
Abstract
Background: Lifestyle medicine (LM) is gaining recognition in medical education. Université Laval, a Francophone university, is the first university in Canada to implement the Lifestyle Medicine Residency Curriculum (LMRC) developed by the American College of Lifestyle Medicine. This study aimed to evaluate the feasibility of implementing LM training for family residents in Quebec City. Method: Eight mentors adapted the English LMRC to Quebec’s healthcare and cultural context while maintaining its core content. In September 2022, 16 family medicine residents participated in the program. Mentors collaborated with program directors to develop French-language materials, contextualize content, and create an online LM platform. Feedback from residents and mentors was collected through surveys, focus groups, and informal discussions to guide continuous improvements. Results: Fifteen of 16 enrolled residents completed the program. Average attendance at monthly sessions was 70 %, with absences mainly due to night shifts or regional rotation. Resident showed strong engagement, with 100% completing modules asynchronously. Key factors for successful implementation included faculty mentors’ and residents’ engagement, and French-language materials tailored to the Quebec healthcare system. Challenges included limited French LM resources and a lack of co-located interdisciplinary teams. Strategic solutions involved creating a centralized online platform, protected learning time, aligning the program with existing curricula, and partnerships with community programs. Conclusion: Implementing LMRC demonstrated the feasibility of integrating LM training into a Francophone family medicine residency. Lessons learned may inform broader adoption in diverse linguistic and cultural settings.
“Strong resident engagement and committed faculty mentorship were central to the program’s successful implementation.”
Background
Importance of Lifestyle Medicine
Lifestyle Medicine emphasizes the prevention, management, and even reversal of chronic diseases through evidence-based lifestyle modifications.1-4 This approach focuses on core principles including a whole plant-based eating pattern, regular physical activity, stress management, restorative sleep, avoidance of risky substances, and positive social connections. 5 These pillars align closely with the goals of modern healthcare systems. 1
Given the rising prevalence of chronic diseases, 6 and the fact that they are frequently encountered in clinical practice, 7 integrating lifestyle medicine into healthcare practices is essential for promoting overall health and well-being.8,9 Numerous studies and clinical guidelines indicate that lifestyle interventions can significantly reduce the risk of developing chronic diseases such as diabetes, systemic hypertension, and cardiovascular diseases,10-13 while also helping to lower healthcare costs. 14
Integrating Lifestyle Medicine into Medical Education
As the burden of chronic disease increases, so does the need for physicians and healthcare professionals trained to deliver lifestyle-based interventions. Interest in lifestyle medicine education has expanded rapidly, particularly among residency programs, where faculty and trainees are increasingly advocating for its integration.15-18 Equipping residents with training in lifestyle medicine enhance their ability to support behavior change and address chronic disease more effectively in their clinical practice. 19
Structured educational initiatives, such as the Lifestyle Medicine Residency Curriculum (LMRC), developed by the American College of Lifestyle Medicine (ACLM) in partnership with Loma Linda University Health, provide promising models. 20 This comprehensive curriculum is designed for seamless integration into medical residency programs. 16 The LMRC includes 40 h of didactic material, 60 h of applied activities, and a 400-h practicum consisting of lifestyle medicine related patient encounters, a 20-h Intensive Therapeutic Lifestyle Change (ITLC) program and 20 h group facilitation, all intended to be completed over a 1-3-year period. 20 The LMRC enables residents to develop both foundational knowledge and practical skills aligned with lifestyle medicine core competencies. 21 These competencies emphasize prevention and therapeutic management of chronic disease in everyday clinical care. Research suggests that building students’ confidence in these areas require clinical exposure to lifestyle-based interventions.22,23 However, LMRC programs have been designed in and for English-speaking U.S contexts.
The Canadian and Francophone Context
Despite international advances, lifestyle medicine remains underrepresented in postgraduate medical education across Canada. Recognizing this gap, the Faculty of Medicine at Université Laval has taken a leadership role, becoming the first Canadian institution to implement the LMRC within its family medicine residency program. While this initiative was developed with the specific needs of Francophone Canadian institutions in mind, reflecting their cultural and healthcare realities, it may also serve as a model and source of inspiration for other universities across the country and elsewhere.
