
Abstract
Keywords
“Lifestyle medicine education continues to expand in response to global healthcare challenges associated with lifestyle-related non-communicable diseases”
Introduction
Lifestyle medicine is an emerging evidence-based speciality, which combines science and application of healthy lifestyles for the prevention and treatment of chronic diseases. 1 Its foundations are embedded in key health behaviours strongly linked to chronic disease: Stress management; Nutrition; Sleep; Physical Activity; Risky Substance Use; and Social Connections.2-4 There is consensus that lifestyle medicine knowledge is essential for healthcare professionals to counsel their patients on prevention of non-communicable diseases and risk factor management,5,6 and should be an essential component of medical and health sciences education moving forward. In 2017, the American College of Lifestyle Medicine and the American Medical Association House of Delegates passed a resolution supporting the incentivisation and provision of funding for the inclusion of lifestyle medicine and education on the social determinants of health in medical education, with the aim of addressing the expanding healthcare costs associated with lifestyle-related non-communicable diseases. 5 Internationally, there is a movement to transform medical education curricula for its inclusion.5,6 However, conventional health care systems are not fully receptive to lifestyle medicine education in medical schools as it requires extra training and resources in already crowded medical curricula.7,8
Educators of future health professionals have a responsibility to equip students with lifelong personal skills to manage their own wellbeing and mental health whilst working in demanding clinical roles. Burnout in healthcare is a common occurrence, and has three key features: overwhelming exhaustion, feelings of cynicism and detachment from the job with health professionals reporting little time for self-care or an appropriate work-life balance.9-11 Poor work-study balance and burnout is also an issue in medicine and health sciences education, with burnout in medical students associated with general distress, poor academic performance, dropout, substance use and suicidal ideation.12-15
Given the academic demands of medical and health sciences education, students can foster unhealthy lifestyle behaviours, which may in turn impact on their health and wellbeing. They report inadequate training in healthy lifestyle behaviours to firstly support their wellbeing in undergraduate education, and secondly to develop healthy lifestyles for navigating future high-stress careers.2,5,7 Medical students who are taught lifestyle medicine reported in quantitative surveys improved personal health behaviours and wellbeing, and an understanding of lifestyle management.1,3,5,7 Students surveyed also report feeling better prepared for future clinical practice: their acquired knowledge qualified them to actively set goals with their future patients, 7 and they agreed that lifestyle medicine is an important contribution to the curriculum.1,7
At RCSI, students are currently taught elements of lifestyle medicine as part of their core curriculum, for example, smoking cessation counselling skills training 11 and resilience skills training 11 ; however, more specific lifestyle medicine training was considered a valuable addition to student learning. As part of the RCSI ‘Good Health and Wellbeing’ initiatives for students, the RCSI Certificate in Lifestyle Medicine was developed as an intensive educational course to give students evidence-based knowledge and practical strategies (1) to instill healthy lifestyle behaviours in themselves; and (2) to support implementation of healthy lifestyle behaviours in their future patients. The course is an optional extracurricular activity delivered online over one academic year through recorded lectures, Multiple Choice Questions (MCQs), knowledge checks, and written reflective assignments.
Previous studies have surveyed students and reported quantitative data regarding their attitudes to lifestyle medicine education.2,4,7,9,11–14 We aimed to build on existing knowledge by conducting an in-depth qualitative examination of student beliefs on the impact of lifestyle medicine education. We conducted a qualitative analysis of student feedback on their experience of completing the RCSI Certificate in Lifestyle Medicine, in terms of impact on their own health behaviours, and preparation for clinical practice. We also wanted to examine students’ experience of an e-learning pedagogical approach to lifestyle medicine, and their recommendations for how to further optimise course delivery to enhance the quality of lifestyle medicine training in our institution.
