
Abstract
Negative symptoms and depression persist in one third of patients with schizophrenia. Previous studies suggested that depression has more impact on self-perceived compared to observer-rated social functions. Reduced emotional experience, a subdomain of negative symptoms, predicts social functioning deficits, although its role in self-assessment is unclear. We examined depression and reduced emotional experience and self-reports and informant ratings of social functioning and social cognitive abilities in 135 patients with schizophrenia. Discrepancies between sources were used to index the accuracy and bias in self-assessment. Less severe depression was associated with self-reports of reduced impairments in social functioning and better social cognitive abilities. Reduced emotional experience was related to informant ratings and self-reports of social functioning. Neither reduced emotional experience nor depression was correlated with discrepancies between sources, despite the bias of patients with lower depression to report that they were higher functioning and more competent. These findings suggest that patients with schizophrenia make global judgments about functioning based on current mood states. There was minimal association between the depression severity and the accuracy of self-assessment, despite positive biases associated with lower depression severity. The determinants of accuracy and bias in self-assessment requires more detailed examination and subdivision of patients based on their depression.
Introduction
Depression is commonly experienced by people with schizophrenia. Within unselected samples of patients with schizophrenia, patients often have a depression severity score close to moderate depression (Strassnig et al., 2015). Additionally, large-sample studies of patients with schizophrenia suggest that a third or more of those studied have experienced an episode of major depression (Harvey et al., 2014). Furthermore, depression experienced by people with schizophrenia is associated with increased suicidal ideation and behavior (Harvey et al., 2018). What is less clear, however, is the impact of depression on everyday functioning. Two recent large-scale (N > 800) studies of depression in schizophrenia demonstrated that depression was not directly correlated with impairments in everyday functioning rated by high-contact informants (Galderisi et al., 2014; Strassnig et al., 2015).
A more consistent impact of mood symptoms, and or the absence thereof, on functioning in schizophrenia is in the domain of self-assessment of cognitive and functional skills (Harvey & Pinkham, 2015). In an analysis of the Clinical Antipsychotic Trials of Intervention Effectiveness [CATIE] schizophrenia trial, Siu et al. (2015) found that patients who reported very low levels of depression generated inaccurate self-assessments of their functioning (i.e., impaired introspective accuracy) and manifested an introspective bias toward overly optimistic assessments. The introspective bias was positive in this study, but these biases can include both overestimation and underestimation of abilities compared to objective reference points. In a later study directly comparing the impact of depression on self-assessments as compared to clinician ratings of functioning (Harvey, Twamley, Pinkham, Depp, & Patterson, 2017), less severe depression was again found to be associated with greater inaccuracy in self-assessment, indexed by lower congruence between informant ratings and self-reports, but not with reduced functioning deficits based on the informant ratings. Patients with more severe depression generated ratings that were more congruent with high contact informants but did not have more functional deficits than patients with lower levels of depression. Thus, different levels of depression may be associated with either increased introspective accuracy or increased introspective bias without any significant impact on actual functioning.
In contrast to the severity of depression, negative symptoms have been shown to correlate with social outcomes, as well as other functional outcomes, across numerous studies (Strauss et al., 2013). Within the domain of negative symptoms, there appears to be differing importance of the symptoms for the prediction of social functioning outcomes. Symptoms of reduced emotional experience, referred to as avolition–apathy, can be separated from reduced emotional expression both in terms of factor structure (Jang et al., 2016) and in terms of subgroups of patients who differentially manifest these symptoms (Strauss et al., 2013). Symptoms of reduced emotional experience have been found to be more consistent predictors of informant-rated impairments in functional outcomes compared with symptoms of reduced emotional expression (Harvey et al., 2017, in press; Strassnig, Bowie, et al., 2018).
