
Abstract
Despite spending more per capita on health care than any other country, health outcomes in the United States rank low. In 2001, in an attempt to improve the situation, The Institute of Medicine defined ideal health care as safe, timely, effective, efficient, equitable, and patient centered. In 2008, to more clearly define the goals of health care, Berwick, Nolan, and Whittington of the Institute for Healthcare Improvement (IHI) introduced the concept of the Triple Aim—the simultaneous improvement of population health and patient experience while controlling costs. In 2011, the 3 goals of the IHI Triple Aim were adopted by the US National Quality Strategy. Whereas the IHI Triple Aim represents a powerful innovation in health care, population health extends far beyond the care delivery system. To increase the potential impact of efforts that promote the Triple Aim, we offer a model that includes the addition of lifestyle medicine and social policy initiatives to provide a bridge from the clinic to the community and address nonmedical determinants of health. Addressing lifestyle and social policy will require the engagement of nonmedical sectors of the community in new partnerships with health care. The power of these partnerships could result in large and sustainable improvements in health, economic status, and well-being.
‘The IHI Triple Aim is to simultaneously improve population health, improve patient experience with health care, and reduce the per capita cost of health care’
Introduction
The US health care system is fragmented, difficult to navigate, and lacking in customer service. Despite significantly higher per capita expenditures for care, it performs poorly relative to other countries, which may, at least in part, be related to the relative investment in social services compared with health services.1,2 Banks et al 3 showed that compared with England, Americans in similar socioeconomic positions experienced significantly poorer health outcomes in several dimensions. Diabetes rates are nearly twice as high in the United States as they are in England. 4 Rapid increases in the cost of care in the United States have not been accompanied by equivalent improvements in outcomes.
Efforts to rectify the situation have been underway for more than a decade. In 2001, the Institute of Medicine (IOM) published Crossing the Quality Chasm. This document highlighted the poor quality of American health care and defined ideal health care as safe, timely, effective, efficient, equitable, and patient centered. 5 In 2008, Berwick, Nolan, and Whittington of the Institute for Healthcare Improvement (IHI) introduced the “Triple Aim.” The IHI Triple Aim is to simultaneously improve population health, improve patient experience with health care, and reduce the per capita cost of health care. 6 Organizations that use the IHI Triple Aim as an organizational compass accept the responsibility to care for a defined population and may consider a program design concept organized around 5 components: (a) focus on individuals and families, (b) redesign of primary care services and structures, (c) population health management, (d) cost control platform, and (e) system integration and execution. 7 The 3 goals of the IHI Triple Aim have subsequently been adopted as major aims for the US National Quality Strategy. 8 More recently, the IOM has published a series of reports that address many of the factors related to this issue through a focus on where investments in public health should be prioritized, 9 how to leverage public policy, 10 and the use of measurement in shaping action and accountability. 11 Furthermore, the IOM has recently introduced the term community well-being as a way to assess the conditions in which people can be healthy and includes elements such as education, employment, safety, transportation, housing, food, and worksites. 12 Taken together, this series of reports provides a strong foundation on which to build population health improvement efforts that extend beyond the clinical care delivery system. Such efforts should represent both health care and public health and involve collaborations across multiple stakeholders within communities.
The nonmedical determinants of health are estimated to account for approximately 80% of the variance in the health of a population.13,14 Hence, addressing clinical issues alone will have limited impact on the population health goal of the IHI Triple Aim. Including lifestyle medicine interventions and social policy initiatives in efforts to improve population health creates a much greater opportunity to leverage the IHI Triple Aim toward improving population health and subsequently reducing the need for costly health care.2,10,15-18
In this position paper, we present definitions of health, population health, and lifestyle medicine, briefly review the determinants of population health, present an argument that lifestyle medicine and social policy initiatives must be adopted if the country is to have the largest possible impact on the 3 goals of the IHI Triple Aim, and present examples of activities that promote an integrated Triple Aim. We posit that an integrated Triple Aim occurs within health care systems in the context of a broader community environment. We recognize that social policy is an integral part of public health, but intentionally emphasize it to highlight the relationship between investments in social programs, health care programs, and overall population health outcomes. If the Triple Aim is to be achieved, the investment ratio between social and health care programs is a critical element in achieving it. 2
Definitions of Health and Population Health
When “health” is narrowly defined as the presence or absence of disease, our thinking is limited to the point that disease is equivalent to ill health and that health care only addresses disease. 19 More than 60 years ago, the World Health Organization adopted a broad definition of health and defined it as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.” 20 This definition acknowledges that individuals seek well-being, not just the absence of disease, and it creates both the opportunity and obligation to look beyond the clinical setting for the determinants of population health that might be improved through lifestyle programs and social policy action.
