
Abstract
Background
Despite the documented success of medical-legal partnerships (MLPs), there is a dearth of robust experimental-based research on their efficacy. This review synthesizes the findings of MLP interventions and identifies opportunities for MLP expansion in vulnerable communities.
Methods
Articles were eligible if they tested the experimental effects of an MLP intervention on health-harming legal needs (HHLNs) and had full text for review. Two reviewers independently screened articles for inclusion and assessed the quality (risk of bias) of each study.
Results
Seven studies were eligible. Populations were largely women, of color, and of lower socioeconomic status. All studies demonstrated positive effects on primary endpoints including stress, diabetes, and immunization. Two studies were randomized controlled trials; each presenting with low risk of bias.
Conclusion
Studies highlighted the transdisciplinary impact of MLPs. However, additional research on efficacy is needed given the small number of studies in review.
Keywords
“Our findings indicate that MLP interventions, whether quasi-experimental or randomized, were largely efficacious in addressing HHLNs.”
Introduction
A population’s health is strongly influenced by determinants such as income, wealth, educational level, race and ethnicity, employment status, and social-environmental drivers.1-3 Communities of color and of lower socioeconomic status face barriers to achieving optimal health because of the uneven distribution of resources and investments1-3 and, without timely intervention, experience disproportionately poorer health outcomes.4-7 The majority of low-income individuals experience 2 to 3 adverse social needs. 7 Inequitable access and unaffordability of quality health and legal services only compound and perpetuate hardships within these communities. 7 Failure to address these needs further widens health outcome disparities for vulnerable communities, particularly, low-income minority (Black, Indigenous, Hispanic) populations who fare the worst against other U.S. groups. 8 Thus, traditional clinical care must increase its reliance on transdisciplinary, patient-centered, preventative strategies to reduce inequities and improve health in at-risk populations.9,10 One innovative model is Medical-Legal Partnerships (MLPs), a collaborative approach that integrates legal aid into clinical settings to target health-harming legal needs (HHLNs) such as food insecurity, unsafe housing conditions, government benefits denial, immigration, guardianship, and HIV/AIDS.11,12 To date, over 300 MLP programs have been instituted across the United States (U.S.),13,14 and low-income, minority children who are most likely to suffer from the lifelong impact of HHLNs (injuries, environmental exposure to mold and asbestos, and sickness) may benefit the most from this innovation. 15
While numerous programs have underscored MLPs’ importance in addressing HHLNs, research examining their causal pathways of effectiveness remains limited. Therefore, our primary goal was to systematically review and evaluate experimental MLP studies to assess their impact in reducing HHLNs, and to identify opportunities for future research and programmatic expansion.
Methods
For this review, we focused our search on experimental designs, including randomized controlled trials and quasi-experimental designs (including pre-post studies). In addition, studies must have been published in a peer-reviewed journal, have the full text for review, and address our population and primary research goal. For the purposes of this review, an MLP intervention was defined as a formal collaboration between legal professionals and healthcare teams, embedded within a healthcare setting where legal services were integrated into patient care to address one or more health-harming legal needs (e.g., housing insecurity, denial of public benefits, family law issues). 16 Eligible studies required that patients either received direct legal assistance or were referred to legal partners through a structured process as part of the clinical encounter. No restrictions were placed on publication year, place of publication, or population. Articles were screened and deemed ineligible if they had primary outcomes outside our scope of interest, were published in a language other than English, or were systematic reviews, gray literature, book reviews, editorials, policy papers, or any other designs that discussed MLP uptake without presentation of data for pre- and post-evaluation.
