
Abstract

Keywords
“...Lifestyle medicine is the use of evidence-based lifestyle therapeutic intervention...”
Introduction
Interdisciplinary solutions created from the collective knowledge and experiences of practitioners and experts from across multiple sectors are urgently needed to effectively address health disparities. With the belief that the power of diversity in ideas and voices can develop effective, innovative solutions, the inaugural Health Disparities Solutions Summit (HDSS), produced by the American College of Lifestyle Medicine (ACLM), was held virtually in late 2020. Organized by ACLM’s Health Equity Achieved through Lifestyle Medicine (HEAL) Initiative, the convening was designed to harness this collective power.
The Summit was born out of the vision of ACLM Immedidate Past-president Dexter Shurney, MD, MBA, MPH, FACLM, DipABLM to address lifestyle-related chronic, disease health disparities, with particular emphasis on inequities impacting dietary lifestyle and stress in historically marginalized communities. The Summit convened physicians, faith-based leaders, academics, and community organizers to identify expert consensus and recommended action steps specific to addressing health disparities through the lens of lifestyle medicine. Lifestyle medicine is the use of evidence-based lifestyle therapeutic intervention—including a whole food, plant-predominant eating pattern, regular physical activity, restorative sleep, stress management, avoidance of risky substances, and positive social connection—as a primary modality, delivered by clinicians trained and certified in this specialty, to prevent, treat, and often reverse chronic disease.
Invited Summit participants engaged in roundtable discussions grounded in three vision statements for eliminating health disparities: (1) Health care providers effectively trained in evidence-based lifestyle medicine, equipped to partner with their patients in underserved communities to minimize stress in the medical setting, ensuring optimal health outcomes; (2) High levels of food and nutrition literacy among patients and providers in underserved communities; and (3) Food as medicine fully integrated into communities, their cultures and values—implemented in underserved communities in a culturally relevant way to achieve health equity.
This paper provides background on the realities of health disparities in the United States, introduces the entrance point of lifestyle medicine (LM) practice in the struggle for health equity, and summarizes Summit proceedings and recommended action steps.
Background
Risk factors that contribute to the development of harmful and costly chronic diseases like type 2 diabetes, hypertension, obesity, some cancers and cardiovascular disease are either non-modifiable (age, sex, race, or modifiable diet, physical activity, and lifestyle). 1 Research shows that, while genes play a role, they do not determine health destiny: Genes may predispose, although lifestyle often activates the predisposition. 2
Too often overlooked, the interrelated aspects of a person’s social and physical environment, also known as social determinants of health (SDOH), have a direct influence over a person’s opportunity to mitigate the modifiable risk factors and achieve optimal health. 3 Longstanding, complex and systematically unjust practices including discrimination based on race, gender, and economic status contribute to differences in a person’s SDOH, thereby limiting the accessibility of healthy lifestyle choices for many within underserved communities. Government subsidies that make unhealthful foods cheap and readily available are problematic. 4 Moreover, fast-food restaurants and convenience stores are often found on every corner in underserved areas, 5 while access to grocery stores or farmers’ markets with an abundance of fresh, frozen, or canned whole, plant-based foods (beans, lentils, fruits, vegetables, whole grains, nuts, seeds, and spices) is inconvenient or unavailable. 6 Magnified in our underserved communities, there is a glaring lack of food, 7 health and lifestyle literacy across our nation’s entire population.
Historically, under-resourced and unsafe neighborhoods, decreased access to health care, food deserts, and a lack of robust educational and economic opportunities have perpetuated the disproportionate burden of chronic disease, shorter lifespans, and other differences in health outcomes among underserved populations.3,8 This unfair difference in health quality, health care access, and health status by which populations of a particular race, ethnicity, gender, or socioeconomic status are systematically impacted is referred to as health disparities. 9
In the United States, more than 60% of the adult population has at least one chronic disease 10 — and, alarmingly, 25% of children 11 — with more than 40% of adults already diagnosed with two or more chronic conditions. 10 According to the CDC, Hispanic and non-Hispanic Black adults have a higher rate of obesity, hypertension, and type 2 diabetes (T2D) compared to their White counterparts, 12 and the prevalence of having both diabetes and cardiovascular disease (CVD) is higher among Hispanics and non-Hispanic Blacks than non-Hispanic. Native Americans, Blacks, and Hispanics—largely due to inequalities within SDOH—have faced an increased risk of exposure to and severity of infections from Covid-19. Recognizing that Covid-19 will not be the last infectious disease our nation and world will face, our current reality must serve as a blaring alarm, emphasizing the pressing need to address lifestyle-related chronic disease health disparities. With this issue at the forefront of so many minds, there is renewed urgency to find sustainable, actionable solutions to protect and support those who are most vulnerable.
The principle underlying commitment to reduce and ultimately eliminate disparities in health, along with its social determinants, is defined as health equity. 13 Several federally-funded programs through the U.S. Department of Health and Human Services, including the Centers for Disease Control and Prevention, Indian Health Services, National Institutes of Health and the Department of Veterans Affairs, have been actively addressing the issue of health disparities through research and community-level initiatives. Additionally, important professional medical organizations like the Institute of Medicine (IOM) have focused on the issue of inequality in health. The IOM performed an assessment on the differences in the quality of health care received by racial and ethnic minorities and concluded in a landmark 2003 report that a comprehensive, multilevel strategy is needed to eliminate these disparities. 14 The report sparked the formation of the Commission to End Health Care Disparities in 2004 by the American Medical Association and the National Medical Association, later joined by the National Hispanic Medical Association. The AMA, NMA, and NHMA, together with more than 50 other medical and health professional organizations formed a consensus and provided multitiered guiding principles to end, not merely reduce, health care disparities. 15
Despite the breadth and depth of work that has been done and is ongoing in this sphere, sobering health disparities remain. As others have identified, education and analysis alone are not enough and clinic and community-level interventions are vital. Knowing that lifestyle medicine, striving to identify and eradicate the root causes of chronic disease, offers powerful solutions, and mindful that there is no one-size-fits-all approach, the Summit was organized with the objective to arrive at action steps informed by leaders who not only have intimate knowledge of structural inequities and SDOH, but who have place-based insights and approaches to health equity.