This article presents our experience implementing lifestyle medicine training for family medicine residents at a French-language university in Québec City, Canada. We describe how the LMRC was adapted to align with the local healthcare context, culture, and community resources, as well as the process of integrating applied learning activities into residency training.
Overall Objective
To evaluate the feasibility of implementing lifestyle medicine training for family medicine residents at a French-language university in Quebec City, Canada. This initiative seeks to strengthen medical knowledge and clinical competencies to support improved healthcare delivery.
Specific Objectives
(1) Adapt the educational content, including didactic materials, to reflect French Canadian culture, the healthcare system, and available community resources. (2) Identify and summarize the steps required to develop and integrate learning activities. (3) Describe and assess the key success factors, implementation challenges, and strategic solutions that support the LMRC’s integration.
Method
LMRC Implementation in Family Medicine Residency Program
In June 2022, a working group of eight faculty mentors collaborated to implement the LMRC within the Family Medicine Residency Program at Université Laval in Quebec, Canada. While the LMRC was originally developed in the United States by the ACLM, our objective was to adapt its content and delivery to align with the realities of the Quebec healthcare system and local culture.
Key Steps for Implementing the LMRC Into a Francophone Family Residency Program.
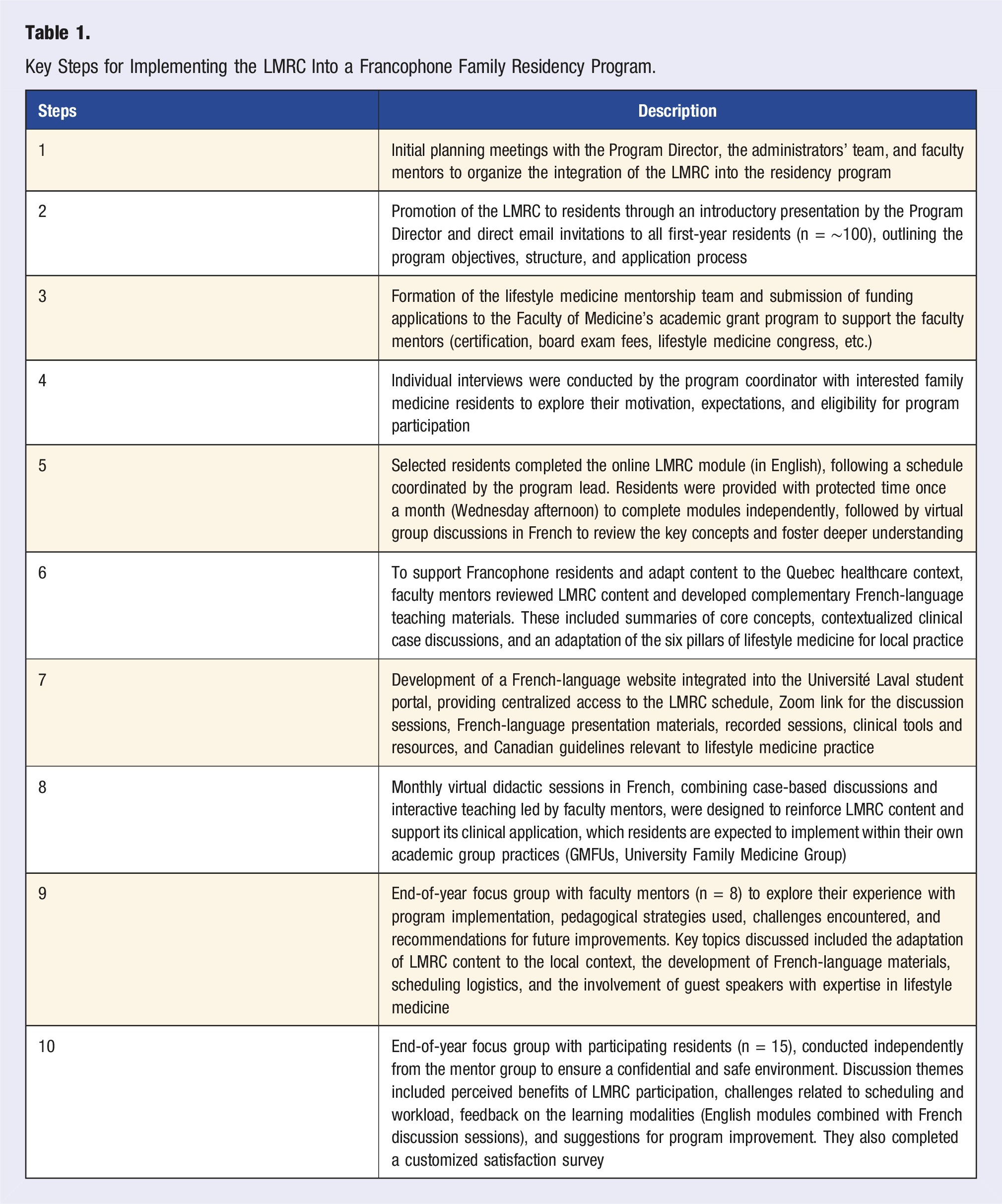
Residents were invited to participate in the LMRC through a selection process coordinated by the Department of Family and Emergency Medicine. In September 2022, the first cohort, consisting of first- and second-year family medicine residents, officially began the program.
