
Abstract
“Addressing time management, energy balance, and mental wellbeing may therefore be key strategies in promoting exercise engagement among medical students.”
Introduction
Medical students face a unique set of psychological and physical challenges stemming from the demanding nature of their training. The academic rigor, competitive environment, and long hours contribute to disproportionately high rates of burnout, depression, stress, and impaired quality of life compared to the general population.1-3 Studies suggest that up to 50% of medical students experience symptoms of burnout, and approximately 25% report clinical symptoms of depression. 1 These issues not only affect student wellbeing but can persist beyond medical school, increasing the risk of long-term psychiatric disorders and suicidal ideation, with serious implications for the future physician workforce. 3
Amid these concerns, regular physical activity and sufficient sleep have emerged as modifiable lifestyle behaviors that significantly improve mental and physical health, reduce symptoms of anxiety and depression, and promote overall wellbeing.4,5 Despite this, research consistently shows that medical students often experience a decline in both exercise and sleep quality during their training. 4 Interestingly, while some evidence suggests that medical students may initially be more physically active than the general population, their activity levels tend to decrease with each year of training.6,7 This paradox highlights a concern regarding the sustainability of wellness behaviors in this population.
There is a growing body of literature suggesting that regular exercise is associated with decreased burnout and improved quality of life among medial trainees.4,6-11 Among medical students specifically, meeting the Centers for Disease Control and Prevention (CDC) guidelines for aerobic and strength training activities has been linked to reduced rates of burnout and enhanced quality of life. 7 Furthermore, satisfaction with exercise has been positively correlated with academic performance, social connection, and personal relationships. 12 The mode, intensity, frequency, and duration of exercise also appear to influence these outcomes, with higher-intensity exercise associated with greater self-reported happiness among medical students.11-13 In addition to these personal benefits, medical students who prioritize their own health behaviors are more likely to serve as effective role models and health advocates for their future patients.6,7,14,15
Despite these benefits, multiple barriers continue to prevent medical students from maintaining consistent exercise routines. Chief among these are time constraints, academic workload, fatigue, and financial stress.9,12,16 These obstacles may fluctuate over time, with third-year students—who typically face demanding clinical rotations—reporting the highest levels of perceived difficulty in maintaining physical activity.12,17 In contrast, fourth-year students often report greater satisfaction with their wellness behaviors, potentially due to more flexible schedules or shifting priorities. 12 Lack of physical activity is not a benign issue; it is associated with increased depressive symptoms and elevated stress.4,9 For example, one study found that students not meeting health-enhancing physical activity (HEPA) levels had significantly higher stress scores than their more active peers. 9
While prior research has explored the relationship between physical activity and select dimensions of medical student wellness, few studies have offered a comprehensive, multidimensional analysis that includes factors such as sleep, social support, perceived academic performance, and common barriers to exercise. Additionally, limited data exist on how these variables collectively influence perceived stress and quality of life among medical students.
To address this gap, we conducted a cross-sectional survey among medical students at an LCME accredited allopathic medical school in the United States. The survey assessed demographic characteristics, physical activity patterns (including adherence to CDC guidelines for aerobic and strength training), exercise type, perceived exercise barriers, sleep quantity and sleepiness, perceived stress, social support for exercise, quality of life, and self-reported academic performance. The objectives were to (1) describe the prevalence and characteristics of physical activity, (2) examine associations between exercise and key wellness indicators, and (3) identify the most significant barriers to maintaining regular physical activity.
Findings from this study may inform the development of targeted wellness interventions aimed at fostering sustainable health behaviors in medical students. By focusing on early prevention of burnout and psychosocial distress during training, this research contributes to the foundation for longitudinal strategies in physician wellness. In addition, our results may help guide institutional policies and programs that support medical student wellbeing throughout their training.
Methods
Study Design and Subject Selection
This is an IRB-approved cross-sectional analysis of students across the 4-year M.D. program at an allopathic medical school in the Southeastern U.S. Students were sent an email invitation to complete an online Qualtrics survey in the fall of 2024. Participation in the survey was voluntary, and no incentive for survey completion was offered. Subjects were included with the criteria of being a full-time medical student at the participating university. Individuals with incomplete survey responses were excluded from the data analysis. There are approximately 120 students per year in the associated M.D. program.
Survey Measures
Exercise Habits
To assess adherence with CDC exercise guidelines, we asked students to specify the number of minutes spent per week on moderate-intensity exercise and vigorous-intensity exercise, and the number of times per week they strength-trained each major muscle. 18
We also collected data on specific types of exercise students engage in and whether they predominantly partake in individual or group exercise. Furthermore, we asked students to indicate any barriers they face in being able to engage in exercise.
Burnout
We evaluated burnout using a non-proprietary, single-item tool that was previously shown to be effective in evaluating burnout in healthcare providers. 19 Students were asked to indicate their level of burnout on a scale of 1-5 (1 = “I enjoy my work. I have no symptoms of burnout.” 2 = “Occasionally I am under stress, and I don’t always have as much energy as I once did, but I don’t feel burned out.” 3 = “I am definitely burning out and have one or more symptoms of burnout, such as physical and emotional exhaustion.” 4 = “The symptoms of burnout that I’m experiencing won’t go away. I think about frustration at work a lot;” 5 = “I feel completely burned out and often wonder if I can go on. I am at the point where I may need some changes or may need to seek some sort of help.”). We considered students to have burnout symptoms if they reported a score greater than or equal to 3. 19
Stress
A 10-item Perceived Stress Scale (PSS-10), one of the most widely used psychological instruments for measuring the perception of stress, was used to assess stress levels among medical students over the past month. 20 Several similar studies have utilized the PSS-10 to assess stress levels in this population.1,9,21,22 Each item was scored from 0 (never) to 4 very (often) based on frequency of experiencing a given scenario (e.g., “In the last month, how often have you felt nervous and stressed”?). We categorized student stress levels into 3 categories corresponding to low stress (0-13), moderate stress (14-26), and high stress (27-40) based on total stress scores. The PSS-10 has been shown to be reliable with Cronbach’s alpha as high as 0.91. 23
Quality of Life
A validated 5 item linear analog scale assessment was used to assess students’ quality of life (QOL) over the past week. 24 Each item targeted a specific domain, including physical, emotional, spiritual, intellectual, and overall wellbeing. The Likert scale runs from 0 (as bad as it can be) to 10 (as good as it can be) for each question (e.g., “How would you rate your physical wellbeing over the past week?”). A mean QOL score was calculated, with scores of 8 or higher indicating high QOL, and scores less than 8 indicating low QOL, consistent with prior research. 7 This 5 item QOL was previously found to be reliable with Cronbach’s alpha of 0.88. 24
Social Support
Perceived level of social support was measured using a 13-item social support and exercise tool.25,26 The items pertain to actions of family or friends that provide support for exercise habits. Students rated each item twice, (i.e., once for family, once for friends). For each item, students were asked to rate how often over the past 3 months family or friends offered different forms of social support for exercise. Items were rated from 1 (none) to 5 (very often), with there also being a rating of 8 (does not apply) based on the frequency for each given scenario (e.g., “Discussed exercise with me”). Social support was scored in accordance with current guidelines. 27 This tool has been found to be reliable with test-retest reliabilities (range, r = 0.55-0.86) and high internal consistencies (range, Cronbach’s alpha = 0.61-0.91). 25
Sleep
Students were asked to report their average amount of sleep per night over the past month (less than or equal to 5 h of sleep, 5 to 7 h of sleep, 7 to 9 h of sleep, or greater than or equal to 9 h of sleep). The Epworth Sleepiness Scale (ESS) was used to measure the level of daytime sleepiness. Students rated their likelihood of falling asleep on a scale of 0 (no chance of dozing) to 3 (high chance of dozing) in 8 daytime situations (e.g., “Sitting and reading”). 28 The ESS has been used as a tool to measure subjective sleepiness among medical students.1,4 Scores were used to categorize students based on levels of sleepiness (<7 unlikely to be sleepy, <9 average level of sleepiness, <15 may be excessively sleepy, <24 excessively sleepy). The questionnaire has shown strong internal consistency as measured by Cronbach’s alpha (0.88). 29
Academic Performance
We also asked students to self-report their typical module grades. First-year students did not answer this question as the survey was administered prior to assessment with formal module exams.