Between January and April 2022, the first author, JCJ, completed a search across Ovid MEDLINE, PubMed, Google Scholar, and Westlaw and LexisNexis to identify articles using a combination of terminology, including: MLP*, “medical-legal partnership,” “medical-legal,” “medical legal” (no hyphenation), pedi*, child*, adolesc*, clinic*, adult*, and parent*. Search terms were combined with Boolean phrases “AND,” “OR” to maximize search results. The full list of search terms can be found in Appendix One. Following completion of the search, all retrieved articles were uploaded into Rayyan QCRI: a web and mobile app for systematic reviews, to aid in screening, sorting, and final selection of articles. 17
The literature search was updated in August 2022, November 2023, and again in July 2025 to ensure inclusion of all relevant experimental and quasi-experimental MLP studies. For each search cycle, first author JCJ and co-author EZ, and later co-author OD (in 2025), independently screened article titles according to predefined inclusion criteria, reviewed abstracts for relevance, and identified studies for full-text review. Any discrepancies in study eligibility were discussed and resolved by consensus without the need for a third reviewer. The 2023 update yielded one new study (Liaw et al., 2023).
18
For the 2025 update, first author JCJ and co-author OD replicated the complete search strategy using the same databases, search terms, and eligibility criteria to identify new studies published between November 2023 and July 2025. Both authors independently screened the results and reached consensus on inclusion. No new eligible studies were identified during this period. As such, the total number of included articles and Figure 1 remained unchanged. PRISMA flow diagram of study identification, screening, and inclusion.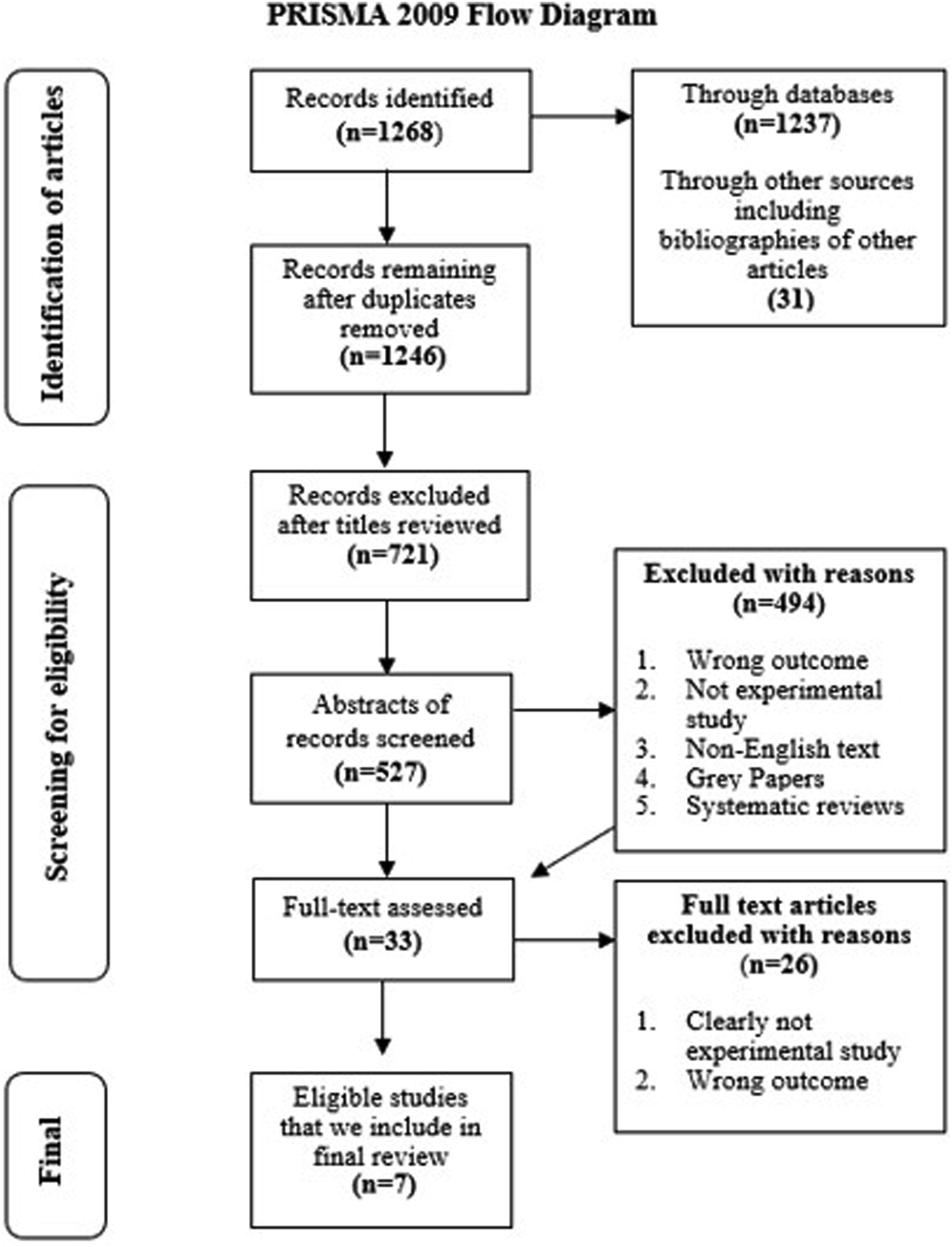
Characteristics of Experimental MLP Studies in Systematic Review.

