF-F = Global Assessment of Functioning Scale for function; MAS-A = Metacognition Assessment Scale abbreviated; SD = standard deviation.
*t-test, t = −2.434, df = 95, p = .017.
** T-test, t = −2.225, df = 95, p = .028.
***t-test, t = −2.123, df = 95, p = .036.
Table 2 contains the correlations between baseline metacognition and baseline negative symptoms, negative symptoms at 3-year follow-up, and negative symptoms at 3-year follow-up after controlling for baseline symptoms. There are significant negative correlations between baseline metacognition and all baseline negative symptoms examined (blunted affect, emotional withdrawal, apathy, poor rapport, and alogia) with correlations (r) ranging from .23 to .49.
Correlations between baseline metacognition (MAS-A) total scores and negative symptoms at baseline and 3-year follow-up.

Note. Numbers in bold are statistically significant. PANSS = Positive and Negative Syndrome Scale; MAS-A = Metacognition Assessment Scale abbreviated.
When examining correlations between baseline metacognition and negative symptoms at 3-year follow-up, correlations become nonsignificant for emotional withdrawal and apathy but remained significant for blunted affect, poor rapport, and alogia where correlations ranged between .36 and .41. The correlations between baseline metacognition and these negative symptoms remained significant when controlling for baseline negative symptoms.
Based on the two-factor model of negative symptoms, validated for PANSS (Harvey et al., 2017), a composite score for the expression domain (blunted affect, alogia, and poor rapport) and experience domain (emotional withdrawal and apathy) was calculated. Results revealed that the expressive domain was found to be significantly negatively correlated with baseline metacognition at 3-year follow-up when controlling for baseline negative symptoms (r = −.27, p = .045), while the experience domain at 3-year follow-up was not significantly correlated with baseline metacognition. Baseline metacognition was not significantly correlated with total negative symptom score on PANSS at 3-year follow-up when controlling for baseline negative symptoms (r = −.207, p = .122).
The potential impact of demographic variables was also examined. Females scored significantly higher on metacognition (MAS-A total) than males at baseline (15.94 vs. 14.11, p = .033) and people who were older scored higher on metacognition (MAS-A total) at baseline (r = .284, p = .029), although controlling for these variables in the analysis did not change any of the significant results, where baseline MAS-A scores predicted negative symptoms at 3-year follow-up after controlling for baseline negative symptoms. DUP and years of education were not significantly correlated with baseline MAS-A total scores.
In an explorative analysis intended to build upon the significant relationships found between the MAS-A baseline scores correlated with some negative symptoms at 3-year follow-up, we examined whether specific domains in metacognition (self-reflectivity, understanding others, decentration, and mastery) were associated with negative symptoms at 3-year follow-up. Results of the correlational analysis are contained in Table 3 and demonstrate that only self-reflectivity is significantly correlated with the expressive component of negative symptoms at 3-year follow-up after controlling for negative symptoms at baseline.
Correlations of metacognitive domains with expressive and experience components for negative symptoms at 3-year follow-up after controlling for baseline symptoms.

Note. Numbers in bold are statistically significant. MAS-A = Metacognition Assessment Scale abbreviated.
Discussion
In this study, we examined the concurrent and prospective links between metacognitive capacity and negative symptoms at the general level and in terms of five specific items: blunted affect, emotional withdrawal, poor rapport, passivity, and alogia. As predicted, overall metacognitive capacity and negative symptoms were significantly related at the global level and at item level for 5 of 5 items with lesser metacognitive capacities predicting more severe levels of negative symptoms. The observed links between metacognition and negative symptoms were found to persist 3 years later at the global level and for three of five symptoms: blunted affect, poor rapport, and alogia. The relationship of initial levels of metacognition with negative symptoms after 3 years was found to persist when controlling for initial total levels of negative symptoms as well as two specific negative symptoms: blunted affect and poor rapport. When negative symptoms were divided into experiential and expressive symptoms, initial levels of metacognition were found to predict expressive negative symptoms after 3 years after controlling for initial levels of expressive symptoms.
Taken together, result is consistent in part with a Bleulerian model which understands the emergence of negative symptoms as a response in part to the experience of fragmentation, particularly in terms of sense of self and others. Specifically, one interpretation of our findings is that with metacognitive deficits, persons lose access to an integrated and coherent sense of self and others and present with graver difficulties, experiencing and expressing internal states in the moment and over a course of years. These individuals may be especially vulnerable to developing further difficulties expressing thoughts and feelings and forming connections with others. It may be, for example, that negative symptoms emerge as persons are unable to form a sense of how their thoughts and feelings are a meaningful response within the larger context of their lives. Other interpretations of these results are possible including that factors which predispose persons to develop negative symptoms may produce metacognitive deficits at earlier phases of the illness.
It was unexpected that metacognition was not significantly related to the development of experiential negative symptoms in general. This may reflect the possibility that the experiential component of negative symptoms could be influenced by a broader range of factors including social networks, social skills, or isolation. As with unexpected findings, further research is necessary before any conclusions are drawn.
These results along with previously longitudinal studies (Hamm et al., 2012; Lysaker, Kukla, Dubreucq, et al., 2015; McLeod et al., 2014; Wells & Cartwright-Hatton, 2004) suggest a number of clinical implications. First, if metacognitive deficits are predictors of the development of symptoms which are generally unresponsive to treatment, it may be that interventions that target metacognitive capacity early in the illness may have a protective effect and can facilitate long-term outcomes such as recovery. There are a number of promising interventions that could improve metacognition within populations with psychosis. These include metacognitive training (Liu, Tang, Hung, Tsai, & Lin, 2018; Moritz, Veckenstedt, Randjbar, Vitzthum, & Woodward, 2011), metacognitive therapy (Morrison et al., 2014) (Hutton, Morrison, Wardle, & Wells, 2014), and metacognitive insight and reflection therapy (MERIT). Of these, preliminary evidence exists that MERIT may affect the forms of metacognition tested in this study and has been linked to reports in qualitative studies leading to richer and more coherent sense of self (de Jong et al., 2018; Lysaker, Kukla, Belanger, et al., 2015). Further studies are required to determine how these interventions impact on different aspects of metacognition.
It is also important to place the results in context of the limitations of the study. The sample size was modest, although this study still included more participants than previous studies examining longitudinal relationships between negative symptoms and metacognitions (Hamm et al., 2012; McLeod et al., 2014). There was a significant dropout rate at 3-year follow-up where people not included in the follow-up had slightly lower scores on metacognition, meaning it could difficult to generalize these results to broader FEP population. Neurocognition was not measured, and research has shown that this can be linked to both metacognition and negative symptoms. Finally, the design of study also prohibited the identification of any possible causal associations between metacognition and negative symptoms.
Conclusion
In conclusion, this is the first study to collect and analyze data on metacognition and negative symptoms over a period of several years. Results thus offer unique opportunities to examine how deficits in metacognition detected at diagnosis of a psychotic illness may impact on the long-term prognosis of negative symptoms among a well-defined and assessed population with FEP. Significant associations were found between a number of negative symptoms and metacognition, where symptoms comprising the expressive domain symptoms (blunted affect, poor rapport, lack of spontaneity and flow in speech) found to be predicted by baseline metacognition at 3-year follow-up. While the study design prohibits causality, it highlights an area of future research to clarify the role metacognition may have in the development and maintenance of negative symptoms.
Footnotes
Authors’ note
The protocol was submitted to the Regional Ethics Committee and pre-approval was found unnecessary. The Data Protection Council, Region Zealand, approved data management (REG-044-2013).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Region Zealand Health Scientific Research Foundation.