
Abstract
Non-communicable diseases (NCDs) are the leading cause of mortality and morbidity worldwide. Underlying NCDs are modifiable risk factors, which may be targeted through Lifestyle Medicine (LM). LM is an evidence-based and clinical discipline that supports healthy lifestyle habits. Much of LM integration in practice is rooted in the education afforded within health professional’s curricula. The study aimed to determine the effectiveness of LM educational interventions within health professional’s curricula on knowledge, competence, self-efficacy/confidence and skills. A systematic review and meta-analysis were conducted with data analyzed using descriptive statistics and a Random Effect Meta-analysis. A total of 14 studies were included. Interventions centered around substance use, nutrition and physical activity with no studies obtained on the sleep health, stress management and social connectedness pillars. Interventions showed a positive impact on improving knowledge standardized mean difference (SMD): 0.71 (95% CI: 0.25-1.18), self-esteem/self-confidence SMD: 1.34 (95% CI: 0.61-2.07), and outcome practice SMD: 0.78 (95% CI 0.29-1.26). There was insufficient power to provide reliable estimates for the attitude outcome. Integrating LM educational interventions within health professional’s curricula is promising and recommended to better equip trainees and future health care providers to support patients with the adoption of a healthy lifestyle.
Keywords
“LM is uniquely positioned to empower patients and communities to make sustainable lifestyle habits, prevent NCDs, and improve patient’s overall health and outcomes.”
Background
Non-communicable diseases (NCDs) represent a global epidemic of the 21st century. The 4 major types—cardiovascular diseases (e.g., stroke, heart disease), cancers, chronic respiratory diseases and diabetes—are the leading cause of mortality and morbidity worldwide.1,2 Globally, 1 in 3 adults are living with more than one NCD, 3 which has resulted in a significant increase in demand of health care services, treatment, and expenditure. Societally, this is coupled with productivity loss due to premature exit from the labor force, increased absenteeism, reduced work capacity, and early mortality. 4 Economically, NCDs are responsible for 90% of annual health care expenditure with projections of an accumulated global economic loss of $47 trillion (US) by 2030. 5 Importantly, the majority of NCDs are attributed to lifestyle choices and behaviors such as unhealthy diets (e.g., high sugar and ultra-processed food), 6 physical inactivity, as well as tobacco and alcohol use 7 ; thereby making NCDs, in part, preventable. Non-communicable diseases also account for 74% of deaths worldwide (∼41 million deaths per year) and 15 million premature deaths yearly among persons between 30 and 69 years of age. 8 Similar to global trends, an estimated 88% of all deaths are attributed to NCDs in the United States and Canada.9,10
Lifestyle Medicine
Lifestyle medicine (LM) is an evidence-based and clinical discipline that applies medical, environmental, motivational, and behavioral principles to comprehensively support healthy lifestyle habits to prevent, treat and potentially reverse NCDs.11–14 LM comprises of 6 pillars: Nutrition, Physical activity, Sleep health, Stress reduction, Social connectedness, and Substance use
12
(Figure 1). This rapidly expanding discipline is an adjunct to conventional medical practice
15
that introduces progressive, life-long lifestyle habits to effectively reduce many NCDs and the additional health complications.16,17 The investment in primary prevention through LM may result in a 4-fold improvement in health outcomes compared to secondary prevention that is often based on pharmacological treatment.
18
Over the past 30 years, there has been a cumulative body of empirical and epidemiological evidence reporting on the significant and positive impact of LM on health.14,17 Seminal publications include the Lifestyle Heart Trial,
19
Diabetes Prevention Program,
20
the Lyon Heart Study,
21
the PREDIMED Study
22
and the Framingham Heart Study.
23