Another definition directly applicable to our discussion of the IHI Triple Aim applies to “population health.” Kindig and Stoddert 21 define population health as “the health outcomes of a group of individuals, including the distribution of such outcomes within the group.” It is of interest to note that this definition concerns itself with what determines health and also the measurement of health outcomes. The authors eloquently argue that this is appropriate because the concept and measurement of health and health outcomes focuses attention on the impact of individual determinants of health and their interactions on some appropriate outcome considered. Furthermore, inherent in the definition is the issue of health equity since it includes the distribution of health outcomes across subpopulations.
The definitions of both health and population health refer to a state measured at a given time and, taken together, they recognize the importance of health being defined as more than merely the absence of disease and that individual health is important since it aggregates up to the health of the population. They also raise the issue that determinants of health, the measurement of health outcomes, as well as the distribution of health outcomes within subpopulations are important considerations.
An Approach to Measurement of Population Health
Representing population health through a measure of disease prevalence alone does not reflect a population’s complete state of physical, mental, and social well-being. As described by Parrish, 22 a full set of metrics for population health outcomes would include (a) life expectancy from birth, (b) age-adjusted or age-specific mortality rates, (c) condition-specific changes in life expectancy and mortality rates, and (d) self-reported general levels of health and functional status. Furthermore, Parrish recommends that population health metrics should communicate both the overall level of health of a population and the distribution of health among different geographic, economic, and demographic groups within the population. If a summary measure is desired, he recommends reporting health-adjusted life expectancy, healthy life years, or a population-based measure of health-related quality of life.22-25
The social and environmental determinants of health are well understood in public health practice and the relationships between them and health outcomes are well established. Despite this, clinical care remains the focus of health reform efforts. The IOM has made clear recommendations to support the development of metrics and measures that reflect population health efforts in these social and environmental domains. 11
A Definition of Lifestyle Medicine
Egger et al 26 have defined lifestyle medicine as “the application of environmental, behavioral, medical, and motivational principles to the management of lifestyle-related health problems in a clinical setting.” We conceptualize lifestyle medicine as having 2 major components: One addresses the behaviors of individual patients to improve their health and well-being and the other addresses social policies that affect the health of populations and support the efforts to improve the health of all individuals within the broader population. This concept is consistent with established public health approaches.9-11 Although the scope of this definition appears broader than the definition that others have used 26 in that it explicitly extends beyond the clinic walls, the breadth of this approach is not without precedent in other areas. When dealing with a cholera epidemic, for example, it would not be appropriate to focus solely on the individuals who have become ill. The scope of intervention would be sufficient only if action were also taken to identify and eliminate the source of the epidemic. The same responsibility is present for all other health conditions that are affected by social policy. That being said, we use the term lifestyle medicine and social policy in this article to emphasize the point that attention to both individual needs and social context through policy is required if interventions are to be optimally effective.
Since lifestyle medicine is designed to address care-related issues along with health behaviors and environmental concerns, it may be regarded as an innovation that bridges several of the health determinants with the objective of improving the health of the individual patient. When a lifestyle medicine approach is deployed in a health care environment focused on best experience for the user and optimizing cost through quality, it may be viewed as an integral part of moving toward achievement of the IHI Triple Aim. Extending the reach of lifestyle medicine through complementary social policy can have a profound and sustained impact on the health of the individual and the population.