Residents completed the core LMRC modules in English, as provided by the ACLM. To support the integration of lifestyle medicine principles within the Quebec clinical context, eight faculty mentors developed complementary educational activities in French. These included French-language modules, real clinical case discussions, monthly virtual interactive sessions, presentations from guest speakers, and additional resources tailored to local practice.
Monthly virtual session brought together all participating residents and faculty mentors to promote knowledge exchange and support the practical application of lifestyle medicine concepts in clinical practice. Resident attendance was tracked using a shared presence sheet completed during each Zoom session by both the lead coordinator and faculty mentors. Reasons for absence were recorded, with the most common being clinical duties such as night shifts or regional rotations.
Throughout the academic year, monthly in-person and virtual meetings were held with residents and mentors to support program engagement, address concerns, and refine implementation based on feedback. At the end of the first year, two separate focus groups were conducted: one exclusively with residents and another with faculty mentors. This separation was intentional to allow residents to freely express their perspectives and experiences in a confidential environment. The focus groups aimed to evaluate the program’s implementation, identify perceived strengths and challenges, and gather suggestions for improvement.
Faculty Review, Online Materials and Accessibility
Faculty mentors carefully reviewed the LMRC modules to ensure alignment within the Quebec healthcare context. While preserving the core 40 h of LMRC content, the team developed eight complementary, culturally adapted lectures, delivered monthly during the first year of implementation. These sessions integrated French-language instructional materials, Quebec-specific healthcare examples, clinical case discussions, and interactive workshops designed to support practical application in local clinical settings. This platform provided residents and mentors with schedules, objectives, lecture slides, clinical tools, resources and certification procedures for the ABLM.
Each LMRC module inspired the development of a two-hour, contextually relevant lecture, often complemented by francophone experts in lifestyle medicine. For instance, the nutrition module featured experts in culinary medicine. Additionally, case discussions tailored to the local patient population reinforced the practical application of lifestyle medicine principles. This approach preserved LMRC’s foundational content while fostering engagement through interactive and contextually relevant learning experiences.
To further support learning and accessibility, all adapted LMRC materials were made available through Université Laval’s existing student portal. This dedicated French-language online platform provided residents and mentors with centralized access to course schedules, learning objectives, lectures, slides, clinical tools, evidence-based resources, and certification procedures for the ABLM. The portal also included supplementary materials for asynchronous learning, such as recorded lectures and relevant guidelines.
Data Collection and Analysis
Resident participation and engagement in the LMRC were monitored through multiple strategies. Attendance at monthly live virtual sessions was recorded by both the session mentor and the lead coordinator through a shared attendance sheet during Zoom meetings. Reasons for absence were collected informally through follow-up communication with residents, most often related to overnight clinical shifts or mandatory regional rotations. Engagement with the asynchronous online modules was monitored through the LMRC learning platform, allowing the teaching team to confirm module completion and track residents’ progress over time.