The strengths of the scientific evidence is further underscored by numerous evidence-based guidelines24–26 (p20) and the World Health Organization recommendations that highlight the necessity of healthy lifestyle habits for the prevention, treatment and management of NCDs at the personal and societal level with the ultimate goal of improving population health.
27
LSM pillar.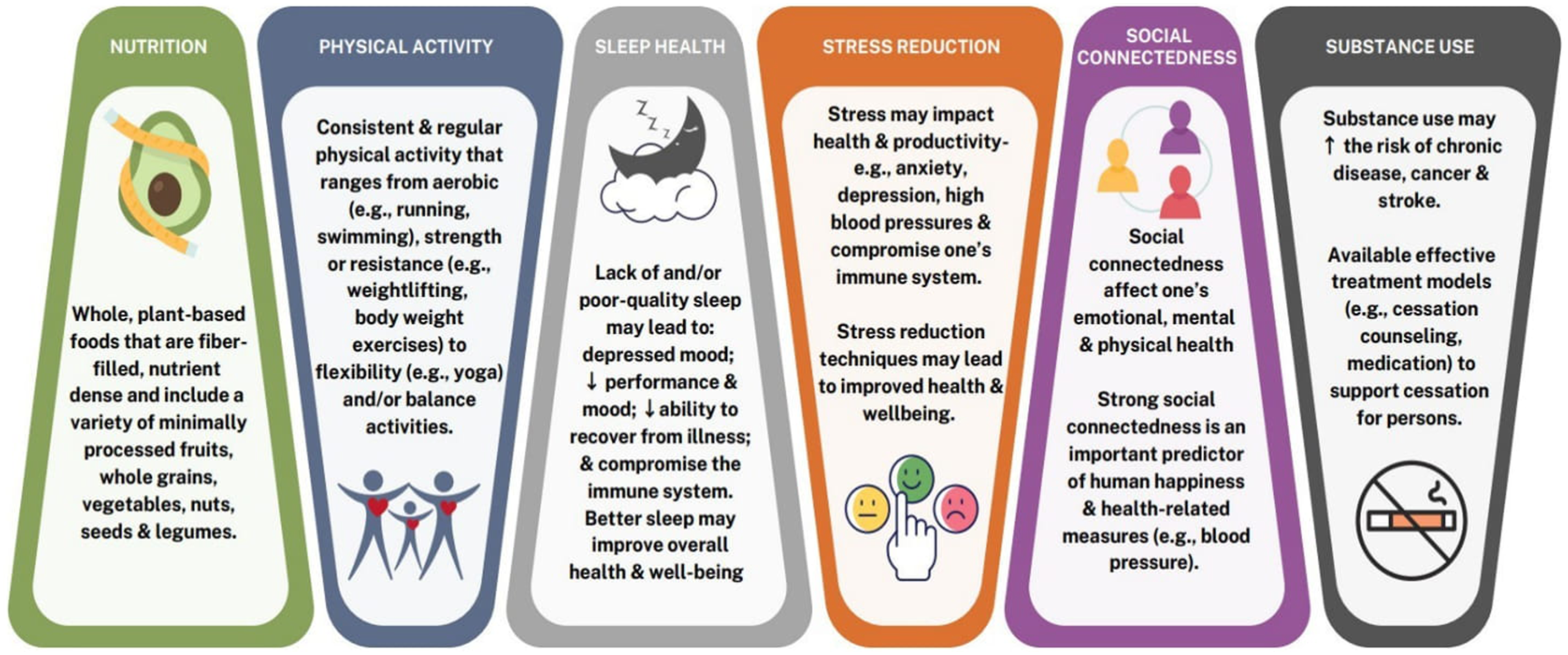
Gaps in Curricula
Lifestyle Medicine holds great promise and potential to address NCDs, however, the integration of LM-related content in health professional’s curricula is minimal to non-existent 28 ; resulting in inadequate LM-related competencies among health professional trainees and health care providers (HCPs). 29 This was reflected in a systematic review on the current practices of LM instruction in medical curricula (N = 32), in which 81% of the studies were conducted in the United States. 30 Of the 32 studies, most reported delivery of education on nutrition (78%) and exercise (59%) 30 with limited education on smoking cessation (34%), stress management (25%), sleep health (16%) and no mention of education on social connectedness. 30 Similar findings were observed in a systematic review (N = 24) that aimed to critically synthesize the literature on nutrition education provided to medical students. 31 The review yielded insufficiency with the incorporation of nutrition in medical curricula irrespective of setting, year of education and country. 31 The lack of foundational LM integration in health professionals curricula results in health professional trainees and in turn, HCPs being ill equipped to counsel patients on LM therapeutic modalities due to their own limited LM-related knowledge, competence, training, and skills.31,32
Over the years, there has been increased momentum and efforts to integrate LM in medical curricula and programs particularly in the United States (e.g., Harvard School of Medicine, University of Texas Rio Grande Valley, New York School of Medicine, University of Florida, University of North Carolina). However, there continues to be glaring gaps and a dearth of training to allied HCPs, specifically registered practical nurse (RPN)/licensees practical nurse (LPN), registered nurse (RN), nurse practitioner (NP) and physician assistant (PA).33,34 Such allied HCPs are uniquely positioned to provide patient education and counseling in their clinical practice and collectively comprise a large group of HCPs. 33 Appreciating the need and importance for LM integration in health professionals curricula 35 and to align with some of the recent medical LM curricula transformation, 36 it is imperative to first understand and map the current LM curricula integration practices. The aim of the study was twofold: (i) to critically synthesize the existing literature on the current state of LM integration in health professional trainees’ education; and (ii) to quantify the effectiveness of such educational interventions on improving health professional trainee’s LM-related knowledge, skills, and competence.
Methods
Design
A systematic review and meta-analysis were conducted. The protocol was not registered, however the study was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 37
Search Strategy and Selection Criteria
The search was conducted in May 2024. The databases used to systematically retrieve relevant publications were: Cumulative Index to Nursing and Allied Health Literature (CINAHL), Scopus, PubMed, and Embase. The following keywords were used in conjunction with Boolean operators to refine the literature search: “lifestyle medicine” OR “nutrition” OR “physical activity” OR “exercise” OR “substance use” OR “alcohol” OR “smoking” OR “stress” AND “sleep” OR “sleep health” OR “social connections” OR “social connectedness” AND “education” OR “information” OR “educational interventions” AND OR “nursing curricula*” OR “registered nurse curricula*” OR “physician assistant curricula*” OR “nurse practitioner curricula*” OR “registered practical nurse*,” OR “licensed practical nurse*” (Supplemental File 1).
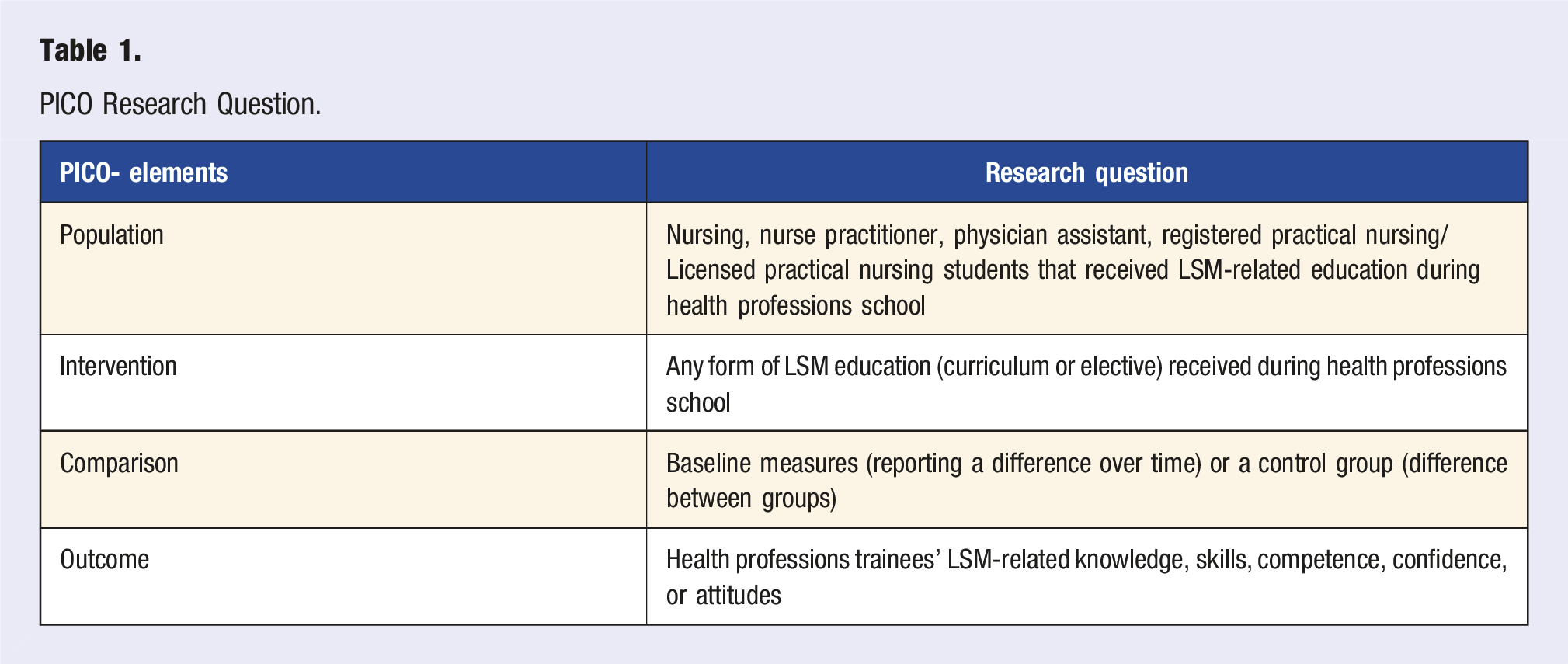
PICO Research Question.