The Determinants of Population Health
Social injustice is killing people on a grand scale
27
Booske et al, 14 at the University of Wisconsin Population Health Institute, have assigned attributable fractions to these components. They concluded health care to be associated with approximately 20% of the health status of a population, health behaviors to be responsible for 30%, socioeconomic factors to be responsible for 40%, and environmental factors to be responsible for 10%. They acknowledge that genes have an impact on health, but they do not include genetics in their model because genetic interventions are neither feasible nor acceptable at a population level. Although the relative impact attributed to these categories varies somewhat among studies, no one suggests that health care is the major determinant of health.13,28-33
Position on the social ladder has been identified as a very powerful determinant of health status. 33 In addition to the effects of the stress that is caused by being at a low social rank, it also constrains choices and opportunities. Ironically, a large social gradient also has a negative impact on the health of the rich, not just the poor. 34 Conversely, healthful natural and built environments and equitable social and economic policies not only promote happiness and harmonious relations among the population but also increase security. 17
Tobacco use, poor diet, physical inactivity, alcohol use, unsafe sex, and illicit drug are important behavioral determinants of health.35,36 Air quality, water quality, and the built environment are 3 important environmental determinants. 28 These environments are influenced by the policies of multiple stakeholders across multiple sectors of the community, including transportation and public health agencies, housing authorities, business and industry, health systems, and school systems, among others.9,10,28,37 Nonmedical determinants of health may be underrepresented in the list of most important clinical preventive services 38 ; however, their large impact on health status compels us to address them if we are to optimize population health. Among Organisation for Economic Co-operation and Development (OECD) countries, an assessment of the association between variations in health services expenditures and social services expenditures with population-level health outcomes showed that a higher ratio of social to health expenditures is a significant predictor of better population health outcomes. 2 The average ratio of social to health expenditures for OECD countries from 1995 to 2005 was 2.00; the ratio in the United States during this same period was 0.91. Increased attention to the broader domains of social policy, such as unemployment, housing, and education, will be needed to achieve a ratio of social to health expenditures in the United States that is better aligned with envisioned population health outcomes.
Leveraging Lifestyle Medicine and Social Policy to Promote the Triple Aim