Methods
Study Design
This was a cross-sectional, retrospective qualitative study. Ethics approval was granted by the Research Ethics Committee at RCSI (REC No.: 202211028). The aim of this study was to evaluate student feedback from the RCSI Certificate in Lifestyle Medicine. An inductive qualitative study approach was used for an in-depth understanding of students perceptions of course participation from a constructivist research paradigm.16,17 Reflexive inductive thematic analysis of free-text comments was conducted. Thematic analysis of free-text comments is a valid qualitative methodology for studies of this nature and data type. 18
Context and Participants
The RCSI Lifestyle Medicine Certificate
The RCSI Certificate in Lifestyle Medicine was developed to equip students with evidence-based knowledge and practical strategies to help them develop healthy lifestyle behaviours and understand the importance of personal health and wellbeing in their future professional lives. Course content was developed based on 6 topics covering 5 of the pillars of lifestyle medicine, namely (1) Stress Management; (2) Nutrition; (3) Physical Activity; (4) Sleep; (5) Smoking Cessation; (6) Alcohol and Substance Use. Students are awarded a Certificate upon completion and a note of the achievement is included on the student’s graduating transcript. The course is open to programmes in undergraduate and graduate Medicine, Pharmacy, Physiotherapy, and Physician Associate students, postgraduate research students, and some staff with student-facing wellbeing roles, including Student Services and the RCSI gym staff.
Participants
The first (2020-2021) and second (2021-2022) cohort of students provided feedback in free-text comments on their experience of the course and suggestions for improvement, its helpfulness in encouraging them to make lifestyle changes, and their use of lifestyle medicine in future professional practice. All students who completed the course evaluation were invited to participate voluntarily in the study by providing informed consent to have their course feedback included in qualitative data analysis.
Data Collection
Students were emailed a Microsoft forms link by the course coordinator, NC, which contained a participant information leaflet and consent form. Consenting students received a copy of their signed documents for their records. The course was evaluated using free-text comments across seven domains – (1) study materials; (2) online mode of delivery; (3) course support; (4) final assignment support (5) areas of support requiring improvement; (6) areas of behaviour change; (7) overall course recommendations. Students completed their evaluations on MS Forms and, following receipt of informed consent, anonymised data were imported to NVivo 12TM.
Data Analysis
Reflexive inductive thematic analysis was conducted using NVivo 12TM. An inductive approach was chosen to allow themes and patterns to emerge naturally, rather than being limited by pre-existing theoretical frameworks. Reflexive analysis acknowledged the data analyst’s potential subjectivity in data interpretation. 