Screening and Data Extraction
Two investigators (JS and SI) screened the titles and abstracts of the studies using the inclusion criteria. Full-text articles were retrieved for all studies that met the selection criteria and/or required more information that was not included in the respective abstract to inform a decision. One investigator (JS) independently assessed the full-text articles using the selection criteria. A second investigator (SI) reviewed the full-text articles and met to discuss any disagreements in order to reach a consensus. The following data were extracted from the articles: (i) general article information—author’s last name(s), publication date, study setting, country, and continent of publication; (ii) study purpose, research design, and target population (where available: age, sex/gender, ethnicity, race, socioeconomic, and sample size); (iii) educational program (e.g., nursing, nurse practitioner); and (iv) sample size. The following data were extracted on the LM educational intervention: (i) type of course (mandatory or elective); (ii) who delivered the information; (iii) mode of delivery; (iv) focus of LM Pillar; (v) topic objectives; and (vi) length/duration; and (vii) year of training.
Risk of Bias Assessment
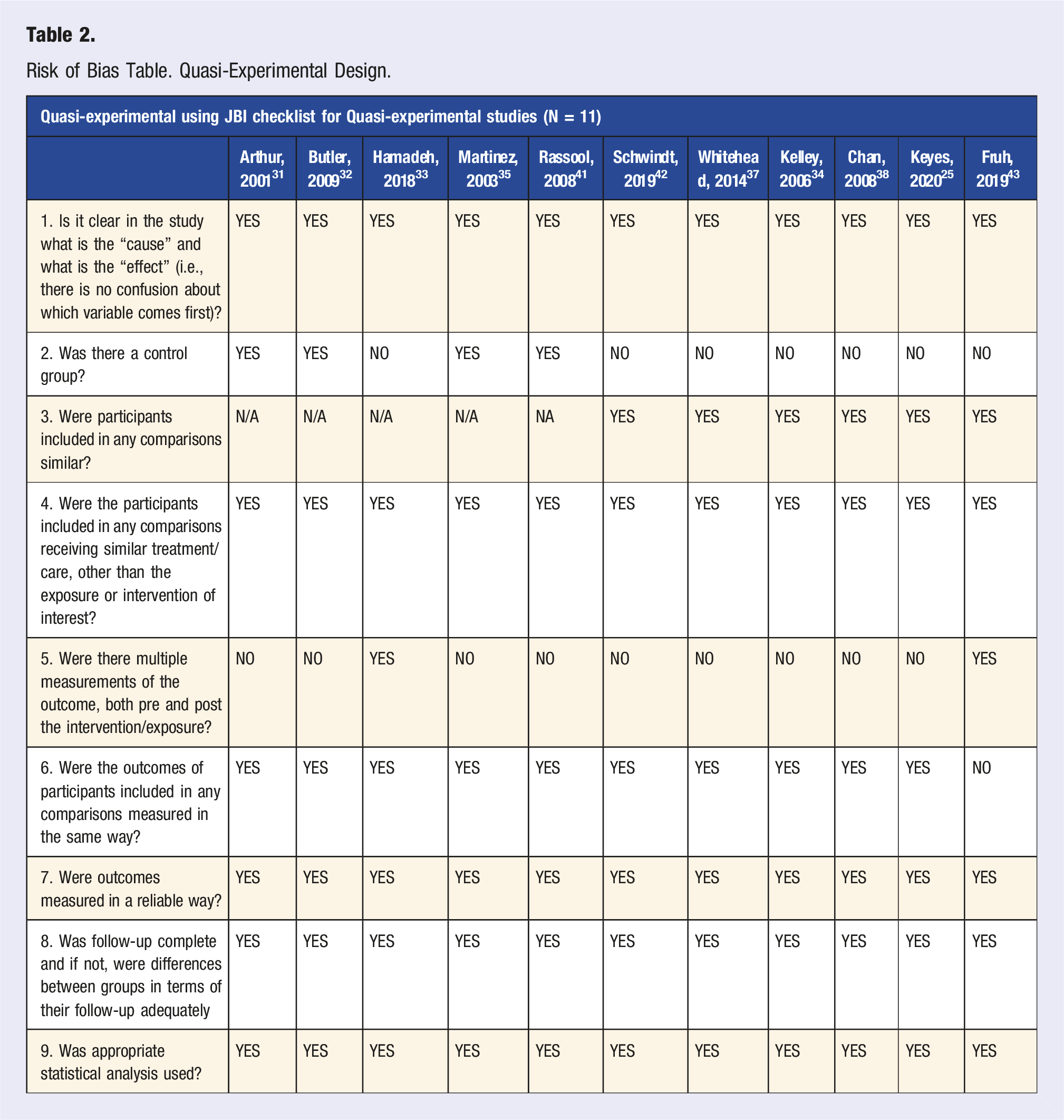
Risk of Bias Table. Quasi-Experimental Design.
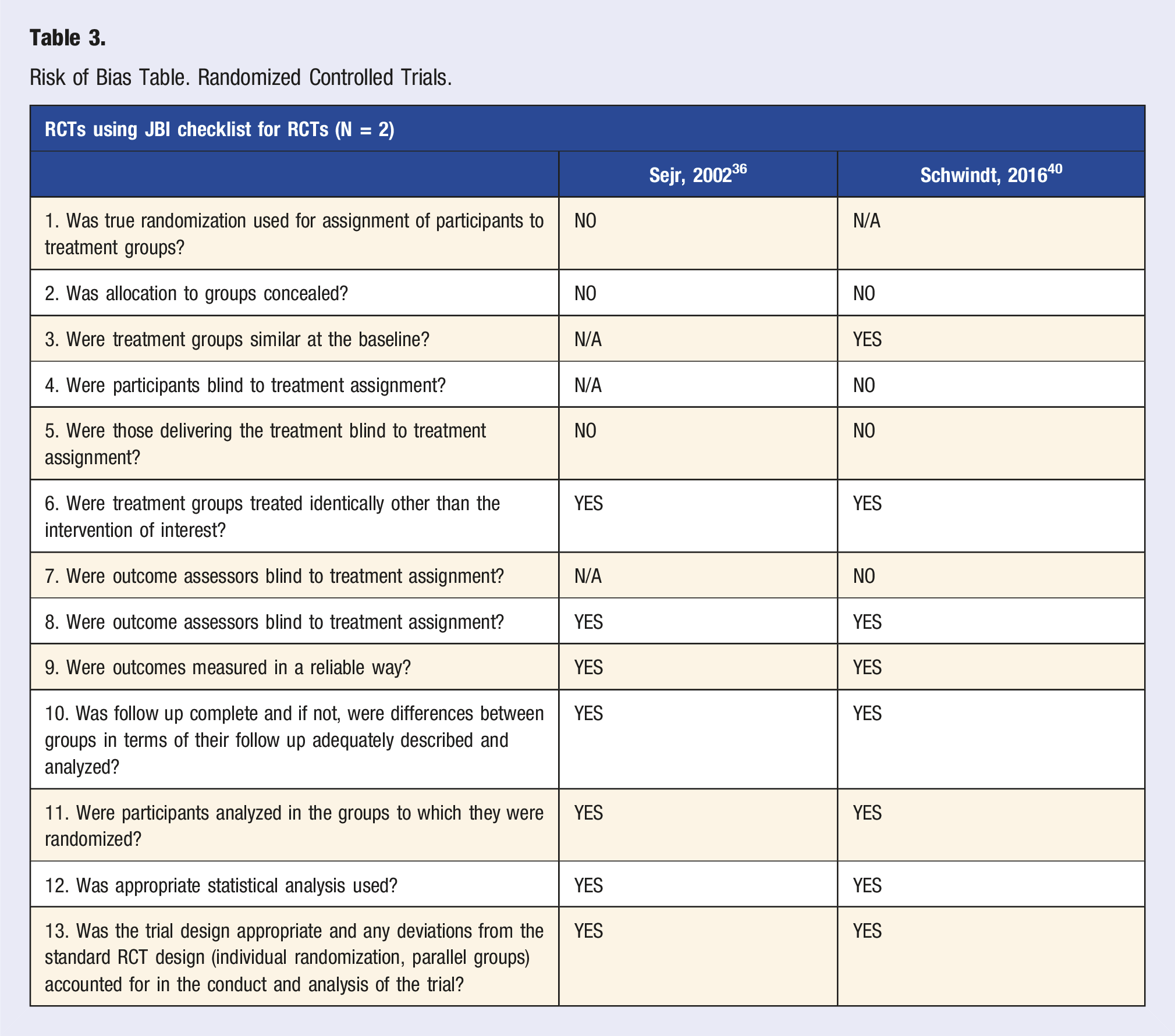
Risk of Bias Table. Randomized Controlled Trials.