At the end of the first-year program, residents were invited to complete a customized anonymous online satisfaction survey. Focus groups were conducted with both faculty mentors and residents to gather feedback about their experiences. Detailed notes from each focus group were recorded and documented by the faculty administrator, shared with participants for validation, and analyzed thematically to identify key themes. Additional data sources were gathered through informal observations from monthly meetings, class discussions, and communication throughout the year. These observations were compiled and used iteratively to refine program delivery and better support resident engagement and learning.
A qualitative thematic analysis was conducted based on data from focus groups, surveys, and observational notes. Given the small size, only descriptive statistics were used to calculate the average of responses. The analysis was structured to organize real-world implementation insights into successes, challenges, and strategic solutions to support program improvement.
Results
Mentors’ Feedback and Program Outcomes - Focus Group
Eight mentors regularly met with the program director and administrators to launch the LMRC and its integration into the Family Medicine Residency curriculum. In addition to their teaching roles, mentors were actively involved in operational coordination, including the creation of a dedicated website for lifestyle medicine resources on Université Laval’s online student portal. Over 20 meetings were held to collaboratively develop a structured didactic program in French, tailored to Quebec’s cultural and healthcare context. During this process, five family physician mentors obtained their certification in lifestyle medicine from the ABLM.
Key insights from faculty mentor focus groups highlighted several important factors that facilitated implementation. All mentors identified that the presence of ABLM-certified faculty mentors was instrumental in guiding the development of the French-language didactic program. They emphasized the need to create a centralized French-language website to house all relevant French materials, recorded sessions and resources. Adaptations to the LMRC were also considered essential to align content with the Quebec medical system and cultural realities. Delivering PowerPoint presentations in French, specifically customized for Quebec residents, was viewed as critical to maximizing engagement and comprehension. Mentors also valued the flexibility of the LMRC model, which allowed for adjusting clinical hours at the ITLC or offering alternative activities better suited to the local context.
Residents’ Feedback and Program Outcomes - Satisfaction Survey and Focus Group
Of the 16 family medicine residents enrolled, one withdrew due to time constraints, leaving 15 active participants in the program. The average attendance at monthly live sessions was 70%, with most absences primarily due to night shifts or regional rotations. Despite these challenges, 100% of residents completed the LMRC modules asynchronously, demonstrating a strong commitment. All 15 active residents completed the LMRC modules, with 12 finishing them within the expected timeline. Feedback from the anonymous satisfaction survey and focus group highlighted several key findings. Over 50% of residents expressed satisfaction with the LMRC modules (content and format), and 82% value the French-language monthly lectures. The relatively moderate satisfaction rate for LMRC modules appeared to be partly since they were tailored to the U. S. healthcare system. Some residents noted that certain references, such as to private insurance or billing practices, did not align with the publicly funded Canadian system or the specific realities of healthcare delivery in Quebec. In addition, many of the patient education materials and tools provided through the LMRC were developed in English, limiting their immediate usefulness for residents working in predominantly French-speaking settings. This mismatch in both system relevance and language made parts of the content feel less applicable to their clinical practice. They also requested additional time to review modules and extend to French classes; there was a preference for more interactive sessions, and they suggested integrating LMRC into the existing residency curriculum. Several residents expressed a strong interest in hands-on training opportunities within real lifestyle medicine clinics alongside interdisciplinary teams. There was notable interest in skill development for additional training in motivational interviewing. Residents suggested further activities aligned with module themes, such as documentary screenings, podcast discussions, and culinary workshops. Lastly, residents emphasized the importance of developing clinical tools linked to the electronic medical record to optimize lifestyle medicine prescriptions.
