
Abstract
The actual causes of premature adult deaths, the preponderance of noncommunicable chronic diseases, and their associated costs are related to unhealthy behaviors, such as poor nutrition, physical inactivity, and tobacco use. Although recommended as the first line of prevention and management, providers often do not provide behavioral change counseling in their care. Medical education in lifestyle medicine is, therefore, proposed as a necessary intervention to allow all health providers to learn how to effectively and efficiently counsel their patients toward adopting and sustaining healthier behaviors. Lifestyle medicine curricula, including exercise, nutrition, behavioral change, and self-care, have recently evolved in all levels of medical education, together with implementation initiatives like Exercise is Medicine and the Lifestyle Medicine Education (LMEd) Collaborative. The goal of this review is to summarize the existing literature and to provide knowledge and tools to deans, administrators, faculty members, and students interested in pursuing lifestyle medicine training or establishing and improving an LMEd program within their institution.
‘. . . Medical education in lifestyle medicine is… a necessary intervention to allow all health providers to learn how to effectively and efficiently counsel their patients toward adopting and sustaining healthier behaviors.’
Background
By 2020, the World Health Organization predicts that two-thirds of all disease worldwide will be the result of lifestyle choices. 1 In the United States, the primary causes of premature adult deaths are related to unhealthy behaviors, such as tobacco use (18.1%) and poor diet and lack of physical activity (15.2%). 2 These findings are widely accepted, and well-established chronic disease practice guidelines uniformly call for behavior change as the first line of prevention and management.3,4 However, physicians often do not follow these recommendations.5,6 A recent survey found that only 30% of US health professionals provided exercise counseling during the prior 12 months. 7 Barriers include lack of time, compensation, knowledge, and resources.8,9
Lifestyle medicine (LM) is a burgeoning field, defined in the Journal of the American Medical Association as the “evidence-based practice of assisting individuals and their families to adopt and sustain behaviors that can improve health and quality of life.”10(pp.202) One of the gaps identified for the lack of prescribing LM was a dearth in training; therefore, LM medical education was proposed as a necessary solution. Goals for primary care LM medical education were defined and include competencies in leadership, knowledge, assessment skills, management skills, and the use of office and community support. 10 Although these suggested competencies were developed largely to guide Continuing Medical Education (CME) for primary care and preventive care physicians, educators at both the Undergraduate Medical Education (UME) and Graduate Medical Education (GME) levels were encouraged to incorporate LM into their training programs. 10 LM curricula have begun to be implemented into both UME,11-13 GME, 14 and CME programs. 15 These curricula have been described 16 and found to improve self-perceived attitude, 15 knowledge, 15 and confidence15,17 toward prescribing LM as well as LM counseling,15,18,19 self-care, 18 and patient outcomes. 20
The vision of changing the US environment to a blue zone, 21 the culture that encourages healthy lifestyle, was described recently by Dr David Katz. 22 A necessary part of this cultural evolution is a well-established system of LM medical education. Other professions such as law, business, design, industry, and engineering should be part of this reform and should learn about healthy environments during their training. Thus, both medical schools such as Stanford University 23 and Harvard Extension School 24 introduced LM courses open to the entire campus (Figure 1).