19 Thematic analysis was conducted using Braun and Clark’s six-phase analysis process20,21: (1) the researchers firstly familiarised themselves with the data by thoroughly reviewing student feedback. (2) CD and LM coded the data separately before meeting to discuss findings; following this, another round of coding was conducted to reflect suggested amendments. A meeting was later convened with a third reviewer, SD, who reviewed predicted codes and supported their finalisation. (3) Potential themes were proposed and tested for relevancy by sampling quotes against suitable codes. (4) To ensure better data representation, themes were edited and quotes were re-applied to suitable codes and tested for accuracy. (5) Themes were then reviewed to match code descriptions. (6) All themes were finalised and represented using quotes from student data. Reflexive practice was central to data analysis as one researcher, LM, was involved in course development and delivered an online module within the course. Open dialogue and consideration of personal assumptions was engaged with throughout. 22
Results
Between 2020 and 2022, 305 students and 5 RCSI staff completed the RCSI Certificate in Lifestyle Medicine: 85% from Medicine; 9% from Pharmacy; 4% from Physiotherapy; 2% were RCSI staff. Of those, 32% (n = 98: 83 Direct Entry Medicine; 15 Graduate Entry Medicine) gave consent for retrospective analysis of their course evaluations. Eighty-one percent of study participants reported trying to change a health behaviour while completing the course, with 97% attempting to change more than one health behaviour. The following themes and sub-themes were identified (Figure 1). Themes and sub-themes identified through thematic analysis.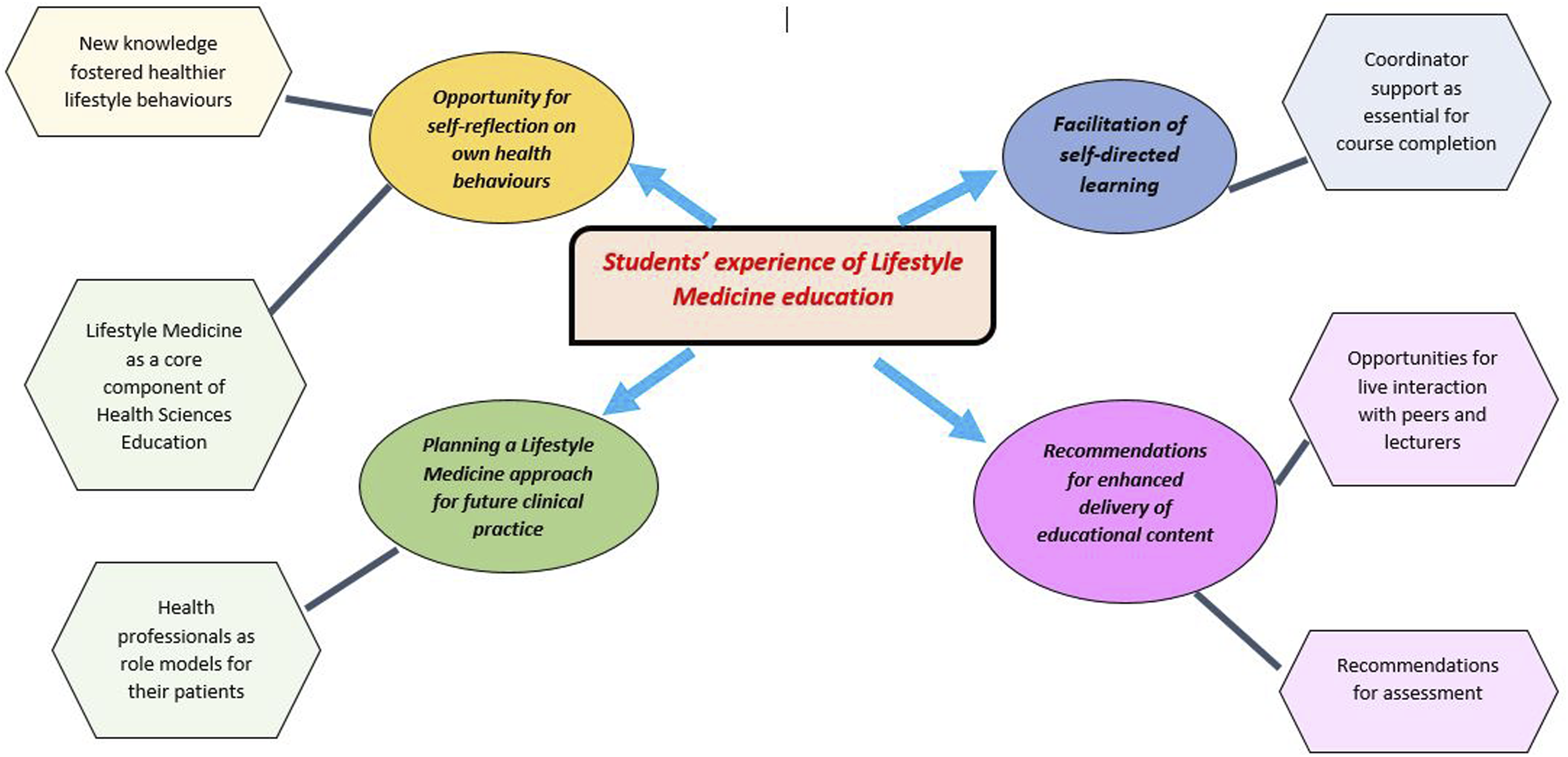
Opportunity for Self-Reflection on own Health Behaviours
Students described the RCSI Certificate in Lifestyle Medicine as providing space for self-reflection on their own lifestyle and health behaviours. The ability to review their lifestyle from the whole-system perspective allowed insight into their current lifestyle, and thus they felt ‘motivated to adopt healthier habits’, meaning that the opportunity to pause and reflect inspired them to take action to improve their health and adopt healthier habits in their daily routine: ‘I am now more conscious of the things I want to change, how they impact me, and where to find helpful resources when I decide to focus on changing those aspects of my life’
Following course completion, students emphasised that they had a new understanding of the importance of their own health, and how personal lifestyle behaviours could support good health: ‘I have become more aware of my health and I have started trying to lead a more active lifestyle’
New Knowledge Fostered Healthier Lifestyle Behaviours
Following education in lifestyle medicine, students had new awareness of the power of lifestyle behaviours, and were motivated to integrate this new knowledge into their own lifestyle: ‘Taking the course and learning about the incredible benefits of exercise and physical activity definitely motivated me to take serious action to improving my physical health’
Students provided examples where they recognised after course completion, that certain behaviours were having a negative impact on their health and required specific attention: ‘My sleep became a lot better after I became more educated around this subject’
They particularly appreciated evidence-based and practical strategies, such as 10 000 steps per day and sleep hygiene techniques to help with ‘consistently reaching the goal’ that they set for behaviour change. Importantly, students regarded drastic changes as ineffective for longer-term behaviour change, and instead perceived small, consistent goals as key to successfully implement long-term lifestyle changes: ‘The modules gave great insight to the positive health benefits associated with small lifestyle changes’
Planning a Lifestyle Medicine Approach for Future Clinical Practice