Based on the rationale that associates lifestyle medicine and social policy initiatives with population health outcomes, Figure 1 depicts an approach that integrates the multiple determinants of health with the IHI Triple Aim. This Integrated Triple Aim recognizes that in order to achieve population health improvements, efforts need to extend beyond the care delivery setting, involve not only patients but also their families, friends, and reach deeply into the physical, psychosocial, and socioeconomic environments that influence community well-being. 12 The center of the model represents the simultaneous pursuit of improved outcomes in the population health, experience, and cost dimensions as outlined by the IHI Triple Aim. The idea that the health care sector as a whole needs to integrate with care delivery efforts to generate optimal impacts is depicted by representing it as a factor in the outer ring. Lifestyle medicine, with a focus on health behaviors, and social policy efforts are the other determinants of health that complete the model.
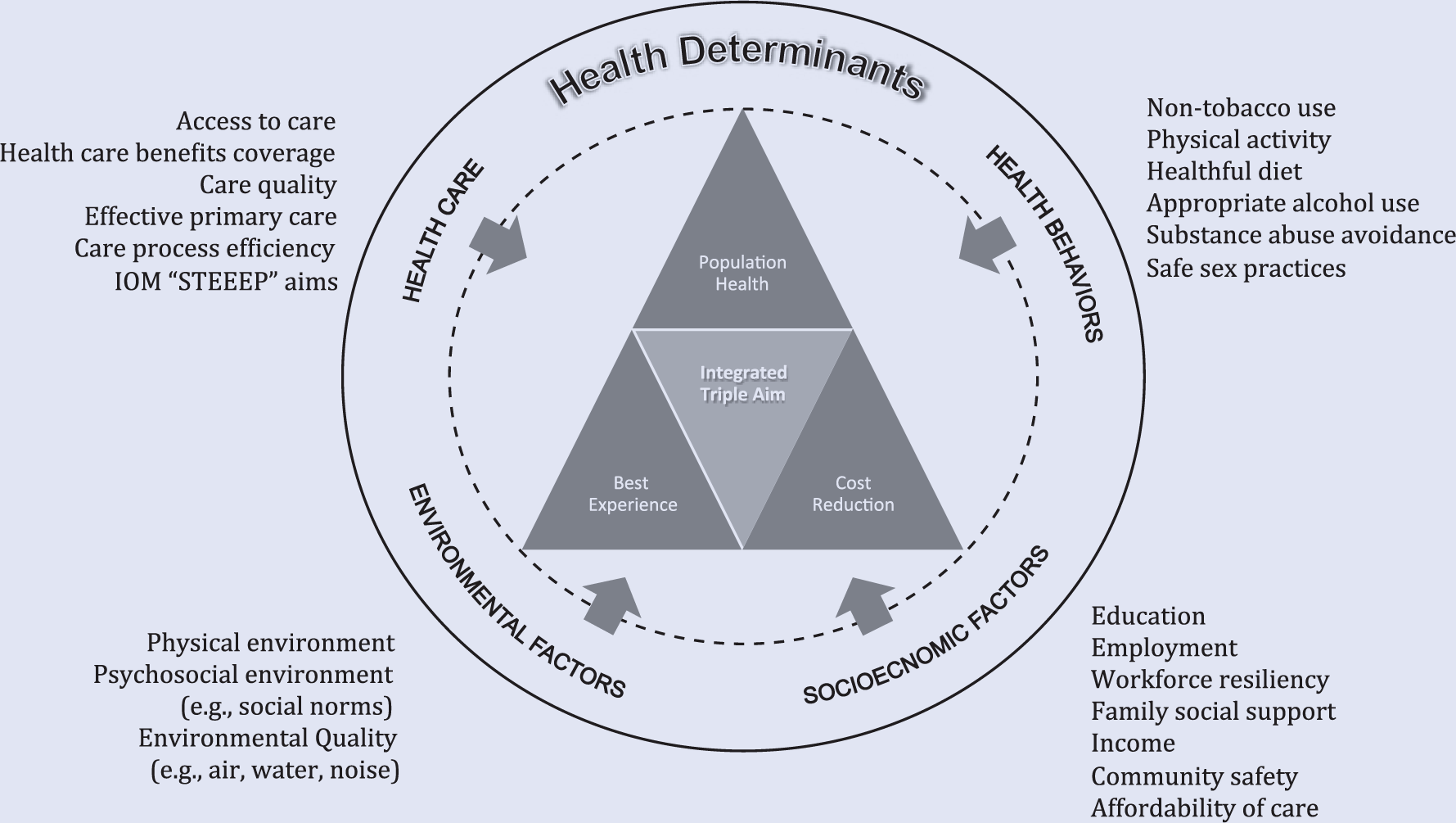
An Integrated Triple Aim in Context of Multiple Determinants of Health.
Since the definition of population health includes the measurement of outcomes, the Integrated Triple Aim is to be accompanied by a robust set of metrics. We, similar to Parrish, 22 recommend that health outcomes should include metrics related to self-perceived health and functional status as well as mortality and morbidity, and we agree with others that health-adjusted life expectancy is an appropriate summary measure of population health.11,22-25 In addition, we recommend total cost of care as the summary measure for the cost dimension. 39 The HealthPartners Total Cost Index and Total Resource Use Index measures 39 are population-based, patient-centered, total cost of care measures. Few publicly available cost and resource measures exist and since this measure is the only total cost of care measure endorsed by the US National Quality Forum, it represents a metric that may be used across the country.
As portrayed by the figure, the 3 components of the Integrated Triple Aim model interact with each other and are responsive to and aligned with activities in the broader community. Social policy represents the primary means through which the broader community is reached and, as a result, all members of population benefit.2,10,18 Examples of stakeholders and sectors that clearly influence population health have been associated with goals and objectives for improving the health of the nation as part of the Healthy People 2020 initiative and include, among others, public health, business and industry, education, mass media, urban planning, land use, and transportation. 40
Promoting the Triple Aim in a Health System
In general, health systems have significant potential to improve population health. 41 A health system that wishes to apply this more integrated approach to the IHI Triple Aim must establish concordance between organizational goals and objectives and the pursuit of population health with best experience at lowest cost. Organizational goals and objectives need to be made relevant for each respective business unit, division, and department where frontline staff interacts with members and patients and where managers execute the key strategies related to generative health-producing processes, programs, and policies. The health system must recognize that as goals become more distal to its own enterprise, it will have less control and influence over such goals. Because of this, partnerships must be established with stakeholders who are closer to the particular goal that is being addressed.
