
Abstract
Objectives: The purpose of this study is to use the National Health Interview Service (NHIS) database to assess the impact of socioeconomic factors on fall risk in older adults in the US. Methods: The NHIS database was retrospectively analyzed to assess several variables related to falls and resulting injuries in older adults. The database covered the period from 2000 to 2018. Results: Our study identified several correlations that have not been previously reported in the literature. Welfare recipiency was associated with more injuries from falls (aOR = 18.8, 95% CI: 1.9-185.6, P = .01), while US citizenship was associated with a lower risk of falls in older adults in the US (aOR = .4, 95% CI: .2-.9, P = .02). Discussion: These findings highlight the importance of evaluating patients for social determinants of health (SDOH) in both the inpatient and outpatient setting. Based on this data, we believe SDOH should be incorporated into fall risk assessments.
“Welfare recipiency was associated with an increased risk of falls, while US citizenship was associated with a lower risk of falls in older adults in the US.”
Introduction
Falls among older adults (age >65) accounted for 3 million emergency department (ED) visits in 2019. 1 Falls were responsible for 34 000 deaths in this patient population in 2019 and are associated with a medical cost of US$50 billion annually. 1 Additionally, social factors including income, education, and employment status, have been shown to have an impact on the health behaviors of individuals.2-4
Several studies have previously examined the risk of falls in older adults, including the influence of socioeconomic factors.5-8 Kim et al. 5 found that older adults in Korea who were less educated and unemployed had a higher risk of falls. Similarly, Paiva et al. 6 found that less schooling and lower income were associated with a decline in physical functioning among older adults in Brazil. A study in China found that worse self-rated economic status was associated with a higher risk of falls among older adults. 7 A cross-sectional study of older adults in the United States (US) found that low levels of education and income were associated with an increased risk of frailty status, which was associated with an increased risk of falls. 8
These studies have largely focused on patient populations outside of the United States. In addition, although prior studies examine certain socioeconomic factors including level of education and income, there are other variables that should be considered. Therefore, there remains a need to examine the relationship between socioeconomic factors and falls in older adults in the United States. The purpose of this study is to use the National Health Interview Service (NHIS) database to assess the impact of socioeconomic factors on fall risk in older adults in the US.
Methods
This study is a cross-sectional analysis of the National Health Interview Survey (NHIS) database, which is a survey collecting data on the health, health care access, and health behaviors of the civilian, non-institutionalized U.S. population. 9 Data are collected by census interviewers and interviews are conducted via computer-assisted personal interviewing using a mix of face-to-face interviews for initial questions and phone calls for follow ups. Harmonized data for several available variables of interest were extracted through the Integrated Public Use Microdata Series (IPUMS) Health Survey database for the period spanning the years 2000-2018. 9 Given that the data were publicly available, this study was determined to be exempt from institutional review board approval.
In accordance with the definition set by the American Geriatrics Society, we defined our population as individuals
To obtain nationally representative estimates for analysis involving FELYR and FELINJURYR, subpopulation sample weights (SAMPWEIGHT—Sample Person Weight, is a “variable that represents the random selection of a sample person in the household to complete a supplement survey,” as described in IPUMS database) were used, because these weights define the sampling of the smallest subset (FELYR in 2016 or FELINJURYR variable in 1997-2014). For “INJCAUSFALL,” sampling weights were PERWEIGHT (Final basic annual weight), which is described in IPUMS database as representing “the inverse probability of selection into the sample, adjusted for non-response with post-stratification adjustments for age, race/ethnicity, and sex using the Census Bureau's population control totals. For each year, the sum of these weights is equal to that year's civilian, non-institutionalized U.S. population”.
Statistical Analysis
All variables were described by raw n (number of persons in the survey), raw percentage (sample percentage), and weighted estimates with 95% confidence intervals (nationally representative estimates).