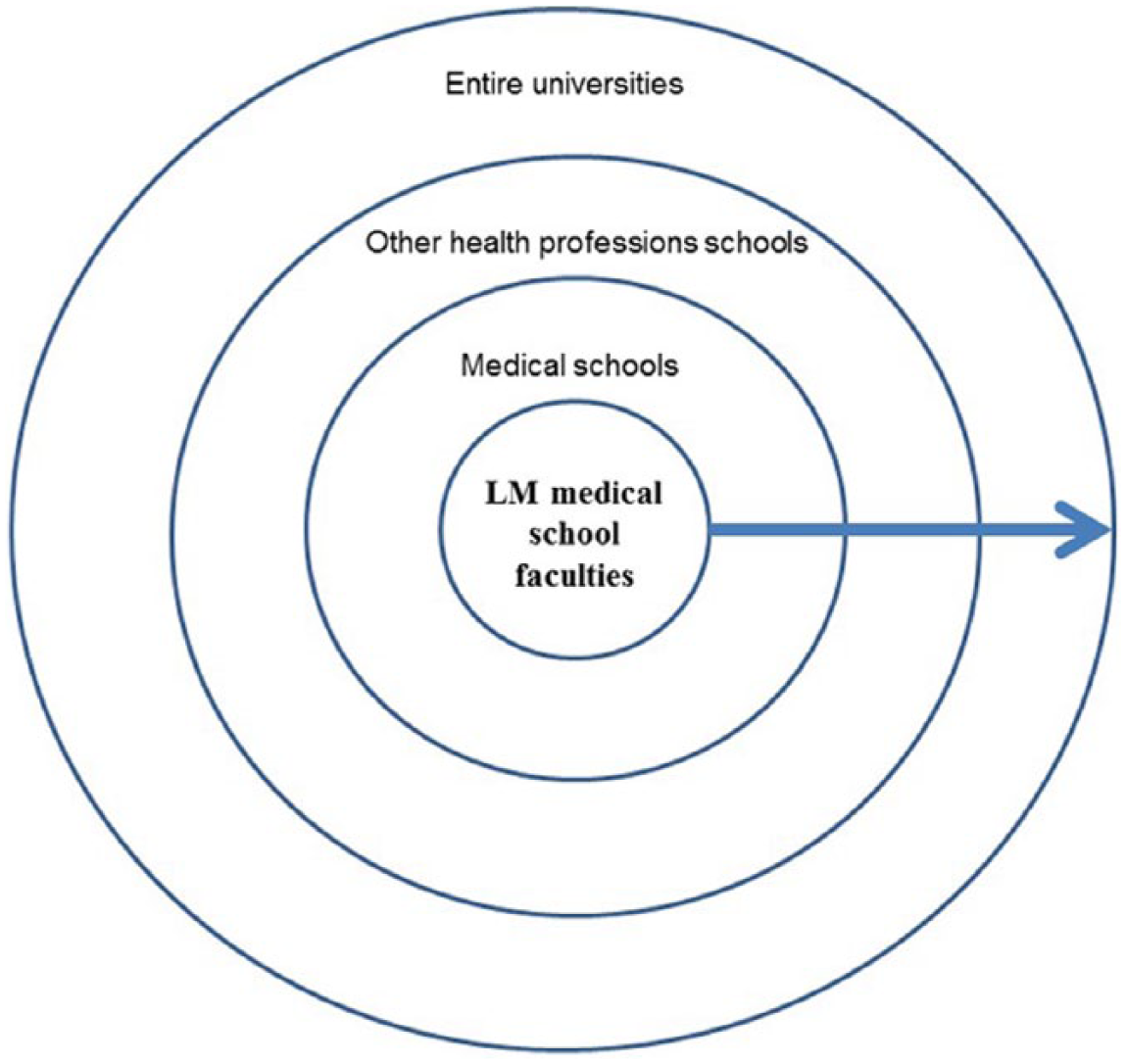
Concentric Circles of Influence. 63
The goal of this review is to summarize the existing LM medical education literature and to provide knowledge and tools to deans, administrators, faculty members, and students interested in pursuing LM training or establishing and improving a LM education program within their institution.
Early Efforts
A lack of formal LM education at the medical school (UME) level was recognized as early as 1975. A survey revealed that only 16% of medical schools offered a course with information specific to exercise as a part of preventive medicine. 25 With regard to nutrition, a survey conducted in 1985 by the National Academy of Sciences found that only 27% of medical schools had a separate, required nutrition course, 26 and subsequent surveys showed little improvement.