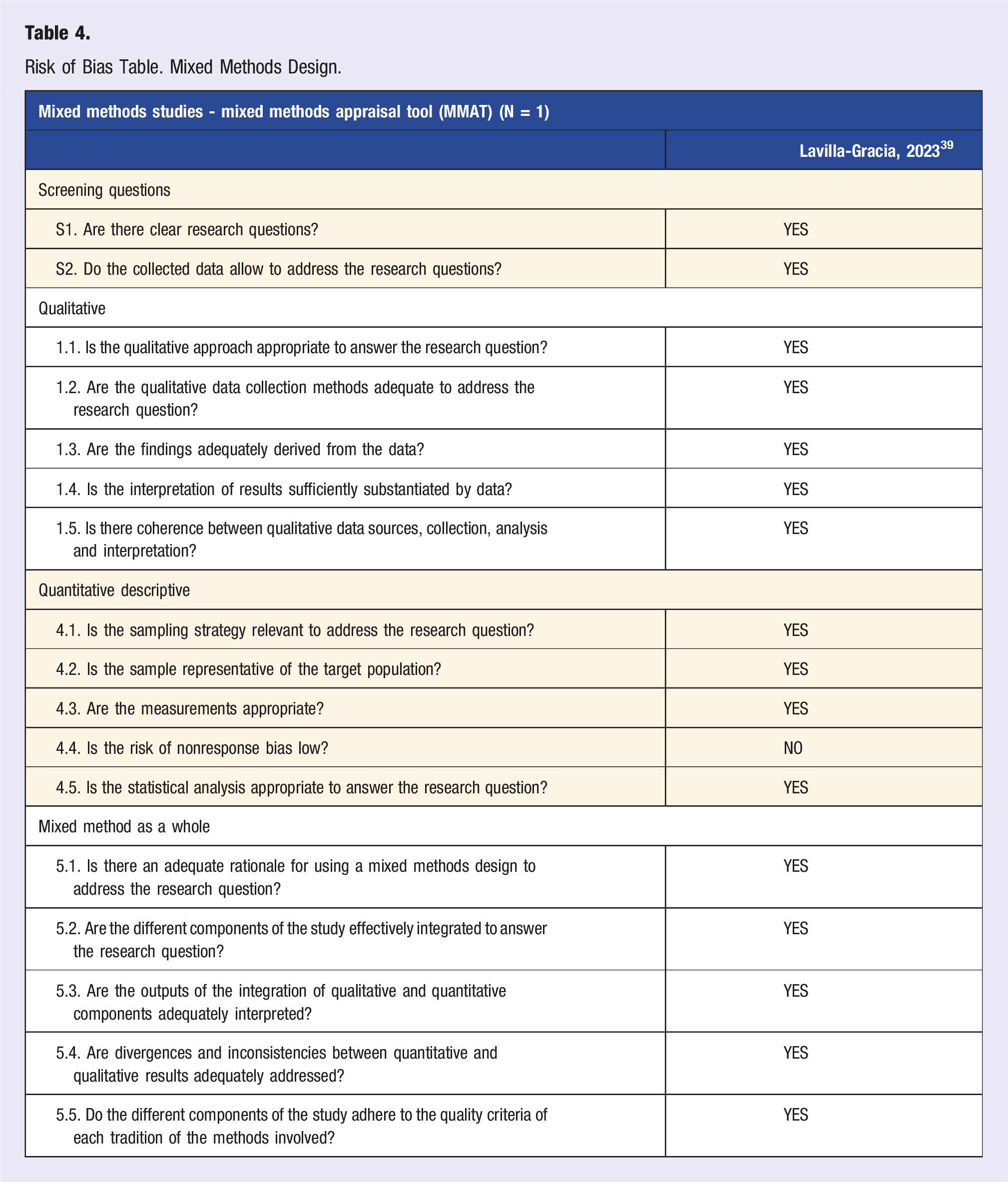
Risk of Bias Table. Mixed Methods Design.
Statistical Analysis
Baseline Characteristics of Studies.