Experiential Learning in Lifestyle Medicine: An Innovative Workshop
After one year of implementation, feedback from residents and mentors gathered throughout the LMRC process revealed a strong desire for additional skill development in motivational interviewing and lifestyle medicine counseling. In response to these insights, the program team piloted an innovative in-person workshop in September 2023 at Monastère des Augustines in Quebec City, a setting renowned for its focus on well-being. The training opportunity was initiated and financially supported by the mentors, who invited the residents to participate. The workshop was led by a psychologist specializing in motivational approaches and cognitive-behavioral therapy and aimed to equip both residents and mentors with advanced tools to better support patients in making sustainable lifestyle changes. Fourteen participants attended, engaging in an immersive learning experience that combined theory with practice. What distinguished this training was its holistic approach: alongside theoretical and practical classes, participants engaged actively in healthy eating experiences, yoga sessions, and outdoor activities. This experiential component reinforced the integration of lifestyle practices into clinical care, aligning with the program’s broader educational goals. This two-day training session was accredited for Continuing Medical Education (CME) by the Faculty of Medicine at Université Laval, reinforcing its value as a pioneering initiative in medical education and as a promising model for future training in lifestyle medicine.
Components of Success, Challenges, and Strategic Solutions
Key Successes, Challenges, and Strategic Solutions Identified by Mentors and Residents During LMRC Implementation.
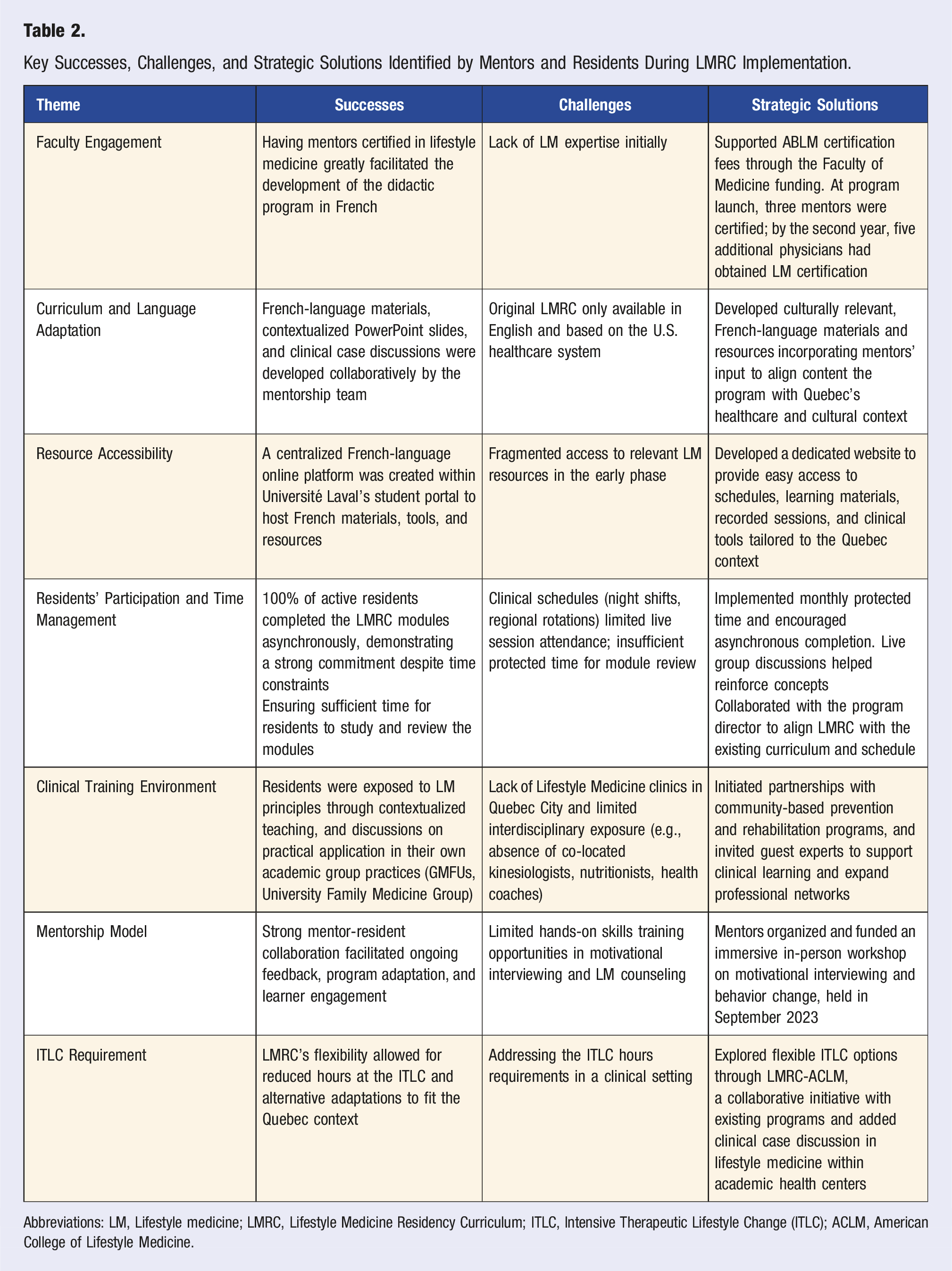
Abbreviations: LM, Lifestyle medicine; LMRC, Lifestyle Medicine Residency Curriculum; ITLC, Intensive Therapeutic Lifestyle Change (ITLC); ACLM, American College of Lifestyle Medicine.