The recall periods for each measure were selected based on the time frames validated for each instrument and the expected stability of each construct. Stress was assessed over the past month, consistent with the PSS. Social support was measured over the past 3 months, reflecting the relative stability of perceived support. Burnout and quality of life were assessed over the past week, to capture constructs that vary over shorter timeframes.
Statistical Analysis
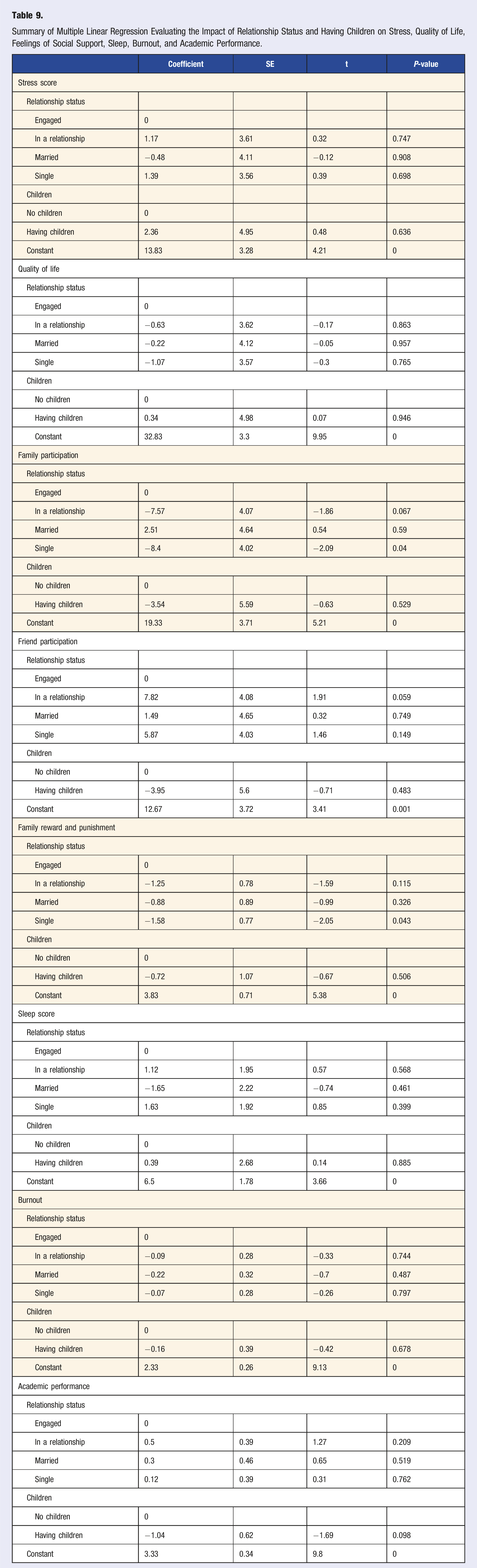
Descriptive statistics were first performed and presented to show the demographic characteristics of the study cohort. Univariate analysis was then conducted to compare the difference between meeting and not meeting CDC exercise guidelines on the variables of stress, quality of life, family participation, friend participation, family reward and punishment, sleep score, burnout, and academic performance. In this analysis, two samples t-test for normally distributed continuous variables or rank-sum tests for not normally distributed continuous variables were performed, while Fisher’s exact test was used for all categorical variables. Multiple linear regression analysis was performed to further evaluate the impact of relationship status and having children on stress, quality of life, feelings of social support, sleep, burnout, and academics. All statistical analyses were performed using Stata MP 18. α < 0.05 was considered significant in all tests.
