
Abstract
Physical, mental, and emotional wellness are just some avenues to maintain a person’s overall well-being. These components of wellness influence each other; mental wellness is known to be affected by physical wellness. Physical wellness in the form of regular exercise stands as a method to mitigate the high rates of depression and burnout among medical students. This study examines the levels of physical activity among preclinical and clinical medical students. This is an observational, non-randomized study with data collection over one month. Fifty-nine percent of students surveyed met the CDC recommendation for exercise. The major reason to exercise was to improve mental health, with 37% of respondents citing this as a motivator. For those who did not meet the physical activity recommendation, lack of time was cited in 75% of respondents. Greater knowledge of prevention methods, risk factors, and outcomes of chronic health conditions may contribute to higher physical activity levels among medical students compared to the general population. Emphasizing exercise and physical wellness campaigns may be a solution for medical schools to improve the overall wellness of their students.
“In our study, the major reason to exercise was to improve mental health, with 37% of respondents citing this as a motivator.”
Introduction
Physical wellness is well-known to affect mental wellness. 1 It is known that the release of endorphins after a workout can provide a source of temporary but necessary relief for those suffering from depression. 2 Based on these reports, regular exercise stands as a major avenue through which depression and burnout among medical students can be mitigated. 3 Medical students spend many hours of the day sedentary as they study. 4 Furthermore, many medical students may rationalize skipping a workout in order to gain more study time. Though missing a workout may be necessary at times, it can easily develop into habit, leading to a lack of exercise for weeks, or potentially months to years. 5 As reviewed in Comprehensive Physiology, lack of physical activity and prolonged sitting time are associated with an increased risk of mortality and chronic illnesses, including heart disease, type 2 diabetes, several cancers, obesity, and depression. 6 Identifying the specific factors that contribute to inactivity at the University of Toledo College of Medicine and Life Sciences (UTCOMLS) is vital to creating a solution to this prevalent problem. By tracking student levels of physical activity across all years of medical school, novel insight may be gained and solutions specific to UTCOMLS may be ascertained.
The purpose of this study is to assess the levels of physical activity among preclinical and clinical medical students at UTCOMLS by examining achievement of the Center for Disease Control (CDC) recommendations for weekly exercise. The information collected from this study will allow the Office of Student Affairs to determine during which years in medical education medical students experience the least physical activity. These time points will be used to determine design of future programs to minimize medical student inactivity.
Methods
Population
The University of Toledo College of Medicine and Life Sciences, located on the University of Toledo Health Sciences Campus (UT-HSC), has approximately 700 students enrolled in four classes designated as preclinical (M1 and M2) and clinical (M3 and M4) levels. Preclinical students matriculate through in-class on-campus courses while clinical students participate in clinical rotations on-site at various health care facilities throughout northwest Ohio, southeast Michigan, and other approved practice sites. Clinical rotations vary in length from 5 to 10 weeks depending on the medical subspecialties. This study was carried out in accordance with the University of Toledo Institutional Review Board (IRB), and assigned the study number 300988-UT. All participants provided written informed consent.
Study Aim/Research Design
The current study sought to examine the levels of physical activity among preclinical and clinical medical students. This study stratified physical activity level by examining achievement of the CDC recommendations for weekly exercise. 6 These guidelines state that for substantial health benefits, adults should do at least 150 minutes of moderate-intensity aerobic physical activity per week, or at least 75 minutes of vigorous-intensity physical activity per week. In addition to aerobic activities, 2 or more days per week of moderate or greater intensity muscle-strengthening activities that involve all major muscle groups is recommended.
The Physical Activity Study was an observational, non-randomized survey study conducted from August 16, 2021, through September 9, 2021, administered through the Office of Student Affairs (OSA). The anonymous survey was distributed via email to all medical students currently enrolled at the University of Toledo College of Medicine and Life Sciences. The survey was limited to this population so that we could ascertain results that would be specific to improving wellness at our university and potentially help in planning interventions to improve physical activity here at UTCOMLS. There was no selection strategy, and everyone interested in completing the survey was allowed to do so. The survey did not contain any information that could reveal the respondents’ identity (e.g., name, address, etc.). Participants were asked to provide their age but not their date of birth.