Students gained an appreciation for using a lifestyle medicine approach to treat chronic disease in clinical practice with their future patients, through recognition of ‘the magnitude of the effect lifestyle aspects have on [our patients’] lives’. Students gained insight into treating patients through biopsychosocial lens, recognising that common chronic diseases ‘come almost entirely from a lifestyle medicine point of view’, and therefore they planned to integrate evidence-based lifestyle medicine recommendations into their future interactions with patients: ‘As future doctors, it is important that we are well equipped with the knowledge and skills to provide advice, encourage and coach our patients in successfully making necessary lifestyle changes to improve their health and help them lead healthier lives’
Importantly, students recognised that using lifestyle medicine in practice requires an individualised approach and consideration of barriers that may prevent patients from implementing positive lifestyle changes: ‘The course is a must for all healthcare professionals to understand potential barriers to improved outcome measures for patients’
Lifestyle Medicine as a Core Component of Health Sciences Education
Students advocated for an emphasis on lifestyle medicine education within their core curricula, viewing it as a ‘fundamental part’ of their future careers in order to develop a holistic clinical skillset: ‘I think it’s a really important part of our education as healthcare providers especially [as] the most threatening diseases in hospitals result from lifestyle factors’
Health Professionals as Role Models for Their Patients
Completing the RCSI Certificate in Lifestyle Medicine gave students an opportunity to foster better empathy for patients by reflecting on how difficult health behaviour change can be to implement consistently. Through attempting to make changes in their own lives, students felt they gained ‘insight into certain patient struggles’. In turn, they reflected on how, by practicing a healthy lifestyle themselves, they can ‘set an example’ for their patients; which motivated them to prioritise their own health during stressful periods in the academic year: ‘It gives insight on how we as healthcare professional(s) can change our own unhealthy habits to be better role models for our patients’
Facilitation of Self-Directed Learning
Students reported satisfaction with the style of online content delivery that allowed them to utilise self-directed learning, which was scaffolded by the paced release of course content over the academic year. The online method of delivery permitted students to fit the course in with their ‘changeable’ demanding college workload: ‘[It] was very enticing that the module could be done in our own time- makes the module very accessible to all lifestyles’
Coordinator Support as Essential for Course Completion
As this was an online, extracurricular activity where students studied alone in their own time, the importance of accessibility and support of the course coordinator was flagged. They highlighted their appreciation for the coordinator who was ‘responsive of queries and understanding when issues came up’, which allowed them to continue with the course even when academic and personal issues impeded their course engagement.
Recommendations for Enhanced Delivery of Educational Content
For development of clinical skills, students suggested that inclusion of real-life case studies and/or patient experiences the curricula would deepen their understanding of treating patients with chronic disease(s) from a lifestyle medicine perspective. Practical examples would help keep the material relevant for ‘people training to be on the front line’.