Results
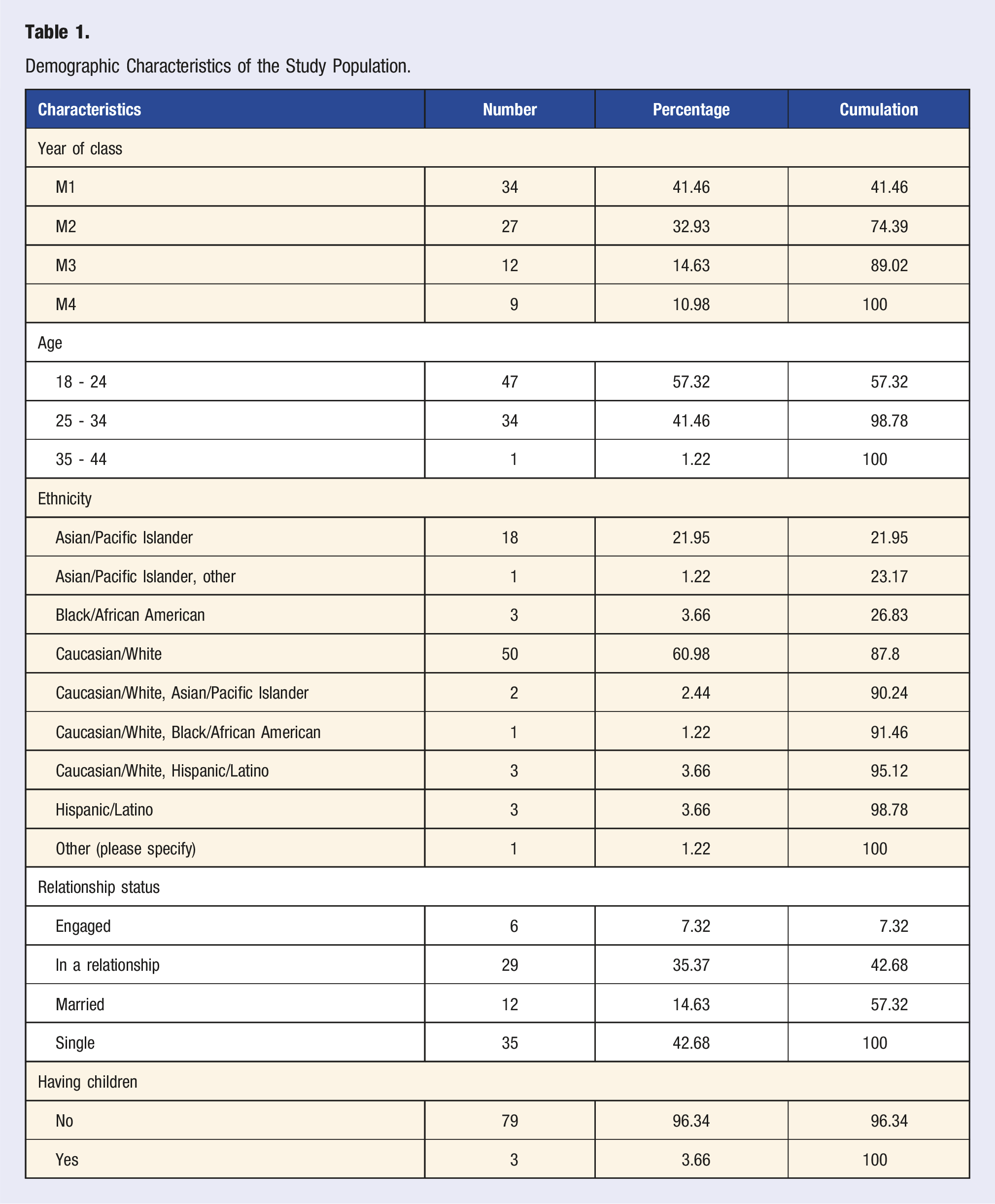
Demographic Characteristics of the Study Population.
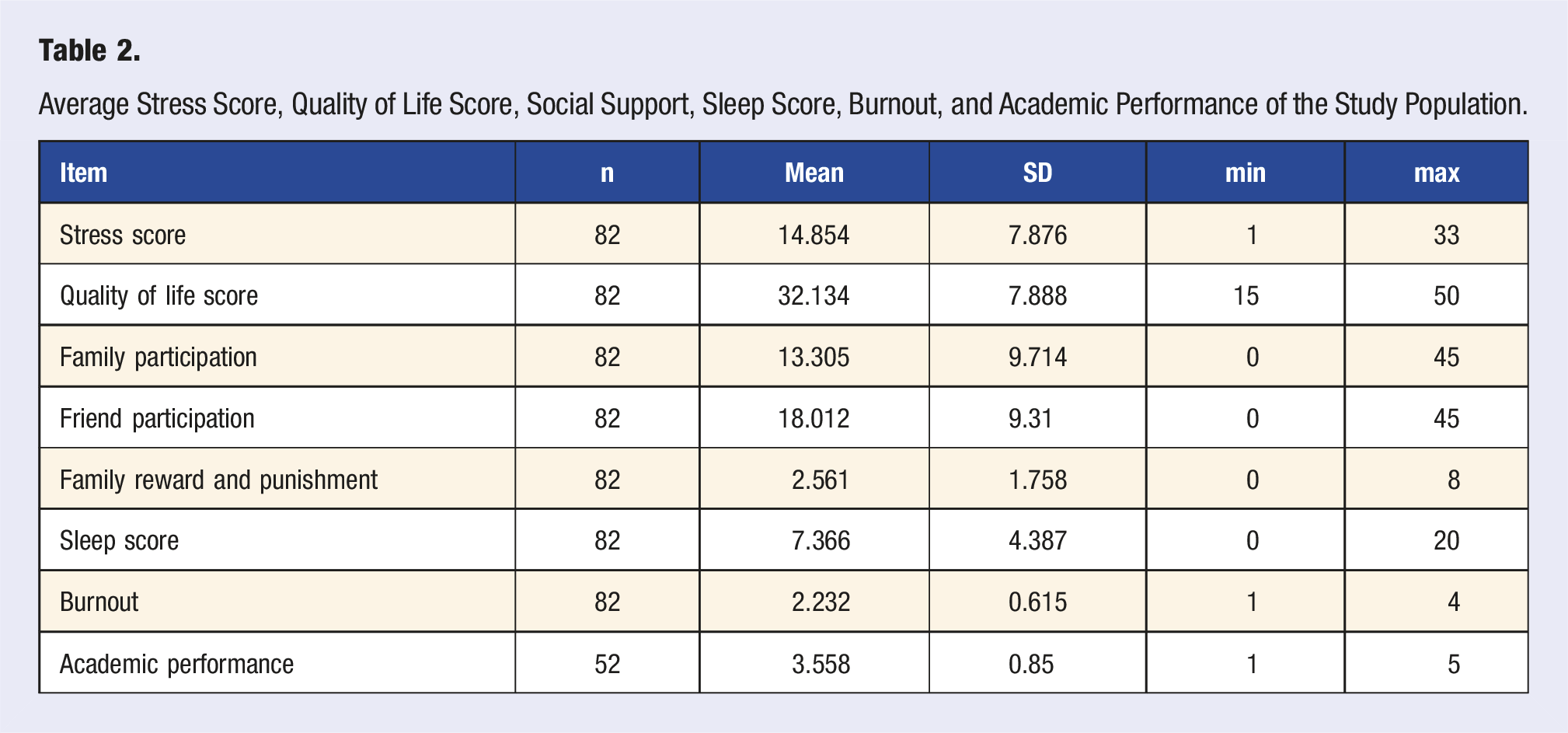
Average Stress Score, Quality of Life Score, Social Support, Sleep Score, Burnout, and Academic Performance of the Study Population.