Survey Data
Consent was obtained from all respondents per the UT-HSC IRB regulations. The survey was anonymous, and respondents’ demographic data was limited to age, sex, race/ethnicity, current status (grade level), height and weight (BMI was calculated), relationship status (single, married, or in a relationship), children, and living status (alone, with roommates, or family). Responses to questions were coded and mutually exclusive using a modified Likert scale, and, when asking about agreement with a statement (strongly agree, agree, disagree, or strongly disagree), a response option neutral (“no opinion”) was provided. For questions relating to exercise (motivations, limitations, type, etc.), forced response options were provided to limit open-ended responses. Open-ended questions were allowed where appropriate (e.g., the number of days per week they exercised). For some questions, respondents were asked whether they agree or not and to evaluate the importance of each option. Responses to survey questions were summarized and expressed as proportions. Descriptive analysis summarized the respondents’ achievement of the CDC recommendations by the level of weekly exercise and whether this was associated with the change in activity level since entering medical school. Bivariate analysis was employed to evaluate survey responses with regard to demographic characteristics in order to look for differences or patterns in responses. In addition, we sought to address the following questions: is there a difference between class level (M1 through M4) or clinical level for the satisfaction with activity level; the effect of educational or extracurricular hours spent per week; are the reasons for exercise related to the type of exercise activity; what is the effect of technology trackers (exercise or food intake); and the role of scheduling exercise time in achieving the CDC recommendations.
Statistical Analysis
Continuous data were tested for normality using Shapiro–Wilk goodness of fit test and are presented as mean ± standard deviation (SD) of the untransformed or log-transformed version or, if neither were normally distributed, as median with interquartile range (IQR). The continuous variables of age, weight, BMI, and height were not normally distributed by the Shapiro–Wilk goodness of fit test even after log transformation. All transformed variables except height were greater than 1 indicating moderate skewness; height was negatively highly skewed. Non-parametric tests were performed for these variables, while all other analyses used parametric tests. Comparisons of continuous data were evaluated depending on the level of comparison using two-sample t-tests or Wilcoxon rank sum test for 2 groups, or one- or two-way ANOVA or Kruskal–Wallis for more than 2 groups. Categorical variables are expressed as counts and chi-square test or, if the frequency of counts was low (≤5), Fisher exact test was used to compare groups. Multinomial logistic regression analysis was used to identify factors associated with the achievement of CDC recommendations for weekly exercise. Firth logistic regression analysis was performed to determine if the self-reported changes in activity level since enrolling in medical school was predictive of the reasons for pursuing physical activity (e.g., improve physical health). The models were tested for interaction and found to be non-significant. All analyses were performed using R Software (version 3.4.2) and SAS JMP (version 15.2). Statistical significance was considered to be P < .05.
Multivariable Models
We sought to identify respondents’ characteristics associated with the achievement of CDC recommendations for weekly exercise (see above). Composite models comprising demographics and select survey questions were developed. Factors included were: reasons for not exercising; hours per week in school and/or extracurricular activity; type of extracurricular activity; amount of exercise per week (days); type of exercise; and living arrangement. Factor selection was guided by significant uni- or multi-variate results from the comparison of class level and/or clinical status. Multi-variate models were constructed using stepwise regression with statistical significance at P < .05.
Results
Characteristics of Participants in the Medical Student Physical Wellness Survey.