Lifestyle medicine physicians and providers are focused on whole person health—improving a person’s quality and quantity of life by decreasing the risk of chronic diseases through dietary and lifestyle changes. They are thus uniquely poised to champion bridging the gap in health equity within underserved populations who are disproportionately burdened by chronic conditions. Moreover, lifestyle medicine practitioners are often educated in motivational interviewing techniques and patient-centered decision-making models which support reclaiming an individual’s power over their health decisions both in and out of the health care setting.
However, those who practice lifestyle medicine must also consider whether healthy choices are available similarly to all of their patients, considering the barriers related to the SDOH that may prevent equal access to those choices. Recommending lifestyle changes without considering access to necessary resources to support that change in lifestyle, or the underlying issues that contribute to lack of access without also actively working to narrow inequity, poses risk of unintentionally contributing to a widening of the gap in health disparities. The field of lifestyle medicine has some extant research on pursuing solutions to health disparities, accounting for structural, systemic, and environmental variables. Foundational among them is the work of Dr. Janani Krishnaswami and coauthors, defining Community Engaged Lifestyle Medicine (CELM). 9
Dr. Krishnaswami, at the University of Texas Rio Grande Valley’s preventative medicine residency program, established an evidence-based framework through which lifestyle medicine could be delivered as a means to address health disparities among vulnerable populations. 9 While “ad hoc” measures to incorporate lifestyle medicine-based community programs are admirable, fidelity to the evidence-based framework of CELM and similar processes grounded in public health research is paramount in creating iterative, lasting change in underserved communities across the US and beyond. The American College of Lifestyle Medicine’s CELM member interest group was founded to bring awareness of this important issue to its members and has since transformed into the larger HEAL Initiative, out of which the HDSS was produced.
Much like the recommendations lifestyle medicine practitioners offer their patients when managing chronic diseases, lifestyle medicine-focused solutions to the chronic burden of health disparities have powerful transformative potential that can only be realized with ample intersectoral support, commitment, and time. The HDSS was designed as a forum to bring focused attention and in-depth discussions to offer solutions to narrow the gap in health disparities as they uniquely relate to each pillar of lifestyle medicine, pillar by pillar.
Four major focus areas emerged from the inaugural HDSS meetings, along with clear action steps within each area to help inform the future direction of lifestyle medicine as it relates to extinguishing health inequity. The themes were focused on advancing (1) active and informed clinician education; (2) patient self-advocacy; (3) championing community engagement and community-based participatory research; and (4) supporting policy and advocacy efforts to create systems change.
First Recommendation: Educate Clinicians and Promote Minority Clinician Representation
Filling the gaping void of lifestyle medicine training in medical education is imperative, as physicians and allied health professionals who practice lifestyle medicine have a unique and powerful role in helping to create a more equitable future for their patients and communities.
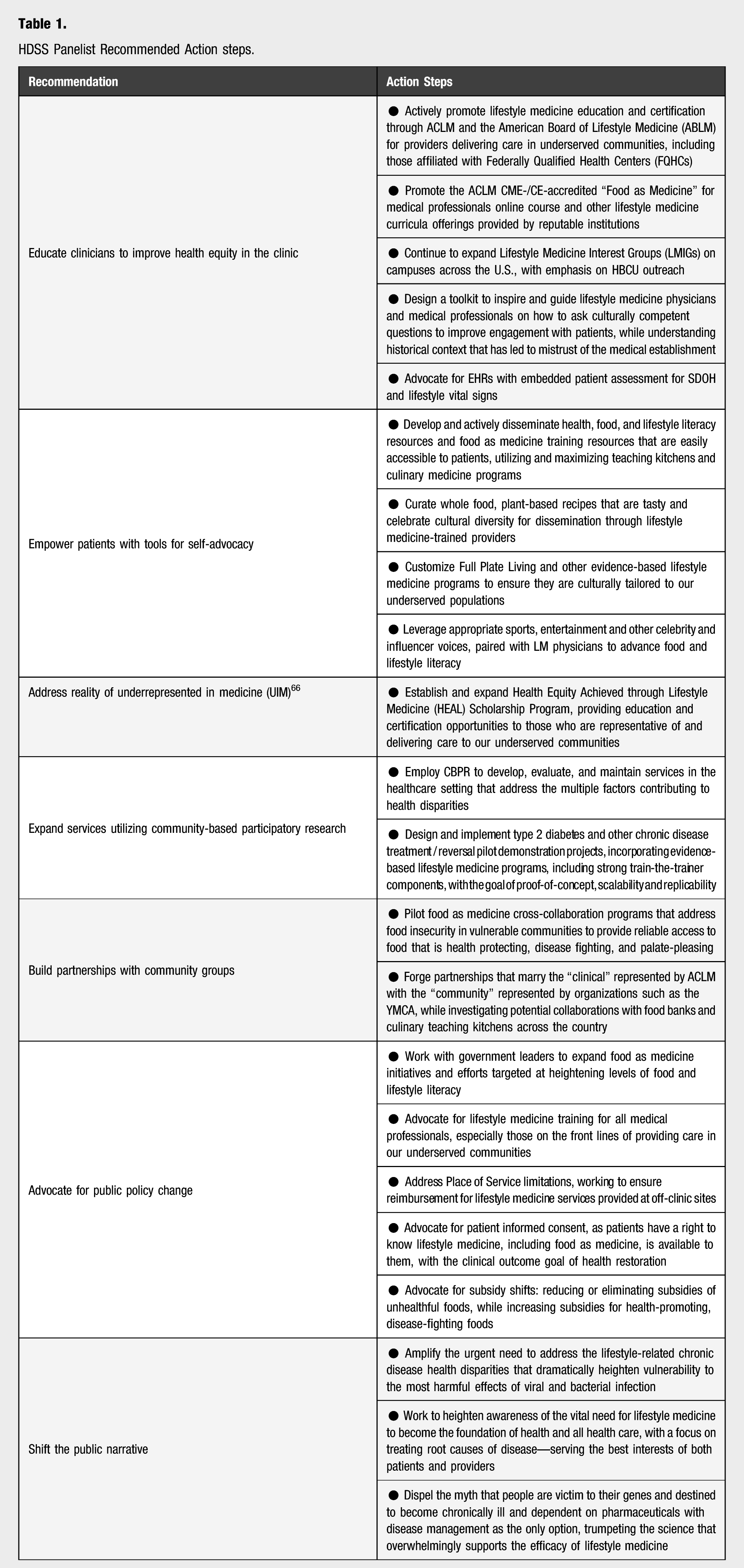
HDSS Panelist Recommended Action steps.