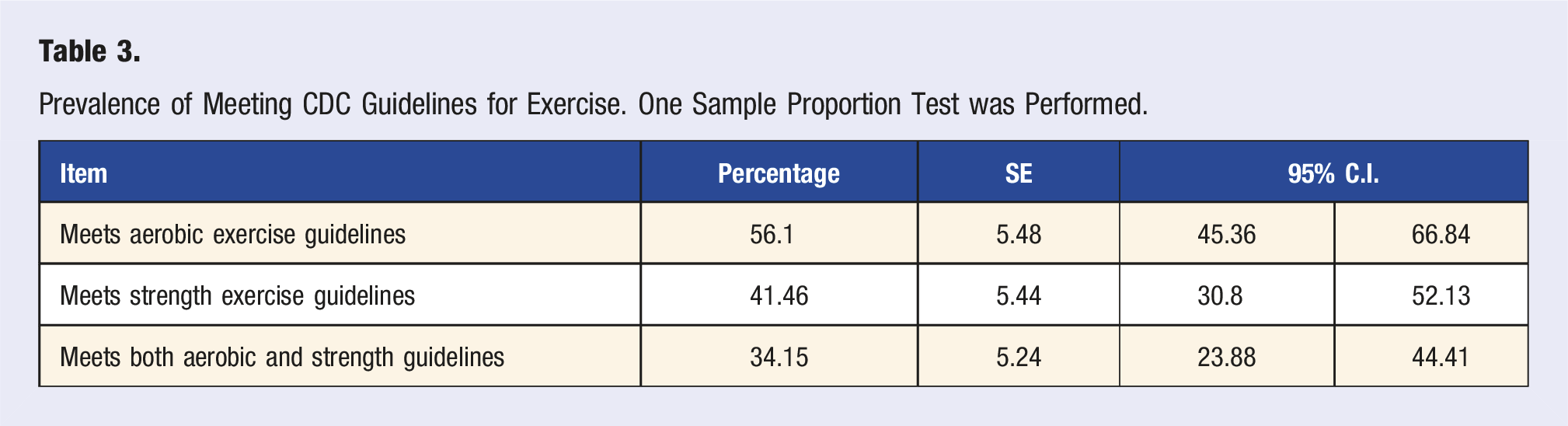
Prevalence of Meeting CDC Guidelines for Exercise. One Sample Proportion Test was Performed.
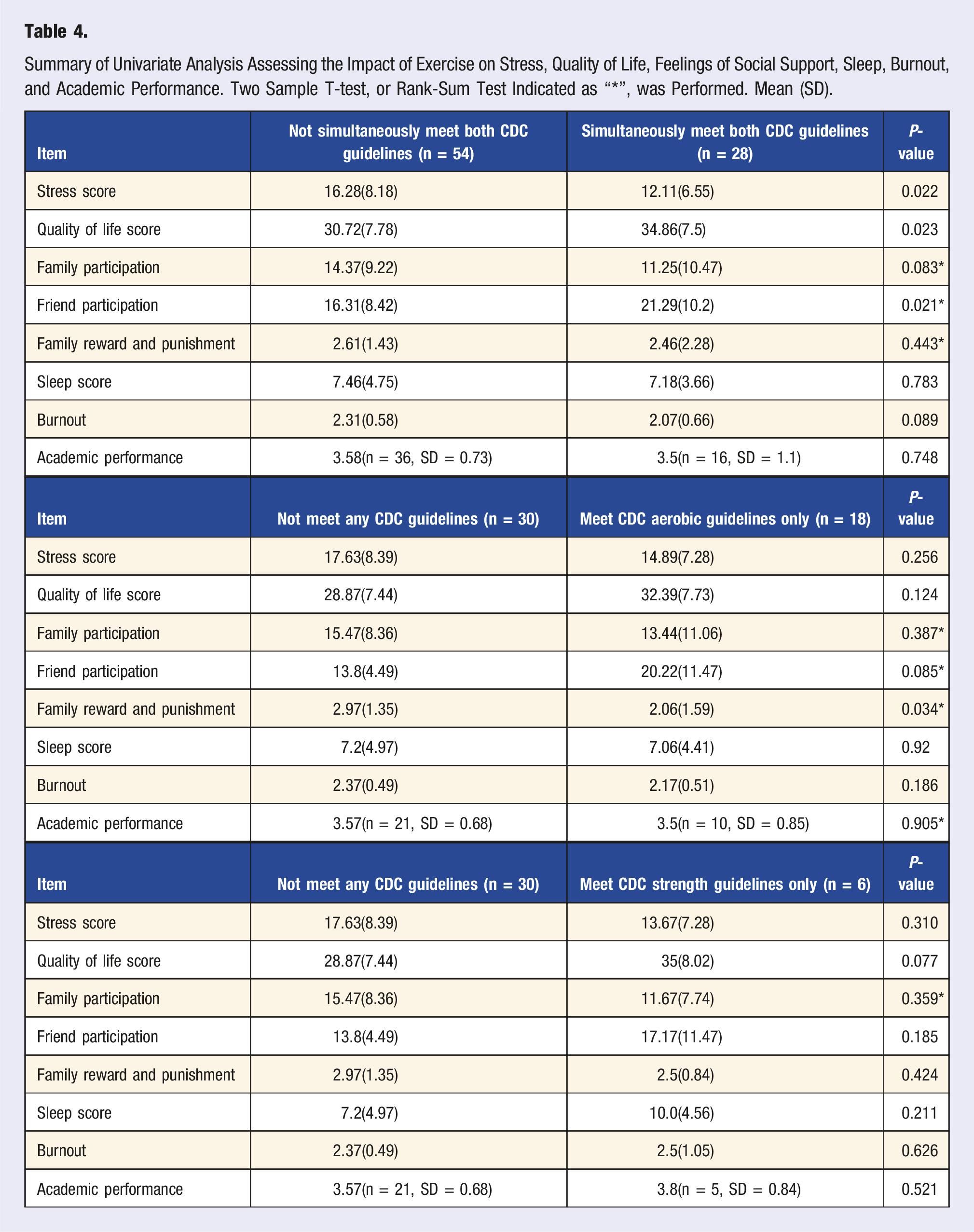
Summary of Univariate Analysis Assessing the Impact of Exercise on Stress, Quality of Life, Feelings of Social Support, Sleep, Burnout, and Academic Performance. Two Sample T-test, or Rank-Sum Test Indicated as “*”, was Performed. Mean (SD).