Note. Intervention complexity and MLP integration varied across studies, ranging from MLP as the primary intervention to MLP as a supportive service integrated within a broader care model. This variation should be considered when interpreting study outcomes.
Notes on abbreviations: RCT: randomized controlled trial; IG: intervention group; CG: Control group; HHLN: health-harming legal needs; ED: emergency department; PSS: perceived stress scale; P: P-Value, PP: posterior probability (Bayesian statistics).
Risk of Bias Assessment Indicators for Medical-Legal Partnership Research Studies.
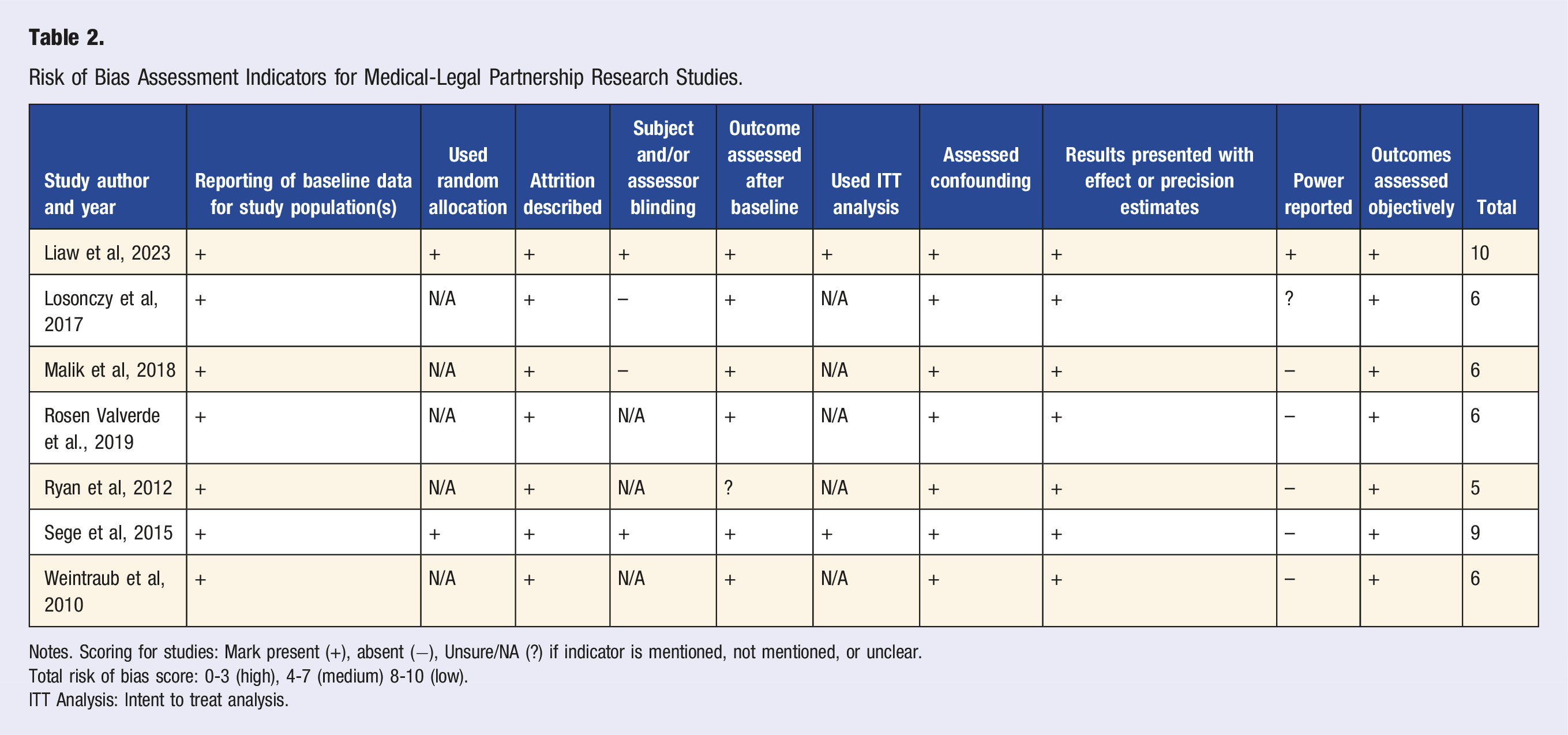
Notes. Scoring for studies: Mark present (+), absent (−), Unsure/NA (?) if indicator is mentioned, not mentioned, or unclear.
Total risk of bias score: 0-3 (high), 4-7 (medium) 8-10 (low).
ITT Analysis: Intent to treat analysis.
Results
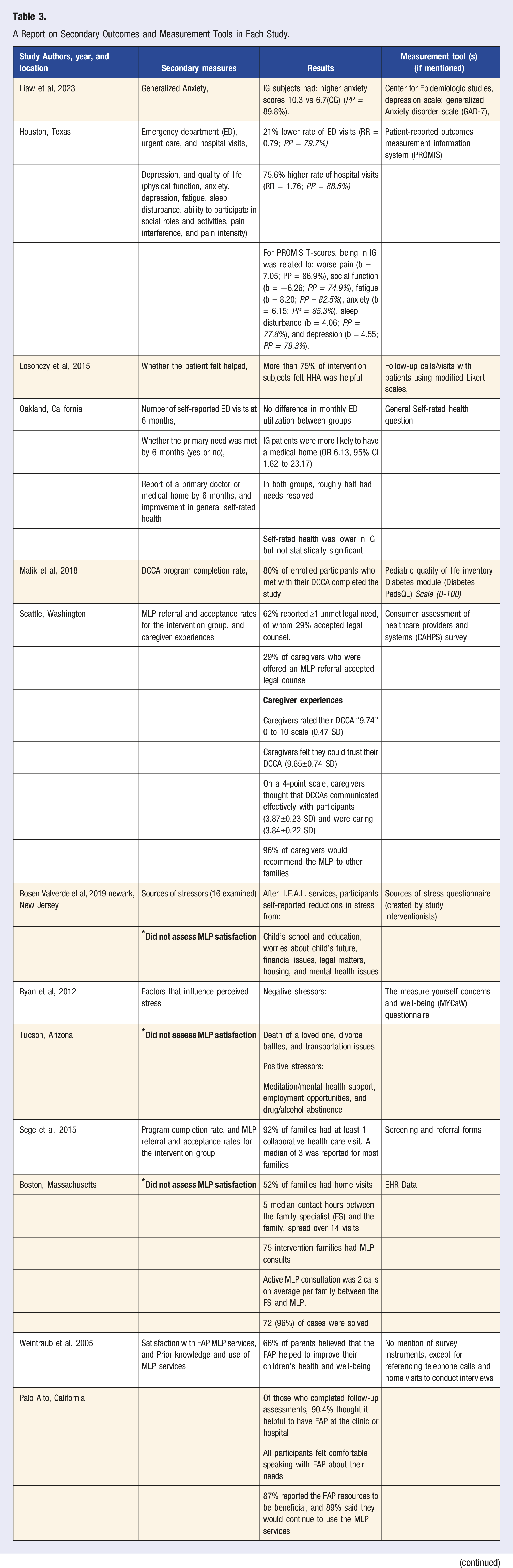
A Report on Secondary Outcomes and Measurement Tools in Each Study.