Multivariable logistic regressions were used to investigate risk factors of falling or injury due to falling. Three binary outcome variables (“Fell during past 12 months”—No/Yes, “Had injury from fall, past 12 months”—No/Yes, and “Number of times injured by fall”—0-none, 1-one or more) were regressed on several predictor variables. Predictor variables included Age (in years, continuous), Sex (categorical), Main Racial Background (categorical with 4 categories), Hispanic ethnicity (categorical with 2 categories), Born in the United States (categorical with 2 categories), U.S. citizenship (categorical with 2 categories), Educational attainment (categorical with 3 categories), Ever worked (categorical with 2 categories), Above or below poverty threshold (categorical with 2 categories), Total combined family income (categorical with 3 categories), Received income from welfare (categorical with 2 categories), Family’s home owned or rented (categorical with 3 categories), Needed but couldn’t afford medical care (categorical with 2 categories). The levels of the categorical variables are listed in the tables. Odds ratios, adjusted for the predictor variables in logistic regression models (AORs), with 95% confidence intervals (CI) are reported. Statistical significance was set at P = .05. P-values were reported to three decimal places. Percentages and AOR were reported to one decimal places.
All analyses were performed with R (R Core Team (2020) Vienna, Austria). The variables of interest were read using R package ipumsr. 11 The analysis was performed with R package survey.12,13
Results
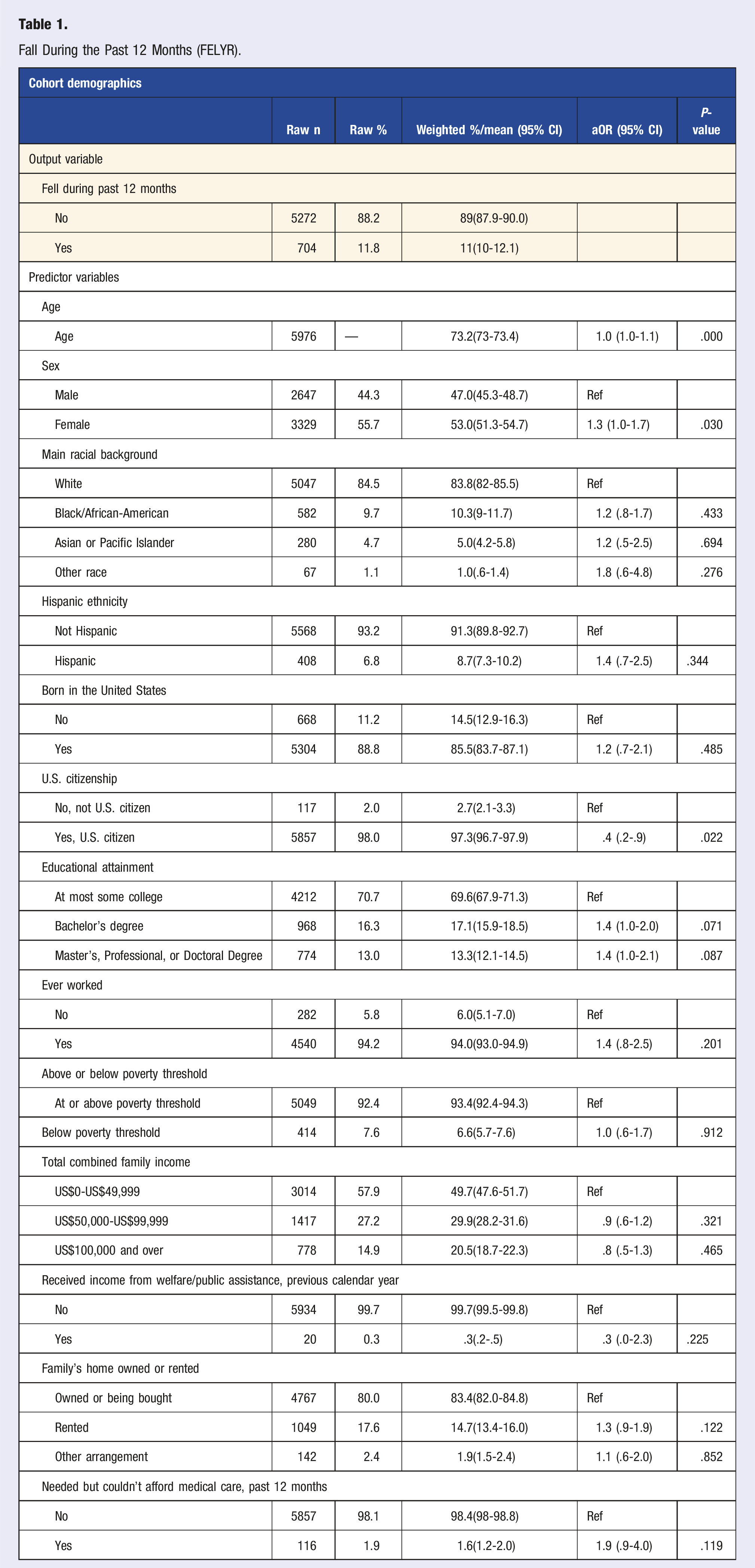
Falls within the Past 12 Months (FELYR)
Fall During the Past 12 Months (FELYR).
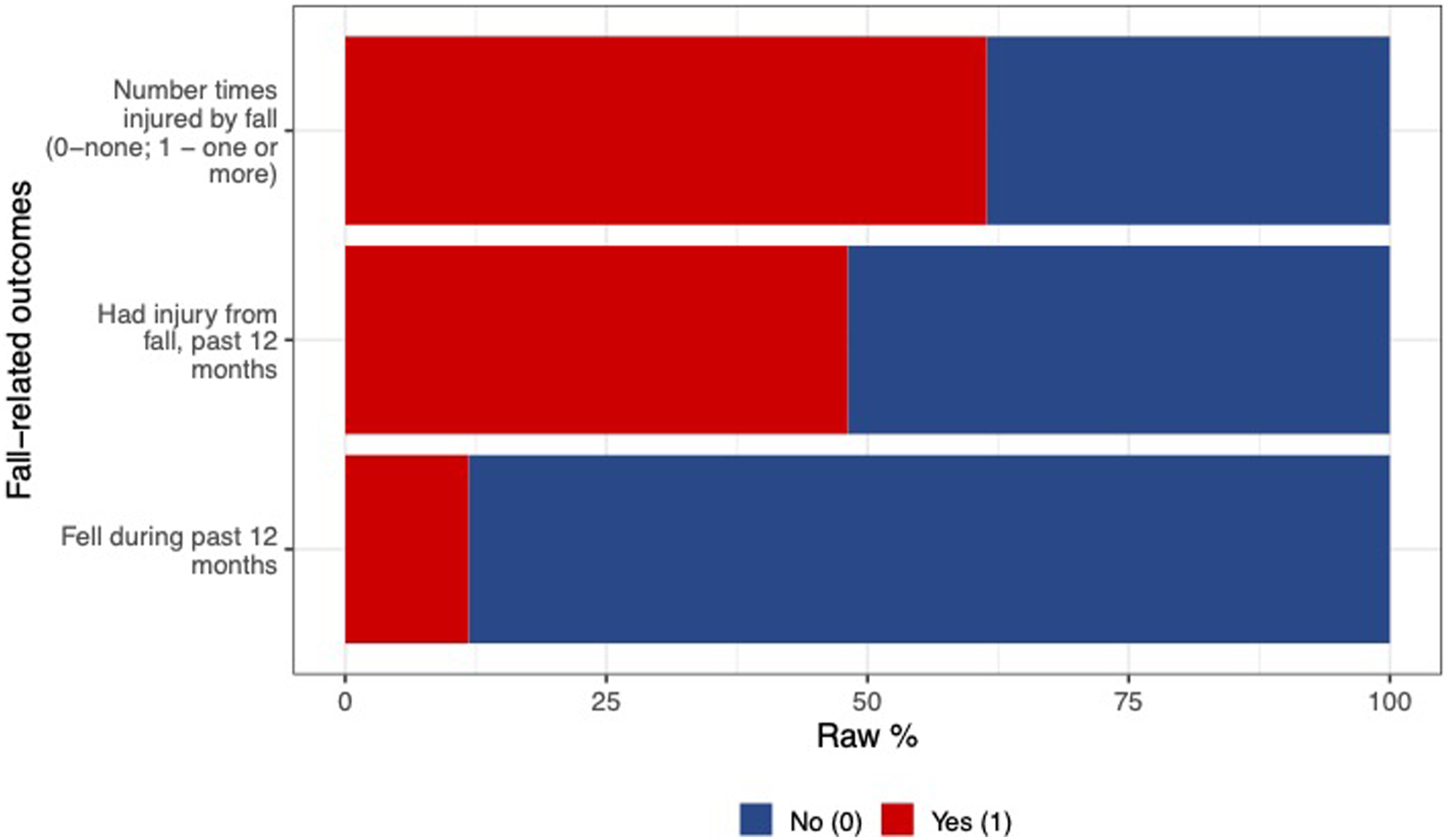
Percent of Individuals Experiencing Fall-Related Outcomes.