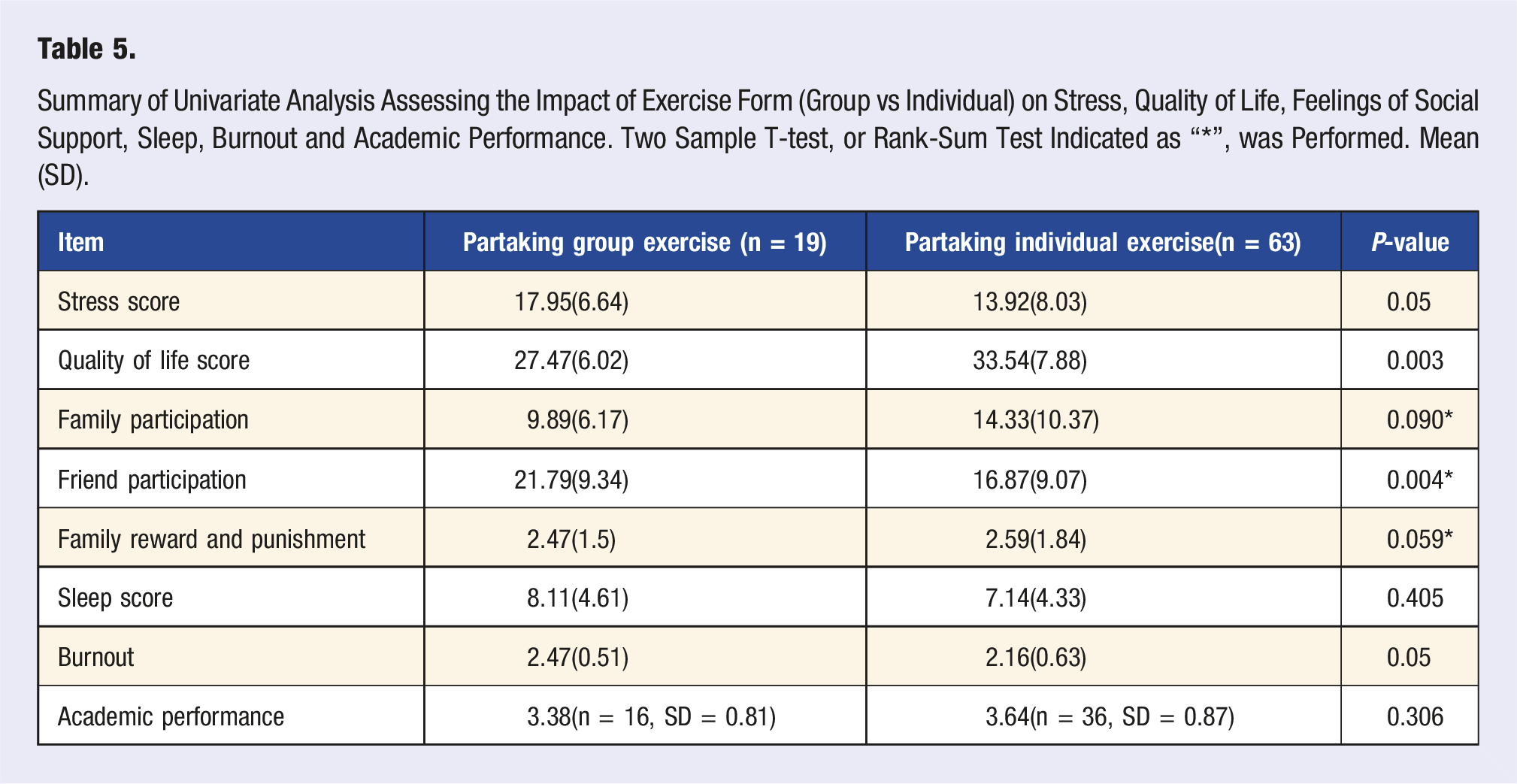
Summary of Univariate Analysis Assessing the Impact of Exercise Form (Group vs Individual) on Stress, Quality of Life, Feelings of Social Support, Sleep, Burnout and Academic Performance. Two Sample T-test, or Rank-Sum Test Indicated as “*”, was Performed. Mean (SD).
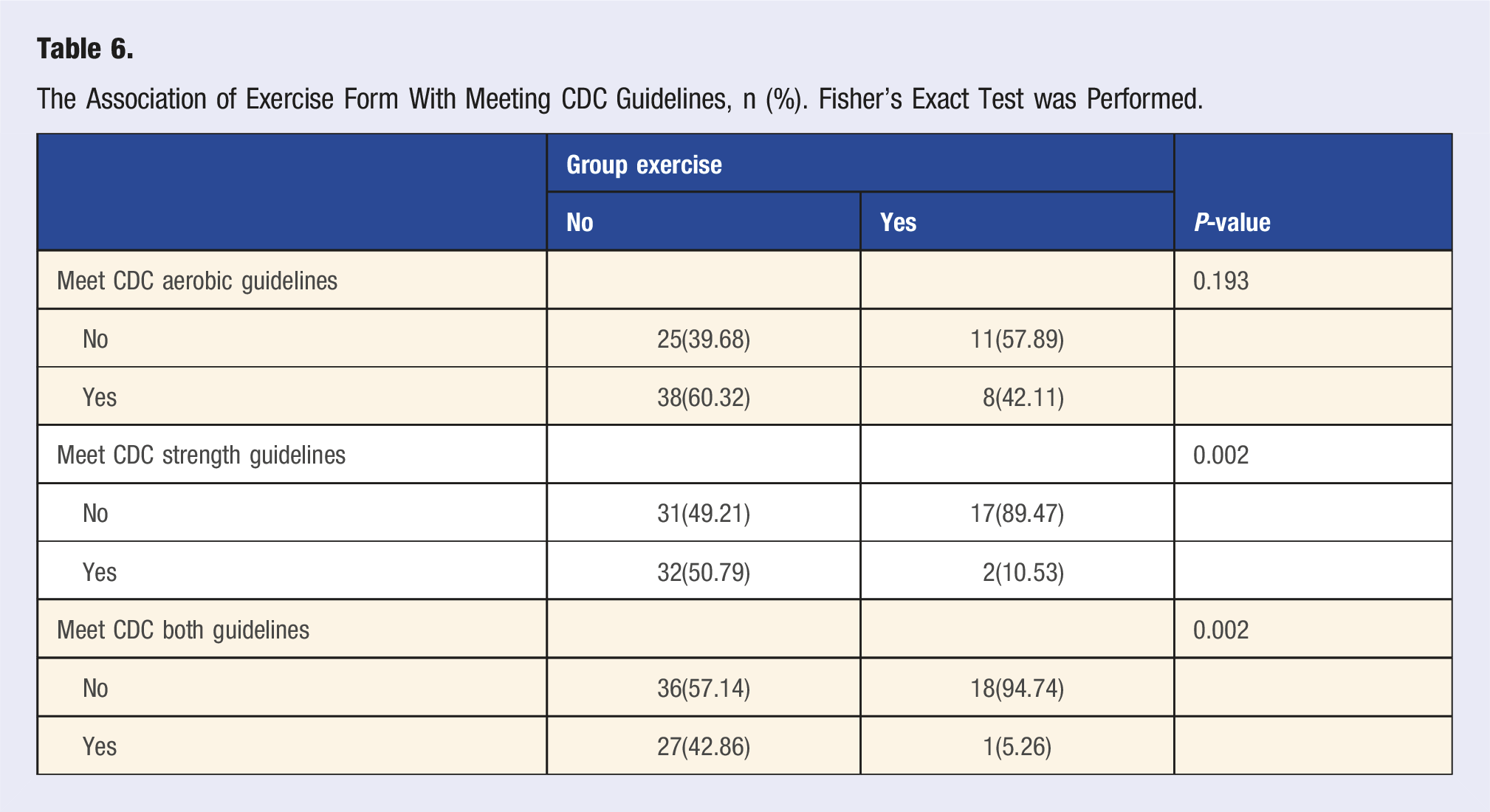
The Association of Exercise Form With Meeting CDC Guidelines, n (%). Fisher’s Exact Test was Performed.