Moreover, addressing lifestyle is recommended as a first-treatment option in many chronic disease guidelines. 21 However, when surveyed, physicians indicate having received little training in clinical nutrition and lifestyle medicine therapeutic modalities. 22
Another critical step towards sustaining real change is for health care providers to understand the historical background and current state of health disparities within the communities they serve. Empowered with this knowledge, the lifestyle medicine-trained clinician can be more intentional and compassionate when working with diverse patient populations. Gaining this important perspective is vital to building trust with patients who may have an understandable mistrust of the medical establishment. 23 This provider perspective and understanding is imperative in order to support patients in making effective lifestyle changes to promote health and reduce chronic disease prevalence. With a better awareness of the role lifestyle medicine can play in narrowing the gap in health inequities, lifestyle medicine clinicians can be champions for diverse populations both within and outside of the clinical setting.
One measure that represents the lack of health equity across communities is the life expectancy gap seen between adjacent zip codes across the country. It is a result of generations of policies and practices that reinforced discrimination and oppression in all aspects of social determinants of health. As a result, historically oppressed and underserved communities have less access to multiple health-promoting resources, including quality education, safe neighborhoods, healthy food, and economic opportunities. 21 Understanding the context of a patient’s life will help physicians approach patients with compassion and empathy, as they offer guidance and share tools for improved health outcomes.
Lack of diversity amongst physicians and other clinicians is another factor that contributes to the lack of equitable, quality care in the health care setting. Underrepresented in medicine (URM) physicians are more likely to practice primary care in underserved communities, and research indicates race concordance between patient and physician leads to greater patient satisfaction and language concordance leads to better compliance with treatments.24,25 Increasing diversity within the health care workforce will help expedite improved equity. The Summit members recommend that support should be provided to increase the numbers of clinicians from minority backgrounds to reflect the rich diversity of the general U.S. population, particularly within communities with disparities in health. Increasing the recruitment of underrepresented minorities in medicine to promote more diversity in medical education and training will not only benefit future patients but will also create a more accurately representative educational space for the learners themselves.
In the meantime, current physicians, regardless of their background, should be trained to improve their relationships with patients in a way that builds trust and encourages patients’ self-advocacy and health literacy. Education should include tools such as shared decision-making training where the clinician prioritizes the patient’s choices as they share high-quality information, discuss the multiple options available, and talk through the decision-making process while prioritizing the patient’s preferences. 26 Further, motivational interviewing training 27 should also be offered to: encourage clinicians to accept the patient where they are in their health journey; support with empathy and compassion; collaborate with the patient to problem-solve challenges in achieving long-lasting lifestyle modification; and be curious about their patients’ motivations and desires so they can effectively support each individual patient. Other trainings to explore to improve clinician support of their patients facing health disparities include: implicit bias training, 28 multifaceted cultural competency training, 29 and the teach-back method. 30
Research should guide the development of educational programs that frame peer feedback so that it is heard, while constructively addressing issues that contribute to health disparities. This will benefit students-in-training, as well as seasoned clinicians. Support should be provided during this time of a clinician’s growth to foster resiliency and avoid clinician burnout across settings—from the community health center, to the academic medical center, to private practice.
To improve health equity, given the lack of nutrition training in medical education, increasing nutrition literacy and food skills amongst clinicians should be a high priority. This may include teaching physician cultural competence of indigenous diets and the cultural significance of food preparation.
Effective patient behavior modification in regard to dietary lifestyle will necessitate development of culturally tailored nutrition education, emphasizing whole food, plant-predominant eating patterns.
Embedding teaching kitchens in clinical settings will be vital, with the goal of marrying “community” with “clinical,” potentially achieved, perhaps, by embedding lifestyle medicine clinics in YMCAs across the nation, or through other creative collaborations that enable lifestyle medicine-trained clinicians to provide patient care through venues that provide the needed space for lifestyle medicine shared medical appointments and culinary “food as medicine” training.
Moreover, what’s needed is the development and tracking of clinical guidelines that support, for example, measuring SDOH and lifestyle factors as a vital sign, 31 with this serving to assess, among other risk factors, dietary history and current eating patterns, incorporating practical, stepwise recommendations into the patient treatment plan. These would be designed to support physician engagement in the community where nutritional insecurity is too often prevalent, enabling the provider to better understand the patient’s environment.