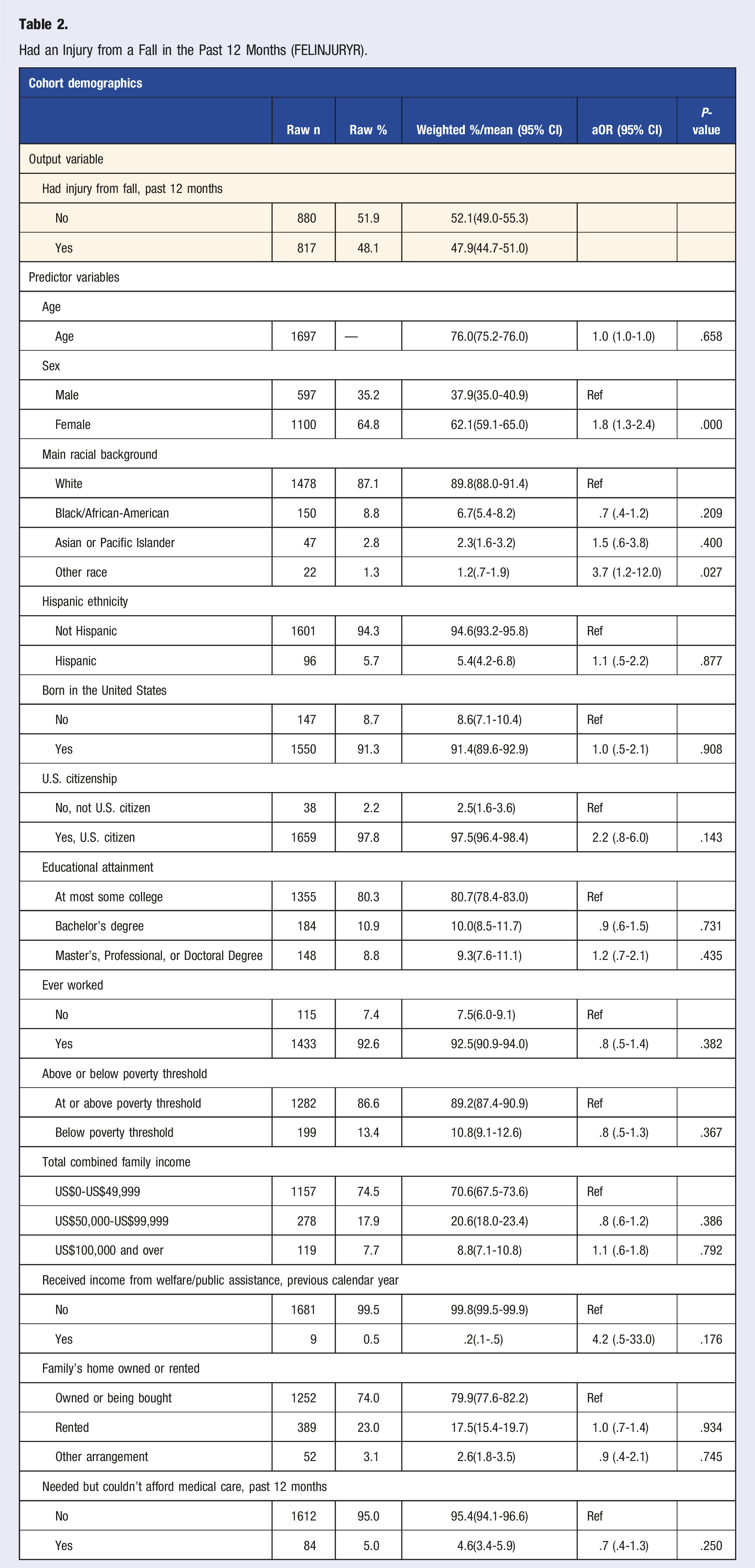
Injury Resulting From a Fall in the Past 12 Months (FELINJURYYR)
Had an Injury from a Fall in the Past 12 Months (FELINJURYR).
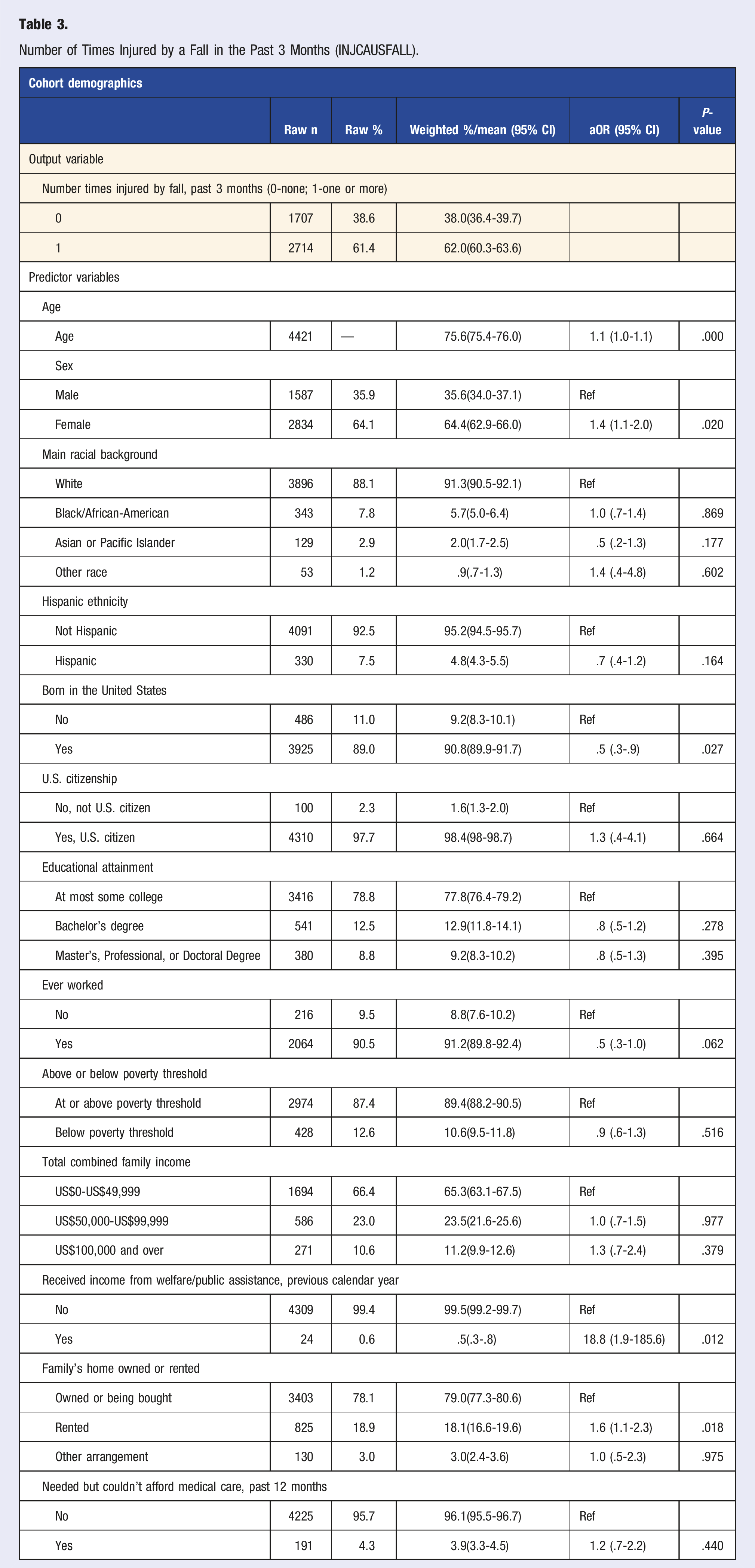
Number of Times Injured by a Fall in the Past Three Months (INJCAUSFALL)
Number of Times Injured by a Fall in the Past 3 Months (INJCAUSFALL).
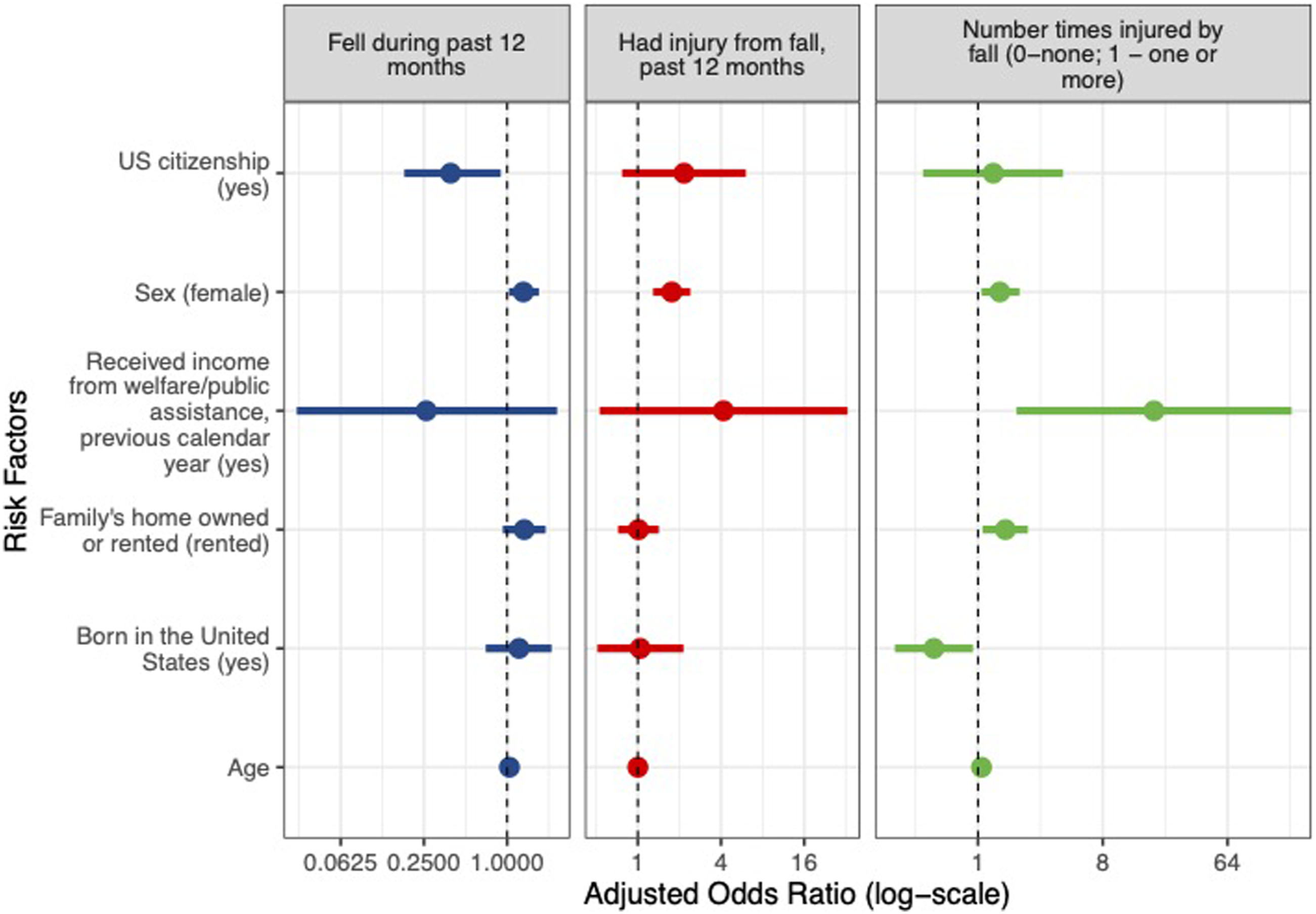
Adjusted Odds Ratios for Select Fall Risk Factors.
Discussion
Falls continue to be a concern for older adults in the US and are associated with a wide array of risk factors. Few studies have examined socioeconomic factors associated with falls in older adults in the US. Our study found several correlations that have not been previously reported in the literature. Welfare recipiency was associated with an increased risk of falls, while US citizenship was associated with a lower risk of falls in older adults in