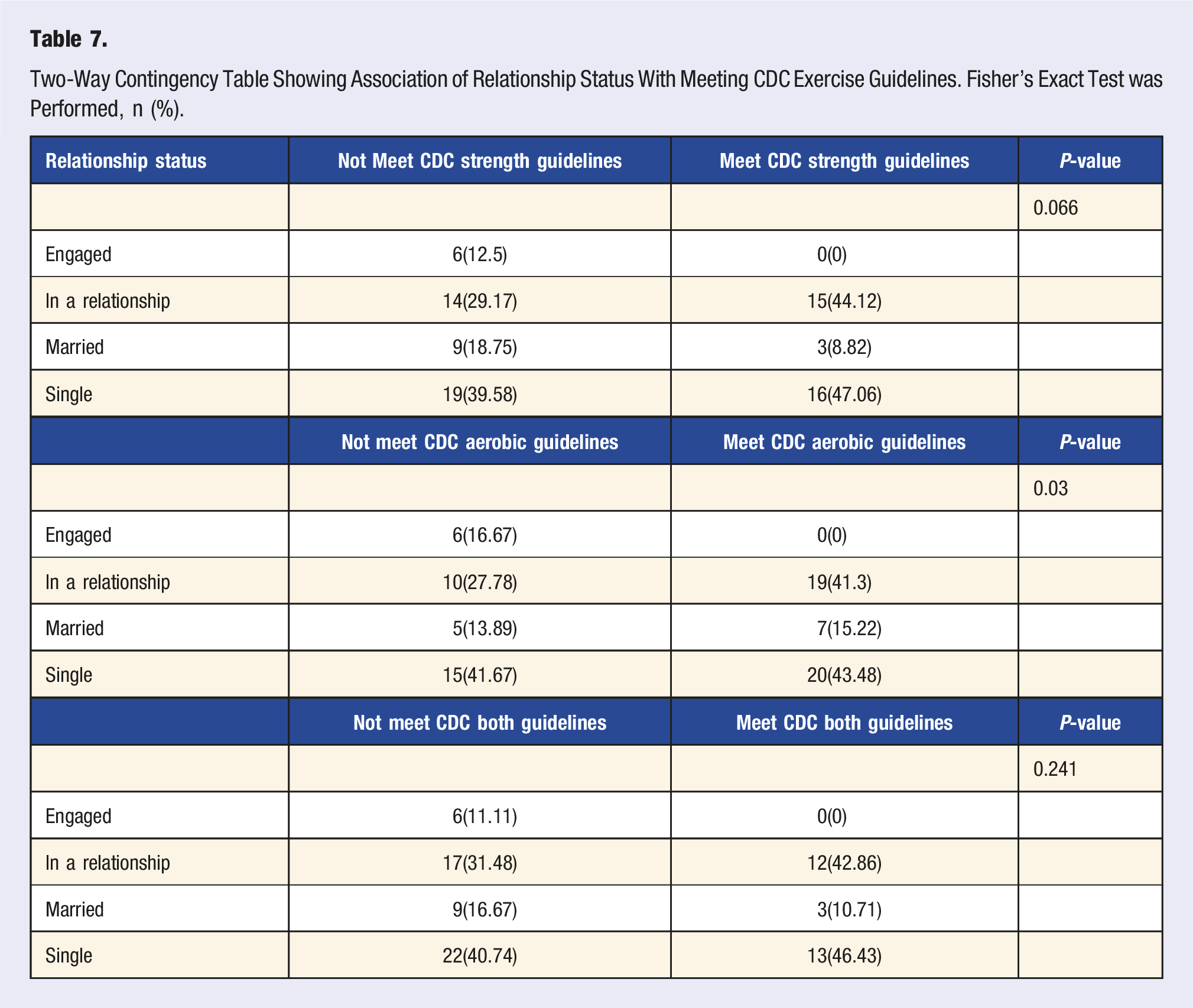
Two-Way Contingency Table Showing Association of Relationship Status With Meeting CDC Exercise Guidelines. Fisher’s Exact Test was Performed, n (%).