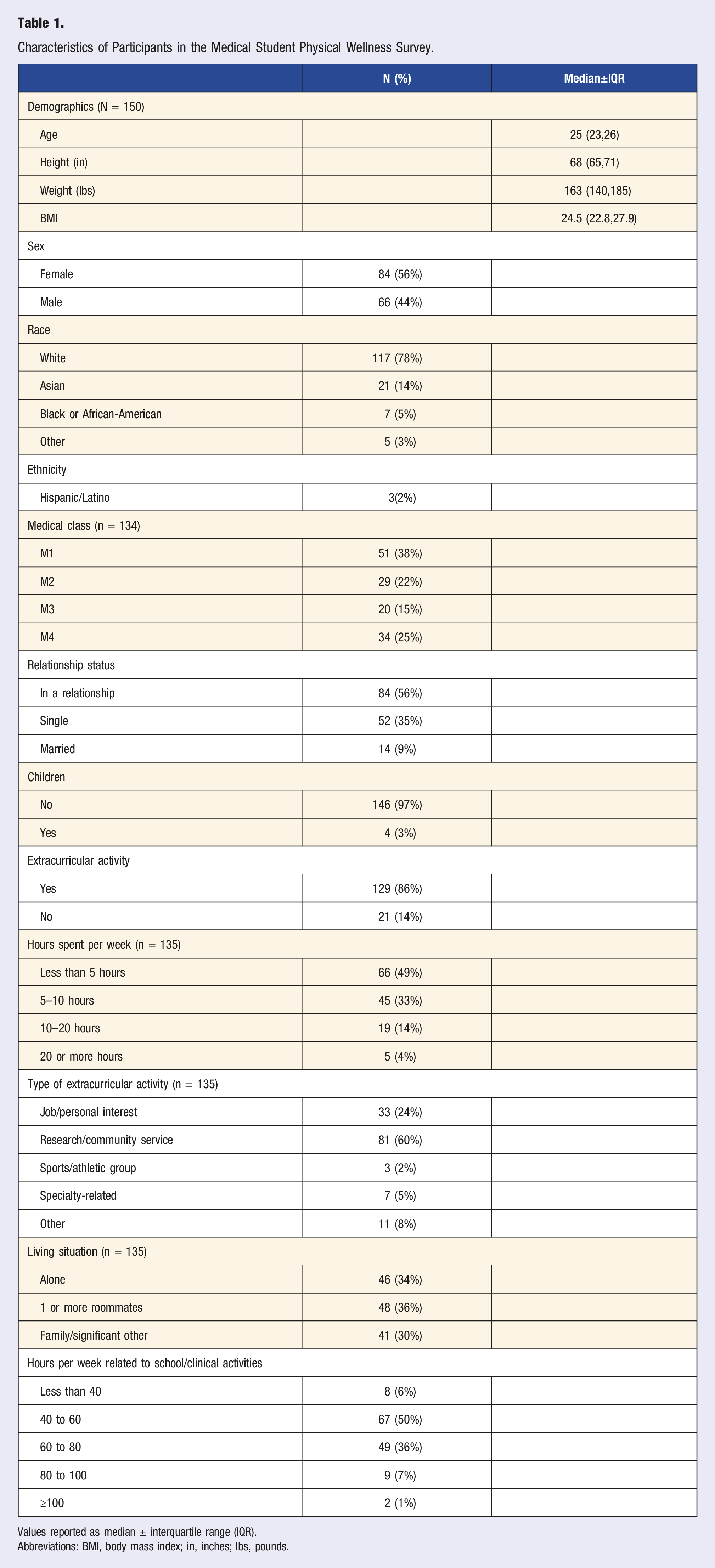
Values reported as median ± interquartile range (IQR).
Abbreviations: BMI, body mass index; in, inches; lbs, pounds.
CDC Physical Activity Guidelines
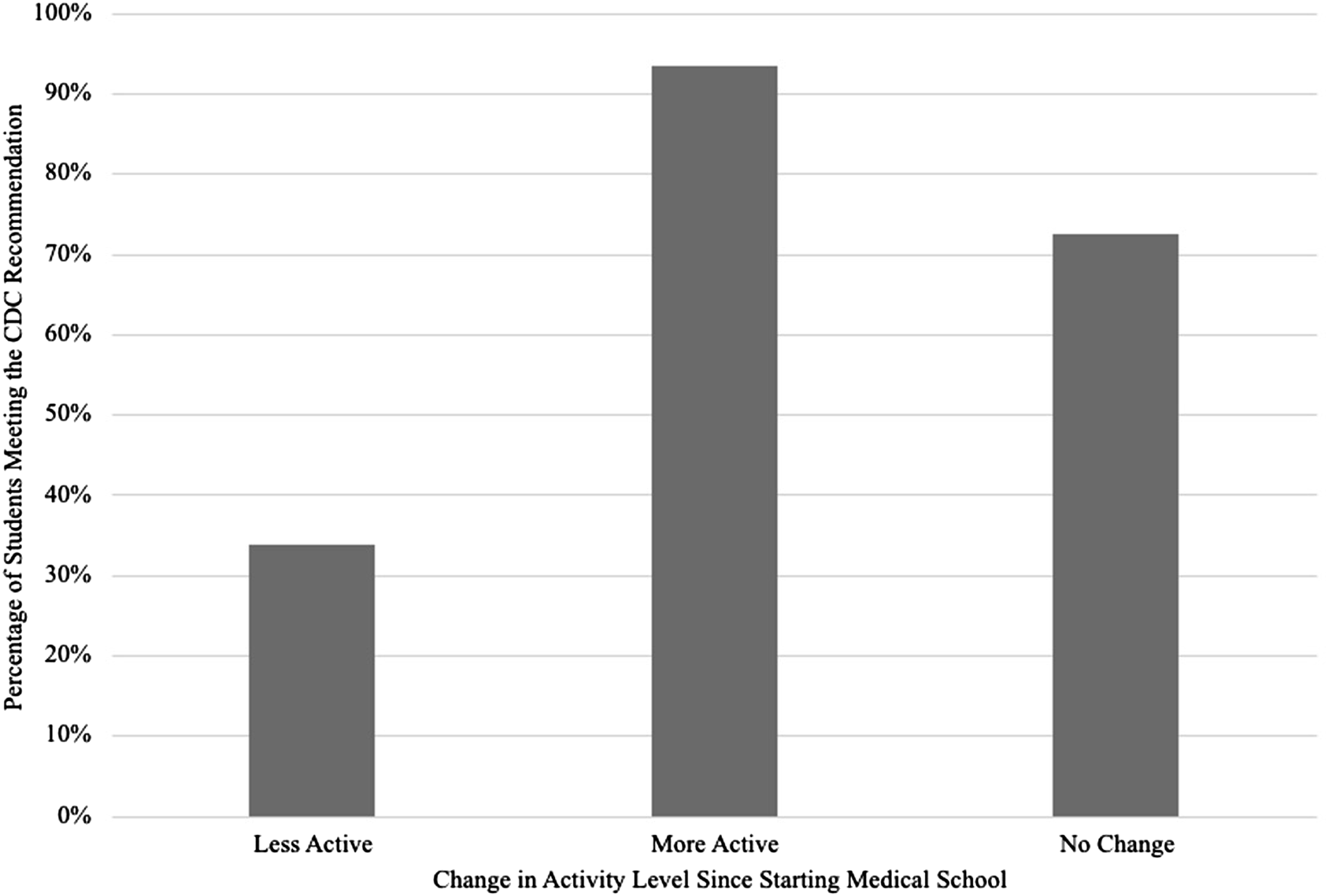
When asked questions pertaining to the Physical Activity Guidelines for Americans, 137 students responded to at least one question. Most students (59%) indicated that they met the weekly activity goals. The type of exercise by motivation to exercise (P = .89) is shown in Figure 1. One factor that significantly affected whether a student met the guideline’s goals was change in activity level since starting medical school (Figure 2, P < .001). Sixty-five respondents reported less activity, with 66% of those not meeting the recommendations. Of the 30 students who reported an increase in activity, 93% met the recommendations. Additional factors that predict achievement of the CDC recommendations include days of exercise per week (P < .001) and scheduling exercise time (P < .001) (Table 3). Types of exercise by reason to exercise among medical students. Percentage of medical students meeting the CDC recommendation for exercise by change in physical activity level since starting medical school.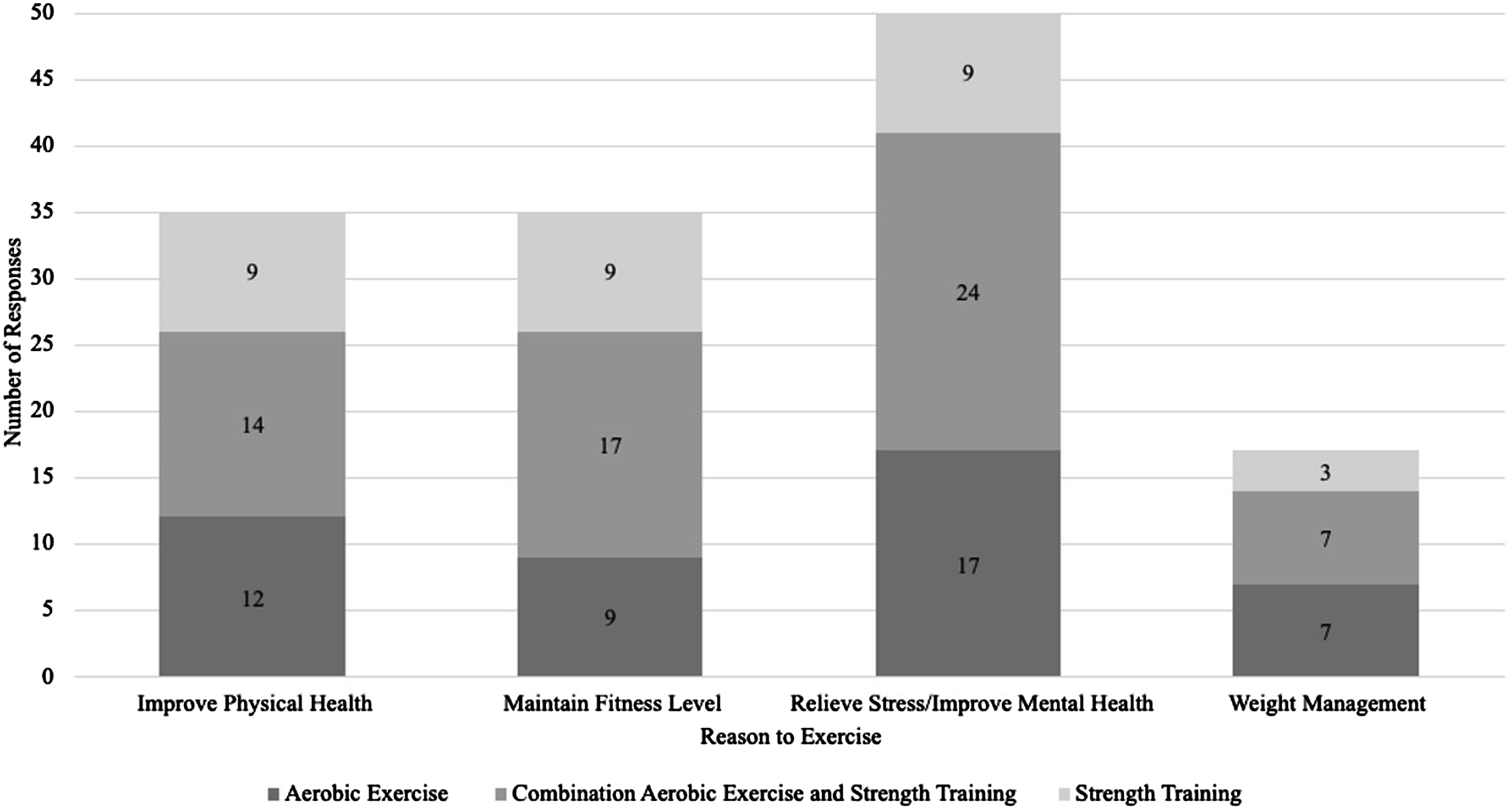