Characteristics of Included Studies
As shown in Table 1, all studies were conducted in the U.S.; all except for Weintraub et al were published within the past 10 years; all samples were predominantly female; and all had majority low-income populations. Across MLP populations with families, most caregivers were female.21-23 Regarding racial/ethnic makeup, four were majority Black.18,21,24,25 one was majority Hispanic, 22 and the last study, Ryan et al, was mainly Black and Hispanic at baseline but became a majority non-Hispanic White population at the study’s end. 26 Only Sege et al and Liaw et al were randomized controlled trials (RCTs).18,21 The remaining five were quasi-experimental, and of these, three were pre-post studies.22,25,26 Participants reported various HHLNs, chief of which were housing concerns,18,21,22,24,25 public benefits,22,25,26 unemployment and income assistance,18,21,24,26 and food insecurity.18,21,24-26
Risk of Bias Assessment Scores
Table 2 shows the risk of bias scores for all studies. Quality scores ranged from low to medium risk of bias. All studies with medium risk of bias scores were associated with the quasi-experimental study design, which inherently has a higher risk of bias due to the absence of random allocation, intent-to-treat analysis, blinding, and other bias-reduction indicators. Sege et al and Liaw et al presented the only low risk of bias scores. 21 We found that all studies reported results that included either effect or precision estimates. All studies also reported baseline measures and attrition, assessed for confounding, and measured one or more outcomes objectively. Six studies assessed outcome measures during a follow-up period,21-24,26 two studies used random allocation, 21 and two used intent-to-treat analysis. 21 Only one study reported the use of power estimates to determine sample size, 18 and only one reported subject/assessor blinding. 18
Summary of Evidence
The included MLPs reported different primary outcomes: (1) to examine changes in perceived stress levels,25,26 (2) to broaden improvements in patients’ identified social needs,21,24 (3) to support youth at high risk for diabetes, 23 and (4) to increase uptake of family social services and improvements in newborns’ health.21,22 Intervention approaches featured various touchpoints, including (1) biweekly contacts with patients through a resource desk, 24 home visits,21,23 phone calls from health and social workers,18,21,23 and in-person sessions with a family specialist (FS) who was trained to support families with infant care needs. 21 Of the four studies with control groups, three provided usual clinical care as their control,21,24,27 while one provided a 6-month waitlist control. 18
Given that the RCT study design is considered research’s gold standard, we discuss the findings of the Sege et al and Liaw et al articles in greater detail. In Sege et al, the authors examined whether the inclusion of a trained FS would better support families with newborns (average age: 10 weeks old) and improve the quality of care. 21 The study, which lasted six months, included clinical visits with the physician and FS, home visits, and ongoing follow-up calls and emails with the FS to ensure that infants completed immunization and preventive care visits. 21 If a case required legal intervention, it was referred by the FS to the MLP Boston case management team to achieve resolution. 21 Compared to the control group, infants in the intervention group were more likely to complete immunization schedules at sixth and eighth months (P ≤ 0.01), more likely to have five or more primary care visits by year one (P ≤ 0.01), and less likely to visit the emergency department compared with the control group (P ≤ 0.03). 21 Additionally, the DULCE intervention worked with the Boston MLP to address food, housing, income, and utility needs across 75 intervention families. Active MLP consultation between the FS and MLP involved 2.3 calls per family, of which most cases were resolved without further legal remediation. 21 In Liaw et al, the authors evaluated whether MLP improved mental health, healthcare use, and quality of life compared to a 6-month waitlist control group. The study relied on social workers to help intervention participants get referral support for issues such as wills and guardianship, housing, security, employment and education, insurance, food, and income. 18 The authors found mixed results regarding intervention efficacy. Compared to the waitlist group, the immediate intervention group had lower perceived stress scores (PSS) 18.8 vs 19.9 in the control group (PP = 74.8%), but higher anxiety scores 10.3 vs 6.7 (CG) (PP = 89.8%). 18 Additionally, the intervention group had 75.6% higher rate of hospital visits (RR = 1.76; PP = 88.5%) but 21% lower rate of emergency department (ED) visits (RR = 0.79; PP = 79.7%). 18
Discussion