the US. In addition, increased age and female sex were associated with an increased risk of falls in older adults, while no difference was found based on educational status. Validated models such as the Hendrich fall risk model have been developed to assess the risk of falls in older adults in the acute care setting. 14 These models take into account many physiologic and health-state associated risk factors, but do not account for the multifactorial nature of falls including social determinants of health (SDOH) and socioeconomic status (SES).
The current study found no difference in fall risk for older adults based on educational status. This is in contrast to several prior studies which have shown that lower educational status is associated with an increased risk of falls.5,6,8,15 It is possible that having a higher level of education may result in increased awareness of the risk of falling and allow patients to be better equipped to access educational resources regarding mitigating fall risk. 15 However, in older adults with mild cognitive impairment, years of education and measures of cognitive function were not found to be associated with falls. 16 The impact of educational status on fall risk in older adults warrants further study.
Similar to prior studies that have demonstrated gender as a risk factor for falls in older adults, we found that females had a higher risk of falling and injury secondary to a fall.17-19 Several potential explanations have been offered including that males may be less likely to report falls 19 and that females may be more likely to have altered gait mechanics 20 and osteoporosis 21 contributing to fall risk. Similarly, increased age has been associated with an increased risk of falls.15,22-25 We found that each additional year of age increased the odds of a fall by 4.0%. Increased age is associated with several potentially contributing factors including cognitive decline, diminished mobility, and increased frailty.
We found that SES and several SDOH were associated with falls or fall-related injuries in older adults. People who were born in the US and those who had US citizenship had lower odds of being injured by a fall. We postulate that individuals with citizenship status may have better access to resources and more willingness to utilize the health care system. On the other hand, those without citizenship status, particularly those of lower SES, may be reluctant to seek out health care and may not have access to various governmental health care services or benefits. Interestingly, Gill et al. 15 found that individuals in South Australia who were born in non-English speaking countries had a lower risk of falls, possibly due to greater family support.