Class Level
As indicated above, the class level breakdown of respondents was 38% M1, 22% M2, 15% M3, and 34% M4; classification of classes is designated as preclinical (M1 and M2) and clinical (M3 and M4) levels. Eighty students are categorized as preclinical and 54 students as clinical. Comparison of the days of exercise per week between preclinical and clinical students was not significant. Additionally, there was not a significant difference between class level and meeting the CDC recommendations (P = .66, Figure 3). Comparisons of responses by medical school class are shown in Table 2. Percentage of medical students meeting the CDC recommendation for exercise by medical school class. Comparison of Physical Activity Levels, Lifestyle Characteristics, Barriers to Exercise, and Satisfaction Among Medical School Classes. Abbreviations: BMI, body mass index; in, inches; lbs, pounds; M1, first-year class; M2, second-year class; M3, third-year class; and M4, fourth-year class. Statistical significance at P < .05. aValues reported as median ± interquartile range (IQR).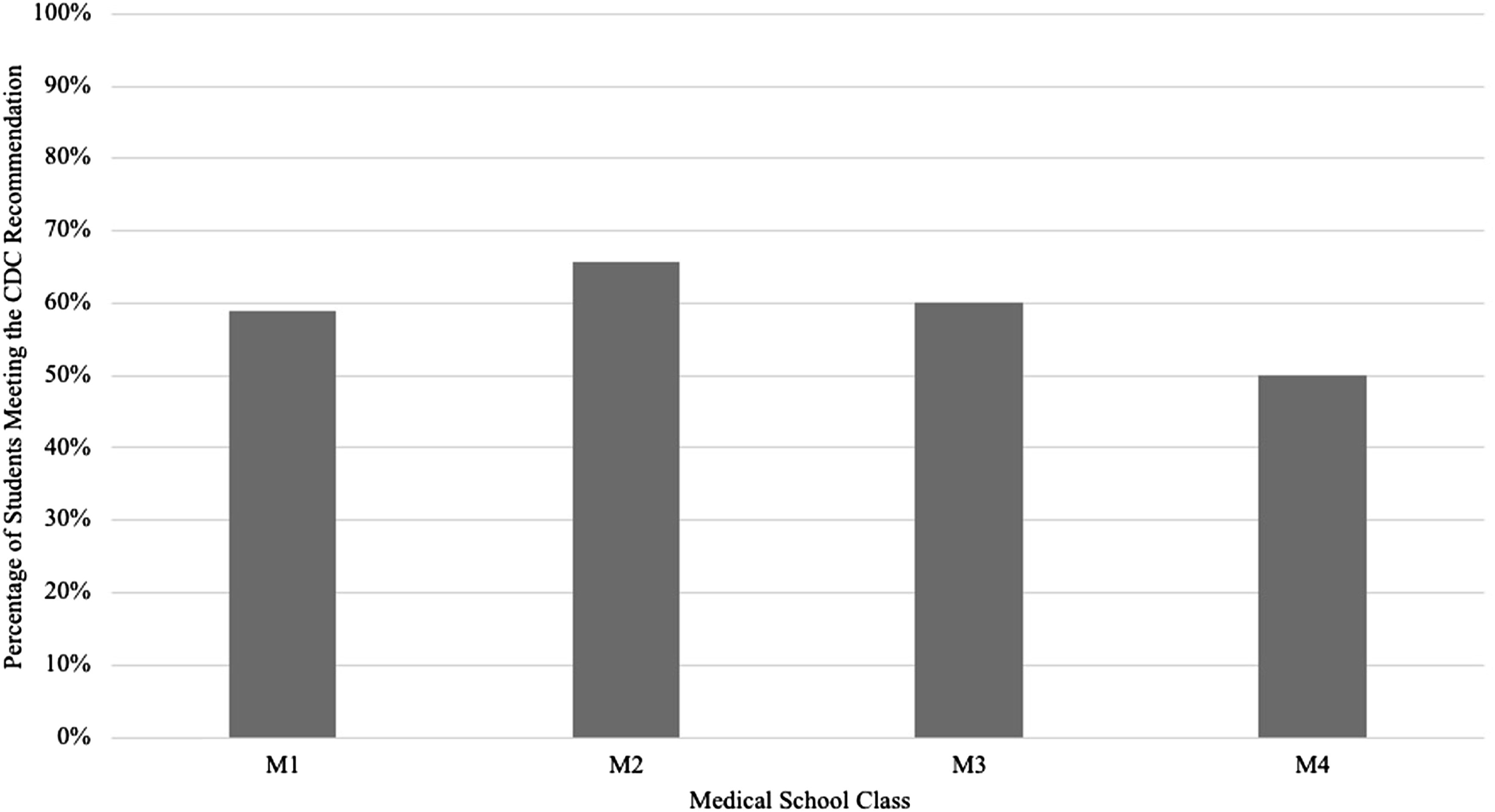