Elements of reduced emotional experience have been shown to share up to 20% of the variance with clinical ratings of impairments in social outcomes (Robertson et al., 2014). Although there is some overlap in the item content between the reduced emotional experience rated on the Positive and Negative Syndrome Scale (PANSS) and informant ratings of social functioning outcomes, the sources of information were still independent in those studies. Reduced emotional experience has also been found to be associated with informant-rated social functioning across the full range of negative symptom severity (Strassnig, Bowie, et al., 2018). When the influence of performance-based measures of social competence and social cognition was added to reduce emotional experience as predictors, close to a third of the variance in informant-rated social functioning can be accounted for (Kalin et al., 2015).
What is less clear is the association between reduced emotional experience and self-assessment of functional abilities, in terms of both influences on introspective accuracy and introspective bias. As patients with reduced emotional experience are found to have reduced levels of social interactions, it is possible that the reduction in real-world social experience might affect their ability to self-evaluate their functioning. We previously found that patients with schizophrenia who had never worked in their lives reported that their work skills were better than patients with current full-time employment (Gould, Sabbag, Durand, Patterson, & Harvey, 2013), reflecting substantial positive introspective bias. We also found, in a different sample, that lack of experience in real-world activities did not correlate with poorer performance on tests of everyday functional skills (Holshausen, Bowie, Mausbach, Patterson, & Harvey, 2014). Thus, real-life experience appears to have a stronger relationship with self-assessment of ability than on the ability to perform the required functional skill. This may suggest that negative symptoms and the resultant lack of social experience might lead to an impaired ability to self-evaluate social outcomes or social cognitive skills. Further, if the patterns of bias were similar to those seen with employment and experience, it would be predicted that higher levels of reduced emotional experience would be associated with positive introspective bias, including overestimation of social cognitive abilities and social outcomes.
In this study, we examine the association between severity of self-reported depression and clinically rated reduced emotional experience with the results of self-assessments and high-contact informant assessments of everyday social functioning and social cognitive abilities. We previously demonstrated that informant ratings of social cognitive ability were correlated with performance on a large-scale battery of social cognitive tests as well as with informant-rated social outcomes (Silberstein, Pinkham, Penn, & Harvey, 2018). In contrast, self-assessments on the social cognition rating scale among patients with schizophrenia did not relate to performance on any of the eight social cognitive tests. Given that introspective accuracy has been previously demonstrated to be an important predictor of outcomes (Gould et al., 2015; Silberstein et al., 2018), we also sought to assess this ability in the current sample and directly test whether depression and reduced emotional experience are related to introspective accuracy for everyday functioning. We hypothesized that reduced emotional experience would be associated with positive introspective bias in that reduced experience might lead to over confidence in both social functioning and social abilities. As noted earlier in the cases of less versus more severe depression, accuracy and bias may actually be independent depending on the level of severity of the symptom of interest.
Our hypotheses for the study were that depression would be strongly related to self-assessments of everyday social functioning and social cognitive abilities in a sample of people with schizophrenia, with reduced depression predicting increased positive introspective bias. We also hypothesized that the severity of depression would be more strongly related to self-reports than informant ratings of social outcomes and social cognitive ability. We also hypothesized that reduced emotional expression would result in introspective accuracy deficits and positive introspective bias induced by lack of real-world experience.
Method
Participants
Data were collected as part of the final phase of the Social Cognition Psychometric Evaluation (SCOPE) study and all of the methods were previously described (Pinkham, Harvey, & Penn 2018). There were three study sites: The University of Texas at Dallas (UTD), The University of Miami Miller School of Medicine (UM), and The University of North Carolina at Chapel Hill (UNC). Participants were stable outpatients with diagnoses of schizophrenia or schizoaffective disorder (n = 135). Only patients with a high contact informant, a caregiver, a case manager, or a psychologist were included in this study, because previous evidence from earlier studies shows that such informants generate ratings with adequate validity (Sabbag et al., 2011). All informants whose data were used reported that they knew the patient “very well.” This led to the exclusion of 83 patients who were reported on in the previous article whose community informants indicated knowing the patient less than “very well,” as indexed by their rating of the knowledge of the patient and their contact with them on the functional outcomes rating scale.