The Bipartisan Policy Center convened a symposium and released a report calling for the inclusion of nutrition and physical activity at all levels of medical education, 27 the US National Physical Activity Plan specifically calls for an increase in physical activity education, 28 and the American Society for Nutrition has requested an increase in nutrition education. 29 In 2008, more than a decade after the launch of Nutrition in Medicine (NIM; providing free, interactive, comprehensive nutrition education), 30 just 27% of US medical schools indicated that they provided the 25 hours of recommended minimum nutrition education. 31 Thus, providing LM curricula is a necessary but not sufficient step toward sustainable change, and a more extensive approach must be undertaken to make the needed reform in medical education.
Exercise is Medicine (EIM) is an example of a tangible implementation initiative. EIM was launched in November 2007 by the American College of Sports Medicine together with the American Medical Association. 32 The goal of EIM is to encourage health care providers to assess physical activity as a vital sign and to include exercise when designing treatment plans for patients. The EIM Education Committee released recommendations for graduating medical students’ knowledge and skills in regard to physical activity. 33 Four focus areas were defined: (1) knowledge (physical activity and fitness assessment), (2) tools (exercise prescription, implementation, and ongoing support), (3) skills (exercise counseling and behavioral strategies), and (4) self-care (personal medical student health). This is one of the first education initiatives of its kind and may be a good model for other levels of medical education and efforts within the spectrum of lifestyle medicine education.
Evolving Curriculum Topics
The components of Lifestyle Medicine curricula implemented in the past decades include nutrition,18,30 exercise, 16 and behavioral change. 17 However, limited curricula include an integrated approach of a varied spectrum of LM topics such as nutrition and exercise, together with behavioral change counseling. 15
Neither reports describing the field of LM34,35 nor the physician competencies 10 define specific behaviors (eg. eating, moving) that constitute LM and should be included in future curricula. The American College of Lifestyle Medicine (ACLM) specifies the domains of diet, exercise, stress management, and smoking cessation as components of the field of LM. 36 However, when polled, LM stakeholders determined nutrition, physical activity, behavioral change techniques, stress resiliency, and personal behavior as equally important domains of a LM fellowship curriculum and more important than smoking cessation to be included in future LM fellowship curricula. 37
In September 2013, the Lifestyle Medicine Education (LMEd) Collaborative was founded to transform medical education to include LM. 38 Its participants include medical school deans, medical students, content experts and representatives of professional associations, government agencies, accreditation agencies, and national assessment boards. To facilitate the setting of achievable goals, the principle areas of initial curricular subjects were narrowed to physical activity, nutrition, medical student’s self-care, and behavioral change. Topics less mature in their evidence base (eg, stress management) or already widely taught in UME (eg, tobacco, alcohol, and other substance abuse) were not included. Although LMEd is initially focused on a targeted audience of US medical students with limited subjects, plans are in place for expansion of the effort to (1) a broader array of subject areas, (2) an interdisciplinary audience of all health care providers, (3) all levels of training (eg, GME and CME), and (4) all parts of the world.
Audience
The Physician
Lianov and Johnson wrote that “acknowledging the crucial role of environmental and community factors in creating and sustaining inappropriate health behaviors does not eliminate the duty of physicians to assist patients in making health behavior changes.”10(pp.202) This attitude is supported by both patients 39 and physicians. 6 Thus, goals for primary care LM education have been defined as previously described. 10 Although these suggested competencies were developed largely to guide primary care and preventive care physicians’ medical education, many of these competencies have relevance for all specialties, and each medical specialty is encouraged to review these competencies and adopt and adapt them as appropriate. 10
Other Health Care Providers
One of the physicians’ competencies to prescribe LM is to practice as part of an interdisciplinary team. 10 When describing LM, a model of care similar to the Patient Centered Medical Home 40 was suggested for delivery, where the physician is a coordinator of a team of health professionals and does not operate independently or on a one-on-one basis. 34 Thus, interprofessional medical education is encouraged for both physicians and other health providers. 41 However, although other providers such as social workers, psychologists, and physician assistants are part of the collective effort for a patient’s behavioral change, LM education is not well developed in their training.