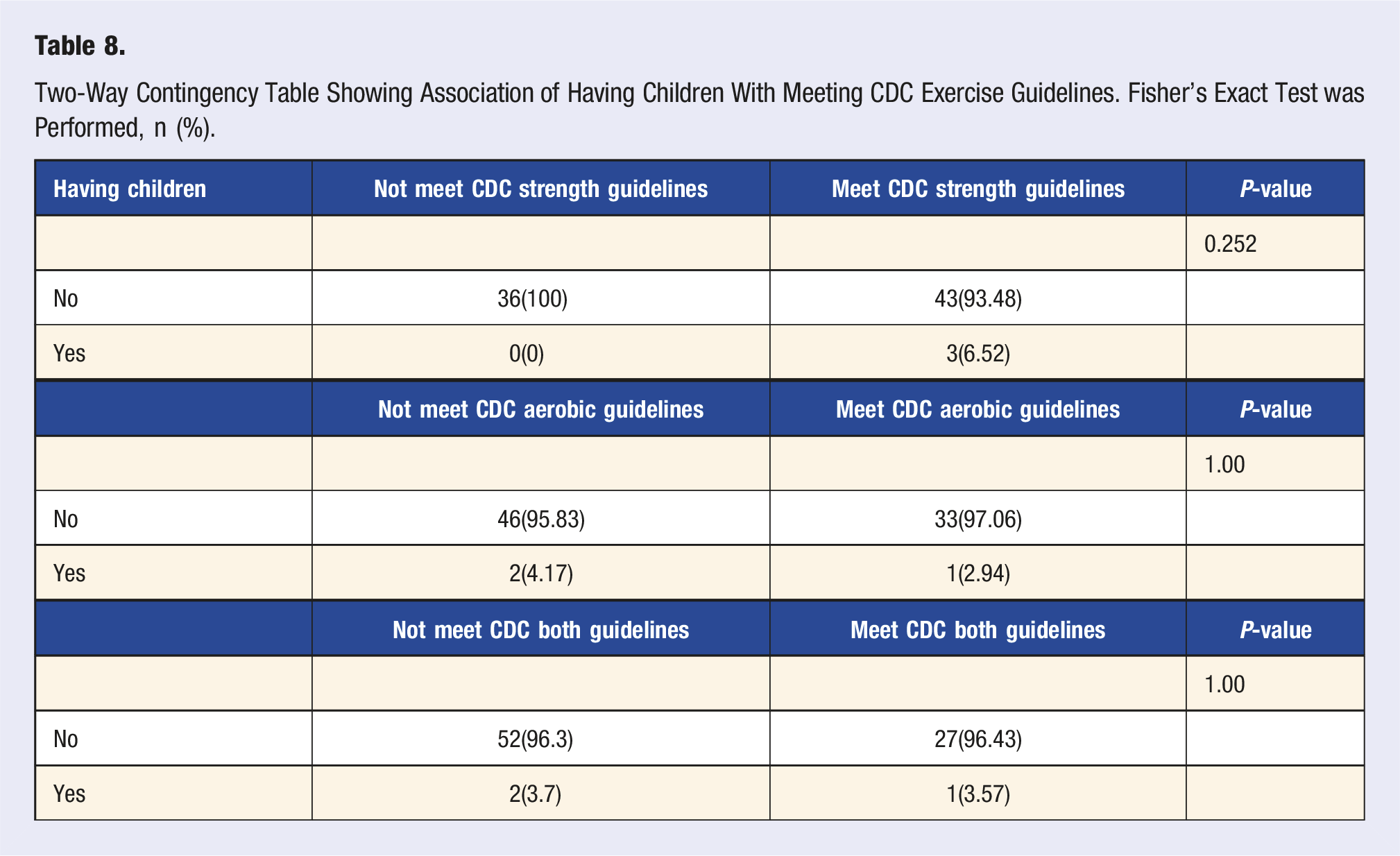
Two-Way Contingency Table Showing Association of Having Children With Meeting CDC Exercise Guidelines. Fisher’s Exact Test was Performed, n (%).
Summary of Multiple Linear Regression Evaluating the Impact of Relationship Status and Having Children on Stress, Quality of Life, Feelings of Social Support, Sleep, Burnout, and Academic Performance.
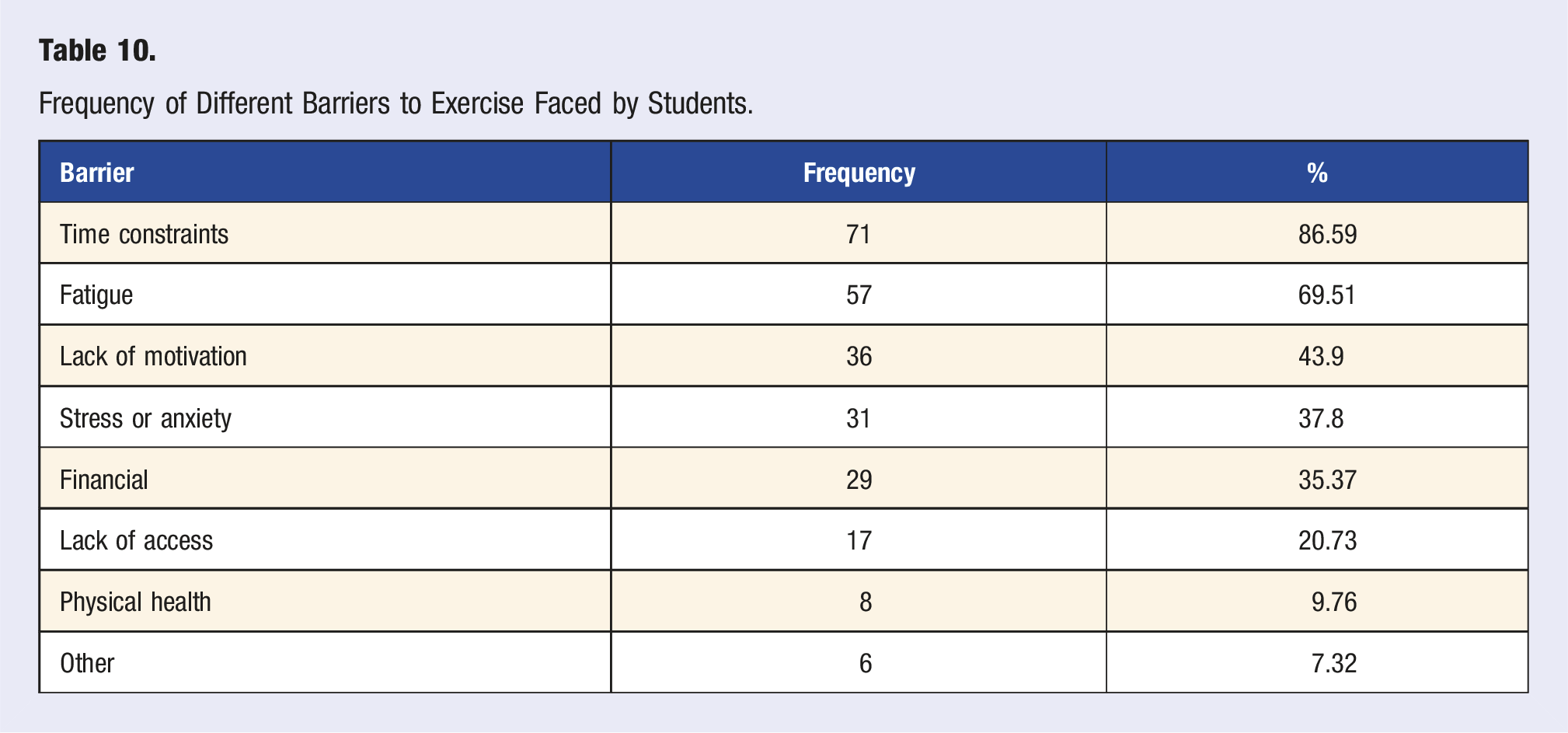
Frequency of Different Barriers to Exercise Faced by Students.