UTD patients were recruited from Metrocare Services, a nonprofit mental health services provider organization in Dallas County, TX, and other area clinics. UM patient recruitment occurred at the Miami VA Medical Center and the Jackson Memorial Hospital-University of Miami Medical Center, and UNC patients were recruited from the Schizophrenia Treatment and Evaluation Program in Carrboro, NC, and the Clinical Research Unit in Raleigh, NC. To be eligible, patients required a Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) diagnosis of schizophrenia or schizoaffective disorder which was generated with a structured diagnostic procedure described previously (Pinkham et al., 2018). Patients could not have had any hospitalizations within the last 2 months and had to be on a stable medication regimen for a minimum of 6 weeks with no dose changes for a minimum of 2 weeks. The study was approved by the institutional review board at all study sites, and all participants signed an informed consent form.
Measures
Negative symptoms assessment
Severity of negative symptoms was assessed using the PANSS (Kay, Fiszbein, & Opler, 1987), which was administered in its entirety by trained raters. These ratings were performed for the entire PANSS, and the subsequent subdivisions of the negative symptom data occurred after the ratings were collected.
Negative symptom models
In previous reports by Khan et al. (2017), Harvey, Khan, & Keefe (2017), and Strassnig, Bowie, et al. (2018), a two-factor model of reduced emotional experience and reduced emotional expression was developed and replicated in multiple samples as well as being tested for relationships to functional outcomes. The items in each of the two factors were as follows:
PANSS reduced expression: PANSS Blunted Affect (N1), Poor Rapport (N3), Lack of Spontaneity (N6), and Motor Retardation (G7);
PANSS reduced emotional experience: Emotional Withdrawal (N2), Passive Social Withdrawal (N4), and active social avoidance (G16).
Based on previous research, including analyses with this sample, we knew that reduced emotional experience was not correlated with the informant ratings of social outcomes and did not examine it in this study. A total score for the 3-item reduced emotional experience scale was created by summing the severity scores.
Observable Social Cognition Rating Scale
Both patients and high-contact informants completed the Observable Social Cognition Rating Scale (OSCARS) (Healey et al., 2015). The OSCARS is an 8-item assessment of social cognition. Each OSCARS item is comprised of a question probing a social cognitive domain (theory of mind, emotional perception, cognitive rigidity, jumping to conclusions, and attributional style), followed by general example behaviors that reflect impairment in that domain. Participants ranked their abilities in each item on a 7-point scale, with higher ratings indicating greater impairment. An additional question assessed the impression of global social cognitive impairment. The global ratings utilized a 10-point scale and again higher ratings indicated greater impairment (range 1–10). The patient was asked the questions in a standard interview format. Informants completed the form by themselves using the same instructions that the interviewer provided to the patients to rate the patient’s level of impairment.
The OSCARS has previously been validated in two comprehensive studies. In the first study (Healey et al., 2015), the internal consistency of the OSCARS was .80 in patients, with test–retest reliability of the items ranging from .50 to .70. Informant ratings on the OSCARS were found to correlate with several different measures of social cognition and social functioning, including both performance-based and rating-scale measures. In the second study (Silberstein et al., 2018), we found that global ratings on the OSCARS accounted for 15% of the variance in a performance-based assessment of social cognition. In this study, we used the informant-rated and self-reported global scores as the outcome variables.