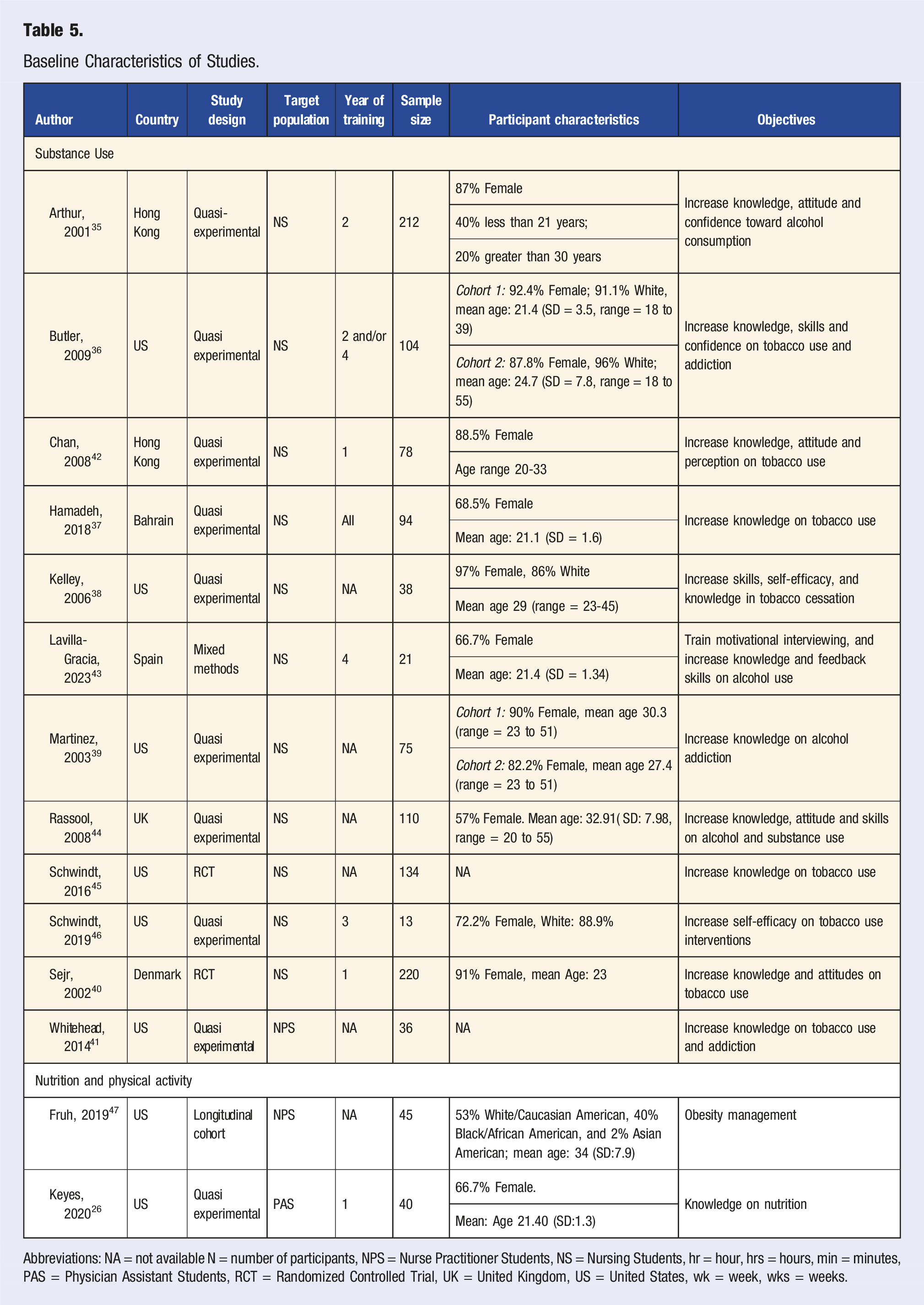
Abbreviations: NA = not available N = number of participants, NPS = Nurse Practitioner Students, NS = Nursing Students, hr = hour, hrs = hours, min = minutes, PAS = Physician Assistant Students, RCT = Randomized Controlled Trial, UK = United Kingdom, US = United States, wk = week, wks = weeks.
For all analysis with sufficient power, we performed sensitivity analysis with different pre–post correlation values (0.3, 0.5 and 0.7) to assess the robustness of the provided estimates. To explore potential sources of heterogeneity among meta-analysis with high level of heterogeneity and sufficient power, we conducted analysis by stratifying studies based on intervention characteristics. First, studies were stratified by Delivery Method into “course” and “lecture” intervention. Second, studies were categorized by duration into interventions delivered in “multiple sessions” vs “single sessions.” Sensitivity analyses were performed to assess the robustness of the meta-analytic results, including the exclusion of studies identified as potential outliers, and a stratification based on country. We refrained from performing a meta-regression given the limited number of observations and prone to overfitting. While heterogeneity remained high after the aforementioned sensitivity analyses, we further assessed the robustness of our meta-analytic estimates through influence diagnostics and stepwise sensitivity analyses. Influence analysis was conducted using Cook’s Distance, DFFITS, and tau 2 deletion analysis to evaluate the impact of study removal on between-study variance. 49 A stepwise sensitivity analysis was performed by iteratively removing high-leverage studies and recalculating heterogeneity statistics. Further, we conducted a Bayesian sensitivity analysis using an informative normal prior on the pre–post correlation coefficient r (mean = 0.5, SD = 0.1),50–52 recalculating Hedges’ g and its variance across a plausible range of r values (0.3 to 0.7). Random-effects meta-analyses were then performed at each level of r, and posterior-weighted effect sizes were computed. In addition, for all outcomes where multiple effect sizes per study were available, we fitted robust variance estimation (RVE) models using the “robumeta” package with hierarchical weights, following current recommendations for small meta-analyses.53,54 All formulas used to perform the statistical analysis are described in Table S1.
Role of the Funding Source
The study was supported by internal institutional funds.
Results
Search Outcome and Study Characteristics
Of the 6, 253 studies originally screened, 206 full-text articles were assessed for eligibility and 14 were included. The PRISMA flow diagram is presented in Figure 2. The reasons for excluding articles were related to (i) no description of the LM intervention; (ii) incorrect target population (e.g., being faculty, HCPs and patients); and (iii) wrong/unrelated outcomes (e.g., oral health). The studies encompassed randomized controlled trials (n = 2, 14%),55,56 quasi-experimental (n = 10, 71%),57–66 one mixed methods (7%),
67
and 1 longitudinal cohort (7%).