Opportunities for Live Interaction with Peers and Lecturers
Although course delivery was fully online, students reported that the occasional opportunity to engage with lecturers and peers would enhance their learning experience. Some students reported feeling isolated when completing the course due to its self-directed nature and suggested arranging student meet-ups to facilitate a learning community, where they could ‘have interaction with other course members/tutors, more collaboration and sharing of ideas’. Students also recommended that ‘live’ sessions with their lecturer during each pillar would facilitate students to ask questions and discuss the content; thus, making the course more ‘impactful’.
Recommendations for Assessment
Overall, course materials were well received, with an appreciation of evidence-based, engaging content and strategies for behaviour change, and signposting to useful resources. For the final assignment, where students developed and monitored adherence to their personal behaviour change plan, students valued having the opportunity to ‘synthesise’ the content. Some students suggested that model answers / further information for the course assignments would help with completing the required assessments, as they noted that the guidelines were ‘open to vast interpretation’ and some students were unclear about what exactly was required.
Discussion
This study sought to conduct a detailed investigation of the impact of the RCSI Certificate in Lifestyle Medicine for health sciences students by qualitatively examining their experiences regarding the role of lifestyle medicine education on their own lifestyle behaviours, their preparation for clinical practice and recommendations for improved lifestyle medicine teaching methods. Our results suggest that the course prompted them to reflect on their health and wellbeing from a holistic perspective and make lifestyle changes in self-identified areas of concern. Our findings also indicate that students recognised the importance of treating lifestyle risk factors for health and intended to adopt a lifestyle medicine approach in their future clinical practice. From a pedagogical perspective, students provided important insights into the value of hybrid learning for an enhanced, collegiate learning experience.
The process of self-reflection in medical education provides space for self-evaluation of beliefs, values and perspectives on professional behaviour and challenges in clinical practice. 23 In this instance, reflective writing as part of continuous assessment fostered the opportunity for students to reflect not only on the role of lifestyle medicine in clinical practice, but more importantly, their own health and wellbeing. Typically, the burdensome nature of a medical curriculum and consequent high stress levels can lead students to adopt unhealthy lifestyle behaviours and coping strategies.24,25 The increasing advocacy for inclusion of lifestyle medicine education in medical schools is commendable; however the focus of the lifestyle medicine curricula is on patient wellbeing and clinical skills,5,26 whereas the primary focus of the RCSI Certificate in Lifestyle Medicine is on healthy lifestyles for the students themselves. We showed impacts on student behaviour through the process of self-reflection on suboptimal health behaviours, in addition to acquisition of new knowledge on the damaging impact of unhealthy lifestyle behaviours on long-term health.
Long-term health behaviour change remains a challenge amongst general populations and chronic disease cohorts, 27 with personal, systemic and environmental challenges identified as barriers to change 28 . Awareness of personal health behaviours has been shown to affect medical students’ competency in preventive counselling with patients, 29 , 30 and in this study, students reflected on their responsibility to be role models to their patients by living a healthy lifestyle. An innovative feature of the RCSI Certificate in Lifestyle Medicine course was a reflective assignment in which students must attempt to change a lifestyle behaviour over a 2-week period and reflect on the barriers and facilitators of this change. In doing so, this helped students identify and experience the challenges faced by patients; they reported that this process significantly impacted their understanding of how to practice with a lifestyle medicine ethos in their future careers. We suggest that education in lifestyle medicine should not only prioritise developing a student’s clinical competencies, but also give them the opportunity to develop empathy through assessments that focus on the lived experience of behaviour change.