Specific level of functioning
Real-world functional outcome was assessed via the 31-item version of the specific level of functioning (SLOF) (Schneider & Strunening, 1983), a self- or informant-rated measure of functioning. In this study, separate patient and informant scores were produced. We focused solely on interpersonal relationships (e.g., initiating, accepting and maintaining social contacts, effectively communicating) and social acceptability (e.g., appropriateness of verbal and physical behavior), because we had previously reported on the general lack of association in this database between negative symptoms and other aspects of outcome (Strassnig et al., 2015; Harvey et al., 2017). Patients were interviewed by a trained rater, and informants completed the scale as a questionnaire, in line with our previous use of this scale in multiple studies (Bowie, Reichenberg, et al., 2006; Harvey et al., 2011; Pinkham, Penn, Green, & Harvey, 2016). Ratings for each item were made on a 1–5 point scale, with higher scores indicating better functioning. An average item score across each subscale was used as the dependent variable in the event of that informants were unable rate specific items. For this scale, like the OSCARS, we had both self-reported and informant-rated scores as the outcomes variables.
Procedures
Participants completed two study visits: baseline and a retest assessment conducted 2–4 weeks after the initial visit (mean interval = 16.69 days). Only data from Visit 1 were used here, and at this visit, all participants provided informed consent and completed the performance- and interview-based social cognitive and functional outcome measures. This visit also included diagnostic assessment and the PANSS assessment described earlier. Diagnostic and symptom raters were trained to reliability using established procedures at each site. All informants received no training and had no information about any performance-based, clinically rated, or self-reported data on the participants.
Data analyses
Informant ratings of the two SLOF subscales and the global social cognition item from the OSCARs and self-reports of the same variables were used as dependent variables. Total scores on the Beck Depression Inventory (BDI-II) as well as the PANSS reduced emotional experience subscale served as predictors.
The differences between high-contact informants’ ratings and self-ratings were used to index introspective accuracy and introspective bias. For SLOF subscales, higher discrepancy scores indicated overestimation of performance compared to informants, as an index of introspective bias. For OSCARS, higher discrepancy scores indicated that patients were also overestimating their social cognitive ability compared to informants. To consider the bidirectional nature of introspective accuracy in self-assessment, we created absolute value scores for the differences and compared each of them to zero with a one-tailed t-test. Thus, even if the average for the sample was zero, this analysis would reveal whether there were impairments in terms of both overestimation and underestimation of skills and functioning.
Pearson correlations were used to assess the relative strength of correlations between four SLOF functional outcomes scores (i.e., self-reported and informant-rated interpersonal functioning and self-reported and informant-rated social acceptability) and the differences between informant- and self-reports, OSCARS ratings (informant, self-report) and differences between informant- and self-reports, depression, and reduced emotional experience.
Next, we computed a set of regression analyses to identify the associations between depression, negative symptoms, and self-rated or informant-rated OSCARS and SLOF scores. These analyses were limited to predictors that showed significance in the correlational analyses. These analyses were computed with separate stepwise entry regressions, predicting each of the outcome variables.
Results
Table 1 presents the demographic information on the subset of patients with high-contact informants who participated in this study. Supplemental Table 1 presents the full information previously published. Table 2 presents the scores on the SLOF and OSCARS variables as well as depression and negative symptoms. Although the mean difference scores for introspective accuracy were all close to zero, not reflecting a consistent direction of introspective bias, the range of scores was quite large and bidirectional. Interestingly, all three of the absolute values for the introspective accuracy difference scores were significantly different from 0, interpersonal: t(128) = 12.99, p < .001; social acceptability: t(128) = 11.98, p < .001, and OSCARS: t(128) = 15.77, p < .001. Thus, deficits in introspective accuracy for social cognition, social functioning, and socially acceptable behavior were present in the sample and were found to be bidirectional.
Descriptive information on the sample of patients with high-contact informants (n = 135).

Scores on ratings of everyday functioning and predictor variables.

Note. SLOF = specific level of functioning; OSCARS = Observable Social Cognition Rating Scale
aMean item score.
bHigher scores reflect less impairment.
cHigher scores reflect more impairment.