The successful implementation of the LMRC at Université Laval was the result of strategic collaboration and ongoing adaptation. One of the most significant enablers was faculty engagement: having mentors certified in lifestyle medicine facilitated the development of a French-language didactic program. Although initial expertise in lifestyle medicine was limited, the Faculty of Medicine supported certification costs through dedicated funding. As a result, three mentors were certified at program launch, and five more joined by the second year.
Curriculum and language adaptation presented a key challenge, as the original LMRC materials were only available in English and designed for the U.S. healthcare system. In response, the mentorship team developed culturally relevant, French-language materials and clinical case discussions tailored to Quebec’s healthcare context.
To address resource accessibility, a centralized French-language online platform was created within Université Laval’s student portal. This initiative resolved early-phase fragmentation by providing easy access to schedules, recorded sessions, learning materials, and clinical tools.
Despite demanding clinical schedules, residents demonstrated strong engagement, with 100% completing the modules asynchronously. Scheduling conflicts, such as night shifts and regional rotations, limited attendance at live sessions. To address this, protected time was introduced monthly, and live group discussions were held to reinforce learning. The LMRC was further aligned with the existing family medicine curriculum in collaboration with the program director.
In the clinical training environment, residents were exposed to lifestyle medicine principles and encouraged to apply them in their academic group practices (GMFUs). However, the lack of lifestyle medicine clinics and interdisciplinary exposure in Quebec City posed a barrier. Strategic solutions included developing partnerships with community-based prevention and rehabilitation programs and inviting guest experts to expand residents’ professional networks.
The mentorship model was central to the program’s success. Strong mentor-resident collaboration supported program adaptation and learner engagement. To address limited training in lifestyle medicine, mentors organized and funded a hands-on workshop on motivational interviewing and behavior change, held in September 2023.
Finally, regarding the ITLC requirement, LMRC’s flexibility allowed for adapted solutions that met clinical expectations in Quebec. This included leveraging the LMRC-ACLM with existing programs and added clinical case discussions in lifestyle medicine into academic health center activities. Overall, the program’s success was underpinned by proactive problem-solving, strong faculty commitment, and continuous feedback from both mentors and residents.
Discussion
Our experience implementing the LMRC at Université Laval demonstrates that lifestyle medicine education can be feasibly and effectively integrated into a Francophone residency program. Originally developed in English, the LRMC was successfully adapted by our team to reflect the linguistic and cultural context of Quebec, ensuring its accessibility and relevance for French-speaking residents and faculty. The program equips residents with evidence-based tools, such as nutrition and physical activity prescriptions, that are essential in the prevention and management of chronic diseases. Strong engagement from both residents and faculty mentors highlights the value of embedding lifestyle medicine into formal medical education.