Improving clinicians’ personal nutrition by adopting a mostly whole food plant-based diet is an important step as they advocate the same from their patients. Providers need to recognize—and help their patients recognize—biased health information, such as deeply entrenched public relations campaigns supporting the meat, sugar, dairy, and fast-food industries.
To address the larger picture of scarcity of healthy foods and food insecurity in many vulnerable communities, food pharmacies (a.k.a. farmacies) are a program option that allows clinicians to prescribe healthy foods to their patients in a way that is accessible for the patient. Multiple children’s medical centers have implemented food pharmacies with success as a means to address food insecurity, by providing nutrition education with healthy foods. For example, a pilot program in Washington, DC provides access to 30 pounds of healthy food during pregnancy, continuing for the following 1–2 years, with this serving as an incentive to mothers to engage in prenatal check-ups. In New York City, the Health Bucks program has pharmacists prescribe fresh produce that recipients of SNAP can use in local farmers markets.32–35
For already practicing and future clinicians-in-training, multiple opportunities are needed throughout all stages of education and clinical practice, designed to convey a better understanding of evidence-based lifestyle medicine, diversity, cultural competency, and health disparities, as well as the historical injustices that underlie adverse effects on the health of patients. Additional emphasis in medical education should be on interdisciplinary team-based models of care and shared decision-making that can help displace the traditional patient-provider hierarchy with a more balanced dynamic between clinical expertise and a patient’s values and needs.
Educating, equipping and empowering providers who are on the front lines of delivering care in under-resourced communities, including Federally Qualified Health Centers (FQHCs), is urgently needed in regard to evidence-based lifestyle medicine and SDOH. Also imperative is establishing safe environments across all sectors in health care, where honest feedback regarding discriminatory practices is encouraged. And, implementing policies and practices in clinical settings to consistently screen for lifestyle vital signs and address barriers to healthy dietary and lifestyle change are essential. These, while also encouraging providers to be healthy examples themselves, are action steps Summit participants identified as being essential to effectively address health disparities.
Second Recommendation: Empower Patients to Self-Advocate
Patients who advocate for themselves by asking questions, by voicing their concerns and preferences, and by making decisions on which they can follow through reap the greatest benefit from their clinic visits. 36 Building self-efficacy—the belief in one’s ability—is necessary for a person to feel empowered to make and sustain any healthy behavior change. For a variety of reasons, including access to care, socioeconomic factors, and historical unequal treatment in the health care system, individuals from medically underserved populations are less likely to self-advocate. During the Summit, multiple angles were discussed to facilitate increasing a patient’s agency to make lifestyle changes that would improve their health.
Maximizing peer-to-peer education is an important mitigation tool to counter the traditional power dynamic between patients and clinicians that can impede self-advocacy. Lifestyle medicine shared medical appointments convene groups of patients with common medical conditions—either in-person or virtually—for education, management, and treatment. This team-based approach often achieves better clinical outcomes, while being less costly to implement. 37 Lifestyle literacy education that is culturally responsive may be incorporated to broaden the evidence-based knowledge of individuals from underserved populations and reduce misinformation. The imperative of incorporating a “train-the-trainer” model was emphasized, one that supports community members becoming health educators and navigators to guide patients or fellow community members to appropriate resources.
Teaching kitchens, which may be embedded in YMCAs, community centers, churches, or clinical offices, provide an excellent setting for lifestyle medicine-trained clinicians to provide patients with culinary education—via a shared medical appointment. This education is geared toward improving nutrition literacy, food skills, and increased level of self-efficacy. The lifestyle medicine “food as medicine” training provided through a teaching kitchen setting also supports the Summit’s goal of actively addressing health disparities by advocating for a dietary pattern shift from the standard American diet to a fiber-filled, nutrient-dense, antioxidant-rich whole food, plant-predominant diet, which evidence overwhelmingly supports as efficacious for not only disease prevention, but also for treatment and even reversal of chronic disease and select autoimmune conditions.38–45 At the Capital Area Food Bank in Washington, D.C., which several Summit participants work with and within, hundreds of recipe cards have been created for high flavor, high nutrition, mainly plant-based meals. The recipe cards that feature flavorful and dynamic dishes are available in multiple languages with accessible wording and layout.
It’s encouraging that success with dietary lifestyle changes in teaching kitchens may have a ripple effect as individuals make changes at home that can impact multiple generations living in a household and across households, as they share their experience with their social network. Teaching kitchens are an excellent place to celebrate culture and connect people with their plant-based traditions that may be hidden or lost by the influence of colonization and Westernization. Summit participants provided useful anecdotes about the power of teaching kitchens to reach immigrant populations with skills and recipes encouraging delicious, whole food, plant-based versions of culinary traditions. It was noted, however, that too often teaching kitchens that already exist sit empty, because they lack a Place of Service code. When a facility lacks this identifier, clinicians using the venue to provide medical education and patient care are unable to receive reimbursement for services provided to patients. 46
Beyond the health clinic, self-advocacy in health can be encouraged with storytelling that influences entire communities. Summit members discussed creative ideas including a cooking storyline on a television series that highlights the challenges of living in a food desert, coupled with creative healthful eating solutions; marketing campaigns that support whole food, plant-based eating; and health topics covered in early reading books for children. One example of this is the Do Not Mute My Health “campaign” in Washington, DC that addressed the life expectancy disparities in different neighborhoods due to diet-related chronic illness. Another suggestion was to leverage the voices of sports and entertainment celebrities and other influencers who have embraced healthful lifestyles, possibly through public service campaigns that drive individuals to seek out lifestyle medicine-trained providers, while also encouraging healthful lifestyle behaviors.