Table 3 presents the Pearson correlations between the negative symptoms and depression and the SLOF and OSCARS variables. Reduced emotional experience was significantly correlated with informant-rated impairments in social functioning and with all three of the self-reported functioning variables. However, reduced emotional experience was not associated with impairments in introspective accuracy or evidence of introspective bias. Total scores on depression were correlated with all three informant-rated aspects of functioning and all three self-reports of functioning. However, depression, examined across the full range of scores, was not associated with introspective bias scores. Only one of the absolute-value scores was correlated with one of the three symptoms variables, with the absolute value of introspective accuracy for social acceptability correlated with the severity of depression, r = .22, p = .015. This suggests that higher levels of depression were associated with more discrepancy between informant and self-report ratings in this functional domain.
Correlations between depression, negative symptoms, social functioning, and social cognition.

Note. SLOF = specific level of functioning; OSCARS = Observable Social Cognition Rating Scale.
*p < .05; **p < .01; ***p < .001.
The regression analyses used reduced emotional experience and depression to predict self-reported and informant-rated social functioning and social cognition. These results are presented in Table 4. Informant-rated interpersonal functioning was predicted primarily by reduced emotional experience, with a smaller contribution from depression. Depression was the only predictor of informant-rated social acceptability and social cognition. Furthermore, depression had a strong relationship with all three of the patient-reported outcomes, with patient-reported outcomes sharing at least 23% of the variance with depression. Interestingly, patient-reported interpersonal functioning deficits shared 13% of the variance with PANSS ratings of reduced emotional experience.
Regression analyses predicting everyday social functioning and social cognition.
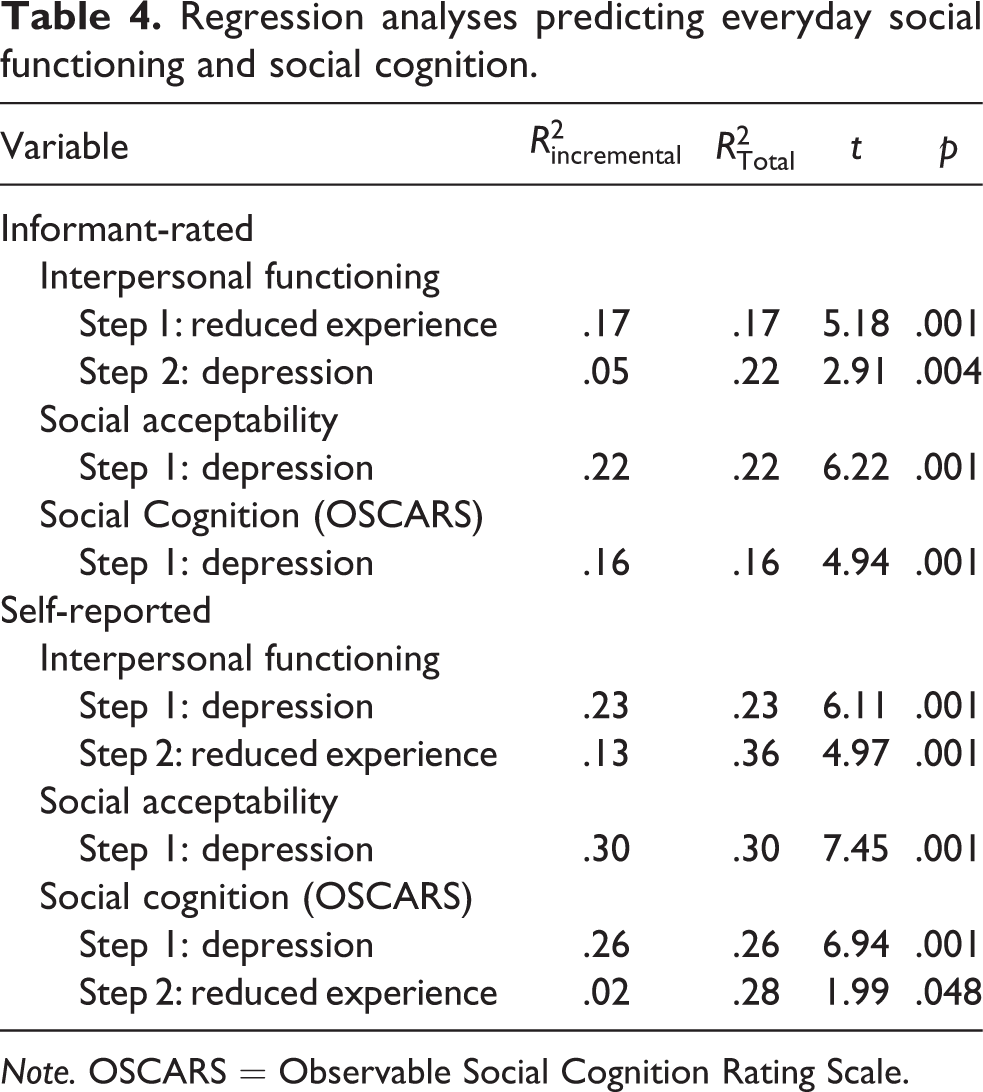
Note. OSCARS = Observable Social Cognition Rating Scale.