To the best of our knowledge, this systematic review is the first to specifically focus on the impact of experimental MLP research and to explore possible opportunities for expansion in pediatric and adult populations. In this review, we defined an MLP intervention as a structured collaboration between legal professionals and healthcare teams to address HHLNs that emerge during clinical care. To be included, studies had to involve direct legal assistance or a facilitated referral to legal partners as part of the healthcare encounter, distinguishing them from interventions limited to legal information, policy advocacy, or general resource provision. Our focus on experimental and quasi-experimental designs was intentional to strengthen causal inference regarding the effects of MLP interventions on HHLN outcomes. While this approach excluded high-quality retrospective cohort studies, such as Beck et al (2022), 28 which remain influential in documenting MLP’s effectiveness in real-world settings, it allowed us to apply a distinct methodological lens that is underutilized in MLP research. This scope offers unique insights into causal impact but also highlights the need to integrate evidence from diverse study designs to build a more comprehensive evidence base that can advance research and inform policy and practice. Our findings indicate that MLP interventions, whether quasi-experimental or randomized, were largely effictive in addressing HHLNs. However, the limited number of only seven eligible studies strongly underscores the scarcity of causal evidence regarding the role of MLPs in addressing HHLNs. This emphasizes the immediate and ongoing need for robust and comprehensive research to enrich our scientific understanding of novel, transdisciplinary interventions, particularly those such as MLPs, which aim to improve the quality of life in vulnerable, underserved populations. Conducting experimental research in MLP settings presents unique methodological and ethical challenges that help explain the limited number of studies identified in this review. Ethically, withholding legal assistance from a control group can be problematic when such services address urgent needs like eviction prevention, access to food benefits, or child custody disputes. Methodologically, recruitment and retention can be difficult because many patients seeking legal assistance face unstable housing, fluctuating contact information, or competing priorities that hinder participation in follow-up assessments. Small sample sizes, often tied to the relatively low volume of eligible cases within a given clinic, limit statistical power. In addition, funding for rigorous study designs like experimental research in MLP remains limited, and substantial contextual variability across clinical sites, patient populations, and local legal infrastructures complicates the development of standardized protocols. To address these challenges, future studies might employ designs better suited to applied healthcare settings, such as stepped-wedge trials, pragmatic clinical trials, or hybrid effectiveness-implementation studies. Clearer guidance is also needed on ethically appropriate control conditions for interventions that provide essential services, to ensure that the pursuit of causal evidence does not come at the expense of patient well-being.
All seven studies documented measurable improvement between baseline and follow-up time points for diverse outcomes of interest, including the reduction of perceived stress,18,25,26 emergency department visits,18,21,24 A1C, 23 and inversely, improvements in childhood immunization rates and enhancements in food and housing insecurity outcomes.21,22 As shown in Table 1, there was considerable heterogeneity in the MLP approaches, which makes direct comparison difficult. The included studies differed in design, intervention complexity, and the degree to which MLP services were a central component vs a supportive element of a broader intervention. This heterogeneity reflects the diversity of MLP models and the realities of adapting them to local needs, resources, and implementation contexts. While this adaptability is a core strength of MLPs, it also limits the ability to draw strong conclusions about the effects of MLP services in isolation from other program components. This variability included the diverse integration of social workers, specialists, therapists, and community health workers to assist patients in successfully navigating the MLP referral and completion process. Support was also channeled through different approaches, including phone calls, in-person home visits, and through help desk resources. However, despite the different ways in which MLP interventions were adapted and channeled to study populations’ needs, a common thread across studies was the need for multiple and frequent touchpoints to support and connect patients throughout the warm handoff process. This review beneficially highlights a myriad of MLP approaches, which ought to be considered when designing interventions and real-world programs that align with patients’ needs and preferences.