Exercise Type and Reason
Comparison of Physical Activity Levels, Lifestyle Characteristics, Barriers to Exercise, and Satisfaction in Those Who Achieved or Did Not Achieve the CDC Recommendation.

Abbreviations: BMI, body mass index; in, inches; lbs, pounds.
Statistical significance at P < .05.
Values reported as median ± interquartile range (IQR).
Educational and Extracurricular Hours
Of all the respondents, only 5% were not involved in extracurricular activities. Of those who were involved in extracurricular activities, 49% spent 5 hours or less per week on them. When responding to time spent for school/clinical activities, 49% of students reported spending between 40 and 60 hours per week. Extracurricular hours had no significance on meeting the CDC threshold, while hours spent on school/clinical activities was significant (P = .23 and P = .03, respectively, Table 3).
Scheduling Exercise
According to the survey responses, 57% of responding students scheduled exercise time regularly. Twenty-eight percent of students scheduled exercise sometimes, and the remaining 15% did not schedule exercise time. Those who scheduled exercise time were significantly more likely to achieve the CDC recommendations (P < .001, Table 3).
Tracking Technology
Use of technology to track physical activity or food intake did not significantly affect a respondent’s likelihood of meeting the CDC recommendation (P = .10 and P = .08, respectively, Table 3). Of the respondents, 66% used technology to track physical activity, and 26% used technology to track food intake.
Discussion
The present study showed several results that may warrant intervention among medical schools to improve physical activity among medical students. Overall, 59% of students surveyed met the CDC recommendation for exercise based on the Physical Activity Guidelines for America through the Department of Health and Human Services. 7 These guidelines state that for substantial health benefits, adults should do at least 150 minutes of moderate-intensity aerobic physical activity per week, or at least 75 minutes of vigorous-intensity physical activity per week. In addition to aerobic activities, 2 or more days per week of moderate or greater intensity muscle-strengthening activities that involve all major muscle groups are recommended.