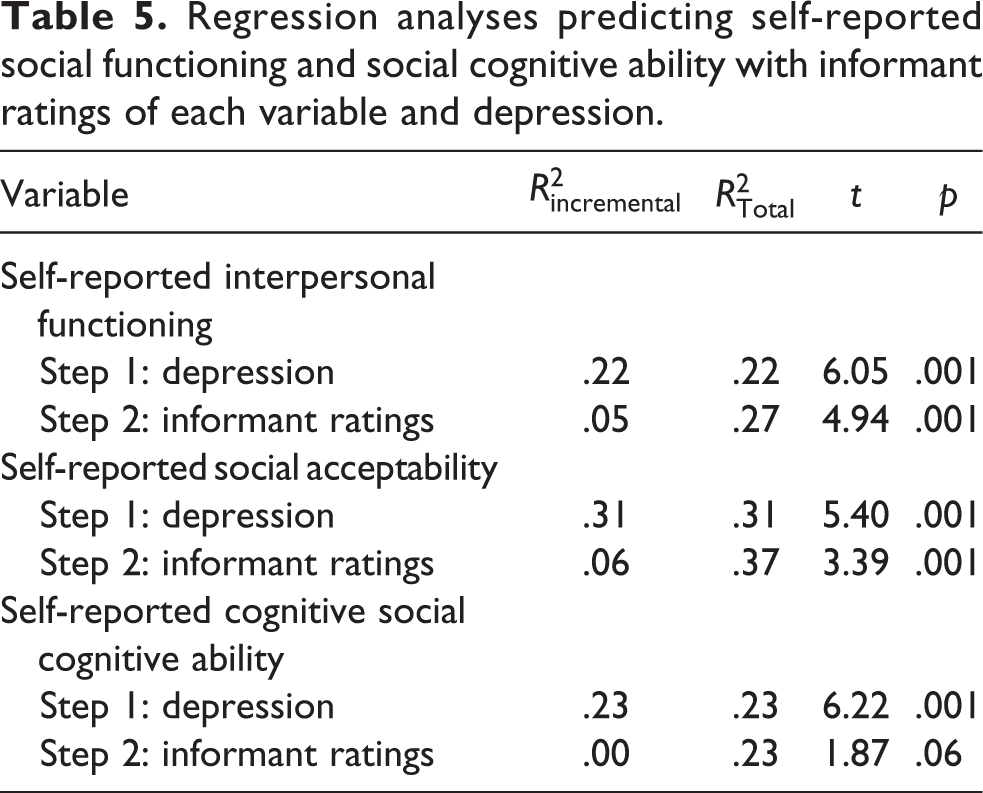
A final set of analyses was conducted to determine the extent to which depression was associated with each self-reported aspect of social functioning while controlling for informant-rated functioning in that same domain. Each of the self-reported functioning variables was predicted by severity of depression and informant ratings on that same variable, using a stepwise regression analysis. The results are presented in Table 5. For all three self-reported social functioning variables, depression entered the equation first. For interpersonal functioning and social acceptability, both depression and informant ratings of interpersonal functioning were significant predictors of self-reports, with depression accounting for markedly more variance in the outcome variables.