An example of this approach to implementation of the IHI Triple Aim is provided by HealthPartners in Minneapolis. 42 HealthPartners is an integrated health system in the upper Midwest that provides care, coverage, research, and education to improve the health of its members, patients, and the community. As the largest consumer-governed, nonprofit health care system in the nation, it has a history of planning for population health improvement. Activities to improve population health at HealthPartners are organized as multiyear, strategic agendas, guided by ambitious goals, and referred to as the Partners for Better Health initiative. The main purpose is improved health of patients, members, and the community and is in direct alignment with the HealthPartners mission. 43 Activities are directed toward multiple dimensions, including health care, health behaviors, socioeconomic factors, and environmental factors. Figure 2 presents a depiction of the HealthPartners Partners for Better Health 2014 population health improvement strategy.
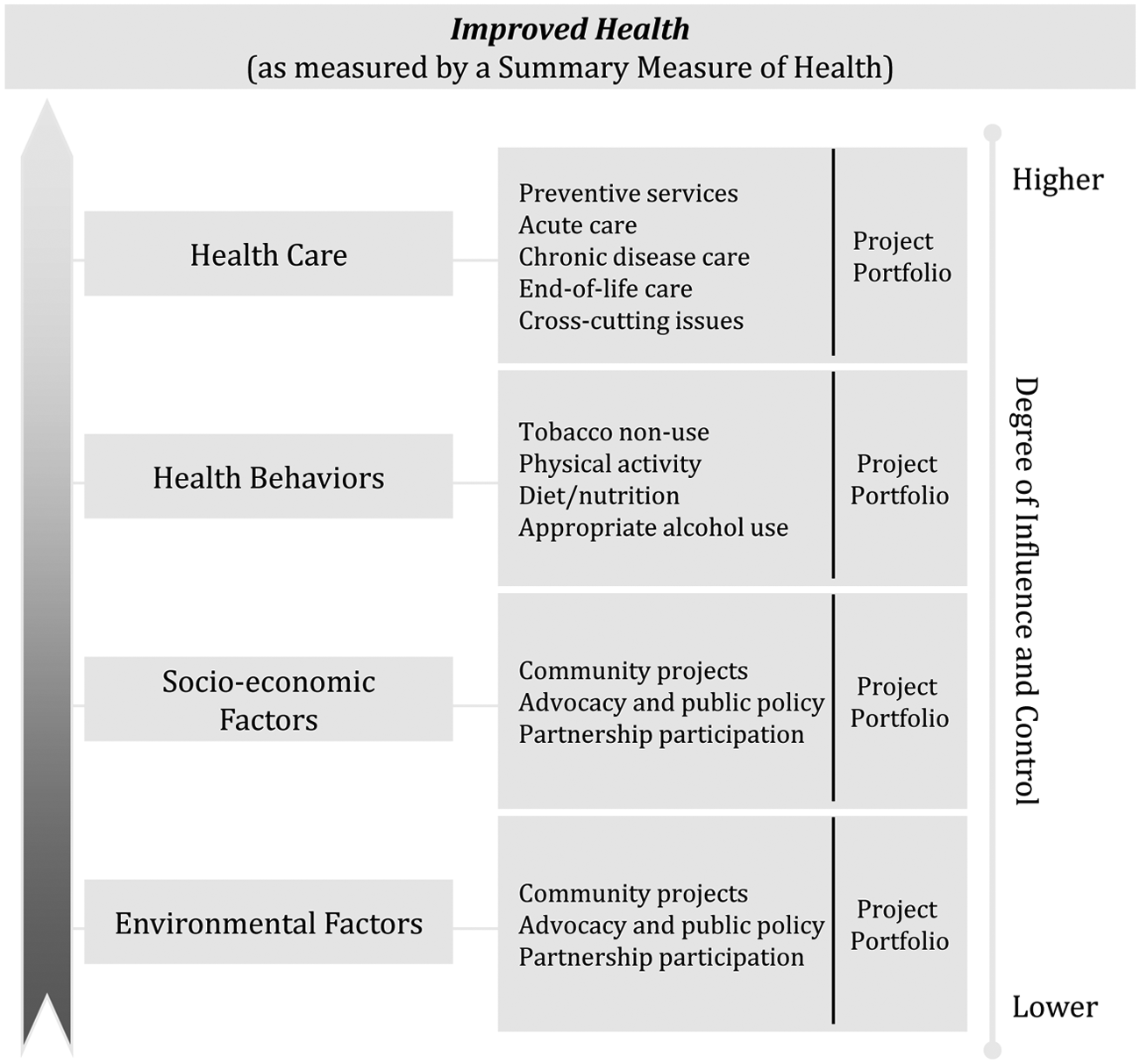
Design for Partners for Better Health Goals 2014 Initiative at HealthPartners.