Significance of Lifestyle Medicine in Chronic Disease Management and Resident Education
Extensive evidence supports the role of lifestyle interventions in reducing the incidence and severity of chronic diseases, making them essential components of both clinical care and medical education.24,25 To meet this need, residents, as future healthcare leaders, must acquire practical skills to support patients in adopting healthier behavior. Programs like the LMRC prepare them to do so by combining evidence-based approaches with real-world application. For instance, the LMRC emphasized interventions such as nutrition and physical activity prescriptions. These strategies have significantly improved blood pressure and glycemic control in patients with diabetes and cardiovascular disease. 26 Resident engagement and feedback during the program reflected an appreciation for learning how to apply these strategies in clinical practice. This aligns with findings from other studies demonstrating the benefits of integrating lifestyle medicine into medical training. 23
Implementation Insights from a Francophone Context
The LMRC’s comprehensive structure, combining both didactic education and practical application, equips residents with the skills needed to apply lifestyle medicine principles in real-world scenarios. Given the French-speaking environment, the training is designed to reflect the linguistic and cultural realities of the region of Quebec City, ensuring that residents can effectively communicate and engage with patients. This hands-on experience is essential for bridging the gap between theoretical knowledge and clinical practice, allowing future healthcare providers to tailor lifestyle interventions in a way that resonates with the values, traditions, and daily lives of Francophone communities.
While international interest in lifestyle medicine is growing, supported by other organizations such as the European Lifestyle Medicine Organization (ELMO), 27 few structure programs have been documented in Francophone residency training. To our knowledge, the LMRC at Université Laval represents one of the first such implementations, positioning it as a potential model for other French-speaking medical education institutions. By fostering this tailored approach, residents are better prepared to integrate lifestyle medicine principles into their patient care, improving health outcomes in diverse populations.
Strengths
The successful implementation of the LMRC at Université Laval highlights several key strengths. First, adapting the curriculum to the cultural and linguistic context of Quebec ensures its relevance and sustainability within the local healthcare system. Additionally, the program’s flexible learning environment, including virtual French-language teaching modules, has improved accessibility for residents across different geographic locations. Another strength is the emphasis on interdisciplinary education, which exposes residents to various lifestyle medicine strategies and fosters collaboration between different healthcare professionals. A particularly noteworthy strength is the mentor-led, in-person and virtually holistic lifestyle medicine training. The original initiative reflects the program’s adaptability and the commitment of mentors to creating meaningful and experiential learning opportunities. Finally, the strong interest and positive feedback from participating residents reinforce the value of integrating lifestyle medicine into family medicine training.
Challenges and Opportunities
Access to the LMRC’s structured curriculum and resources was essential to support its integration into residency training. However, adapting the program to Quebec’s cultural, linguistic, and health system context presented both challenges and unique opportunities.
A key challenge was the absence of dedicated lifestyle medicine clinics in Quebec City, limiting residents’ exposure to interdisciplinary teams, including kinesiologists, nutritionists, and health coaches. In this context, establishing partnerships with local lifestyle programs and aligning with provincial health priorities became important strategies to enhance residents’ access to community-based resources and support systems. These collaborations contribute to a more holistic approach, allowing residents to integrate available resources into their patient care strategies. In the longer term, securing funding to develop interdisciplinary lifestyle medicine clinics in the university family medicine group could provide centralized hubs for training and further enrich the learning experience for residents.
The current two-year length of the family medicine residency program in Canada leaves limited time to incorporate additional content such as the LMRC. Ongoing efforts to extend the residency training to three years may create more opportunities for the integration of lifestyle medicine into medical education.
Importantly, implementing the LMRC in a real-world residency training context created a valuable opportunity to gather feedback from residents and mentors throughout the process. The iterative and participatory approach allowed the program team to rapidly identify emerging needs, notably, residents’ desire for more hands-on skill development in motivational interviewing and behavior change counseling. In response, mentors played a key role in bridging this gap by organizing and funding an immersive, in-person lifestyle medicine workshop in September 2023. This innovative initiative illustrates the potential of faculty-driven solutions to address training gaps and respond to learners’ evolving needs while more formal resources and infrastructure continue to develop.
Limitations
One limitation of this project is the relatively small sample size, as it is a new program, which may limit the generalizability of the findings to a broader population or other groups of residents. Additionally, the study’s focus on participants from a specific geographic region (e.g., Quebec City and surrounding areas) may not fully reflect the diverse health needs and behaviors of individuals in different urban or rural settings. However, we offered the French class virtually to enhance inclusivity for residents practicing outside of Quebec City.