Regression analyses predicting self-reported social functioning and social cognitive ability with informant ratings of each variable and depression.
Discussion
This study examined the association between the severity of depression and reduced emotional experience and self-reported and informant-rated assessments of everyday social functioning and social cognitive abilities as well as differences in those ratings intended to index impairments in introspective accuracy and introspective bias. Patients were found to have statistically significant levels of impairment in introspective accuracy, defined as the difference between informant and self-ratings across functional domains. On average, patients were as likely to overestimate their skills and performance as to underestimate. The level of introspective bias, an overly optimistic self-assessment, in the sample was not significantly different from 0, suggesting no specific direction of introspective bias in this sample, in contrast to several previous studies in independent samples were people with schizophrenia manifested positive introspective bias for several different functional domains (Bowie, Twamley, et al., 2006; Durand et al., 2015; Harvey et al., 2017). However, consistent with previous reports, the severity of depression was substantially associated with self-reports of everyday functioning, with lower severity associated with reports of better social functioning.
Severity of depression on the part of patients was consistently associated with self-reported social functioning and social cognitive ability. Within the domain of negative symptoms, reduced emotional experience was, as expected, associated with informant ratings of social impairments but was also correlated with all self-reported assessments of social functioning and social cognition. Reduced emotional experience was not correlated with informant ratings of either socially acceptable behavior or social cognitive abilities. The symptomatic predictors of self-reports were quite consistent, and patients with more severe depression and reduced emotional experience reported that they were more impaired in both everyday functioning domains of social outcome and in social cognitive skills.
Also of interest is the finding that severity of depression correlated with informant ratings of all three functional domains, although the regression analyses reduced this result for interpersonal functioning. Importantly, depression was previously found to be unrelated to performance on social cognition tests in this sample (Strassnig et al., submitted). Thus, while informants are sensitive to social cognitive abilities and can rate them accurately in reference to social cognitive test performance (Silberstein et al., 2018), depression on the part of patients appears to affect rater judgments of social cognitive ability, possibly inducing a rater bias.
Another finding of importance is that introspective accuracy seems to be separate from depression and negative symptoms. The lack of an association between introspective accuracy and depression runs counter to our hypothesis and our previous findings regarding other elements of everyday functioning (Harvey, Twamley, et al., 2017). In that study, however, depression was divided on the basis of severity into three groups, with the group with the least severe depression manifesting a strong positive introspective bias regarding their social functioning and the most depressed group showing evidence of unimpaired introspective accuracy and no introspective bias. The impact of depression on introspective accuracy may also be more pronounced when task performance is used to anchor introspective accuracy assessments (Durand et al., 2015).
The presence of negative symptoms of reduced emotional experience correlated with patients endorsing greater interpersonal functioning deficits and more social cognitive limitations and did not correlate with either introspective accuracy or introspective bias. This finding suggests that reduced emotional experience is not exerting a systematic bias toward over-estimating functioning on the part of patients based on lack of recent social experience. A potential limitation of the present study, however, is that PANSS is not designed as a measure for negative symptoms.
A previous study of depression and negative symptoms had somewhat similar findings. Strauss, Sandt, Catalano, and Allen (2012) examined the correlations between depression, reduced emotional expression, and reduced emotional experience and subjective quality of life. As in our study, both depression and reduced emotional experience were correlated with greater subjective impairments in functioning and illness-related burden, while reduced emotional expression was only correlated with one of seven outcome variables. As that study did not collect informant ratings to compare to self-reports, the authors were not able to examine the differential importance of these factors for differential prediction of these outcomes.