68
All studies were published between 2001 and 2023. Participant numbers for the studies widely ranged from 13 to 220. PRISMA flow diagram.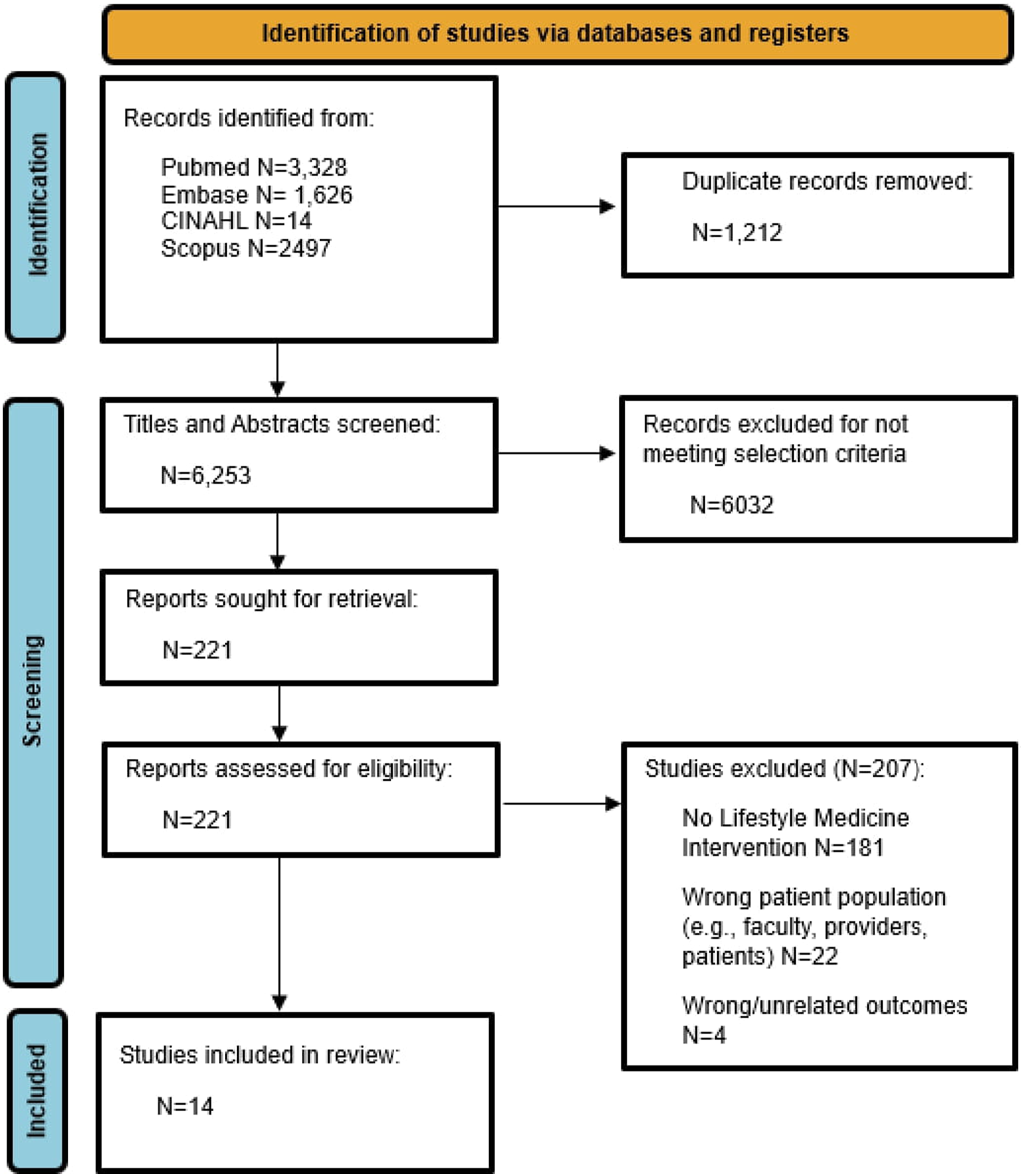
Of the 14 studies, more than half (n = 8, 57%) were conducted in the United States,55,58,61,62,64,68,69 3 in Europe; Denmark (n = 1, 7%), 56 Spain (n = 1, 7%), 67 the United Kingdom (N = 1, 7%)63] and 3 in Asia; Hong Kong (n = 2, 14%),57,59 and Bahrain (n = 1, 7%]60. Further, of the 14 studies, the majority involved trainees from nursing (n = 11, 79%),55–64,67 nurse practitioner (n = 2, 14%),65,68 and 1 physician assistant (7%) programs. 66 Of the 14 studies, 43% (n = 6) did not specify the year of training,55,61–63,65,68 and among the others (n = 8, 57%) the years ranged from first year to all years of the respective health professionals program.56–59,64,66,67
Educational Intervention Description
The LM educational interventions were integrated in mostly public institutions (64%), embedded within mandatory classes (64%) and delivered by faculty (100%). The LM educational interventions were predominately delivered through modules (57%), followed by lectures (29%), and courses (11%), with problem-based learning accounting for 4%. The common mode of delivery for the LM educational interventions was in-person (75%) for an average duration ranging from 1 to 24 h (Table 5).
LM Characteristics
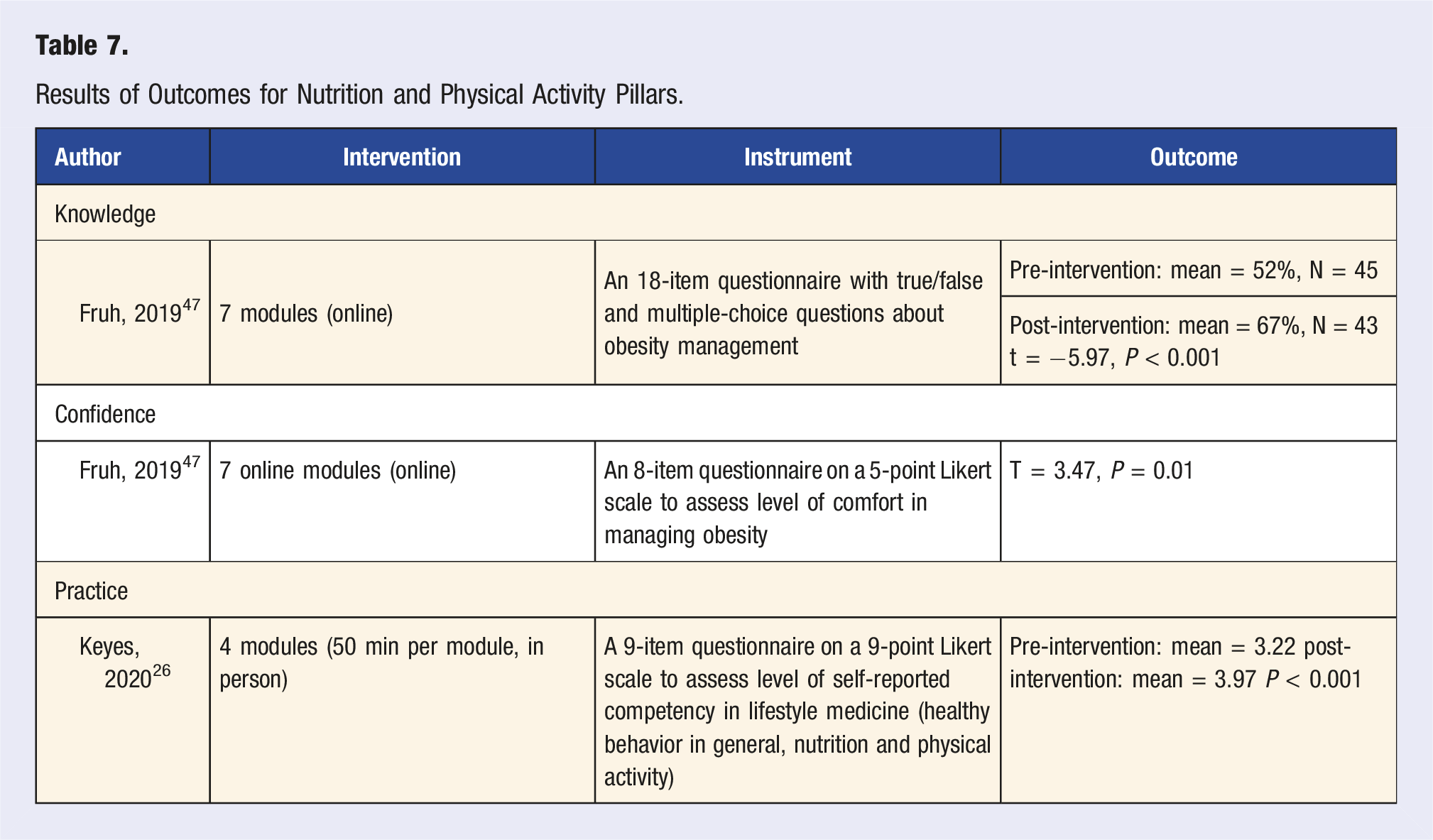
Specific to the LM pillars, 12 studies (86%) focused on substance use, and 2 (14%) addressed nutrition and physical activity. No studies were retrieved for the other LM pillars—sleep health, social connectedness and stress. A summary of the baseline characteristics of the 14 studies are presented in Table 5.