Another important limitation is that we did not use a robust implementation framework to guide or evaluate the development, delivery, and outcomes of the LMRC. At the outset, our primary goal was simply to implement the LMRC and respond pragmatically to residents’ needs within our local context. However, as the project evolved, we recognized the complexity involved in integrating lifestyle medicine into residency training and the importance of building supportive structures around the program to fit local contexts and realities. This experience highlights the value of applying established implementation science frameworks in future iterations, both to strengthen program evaluation and to capture key factors influencing adoption, scalability, and sustainability.
Future research with a larger, more diverse population across various medical specialties and languages could help confirm the applicability of the findings to other residency programs and healthcare settings.
Practical Implications for Other Lifestyle Medicine Programs
• The experiences and lessons learned from the implementation of the LMRC at Université Laval provide valuable insights for institutions considering the incorporation of lifestyle medicine into their curricula. The following practical recommendations can support successful adoption: • Cultural adaptation and local context: Adapt the curriculum to the region’s cultural and healthcare landscape. Align content with local health priorities and practices to enhance relevance and acceptance. • Integration into existing curricula: Collaborate with program directors to identify optimal time slots for integrating LMRC without overburdening residents. • Mentorship and Expertise: Engage mentors certified by recognized lifestyle medicine organizations (e.g., ABLM) to support program implementation, ensure consistency, uphold training quality, and effectively guide residents throughout their learning journey. • Online Platforms and Flexibility: Develop a centralized, accessible online platform in the local language, offering asynchronous learning options to accommodate residents’ schedules. • Partnerships with community resources: Establish partnerships with local lifestyle programs and healthcare organizations to provide residents with practical, community-based experiences.
Future Directions
The establishment of the LMRC at Université Laval not only sets a precedent for lifestyle medicine education in Canada but also reflects a broader vision for advancing public health outcomes. Our goal is to promote and sustain behaviors that foster both individual and collective health through a supportive environment, personalized guidance, and activities that raise awareness about healthy lifestyles. By cultivating healthcare providers who prioritize prevention and patient-centered care, the LMRC aims to have a positive impact on resident competencies, patient outcomes, and community health indicators. Future research should focus on evaluating the long-term impact of LMRC using a structured implementation and evaluation framework. Specific metrics such as changes in residents’ competencies, integration of lifestyle medicine practices in patient care, and patient health outcomes (e.g., improved weight management, blood pressure or reduced incidence of cardiovascular events) would be valuable to capture both clinical and educational impacts.
As lifestyle medicine continues to evolve, keeping pace with emerging evidence and adapting educational programs accordingly will be essential for maximizing its impact. Furthermore, there is a need for a national curriculum standard for Lifestyle medicine concepts that aligns with established frameworks such as CANMeds, 28 to ensure consistency and integration across Canadian medical education.
Conclusion
The implementation of the LRMC at Université Laval, a Francophone institution, has proven both feasible and well-received. Resident feedback collected over two years has been consistently positive, though challenges remain in sustaining and expanding the initiative. Strong resident engagement and committed faculty mentorship were central to the program’s successful implementation. By sharing the lessons learned, we aim to demonstrate that lifestyle medicine can be effectively integrated into residency training across diverse linguistic and cultural settings. Future success will depend on strengthening partnerships with community-based healthy lifestyle programs to enhance training opportunities and ensure long-term sustainability.
Footnotes
Acknowledgments
The authors would like to express their gratitude to the family medicine residents for their commitment to advancing education in this field and for their active participation in implementing the curriculum at our university. We also extend our appreciation to the administrative support teams at LMRC, ACLM, and the Department of Family Medicine and Emergency Medicine, Faculty of Medicine, Université Laval, for their invaluable assistance. Additionally, we thank the guest speakers, including in lifestyle medicine specialists, for their insightful contributions to the program.
Author Contributions
The initial draft of this commentary was written by Caroline Rhéaume. The remaining co-authors critically reviewed the manuscript and gave their approval for the final submitted version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. However, the mentors received a grant of $4529 from the Support Funds for Academic Activities of the Family Medicine and Emergency Medicine Department at the Faculty of Medicine, Université Laval, to cover the costs of American Board of Lifestyle Medicine (ABLM) courses and examinations. This funding did not influence the study design, data collection, analysis, or interpretation of results.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.