Partnering with patients to improve self-confidence is vital to sustaining both individual and community health long term. This can be bolstered through the multi-pronged delivery of interculturally competent educational efforts. Learning from peers in shared medical appointments, having easy access to culturally responsive lifestyle medicine-focused educational materials and reinforcement of that information through trusted, resourceful community liaisons were some of the important takeaways from Summit participants. Partnering with a community to develop plant-based culinary medicine workshops that celebrate the rich cultural culinary traditions of that community can inspire more individuals to gain hands-on practical cooking skills to further increase self-efficacy. Finally, pushing for storylines on television, movies, print media where communities can see themselves positively reflected can be an added layer of encouragement and reinforcement.
Third Recommendation: Build Community Engagement
Building community partnerships was a leading consensus of Summit participants. Establishment of trust and the sharing of knowledge, experience, and perspectives can only come from inclusion of community stakeholders, including residents. With a shared mission and pooled resources, the process of successfully creating a health equity infrastructure that extends beyond the clinic to the greater community can start and build momentum for larger positive societal change.
The importance of collaboration with local government agencies, social workers and community navigators, while engaging with potential partners within health and food industries, housing, childcare, and transportation, were noted as important steps toward identifying and tackling barriers to successful lifestyle medicine initiatives. Potential partners also include churches and places of worship, YMCAs, FQHCs, and other community centers, as well as school systems. Partnering with food establishments, such as food banks, grocery stores, and restaurants may be advantageous in working toward resolving issues of food insecurity, so families not only have access to enough food, but, more importantly, food that is nutritious and palate-pleasing. 48 In some communities, creative programs now exist for ride sharing and food pick-up locations for those without easy access to transportation.
Summit participants acknowledged the immense influence of select local leaders and community stakeholders, for example, churches and barbershops, as well as local chapters of national organizations representing people of color, including sororities, fraternities, NAACP, and HBCUs. This is another angle where partnerships can work toward narrowing health disparities. These trusted groups have a unique ability to influence culture and change norms at multiple levels, as they amplify and reinforce lifestyle medicine recommendations for reducing health disparities. For example, buy-in for nutrition literacy and food skills could be increased by having a men’s prayer breakfast be the setting for bringing in a local chef influencer to share tasty food that is healthy, affordable, and easy to prepare.
The success and challenges of community partnerships must be analyzed and recorded to provide data to push for local policy changes that fund and support similar culturally tailored outreach and program development across other communities. The Community-Based Participatory Research (CBPR) approach is recommended here because the collaboration between the community, involved organizations, and the research group encourages identification of problems relevant to the community, culturally appropriate problem solving, and a more personalized approach to the unique needs of a community. 9 Given the community participants are partners in the research, the benefits for them can be achieved sooner and with a stronger result. With meaningful participation at all stages of program development and evaluation, the unique circumstances of different communities can be addressed with a menu of options to ensure success of the lifestyle medicine initiatives.
Care will be needed not only to build upon success but also to address potential barriers at all points, from initial pilot program to ongoing program evaluation and long-term growth and sustainability. Research in racism, which many historically marginalized communities face, shows multiple paths that can impact health, including decreased access to jobs, homes, and education, adverse mental and emotional health, increased allostatic load with pathologic stress, decreased healthy behaviors, and increased unhealthy behaviors. 49 It is critical CBPR cultivates individual and systemic change that becomes operationalized, contributing within communities and organizations to improved health equity.
Summit participants noted that many organizations are already working in the nutrition food space, including Cooking Matters, which incorporates volunteer chefs, dietitians, and other experts to teach food skills to families at risk for hunger, so they can maximize food resources and learn to prepare healthy meals. 50 Research showed success at three and six months with participants’ confidence and ability to stretch food dollars and WIC foods farther with their programs like hands-on cooking classes and grocery store tours. 51 Another robust, successful food literacy program is the Culinary Literacy Center at the Free Library of Philadelphia, 52 with 30 teaching kitchens across the city. Its programs teach math and language through kitchen activities. Hungry Harvest is another example of an organization working to lower food waste and help reduce food insecurity. 53
Two other important resources were noted: Michelle Obama’s initiative, Partnership for a Healthier America, which is focused on changing the food landscape to achieve health equity by working with the private sector across the supply chain and with other nonprofit organizations. 54 Another program was an online, culinary education program called Swich—offered free-of-charge—with a bold vision of teaching more than 100 million people how to cook and how to make the shift to a whole food, plant-predominant dietary lifestyle. 55
Building trustworthy, long-term partnerships within a community to work towards a shared goal is central to creating successful and lasting change. Members of a community know best what their unique needs are, including what issues should be prioritized. Community members also provide invaluable insight about the strengths and weaknesses of previous programs and practices that may have worked well or fallen short of expectations. Therefore, for any lifestyle medicine-focused initiative to truly benefit a community, the collective voice of its members must help shape its development at every stage from planning to implementation and evaluation.
Fourth Recommendation: Advocate for Policy change
The year 2020 marked the 35th anniversary of the Report of the Secretary’s Task Force on Black and Minority Health, widely known as the Heckler Report, released in 1985 under the leadership of then-U.S. Department of Health and Human Services Secretary Margaret Heckler. The Heckler Report, which documented persistent racial and ethnic health disparities, and outlined recommendations to reduce them, marked the first time the US government attempted to comprehensively examine the health status of racial and ethnic groups. In the decades since, consequential federal efforts to promote health equity, from establishment of the National Center on Minority Health and Health Disparities within the National Institutes of Health (NIH) to the Affordable Care Act, each traceable to the Heckler Report, have been made.