Discussion
In our surveyed medical student sample, 56.1% met CDC aerobic guidelines, 41.46% met the strength training guidelines, and 34.15% met both aerobic and strength training guidelines. Similarly, a 2012 study of over 4000 M.D. students across the U.S. found that 62.7% met CDC aerobic guidelines, 38.5% met the strength training guidelines, and 34% met both aerobic and strength training guidelines. 7 According to the 2020 CDC National Health Interview Survey, 24.2% of U.S. adults met both aerobic and strength training guidelines. 30 This suggests our medical student sample is more physically active than similar-aged adults among the general population.
Our findings show that meeting only the aerobic or strength training guidelines did not significantly affect the outcome variables, when compared to students who met neither CDC guidelines. However, meeting both CDC aerobic and strength exercise guidelines was associated with a higher quality of life in our medical student sample. This is consistent with a prior study that found that quality of life was higher among medical students who met CDC recommendations. 7 We also found that meeting both CDC aerobic and strength exercise guidelines was associated with lower stress levels. This supports prior research showing that self-care activities like physical activity weaken the link between perceived stress and quality of life in medical students. 31 These results provide further support for the notion that engaging in exercise is essential for medical students’ wellbeing.
Meeting both CDC aerobic and strength exercise guidelines was associated with a higher level of social support provided by friends. This result suggests that the importance of social support in promoting exercise among medical students should not be underestimated. Other studies have found that medical students who engage in group exercise report a higher quality of life.8,21 Specifically, team-based exercise has been stated to lead to physical activity participation due to a greater sense of accountability. 8 Thus, encouragement from peers plays a role in fostering consistent exercise habits among students and promoting overall wellbeing.
Interestingly, we found that partaking in individual exercise (compared to group exercise) was associated with lower stress and burnout scores, and higher quality of life in our student sample. However, a greater proportion of students in our study participated in individual exercise (n = 63) compared to group exercise (n = 19). Several previous studies have found a link between exercise and burnout, with research identifying exercise as protective against burnout. 7 Studies have also identified a dose response effect between exercise and burnout and quality of life with higher intensities and frequency of exercise maximizing this benefit. 11 In our sample, students who engaged in group exercise were significantly less likely to meet CDC strength guidelines and combined aerobic and strength guidelines compared with those who exercised individually, while meeting aerobic guidelines alone did not differ between groups. This pattern suggests that many group-based activities may emphasize aerobic components but may not consistently provide sufficient strength training to meet full guideline recommendations. Although group exercisers reported greater friend support, these findings indicate that higher social support does not necessarily translate into meeting the full range of physical activity recommendations. Thus, the more favorable outcomes observed among students who exercised individually may reflect greater adherence to recommended exercise types and intensities, rather than group differences being driven only by sample size.
Thus, it is possible that the benefits seen in the individual exercise group were influenced by the larger sample size or by a higher intensity and frequency of exercise in that group.
While we observed improvements in stress and quality of life, meeting both CDC aerobic and strength training guidelines was not associated with a statistically significant decrease in burnout or levels of sleepiness in our sample. To our knowledge, this is the first study using a non-proprietary, single-item tool to measure burnout in the medical student population. We chose this tool as it was shown to be reliable in measuring burnout in healthcare providers compared to a validated single-item standalone burnout measure from the MBI Emotional Exhaustion subscale. 19 However, other studies have more commonly used variations of the Maslach Burnout Inventory (MBI) to assess burnout in medical students. We acknowledge that the MBI remains the most widely validated instrument for assessing burnout. Future studies using the MBI could provide additional insight into the specific components of burnout—emotional exhaustion, depersonalization, and reduced personal accomplishment—that may not be fully captured by a single-item measure.
The most common barriers to exercise reported among students included lack of time (86.59%), fatigue (69.51%), and lack of motivation (43.9%). Only a minority of students identified physical health (9.8%) or other reasons (7.3%) as limiting factors. These findings suggest that the primary obstacles to physical activity in this student population are largely modifiable and reflect the demanding and emotionally taxing nature of medical school. Addressing time management, energy balance, and mental wellbeing may therefore be key strategies in promoting exercise engagement among medical students. Medical schools, residency training programs, and hospitals may consider having on-site, accessible fitness options and promoting physical activity as a burnout prevention tool so that healthcare students and professionals can use exercise to their mental health benefit.
Our study’s findings provide a more in-depth perspective into the benefits of exercise for medical students. Our findings suggest that exercise benefits both quality of life and can help reduce stress. We’ve also expanded the current base of research by identifying the unique benefits of combined aerobic and strength training and by examining the unique benefits of group vs individual exercise. Ultimately, adequate sleep, lower stress levels, and high levels of social support are factors that are associated with combating burnout and promoting resiliency in the medical student population. 1 Exercise may therefore be of significant value in helping students address the unique set of challenges they face and promote overall medical student wellbeing. Establishing healthy exercise habits not only offers individual benefits to the medical student but also has the potential to influence medical students’ future patients. A physician’s personal exercise habits and attitudes towards prevention directly influence their likelihood of counseling patients on physical activity, highlighting the importance of promoting self-care among medical trainees.
There are several limitations of this study including a relatively simple sample size, especially with lower numbers in years MS-3 and MS-4. We administered the survey at the beginning of the academic year, and the majority of students who completed the survey were first-year medical students. The timing of data collection may not have provided an accurate gauge of more usual levels of burnout experienced among medical students as the academic year progresses. Future research may therefore look to assess levels of burnout at different time points of the academic year, especially at times where burnout is likely to be heightened, such as around medical licensing exams. We also believe obtaining a larger sample size would be useful in examining if burnout varies by class year, or from pre-clinical to clinical students. In sum, our findings add to the compelling body of research highlighting the power of physical activity as a wellness tool to improve various aspects of psychological health and quality of life for the future physician workforce.
Consent to Participate
Per the approved IRB protocol, the explanation of research was provided in the emails to students containing the survey link. Participation in this study was voluntary. Students were free to withdraw their consent and discontinue participation in this study at any time without prejudice or penalty.
Footnotes
Author Contributions
RB led the project and assisted with study conception, survey tool development and administration, interpretation of study findings and writing of the manuscript. DS assisted with study conception, survey tool development, and writing of the manuscript. MV assisted with study conception, data curation and analysis and writing of the manuscript. AB assisted with study conception and reviewed and approved the manuscript. KD oversaw the project progress, provided supervision, and reviewed and approved the manuscript. XZ led the statistical analysis and wrote the results section of manuscript. All authors approved the submitted version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
The study was approved by the University of Central Florida Institutional Review Board and determined to be human subjects research that is exempt from regulation. IRB ID: STUDY00006920