Individuals receiving income from welfare had higher odds of being injured by a fall. These individuals are typically of lower SES which may contribute to fall risk in multiple ways. Low SES is correlated with cognitive impairment which is a known risk factor for falls. 26 Additionally, individuals of lower SES may have varying perceptions of and more difficulty accessing health care resources including assistive devices like canes or walkers. 27 Renting a home was also associated with a higher odds of being injured by a fall. Gill et al. previously reported that individuals who reported that their home was not in need of maintenance were significantly less likely to fall, which may indicate a safer home environment.15,28 It is possible that individuals who rent their home, particularly those of low SES, may have less than ideal living situations that increase risk of falls including outstanding repairs or maintenance and difficulty with proper accommodations for wheelchairs or other assistive devices. In addition, those who rent a home may not be allowed to make modifications to their home that have been shown to reduce fall risk such as installing guard rails on stairs or grab bars in showers. 29
Fall risk assessment is complex and multifactorial. Our paper supports the notion that socio-economic factors play an important role in determining which patients are at risk for falls. This paper identifies novel demographic considerations in this realm including welfare recipiency and US citizenship among other factors such as age and biologic sex. Individual clinicians and public health programs can make use of these demographic risk factors when identifying potential beneficiaries and for creating community programs and public health policies for fall reduction interventions. This is of particular importance for those practicing Lifestyle Medicine, aspsychosocial interventions targeting nutrition,30,31 inactivity, 32 and other modifiable risk factors, 33 may be paramount to preventing falls and ensuring an improved quality of life for older adults. 34
The widespread use of electronic health records (EHR) has allowed clinicians and public health officials to capture a broad spectrum of demographic data, which through various means (i.e., risk stratification scores, predictive algorithms and clinical determination) helps to identify individuals at risk for falling. 35 Based on this data, we believe SDOH should be incorporated into fall risk assessments. Inclusion of socio-economic risk factors into EHRs, which is already available in some of the EHR programs, could be used in clinicians’ standard practice to aid in the accuracy of falls risk assessments, and aforementioned interventions. This may help prevent quality of life altering and financially costly injuries to older adults. In addition, with the advent of machine learning algorithms in assessing fall risk, incorporating these variables may help increase the accuracy and quality of these models.36-38 However, unless identified, accurately determining patients at risk for falls will remain a difficult endeavor.39-41 Future studies should focus on assessing the benefit of incorporating these risk factors into clinical risk assessments.
Limitations
Several limitations to this study should be noted. Given that the study was a cross-sectional analysis, we were unable to determine any causal relationships between the variables that were analyzed. Although the NHIS database is comprehensive, it is based on surveys of the population and therefore individuals must self-report answers to various questions. As a result, data may be subject to sampling bias and recall bias. In addition, certain individuals may be more reluctant to be forthcoming regarding certain information related to their health or SES. Although the database contains information associated with SES, further clarifying data such as geographic data and zip code were not elucidated. Furthermore, one of the fall variables analyzed included only individuals who reported no problems with dizziness or balance in the past year, which limits generalizability and results may differ from the general population given that both of these issues are significant risk factors for falls in older adults. Finally, the NHIS is available in only English and Spanish and consists only of the US population, which may limit generalizability to other populations that do not speak these languages within the US.
Conclusion
This study provides an analysis of falls in older adults in the US with a focus on social determinants of health and their impact on fall risk and injuries. Similar to prior studies, female sex and increased age were associated with an increased risk of falls in older adults. Contrary to prior studies, we found no statistically significant association between educational status and fall risk in this population. Several unique findings in this study related to SES include lack of US citizenship, receiving income from welfare, and renting a home. These findings highlight the importance of evaluating older adults for SDOH and the potential need to include these variables in standardized fall risk assessments.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.