However, health disparities persist and, while overall health is improving, inequalities are worsening. The Summit vision statements were constructed as direct response to the mechanisms behind these gaps. Summit attendees also emphasized that the leadership, sustained investment, societal commitment and action, and meaningful empowerment of individuals, and communities required to achieve health equity will not be fully realized without expansive policy change. Gaps between health disparities objectives and policy, and between policy objectives and programs—and measures meant to achieve them—impact everyone; although, like disparities in health care access and quality, the burden of the impact is disproportionately placed on communities of color.
An illustrative case is the Dietary Guidelines, updated jointly by the U.S. Departments of Agriculture (USDA) and Health and Human Services (HHS) every 5 years. The Guidelines, most recently updated just after the close of the HDSS in December 2020, dictate federal nutrition policies and form the basis for nutrition education efforts and governmental food assistance programs including the National School Lunch Program, the Elderly Nutrition Program, the Food Distribution Program on Indian reservations, the Supplemental Nutrition Assistance Program (SNAP), and the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC). Even at the close of a pandemic-riddled year that saw the greatest pains stemming from the systemic impacts of racism on food security and the needs and vulnerability of people living with chronic diseases, the Guidelines update did not take the opportunity to recommend optimal nutrition for prevention of chronic disease or address health disparities. This is despite expert commentary from leading authorities and physicians urging the USDA and HHS to ensure the 2020–2025 guidelines “indicate that dairy products are unnecessary and warn of their particular health toll on people of color,” 56 and a 2018 American Medical Association 57 resolution recognizing that lactose intolerance is common among many Americans, especially Black, Indigenous, and People of Color (BIPOC) Americans.
For lifestyle medicine, specifically the nutrition pillar that advocates for a whole food plant-predominant eating pattern, to reach all Americans—especially those who most acutely experience the costs of lifestyle-related chronic disease—the safety net programs for those experiencing food insecurity must no longer be influenced by industry lobbies and must be based on inclusive research with attention paid toward cultural competence and relevance. As long as the status quo remains, those who point to the incongruity of prescribing lifestyle medicine to those experiencing hunger will be identifying a true tension at best, an insurmountable barrier to avoiding lifestyle-related morbidity at worst.
To achieve lasting change that reduces disparities of health, the Summit members recommend public policy innovations that improve population health by addressing the social determinants of health that will have the greatest impact. 58 This includes reducing segregation and improving the social and physical conditions of the neighborhoods, workplaces, and schools of underresourced communities. 59 By addressing health care and the larger picture of what impacts health, the disparities in health seen from zip code to zip code can be reduced. 60
At the national level it is important to garner champions in government organizations like Congress, CMS, the FDA, the Office of Minority Health and the Covid-19 Health Equity Task Force by developing relationships and educating them about the valuable role of lifestyle medicine in reducing the health disparities that vulnerable communities face. 61
Making inroads at the state and local levels to gain the strength needed to push for policy change is also critical. There are more than 3000 community health departments with preventive health professionals whose number one goal is chronic disease prevention. Massachusetts has implemented a Food is Medicine State Plan Roadmap–a multifaceted approach to connect nutrition services to residents with the goal of preventing and treating diet-related illness—a creative approach that could be replicated in other states. Its key pillars include patient screening, provider nutrition education, a patient referral system, community -based nutrition organizations (CBOs) and a sustainable funding model. 62 Following their progress closely will be important to learn what is appropriate and replicable in other states.
There are other potential allies: The Food is Medicine Coalition (FIMC) is a group of non-profit, medically-tailored food and nutrition services providers nationwide that advocate for public policy supporting access to food and nutrition services for people with critical and chronic illnesses. 63 There are multiple creative ideas to promote better access to nutrition, as well as to create jobs, for example, supporting plant-based agriculture with government investment in community-owned food cooperatives, as the federal government has done before with the Fresh Food Financing Commission. 21
Summit participants discussed the potential in working with health care payers, including public and private health insurers, provider organizations like the AMA, and hospital health systems and community health centers to find ways where these groups can utilize favorable reimbursement models to enable healthy eating and health outcomes. Payment models that are practical need to be explored, advocating for reimbursement of lifestyle medicine shared medical appointments at sites that are most convenient for patients, 64 such as YMCAs, community centers, churches, teaching kitchens, grocery stores and library sites, rather than only at Place of Service authorized clinical sites. This would better enable clinicians to meet the needs of the community and provide services that are reimbursable. An example of corporate social responsibility is Cigna Foundation’s initial steps with a pilot to explore social determinants of health and health outcomes to influence reimbursement. 65
As important as education of clinicians and empowering patients, discussion of policy change must involve recognition of where the relevant power lies, and the type of collective action required to see the policy landscape shift. Cross-disciplinary voices like those convened at the Summit—the voices of patients, doctors, nurses, researchers, and faith-based organization leaders—are vital. Stories must be shared at the local, state, and national levels, reaching those in position to effect change, compelling them to catch the vision of the vital need for lifestyle medicine to become the foundation of health and all health care. This is essential in our quest to address lifestyle-related chronic disease health disparities.
The inaugural HDSS, produced by ACLM’s HEAL Initiative, was an initial and important step in convening thought leaders to identify expert-recommended action steps ACLM and other organizations can and should take to boldly address the lifestyle-related chronic disease health disparities that are ravaging our underserved communities. Lifestyle-related chronic disease, disproportionately prevalent in our communities of color, not only heightens vulnerability to infectious disease and its most harmful effects, but, in and of itself, robs years from lives and life from years, while taking an incalculable economic toll. The time for action is now.