Regarding racial and ethnic makeup, most of the studies’ populations were composed of Black and Hispanic participants. Socioeconomically, MLP programs were targeted at participants from low-income households, a demographic that also largely received governmental assistance for income and nutritional support. Furthermore, many of the studies’ populations were from households headed by single women. In addition, most participants across the seven studies presented numerous HHLNs; the most pressing and commonly mentioned needs included food and housing insecurity, unemployment, and government benefits. These findings align with results from both observational and experimental studies, which demonstrate an accumulation of adverse health needs within racial-minority, low-income populations.5,28-36 Yet, despite the strong need for MLPs, most of our studies experienced a significant loss in follow-up among Black and Hispanic participants.25,26 Researchers who work with vulnerable populations are largely attuned to the unique circumstances and concerns experienced by these communities.36-40 These include the inability to schedule time off work, affordability, socioeconomic vulnerabilities impeding access (e.g., transient population/frequently moving, lack of support, cultural and language barriers), and overall mistrust in the medical and legal communities.36-40 These various factors harm study retention, which in turn (1) hinders external validity to populations who would strongly benefit from MLPs; (2) impedes replication in larger-scale studies that have the potential for greater dissemination, 5 and (3) stymies the advancement of innovative health-enhancing programs in low-income, minority communities. One possible solution is the embrace of more community-based participatory research. Interventionists must equally integrate the voices of those who are the intended recipients of these interventions.5,29 This strategy shifts the power dynamic from legal and clinical teams to the very communities that MLPs are directed toward. Furthermore, it nurtures empowerment, leading to increased engagement and support among these populations for MLPs and the role they play in resolving a HHLNs across vulnerable communities.
In this study, most studies presented a medium risk of bias scores, thus undermining the validity of MLP efficacy. This was due to the absence of many metrics (e.g., random allocation, intent to treat analysis, and power) for all the quasi-experimental studies. Only two studies, Sege et al, and Liaw et al, evaluated MLP implementation using rigorous RCT standards. These studies’ approaches are worth replicating to strengthen the evidence base of MLP interventions in research and practice settings. 41 Another challenge is that these studies were multimodal and involved activities such as home visits and diabetes education that complement legal services. While these programs offer a more holistic delivery of services, their well-integrated nature makes it difficult to isolate the specific effects of legal services. This review demonstrates that the scientific landscape on MLP research is still evolving and would benefit from the high-quality RCTs that rigorously test effectiveness and feasibility in populations that need them the most. These findings furthermore highlight the need for organizations to transform into systems where delivery, training, learning, and research activities are routinely to enhance the implementation processes of MLP programs. 42 The importance of RCTSs in efforts to evaluate MLP’s effectiveness cannot be overemphasized. As the gold standard for causal inference in health services research, RCTs offer the highest level of methodological rigor by minimizing selection bias and ensuring that observed effects are attributable to the intervention itself. This is important for MLP programs, which often function within complex, multi-layered social environments where many confounding variables are of issue. Throughout our review, we engaged in repeated and comprehensive database searches over an extended period. Despite the breadth of this search, we identified only two RCTs that met our inclusion criteria. This reveals a persistent gap in high-quality evidence and highlights the urgent need for well-designed RCTs that support MLPs' effectiveness and provide policy-relevant findings.
A key observation of our review was the limited geographic variation of our eligible studies. Among the seven studies, the majority were conducted in coastal cities, with only one taking place in the South (Texas), and none in the Midwest region. Despite the existence of over 300 MLP programs nationwide, there are notable disparities such that very few are implemented across Southern and Midwestern states. Research shows that the South, in particular, is home to a significant share of the U.S. BIPOC population (Black, Indigenous, and People of Color), and experiences disproportionately poorer health and socioeconomic outcomes relative to Northeastern and Midwestern states. 43 For example, U.S. residents living in the South are more prone to higher rates of chronic diseases, cancer, and infant mortality, and are disproportionately uninsured, underinsured, and of lower socioeconomic status. 43 MLP programs to tackle the disproportionate distribution of HHLNs by region are strongly warranted but require system-level alignment of efforts. These strategies encompass rigorous scientific testing, transdisciplinary partnerships, financial and social capital investments, policy and community advocacy, and higher-level teaching and training across medical and legal institutions. Collectively, these elements may prove promising to effectively tackle the HHLNs that contribute to health disparities across the Southern and Midwestern U.S. regions.