Substance Use Pillar
Among the 12 studies that focused on the substance use pillar of LM, the majority (n = 8, 67%) aimed to improve knowledge, attitudes, work satisfaction, confidence, or skills related to tobacco misuse or cessation. The remaining studies (n = 4, 33%) targeted alcohol or other substance misuse. The educational interventions were primarily delivered in person (n = 9, 75%), with some utilizing a hybrid approach of online and in-person methods (n = 2, 17%) or solely conducted online (n = 1, 8%). Across these studies, 11 interventions were aimed at increasing knowledge, 9 at improving attitudes, 2 at enhancing work satisfaction, 8 at boosting self-esteem/confidence, and 9 at advancing practice/skills.
Outcome: Knowledge
Results of Outcomes for Substance Use Pillar.

aNo differences between the 2 groups (6-h- and 2-h intervention) in pretraining skill, knowledge, or activity scores. Significant difference between the 2 groups on mean baseline confidence score, with the 6-h group (seniors) being more confident at the initial assessment (mean = 30.5, SD = 7.2) than the 2-hour group (mean = 25.9, SD = 7.1) (t = 3.2, P = 0.002).
bsignificant difference between control and intervention group.
cno significant difference between 2 groups.
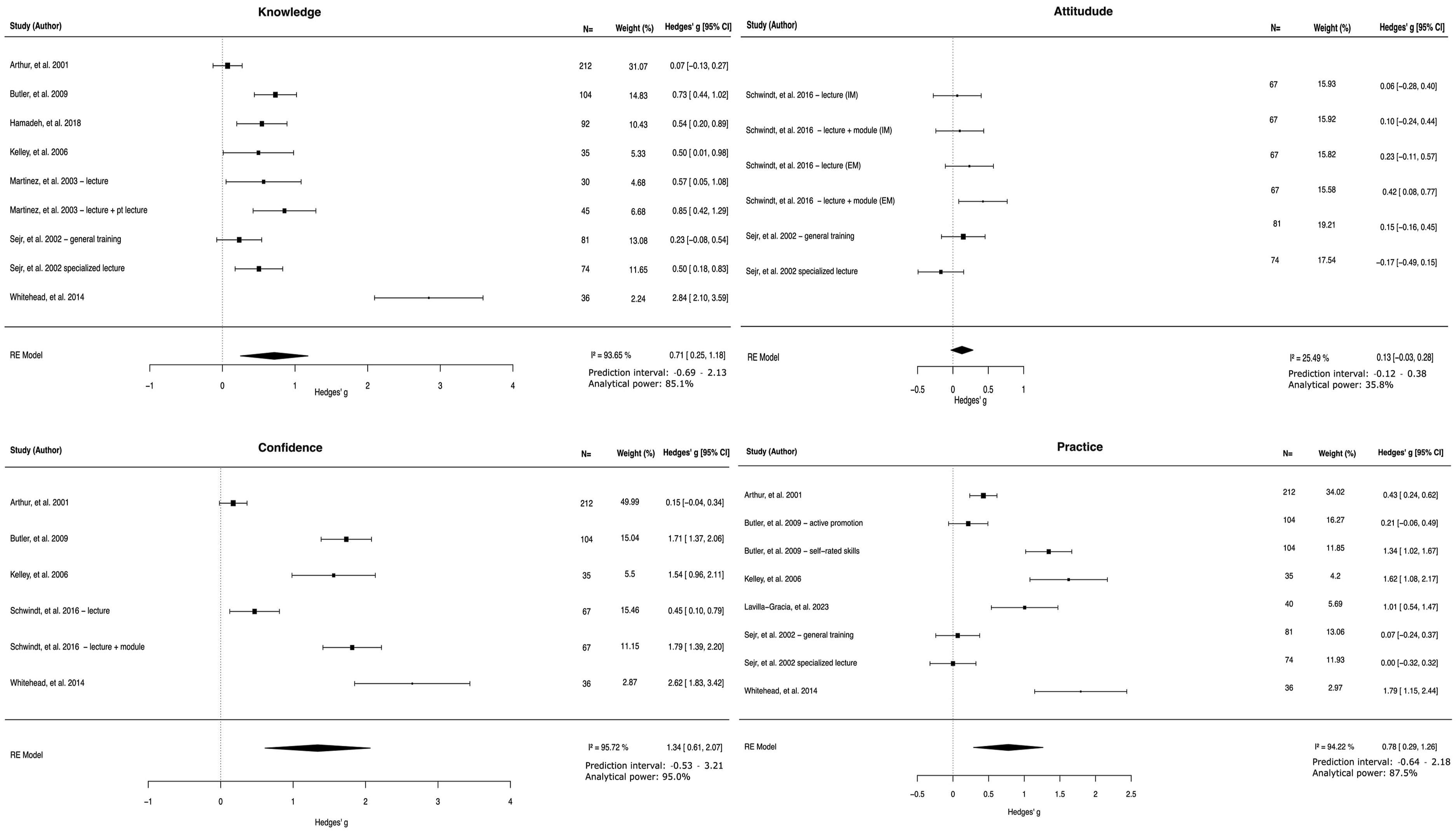
Meta-analysis.
Outcome: Attitudes
Four studies described 9 educational interventions that aimed to increase attitude; however, none used the same instrument (Table 5). Data to calculate the SMD was provided by 2 studies describing 6 educational interventions; 1 on general attitude, 56 and 1 on intrinsic motivation and extrinsic motivation. 55 The RE meta-analysis showed an insignificant effect of these educational interventions on attitudes SMD: 0.13 (95%CI: −0.03 – 0.28, PI: −0.12-0.38) with a moderate level of heterogeneity (I2: 25.49%) (Figure 3). Analytical power for this meta-analysis was 35.8%.