Conclusion
The American College of Lifestyle Medicine (ACLM), through its Health Equity Achieved through Lifestyle Medicine (HEAL) Initiative, is committed to addressing the issues chronicled herein and action steps outlined above. Building upon the work of many organizations that have long been on the forefront of tackling the multifaceted issues driving health disparities, ACLM, and the lifestyle medicine-trained clinicians and health care leaders it represents, have the opportunity and responsibility—in light of their unique area of expertise—to address the facet of health disparities specific to lifestyle-related chronic disease.
This timely inaugural HDSS brought together researchers, health care professionals, clergy, and community leaders, not only to spark important conversations, but to also unite the larger lifestyle medicine community to become a galvanized force for change, advocating for health equity.
Summit participants agreed that the time is now to identify and eradicate the root causes of the chronic diseases that are disproportionately impacting our underserved communities. There was consensus that lifestyle medicine is the needed foundation of a transformed and sustainable system of health care delivery, bringing health, hope, and healing to ALL people.
Sidebar: HDSS Featured guests
In addition to the distinguished panelists who participated in the Health Disparities Solutions Summit, each of the three summit sessions showcased an honored guest: the 17th U.S. Surgeon General Richard H. Carmona, U.S. Congresswoman Robin L. Kelly (D-IL 2nd District), and Brooklyn Borough President Eric Adams. Each shared enlightening remarks through the lens of lifestyle-related chronic disease health disparities, emphasizing the importance of lifestyle medicine as an essential component of a comprehensive solution.
17th Surgeon General of the United States Richard H. Carmona, President of the Canyon Ranch Institute
Having served on ACLM’s Board of Advisors since the College’s inception, Dr. Carmona is a foremost champion of lifestyle medicine, opening his summit remarks by saying, “ACLM is just what the doctor ordered.”
Sharing his personal story of being born in New York City to Puerto Rican immigrants and raised in Harlem, Dr. Carmona grew up in an underserved community and knows too well the realities its residents face. These life experiences elevated his passion to eradicate health disparities. He never lost sight of where he came from and is dedicated to supporting struggling communities. “The remedies are as much social as they are medical,” said Carmona. “We need to connect with people to give them hope. To get people past despondency. From criminality and unemployment to finding their purpose.”
Acknowledging the realities of SDOH, Carmona said, “Food deserts are real, too many people are living day to day, paycheck to paycheck. We cannot allow the zip code where someone lives be the foremost determinant of health.”
“We are spending close to 19% of our GDP on sick care,” said Carmona. “Most of these dollars pay for treatment of preventable disease. The government can’t buy its way out of these problems or ignore them. The only solution is lifestyle medicine—modifying lifestyle to reduce disease burden.”
Asked for his advice regarding lifestyle medicine advocacy, Dr. Carmona replied “The people who have a great deal of power are the congressional staffers. Cultivate relationships with health policy staff leads, as they are helping to determine the legislative agenda. Identify the relevant committees, noting ACLM member connection to committee members. Build relationships over time. Become a trusted source of information so you’re looked to as a subject matter expert—someone who has the pulse of the community. Pursue a nonpartisan approach, because lifestyle medicine is for all people.”
Reflecting on work he led in the aftermath of Hurricane Katrina, he recalled reaching out to the faith-based community: a group of ministers who met on a regular basis, recommending this approach in regard to addressing lifestyle-related chronic disease health disparities. “In good times and bad times, people have their faith. Engage these leaders in a way that begins to build trust. Motivate, gain credibility, and earn the privilege to serve them and their congregations at a higher level.”
“Don’t forget the power of a story,” emphasized Carmona. “You have a powerful story to tell. Thank you (ACLM and HEAL) for the work you do and the commitment to make the country better and to give people the chance to achieve their dreams.”
Congresswoman Robin L. Kelly
Representative Kelly, who is chair of the Congressional Black Caucus Health Braintrust, is deeply entrenched in addressing issues of health equity and was quick to affirm her support of the need for a lifestyle medicine-first approach to health care, noting “I wholeheartedly support your efforts and agree that food is medicine.” Since the 2015 publication of her Kelly Report on Health Disparities in America, she has been working, in her words, to “turn recommendations into policy.” 67
“We know that the system is complicated and baked in. Food deserts, type 2 diabetes prevalence, and life expectancy maps overlap,” said Kelly. “In order to craft good policies, we must understand the Social Determinants of Health—what I often refer to as the Social Determinants of Life—as the root causes.”
In her Kelly Report, she emphasized “The whole can only ever be as healthy as its parts. For America to achieve true health equity, lawmakers, community leaders, and industry stakeholders must come together to reduce disparities and improve health outcomes nationwide. We all have a part to play in creating a healthier America.”
Her Summit remarks echoed this call to action, urging ACLM and its HEAL Initiative Members to “send letters or emails to congressional leaders and committee chairs,” adding, “Stories change hearts. Democrats, Republicans, Independents—let them all know what’s going on, because you are the medical professionals. We have doctors, nurses, dentists, and other clinicians in Congress. They, and our other congressional leaders, want to hear from you.”
Brooklyn Borough President Eric Adams
Borough President Adams is a living, breathing testimony about the healing power of lifestyle medicine. He shared with Summit panelists that his turning point came when he had stomach pain, ulcers and was in a crisis condition with type 2 diabetes, having lost sight in one eye, with vision waning in the other. He had tingling in his hands and feet and faced the painful reality that neuropathic nerve damage too often leads to amputation. He found himself taking multiple medications, with his physician—at the time—explaining that he was genetically predisposed and should accept a lifetime of disease management.