Strengths and Limitations
This study was not without limitations. First, we only included English printed studies, eliminating potential experimeental MLP studies conducted in other countries. Second, the included studies varied widely in design, intervention type, and MLP integration. In some, MLP constituted the primary intervention, while in others, it was one of several supportive components, making it difficult to isolate MLP-specific effects. Variability in outcome measures and screening tools further complicates synthesis and interpretation. Studies used differing definitions of success, diverse legal screening practices, and a wide range of reporting formats, limiting direct comparability. While this lack of standardization poses a barrier to building cumulative MLP evidence, it also reflects the adaptability of different MLP models to meet local contexts and needs. Third, our focus on experimental and quasi-experimental designs, while methodologically rigorous, excludes important observational studies that could have enriched the review’s breadth. Finally, small sample sizes and substantial variability in measurement tools and outcomes prevented formal synthesis and limited cross-study comparison.
Despite these limitations, our study had notable strengths. It explicitly focused on peer-reviewed experimental studies, which are better suited to assessing causality, and employed an extensive search across clinical, public health, and legal databases without restriction by place or year of publication. This review adhered to PRISMA guidelines, systematically assessed the methodological quality of included experimental studies using the CONSORT checklist and used two independent reviewers for study selection, eligibility determination, and quality assessment. The methodological heterogeneity of included studies also underscores the real-world applicability of MLP interventions, demonstrating that the core MLP framework can be effectively adapted to diverse settings and populations.
To improve the evidence base for MLPs, future research should employ more rigorous, standardized, and inclusive approaches. Prioritizing RCTs with clearly defined and isolated intervention components will improve causal inference and clarify intervention effects. The use of validated, standardized outcome measures and consensus-driven core indicators i will also enhance comparability and facilitate synthesis across studies. Expanding geographic representation, especially in the Southern and Midwestern United States, where health inequities are more pronounced, will improve the generalizability and equity relevance of findings. Finally, incorporating community-based participatory research frameworks will foster meaningful stakeholder engagement, help improve participant retention, and ensure that interventions are culturally and contextually relevant.
Conclusion
MLP interventions were found to be successful in resolving HHLNs among targeted populations. Our review underscores the need for (1) further rigorous experimental studies that establish the impact of MLPs on social needs and health-related outcomes in vulnerable populations and (ii) implementation science approaches to support effective adoption and scalability across practice settings, ensuring the greatest benefit for at-risk populations.
Consent for Publication
This systematic review presents evidence on Medical-Legal Partnerships’ impact on adverse social determinants of health (health-harming legal needs). As such, consent for publication was not applicable.
Footnotes
Author Contributions
Dr Jemima John: Conceptualization, Methodology, Writing—Original Draft, Writing—review and editing, visualization.
Mentors, Drs. Thomas Murphy and Shreela Sharma supported via Writing, review and editing, Project administration, Resources, and Funding acquisition.
Dr. Emily Zeintek: Validation, Writing—review and editing.
Dr Thien-An: Validation, Writing—review and editing.
Odinakachukwu Dimgba: Validation, Writing—review and editing.
Drs. Winston Liaw, Catherine Burnett, and Mary Aitken: Writing—review and editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: University of Texas Health Science Center Stanley Scholar Foundation: UTH fund code: 60655.
Ethics Approval
Given that this is a systematic review of the evidence on medical-legal partnerships’ impact on adverse social determinants of health, consent, and approval were deemed irrelevant.
Data Availability Statement
As the corresponding author, I assert I can provide full access to all research material (review files from Rayyan software, selection manuscripts, and writings) tied to this paper.