There is a global acknowledgement that lifestyle medicine education must be more competency-based 7 and contain experiential teaching with inclusion in the clinical year. In this study, students noted that practical strategies for working with patients and opportunities to practice their communication skills would help to embed the lifestyle medicine approach as a clinical competency. They also requested more real-world case studies that highlight the varying challenges within diverse populations. Lack of skills practice is commonly noted in institutions delivering lifestyle medicine education,5,7 with an institutional curriculum mapping exercise demonstrating a dearth of standardised comprehensive curricula for lifestyle medicine, 6 as 60% of teaching hours are dedicated to theoretical knowledge. For current healthcare professionals, one of the identified reasons for the lack of prescribing of lifestyle medicine was a lack of training. 6 For example, general practitioners managing patients with depression in the community highlight that a lack of education for using lifestyle medicine in practice inhibits confidence in providing optimal care regarding risk factor management and better mental health. 31
Online learning in medical education is regarded as a useful pedagogical method that is now commonly used in healthcare institutions, 32 and face-to-face or virtual delivery has been demonstrated to produce similar levels of lifestyle medicine skills competencies. 33 In this study, whilst the online approach was appreciated by students, interaction with peers and staff was suggested as a way to solidify content and create a community of like-minded students with an interest in lifestyle medicine. This study showed that for enhancement of student wellbeing in addition to lifestyle medicine competencies, a hybrid approach, with a mix of face-to-face and virtual attendance, was proposed by students as an effective way to deliver both theoretical lifestyle medicine content and skills practice in a peer-supported environment, whilst meeting students’ learning expectations.
Limitations and Directions for Future Research
This study gave a retrospective cross-sectional snapshot of the self-reported behaviour change of our students; a baseline measure of their lifestyle behaviours wasn’t assessed, and therefore their perceptions of the influence of lifestyle medicine on their lifestyle may have been affected by recall bias over time. Future iterations of evaluation of the RCSI Certificate in Lifestyle Medicine would be strengthened from an objective, quantitative, pre-course and post-course survey of health behaviours alongside qualitative evaluation. This mixed-methods study design would reflect level 3 assessment of the Kirkpatrick framework for evaluation of training interventions, and facilitate an objective examination lifestyle change directly following course completion. 34 Further, longitudinal follow-up of the student cohort post-graduation as healthcare professionals would enable examination of the long-term implementation experiences of lifestyle changes adopted during the RCSI Certificate in Lifestyle Medicine, as previous research has showed that following lifestyle medicine education, over time unhealthy lifestyle behaviours can re-surface in the student population. 24 Longitudinal data post-graduation would enable the identification of barriers and facilitators to practicing lifestyle medicine in real-world clinical practice; such data would be valuable for the further development of educational content for lifestyle medicine.
Conclusion
Lifestyle medicine education continues to expand in response to global healthcare challenges associated with lifestyle-related non-communicable diseases. The RCSI Certificate in Lifestyle Medicine supports the development of reflective practitioners with greater knowledge and skills in the prevention of chronic disease in both them and their patients. Moving forward, medicine and health sciences curricula must integrate lifestyle medicine education into core teaching via a hybrid learning approach as there is clear recognition from students, as a new generation of health professionals, that a lifestyle medicine approach is paramount to prevention and treatment of chronic disease.
Supplemental Material
Supplemental Material - ‘I Feel Like It was a Springboard for Certain Changes in My Life’. A Qualitative Analysis of Medicine and Health Sciences Students’ Experiences of Lifestyle Medicine Education
Supplemental Material for ‘I Feel Like It was a Springboard for Certain Changes in My Life’. A Qualitative Analysis of Medicine and Health Sciences Students’ Experiences of Lifestyle Medicine Education by Lisa Mellon, Cheyenne Downey, Niamh Corbett, Sally Doherty, Mary Clarke, Frank Doyle, Caroline Kelleher, Aisling O’Neill, Maria Pertl, Anne Hickey in American Journal of Lifestyle Medicine
Footnotes
Author Contributions
LM was responsible for the design of the study, data analysis and manuscript writing. CD was responsible for data analysis and manuscript writing. NC was responsible for data collection and manuscript writing. SD was responsible for data analysis and manuscript writing. MC, FD, CK, AON, MP were responsible for manuscript writing. AH was responsible for design of the study and manuscript writing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Consideration
Ethics approval was granted by the Research Ethics Committee at the RCSI University of Medicine and Health Sciences (REC No.: 202211028)
Data Availability Statement
Data sharing is not applicable to this study as qualitative data holds potentially identifiable information.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.