Application to the Current Continuum of Medical Training
The continuum of LM medical education should be implemented across all levels of medical education, as described in Figure 2. It should include medical school (UME), residency and fellowship training (GME), and CME 42 and, arguably, an option for premedical training. 43 Described below are the current initiatives within the established continuum of medical training.
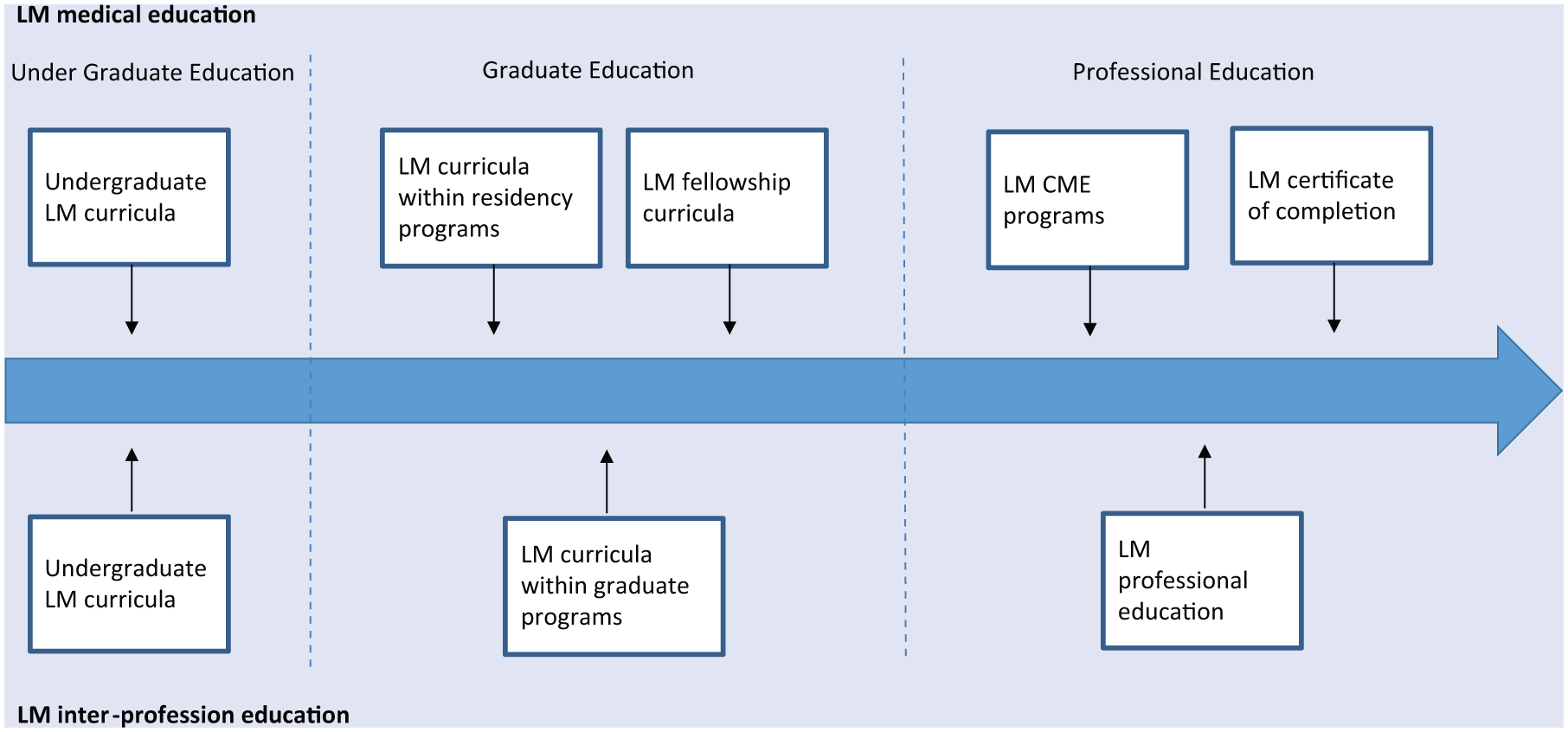
Lifestyle Medicine (LM) Education Continuum.