Although the severity of depression was not correlated with either introspective accuracy or introspective bias in this study, patients referenced their level of depression when reporting their social functioning. Their depression shared more variance with their self-reports of functioning than information coming from informant ratings. This effect was most pronounced for self-reported social cognitive ability, where informant ratings of social cognitive ability shared no variance with self-reports when depression considered. For social functioning, possibly because of the availability of objective anchor points for self-assessment, there was some shared variance with informant ratings, but the majority of the influence on self-reports was mood symptoms. However, self-reports of depressed mood, collected at a single time point, manifested the strongest relationships with self-assessments of global social cognitive ability, everyday social functioning, and problems in interpersonal relationships.
These findings are consistent with a recent study of patients with schizophrenia and bipolar disorder (Strassnig, Kotov, et al., 2018), wherein patients were asked to rate their disability with a structured self-report scale and the ratings were then related to achievement of concurrent functional milestones. Regression analyses indicated that cognitive performance, physical performance, independence in residence, and current employment shared no variance with self-reported disability in the sample. In contrast, Hamilton Depression Rating scale scores collected at a single time point accounted for 11% of the variance in self-reported disability, across the two diagnoses. Thus, reports of everyday functioning in schizophrenia, and possibly bipolar disorder, do not appear to be nearly as strongly linked based on objective indicators of everyday functioning as to the severity of depression on the day of assessment.
The results of a recent study examining social cognitive introspective accuracy with neuroimaging strategies may provide some clarity regarding the origins of these impairments (Pinkham, Klein, et al., 2018). In patients with schizophrenia, there was significantly less activation than Healthy Controls (HC) in a critical cortical region, the rostrolateral Pre-Frontal Cortex (RLPFC) while performing social cognitive introspective accuracy tasks. RLPFC activation predicted the performance of HC on the introspective accuracy task, while it did not in patients. Critically, RLPFC activation while performing introspective accuracy tasks predicted high-contact informant ratings of everyday social functioning generated with the SLOF. Thus, introspective accuracy competence has specific brain functioning correlates that are also socially relevant, implicating a direct influence of introspective accuracy competence on objectively measured social functioning.
Conclusions
Introspective accuracy was significantly greater than 0 in this study, but introspective bias was not. People with schizophrenia did not report that their functioning was better than that seen by high-contact informants as they did in several previous studies, but they did appear to rely on mood states to make global statements about their functioning across different domains. Deficits in reduced emotional experience were not associated with introspective accuracy or introspective bias and introspective accuracy and introspective bias were not correlated with each other. Future research should identify the factors that are associated with introspective accuracy deficits, with some suggestions that there are specific brain functioning differences between HC and people with schizophrenia that determine introspective accuracy and related social dysfunctions.
Supplemental material
Supplemental_Table_1_(4) - Depression and reduced emotional experience in schizophrenia: Correlations with self-reported and informant-rated everyday social functioning
Supplemental_Table_1_(4) for Depression and reduced emotional experience in schizophrenia: Correlations with self-reported and informant-rated everyday social functioning by Philip D. Harvey, Elizabeth Deckler, Mackenzie T. Jones, L. Fredrik Jarskog, David L. Penn and Amy E. Pinkham in Journal of Experimental Psychopathology
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Harvey has received consulting fees or travel reimbursements from Alkermes, Boehringer Ingelheim, Intra-Cellular Therapies, Jazz Pharma, Minerva Pharma, Otsuka America, Roche Pharma, Sanofi Pharma, Sunovion Pharma, Takeda Pharma, and Teva during the past year. He receives royalties from the Brief Assessment of Cognition in Schizophrenia. He is chief scientific officer of i-Function, Inc. He has a research grant from Takeda and from the Stanley Medical Research Foundation. Dr. Pinkham has served as a consultant to Roche Pharma. Jarskog has received research grant funding from NIH, Auspex/Teva, Boehringer-Ingelheim and Otsuka. The other authors have no reportable biomedical activities.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a grant from the US National Institute of Mental Health, MH 93432, to Drs. Harvey, Penn, and Pinkham.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.