“Instead of living with diabetes, I was determined to find another way,” Adams said. “My search led me to the lifestyle medicine physicians who are championing treatment and reversal of type 2 diabetes and other chronic conditions. Dr. Caldwell Esselstyn invited me to meet with him and, at 56 years old, I was hearing new terminology about the steps I could take to reverse my chronic disease.”
Adams noted that, “At first, the concept of reversing my disease seemed far-fetched. But, after three weeks of following a whole food, plant-based diet, my ulcers went away. In three months, I’d lost 35 pounds, the neuropathy was gone, and my A1C dropped from the teens to prediabetic levels. I discovered that the fountain of youth is food—using food as medicine.”
“It’s not your DNA, it’s your dinner” is his response when anyone expresses their belief that they are victim to their genes in regard to their health destiny.
Emphasizing that we must turn “pain into purpose,” Adams’ recommendations include advocating for medical professionals to be trained in lifestyle medicine and clinical nutrition. He’s actively promoting whole food, plant-based menus in schools, removing processed meats, and expressed hope in seeing hospitals and correctional institutions change their menus to reflect more plant-forward offerings.
Adams was enthusiastic in acknowledging nutritional psychiatry, saying that “It’s showing the connection between the foods we eat and mental health. Food impacts our entire bodies, including our hearts, kidneys, and lungs. Now we’re looking at the brain—how well our heart beats and how well our minds think. It’s encouraging!”
Adams takes pride in the work being done at Brooklyn’s Bellevue Hospital—the oldest hospital in America noting his outstanding partnership with Michelle McMacken, MD, DipABLM, a member of ACLM’s Board of Directors, who leads the hospital’s Plant-based Lifestyle Medicine Program.
In closing, Adams said, “We’re on a mission. We’ll lean into this and advocate for lifestyle medicine for all people. Thank you (ACLM and HEAL) for what you’re doing. You’re saving lives.”
Summit Panelists & Support Staff
Arefa Cassoobhoy, MD, MPH, Chief Medical Editor and VP of Medical Affairs, Everyday Health Group
Catherine Collings, MD, MS, FACC, DipABLM, President, American College of Lifestyle Medicine; Director at Lifestyle Medicine Silicon Valley Medical Development
Marsha-Gail Davis, MD, American College of Lifestyle Medicine Board Young Director and Health Equity Achieved through Lifestyle Medicine (HEAL) Initiative Co-chair; Primary Care Internal Medicine Physician at Piedmont Atlanta Hospital
Kofi D. Essel, MD, MPH, FAAP, Director of the GW Culinary Medicine Program, The George Washington University School of Medicine and Health Sciences; Pediatrician at Children's Health Center Anacostia
Nicole Farmer, MD, Research Physician, National Institutes of Health Clinical Center
Anthony Iton, MD, JD, MPH, Senior Vice President of Healthy Communities, The California Endowment
Michael Jones, Sr., Senior Pastor, Friendly Temple Missionary Baptist Church
Janani Krishnaswami, MD, MPH; Founding Co-Chair, American College of Lifestyle Medicine Community Engaged Member Interest Group; Program Director, University of Texas Preventive Medicine Residency Program
Radha Muthiah, President and CEO, Capital Area Food Bank
Monique Rainford, MD, FACOG, Assistant Clinical Professor, Yale University School of Medicine
Joseph Ravenell, MD, Associate Professor of Population Health and Medicine and Associate Dean for Diversity and Inclusion, NYU Grossman School of Medicine
Yumi Shitama Jarris, MD, MPH, Associate Dean of Population Health and Prevention, Georgetown University School of Medicine
Dexter Shurney, MD, MPH, MBA, FACLM, DipABLM, Immediate Past President, American College of Lifestyle Medicine; Senior VP and Chief Medical Officer, Adventist Health Well-being Division and the Blue Zones Institute
Theresa Stone, MD, FACP, American College of Lifestyle Medicine Board Member and Health Equity Achieved through Lifestyle Medicine (HEAL) Initiative Co-chair; Program Director of the Fresh & Savory Culinary and Lifestyle Medicine, Medstar Health at Lafayette Centre
Jasmol Sardana, DO, FACLM, DipABLM; Founding Co-chair, American College of Lifestyle Medicine Community Engaged Member Interest Group; Internal Medicine and Lifestyle Medicine Physician, Barnard Medical Center
Susan Topping, Senior Director of Food, Policy and Impact, Capital Area Food Bank of DC
Kim Allen Williams, MD, FACC, FAHA, MASNC, FESC, Past President, American College of Cardiology; Chief of the Division of Cardiology, Rush University Medical Center
Susan Benigas, BS, Executive Director, American College of Lifestyle Medicine
Monica Black Robinson, BS, HDSS Project Manager; Diversity Equity & Inclusion Professional, Washington University
Samantha Gallion, BS, MA, Grants Development Manager, American College of Lifestyle Medicine
Claire Wade-Hak, RDN, DipACLM, Former Director of Membership, American College of Lifestyle Medicine
Supplemental Material
Supplemental Material, sj-pdf-1-ajl-10.1177_15598276211052248 - Building Health Equity: Action Steps From the American College of Lifestyle Medicine’s Health Disparities Solutions Summit (HDSS) 2020
Supplemental Material, sj-pdf-1-ajl-10.1177_15598276211052248 for Building Health Equity: Action Steps From the American College of Lifestyle Medicine’s Health Disparities Solutions Summit (HDSS) 2020 by Arefa Cassoobhoy, Jasmol J. Sardana, Susan Benigas, Jean Tips and Alexandra Kees in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
The authors wish to acknowledge the generous support provided by the Ardmore Institute of Health to address lifestyle-related chronic disease health disparities with particular emphasis on inequities impacting dietary lifestyle and stress in historically marginalized communities.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.