Undergraduate Medical Education
Although CME training may be simpler to institute, reforming medical school curricula is a more potent and lasting change agent. Although it is recommended to start LM medical education in medical schools or even in premedical training, 26 the majority of medical schools do not include it as part of their curriculum. 16
LM curriculum incorporated with UME has been shown to improve students’ knowledge, confidence, skills, self-care, 16 and patient counseling, 19 with improvement in patient-reported outcomes. 44 There is a variety of delivery options for LM in medical schools. First, there is significant documented interest of the medical students in the topics of LM,45,46 and this interest could be leveraged to initiate student-led education. This is being pursued in some medical schools by the formation of Lifestyle Medicine Interest Groups. 47 Second, the perceived importance of LM education by deans 26 can be leveraged for an approval of an elective LM program 23 or a required course within the curriculum.12,48 Finally, following the vision of “Lifestyle in Medicine,” 22 LM topics may become foundational as a required part of medical school training, as is done in the University of South Carolina School of Medicine Greenville curriculum, 11 or a combination of required training and elective within the curriculum, as is delivered at the Western University College of Osteopathic Medicine of the Pacific. 49
Graduate Medical Education
Within the specific competencies for primary care and preventive medicine10, educators at the GME levels were encouraged to incorporate the relevant LM competencies into training programs. 10 Moreover, the ACLM has suggested the development of a competencies-based fellowship in LM that will train physicians to become clinical specialists in LM. 50 Mechanick et al 51 suggested that a LM fellowship will train physicians to be experts—in competencies, knowledge, skills, and attitude—but also have a broader knowledge based in leadership roles, teaching, and skills in original research. 51 With this perspective, LM expertise, in addition to clinical practice, will have components related to developing LM training programs and advocating for these programs at the undergraduate, graduate, and postgraduate levels. 51 A research fellowship in LM, aimed to train an expert in LM, is being piloted as a GME path in the Institute of Lifestyle Medicine, Joslin Diabetes Center at Harvard Medical School. 37
Whereas robust implementation of LM at the GME level is lacking, an inaugural model of a residency program that includes a LM educational curriculum is the Yale Preventive Medicine residency program in collaboration with the Institute of Lifestyle Medicine. 52 This program is based on the LM competencies 10 and includes a combination of on-site didactic lectures, online curriculum, 53 and a 2-week clinical observation.
Continuing Medical Education
The few publications describing LM CME programs vary in objectives, methodology, duration, and participants.15,18-20,54-57 These programs ranged in length, from 1 hour 55 to 32 hours of training. 18 Some CME program goals were designed to improve management of specific health conditions such as pediatric obesity,19,54,55,57 whereas others targeted specific behaviors, such as eating.18,20 The published outcomes of these training programs include an increase in patient counseling 19 and an improvement in patient-reported outcomes. 20 To date, just 1 article 15 describes CME programs that address overall physician competencies in LM. 10 It is critical to continue to provide education and to evaluate it in practicing physicians to improve these necessary skills.
Delivery Methods
Live: Didactic
Previous research has indicated that live face-to-face CME formats, as compared with print and Web-based delivery systems, are often preferred 58 and have equal or greater impact on physician behaviors. 59 Although Web-based modules have become popular, live in-person lecture formats still constitute the majority of programs through all levels of UME, 11 GME, 37 and CME. 15
Live: Experiential
Interactive modules and small-group training has been reported and is particularly efficacious compared with the traditional didactic delivery style. 60 Recent reports describe lifestyle medicine CME programs that include experiential components such as yoga and spinning classes 15 and cooking sessions. 18 In addition, simulated patient modules were described in UME programs17,61 and small-group discussions in an interprofessional training, 62 and both walking exercise and cooking classes were described in a LM training program for nurses. 63 Although more difficult to include, incorporating interactive and experiential learning as part of future LM curricula is recommended.