We found no significant difference between medical school class level and meeting the CDC recommendation. This may be due to varying commitments throughout medical education, with preclinical students completing required courses and additional study time, and clinical students completing required rotations with additional study time for NBME subject examinations as well. Regardless of medical school class, students experience time commitments that influence their ability to exercise.
According to the Physical Activity Guidelines for America, between 2008–2016, only 26% of men, 19% of women, and 20% of adolescents reported sufficient activity to meet the aerobic and muscle-strengthening guidelines. In our survey, 51% of women and 67% of men met these guidelines. Greater health knowledge, including prevention methods, risk factors, treatment protocols, and outcomes, may contribute to the stark contrast in physical activity level among medical students compared to the general population.
Though most students in our survey met the CDC recommendation for physical activity, there were 41% of students who did not. For those who did not, not enough time was cited 75% of the time as the reason for not exercising. Additional free time and flexible scheduling means more opportunities for self-care, including physical and mental wellness. The Accreditation Council for Graduate Medical Education (ACGME) standards restrict residency hours to an 80-hour weekly limit, averaged over 4 weeks, to protect against the negative effects of sleep loss and to allow for adequate time for patient hand-off. 8 Interestingly, unlike the ACGME, the Liaison Committee on Medical Education (LCME) does not have a mandate on medical student work hours. 9 To portray support for medical student wellness, the LCME could adopt a similar approach, restricting class time to a reasonable amount of hours per week and encouraging students to balance their extracurriculars with personal wellness.
In our study, the major reason to exercise was to improve mental health, with 37% of respondents citing this as a motivator. Improvement in mental and physical wellness among medical students and residents has been a long-time battle for medical students and residency programs. In 2017, the ACGME revised its program requirements to better address wellness. 10 The ACGME stated that “psychological, emotional, and physical well-being are critical in the development of the competent, caring, and resilient physician.” Exercise has been shown to improve all three of these aspects of wellness. If medical schools aim to improve both mental and physical health of their students, encouraging exercise through physical wellness campaigns may be a reasonable solution.
The University of Toledo College of Medicine and Life Sciences implemented the Fit for Health Program in the fall of 2020. This is an incentivized physical activity program where students are entered into a monthly raffle if they meet the U.S. physical activity guidelines of at least 3 days of activity totaling a minimum of 150 minutes of exercise each week. Raffle winners receive prizes like gift cards to Amazon and/or Chipotle. This program is run through a fitness application where membership is free, and activity is monitored. Students benefit from seeing other students’ activity, encouraging each other by commenting on completed workouts on the main feed of the application, and gaining motivation through the possibility of winning the raffle each month. As medical schools and residencies continue to emphasize comprehensive wellness, incentivized physical activity programs may be a viable strategy to mitigate the pervasive burnout amongst medical students and residents.
Conclusion
In our examination of physical activity levels of medical students at the University of Toledo College of Medicine, we found that forty-three percent of respondents reported less physical activity since beginning medical school, while 20% reported an increase in activity. Overall, a majority of students met the CDC recommendation for exercise. For those who did not meet this recommendation, not enough time was cited 75% of the time as the reason for not exercising. Additional free time and flexible scheduling means more opportunities for self-care, including physical and mental wellness. We recognize, however, that our conclusion is not generalizable given this data was collected from a singular university.
Limitations
Limitations to this study include a small sample size, modest response rate, absence of valid questionnaire, lack of power calculation analysis for determining sample size, imbalance of preclinical and clinical students, and lack of generalizability. We administered the survey only to students at the University of Toledo College of Medicine, so our conclusion is only relevant to this institution specifically and thus is this not able to be generalized. The survey was sent out to all medical students at UTCOMLS for a total of 709 recipients. We received 150 responses for a response rate of 21%. As previously stated, we did not conduct a power analysis for this study to determine the appropriate minimum sample size. Most of our respondents were preclinical students, which could alter our results when comparing preclinical and clinical students. Additionally, it is possible that those who felt most strongly about exercising responded to this survey, also skewing the results but towards more active respondents. Given the self-reported nature of this study and absence of valid questionnaire, we also recognize the possibility of response bias in our survey.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.