The Partners for Better Health 2014 goals are part of an enterprise-wide strategic plan that also includes goals related to patient experience with health care and affordability of health care services. The Health Council is responsible for oversight of the population health agenda, and the Health Council coordinates its functions with those of an Experience Council, People Council, and an Affordability Council. The interrelationships among these four councils ensure that operational activities represent coordinated efforts. The presence of explicit goals and project portfolios related to socioeconomic and environmental factors is evidence of the integration of nonmedical determinants of health into the population health initiative. As an example of bringing these goals to life, the sidebar box presents a case study of bringing these concepts to life at the worksite.
Achieving the Triple Aim at the Worksite
Improving the health of populations refers to a process that is considered to be active, dynamic, integrated, and designed to measure health outcomes over time for both the group as a whole as well as the individuals within it. This process may be referred to as population health management and has been defined in the context of the workplace as “the strategic and operational processes used to generate the health outcomes of a defined group of individuals collectively associated with a company’s health improvement efforts.” 44 When considering the defined population associated with an employer group, HealthPartners has published on achievement of the IHI Triple Aim as a result of the implementation of a comprehensive, multicomponent worksite health promotion program.45,46 The design of this strategy was informed by recommendations from the Community Preventive Services Task Force as outlined in the Guide to Community Preventive Services. 47 At the beginning of each of 3 years, employees completed a health assessment and were provided health improvement programs that were relevant to risk factors identified. Completion of the health assessment and participation in the follow-up programs were rewarded with a deductable or co-pay differential in the following year (a $250 annual value). At the end of 3 years, a significant improvement of 6.1% in the population health summary score was observed, participation and satisfaction rates with the programs were more than 90%, and a return on investment of 3:1 was calculated using 3 different methods. In addition, significant productivity improvements were observed. In this example, simultaneous achievement of exceptional program experience, population-level indicators of health improvement, and reductions in health care expenditures as well as productivity losses were observed within a 3-year period.
Addressing the Challenge of Social Policy
Whereas the illustration of achieving the Triple Aim at the workplace is a good example of bringing this concept into reality, it represents a limited view of how social policy may be leveraged. One of the most celebrated examples of harnessing the power of social policy for population health may well be the North Karelia Project in Finland. 48 In the 1960s, Finland was suffering from an epidemic of coronary heart disease recording the highest mortality rates in the world. 49 The root causes of the epidemic were widespread tobacco use and elevated cholesterol and hypertension levels. Clinical interventions and social policies—particularly tobacco and food policies—were implemented. As a result, cholesterol, blood pressure, and smoking rates declined markedly; cardiovascular disease, lung cancer, and total mortality rates improved significantly; and today middle-aged Finnish men and women have a life expectancy that is 10 years longer than it was in the 1970s. 48
The leverage of social policy to complement and support clinical practice was an important component of the success celebrated in Finland. To optimize the chances for social policy potential to be identified and pursued, Finland has adopted the Health in All Policies (HiAP) model. 50 By using HiAP, leaders and policy makers examine policy in all sectors to be sure that a change in policy in one sector does not threaten the health, well-being, and health equity of the population. 51 HiAP can also be used to examine how policies that are not in the health sector might be changed to promote population health and well-being. In this regard, it is highly promising strategy to consider social policy initiatives in sectors such as education, housing, law, and others to improve the health of the population.2,10
Conclusions
By crystallizing the goals of health care into just 3 components, the IHI Triple Aim represents an important advance in health care systems thinking. It prompts population health improvement along with improved experience and the control of health care costs. To optimize the goals of the IHI Triple Aim, we have presented a model that includes the addition of lifestyle medicine and social policy initiatives to address the nonmedical determinants of health that are central to sustained success but largely act to support individuals and population outside the clinical care delivery setting. Addressing lifestyle and social policy will require the engagement of nonmedical sectors of the community in new partnerships with health care. The power of these partnerships could result in large and sustainable improvements in health, economic status, and well-being.