Online
Currently some institutions are using an online platform as the primary or sole venue for LM programs,24,31,64 whereas others used Web-based modules together with in-person training. 14 The online venue might be used in a variety of options, such as recorded in-person lectures, 65 recorded video clips, interactive modules, 53 and Web/phone environment that is capable of hosting live online discussion from all over the world. 24
The Provider Environment
Providers’ personal behaviors are associated with promotion of primary prevention 66 and with their patients’ behaviors. 67 A variety of programs in the UME12,13 and CME levels 62 are using self-behavior as one of the venues for education. Furthermore, one program described by Shai et al 62 demonstrated correlation between the improvement of providers and patients’ behaviors. Incorporation of self-behavior modules into LM curriculum or tracking the participants’ self-behavior as one of the program’s outcomes is recommended.
The Future of LM Curricula
As described previously, the LMEd collaborative was founded in September 2013. This collaborative aims to transform medical education to include LM curriculum in undergraduate medical school. 38 Supported by a presidential grant from the Josiah Macy Jr Foundation and early investment by the Ardmore Institute of Health, LMEd focuses on the opportunities for and challenges to implementing LM curricula by identifying necessary infrastructure and key stakeholders and by determining the needs of those constituency groups. The LMEd collaborative has identified 5 goals: (1) provide high-quality curricular material on an easily navigable Web site; (2) solicit the support of medical school deans, critical administration, and faculty to advocate for and implement lifestyle medicine curricula in medical school education; (3) have an impact on federal and state policy through increased awareness and legislative initiatives that encourage adoption of lifestyle medicine into medical school education; (4) develop and conduct assessment in the following areas: student health, student knowledge, and program effectiveness; and (5) support medical students as effective champions of lifestyle medicine, whose engagement with the curriculum will lead to increased adoption within medical schools and enhanced collaboration nationally.
These 5 strategic areas are currently being expanded on by the collaborative participants to form a national strategic plan incorporating the initial LM subjects (nutrition, physical activity, behavioral change, and self-care) in the 170 osteopathic and allopathic medical schools in the United States, educating more than 106 000 medical students. Although LMEd is still in the early stages, the next steps being explored include extension of this initiative internationally (eg, European Union medical schools), interprofessionally (eg, nurses, physician assistants, pharmacists), and through all levels of medical training—GME, CME and premedical training. The expansion will also include a broader array of subjects (eg, sleep, stress resiliency, tobacco cessation).
LM medical education continues to evolve. A certificate of completion is currently being developed by the ACLM/ACPM. 68 This ~30-hour online CME course aims to teach the rudiments of LM, including topics within the fields of physical activity and exercise, nutrition and food, caregiver health, and health coaching. Although the primary audiences are practicing physicians, residents, and medical students, all health professionals might benefit from this training.
Next steps toward securing LM education may include developing a Certificate of Competency in LM and progressing to creation of board certification in LM, similar to the course of development of the American Board of Obesity Medicine. We recommend that it is time to lay the groundwork for the creation of an American Board of Lifestyle Medicine, started by a wide consortium of LM stakeholders and educators, that will eventually develop standardized, sanctioned training that will include a combination of online and live training and assessment.
Conclusion
Lifestyle Medicine continues to take hold and expand in logical response to the global pandemics of noncommunicable chronic diseases (ultimately caused by modifiable health behaviors). There is an urgent need within this effort to create and implement comprehensive LM education for all health professionals, at all levels of training, worldwide. Early steps toward this goal are demonstrating positive results through systematic implementation, medical student engagement, physician health practices, and clinical outcomes, though much work remains.
Footnotes
Acknowledgements
This review article is based on “Education in Lifestyle Medicine” delivered at American College of Lifestyle Medicine Annual Conference; October 22, 2014; by Edward M. Phillips, MD.