Two studies did not provide sufficient data to calculate a SMD: one showed that the educational intervention of a 2-h online module and 3-h in person training significantly increased the intent to ask about tobacco use and provide counseling for tobacco cessation, 64 the other one found no absolute difference in number of misconceptions in attitudes and beliefs after a 2-h in person lecture. 59
Outcome: Work Satisfaction
Two studies described work satisfaction, both using different instruments to assess (Table 6). One showed a significant improvement regarding work satisfaction after a 5-week problem-based learning intervention. 57 The other study only showed results after the educational intervention, 67 showing that work satisfaction was high (mean = 4.5 out of 5). There was insufficient data to perform a meta-analysis.
Outcome: Self-esteem/confidence
Seven studies described 8 educational interventions, of which 2 used the same instrument (Table 6). Five studies describing 6 educational interventions provided data to calculate a SMD.55,57,58,61,65 Meta-analysis, including 521 participants, showed an overall SMD of 1.34 (95%CI: 0.61 – 2.07, PI: −0.53 - 3.21) with a high level of heterogeneity (I2 = 95.7%) (Figure 3). Retrospective power analysis showed an analytical power of 95.0%. Two studies did not provide enough data to calculate an SMD, both show that their intervention significantly improved confidence in counseling.63,64
Outcome: Practice
Seven studies described 9 educational interventions, of which 2 used the same instrument to measure the outcome58,61 (Table 6). Six studies provided data to perform a meta-analysis.56–58,61,65,67The overall effect size was significant with a SMD: 0.78 (95% CI: 0.29 – 1.26, PI: −0.64 – 2.19) and a high level of heterogeneity (I2: 94.2%). Retrospective power analysis indicated an analytical power of 87.5%. One study did not provide sufficient data to calculate a SMD, but showed a significant increase in counseling abilities in tobacco cessation. 64
Nutrition and Physical Activity Pillars
Results of Outcomes for Nutrition and Physical Activity Pillars.
Stratification on Delivery Methods and Duration
Knowledge
Stratification by delivery method showed that course-based interventions had non-significant effects with high heterogeneity, whereas lecture-based interventions were significantly effective with low heterogeneity. Stratifying by duration revealed that multiple-session interventions were non-significant with high heterogeneity, whereas single-session interventions were significantly effective with moderate heterogeneity (Figure S1).
Confidence and Practice
For both confidence (Figure S2) and practice (Figure S3) the single study for lecture-based interventions was not considered. Effect sizes remained significant across stratification. No difference in heterogeneity was observed.
Sensitivity Analysis
Different Pre–Post Correlation Values
Obtained estimates remained significant and consistent when different pre–post correlation values were used (Table S2).
Excluding Outliers
In the sensitivity analysis, we excluded Whitehead, et al (2014) 65 as a potential outlier in the meta-analyses performed for knowledge, confidence and practice. All effect sizes remained significant, while heterogeneity went from high to moderate for the knowledge outcome (Figures S4-6).
Stratification Based on Country
In the second sensitivity analysis, we performed meta-analyses stratified studies based on country. This was only possible for the US, as there was insufficient data for the other countries to perform a meta-analysis. All effect sizes remained significant, while heterogeneity went from moderate to low for the attitude outcome (Figures S7-9).
Influence Diagnostics and Stepwise Sensitivity Analysis to Reduce Heterogeneity
After excluding high-leverage studies identified through influence diagnostics and stepwise sensitivity analysis, heterogeneity was reduced while effect sizes remained significant and directionally consistent (Table S3). For knowledge, removing Arthur (2001), Whitehead (2014), and Butler (2009) reduced heterogeneity from high to low (I2 = 18.90). For confidence, excluding Arthur (2001) and Schwindt (2016) eliminated heterogeneity (I2 = 0). For practice, removing Arthur (2001) and both arms of Sejr (2002) lowered heterogeneity to a moderate level (I2 = 35.17%).
The posterior-weighted SMDs were 0.956 (SE = 0.317) for Knowledge, 0.129 (SE = 0.083) for Attitude, 1.714 (SE = 0.561) for Confidence, and 0.887 (SE = 0.364) for Practice. RVE models yielded pooled estimates consistent with the Bayesian analyses: knowledge (SMD = 0.68, SE = 0.21, P = 0.016), attitude (SMD = 0.13, SE = 0.10, P = 0.36). confidence (SMD = 1.34, SE = 0.33, P = 0.02), and practice (SMD = 0.76, SE = 0.22, P = 0.016).
Discussion
Health care providers are trusted sources of health information and are in a unique position to have a profound impact on addressing the escalating burden of NCDs. In the ever-changing landscape of healthcare, LM is uniquely positioned to empower patients and communities to make sustainable lifestyle habits, prevent NCDs, and improve patient’s overall health and outcomes14,70,71 (p. 959). This study is the first, to our knowledge, to critically synthesize the literature on the current state of LM integration in health professionals’ curricula and quantify the effectiveness of such educational interventions on the knowledge, skills and competence among health professional trainees. The results showed a relatively smaller quantity of published studies regarding LM educational interventions in health professionals curricula compared to medical trainees—for example, an estimated 3 quarters of the published LM educational literature pertains to medical programs. 30
Overall, the LM educational interventions embedded within the health professionals’ curricula had a statistically significant and positive impact on increasing LM-related knowledge, confidence and practice among health professional trainees, particularly related to the substance use, nutrition, and physical activity pillars. There was insufficient power to provide reliable estimates for the attitude outcome. Both RE meta-analysis and Bayesian analyses showed inconclusive results. Additional studies with larger sample sizes are needed to obtain reliable effect estimation in this domain. Furthermore, there remains a significant gap in the LM educational literature on the sleep health, social connectedness, and stress management pillars. The findings from this review are consistent with the limited but current LM and educational literature.30,31,72 As an illustration, across the international medical schools sampled (N = 106), education on sleep health was found to be under 2.5 h and 27% of the responding schools did not provide any sleep health education. 73 Similar findings were reported with the social connectedness and stress pillars of LM—with insufficient data available to report on the hours of related education in the UGME curricula. 36 These findings are in parallel with a systematic review on nutritional education provided to medical trainees (N = 24). Specifically, nutritional education was found to be insufficiently incorporated in medical curricula, 31 which has implications on medical trainees being able to develop their knowledge, skills and confidence in providing nutrition-related care to patients in clinical practice. 31 Additionally, in a systematic review on RNs’ perceptions of their roles with promoting physical activity to patients , they had (i) poor knowledge of related guidelines; (ii) limited training, skills and techniques to educate and advise patients on physical activity; and (iii) lack of skills to develop care plans to promote physical activity for patients. 72
Further to the integration of only half of the LM pillars in the health professionals’ curricula found in this study, most were incorporated in U.S. based academic institutions. This finding is in parallel with a scoping review on culinary medicine for nutritional education in medical schools. 74 Potential explanations to this geographic footprint are fourfold: (i) the increasing interest in LM in general and as a paradigm shift in the prevention and/or management of modifiable risk factors associated with NCDs in North America; (ii) recognized LM-related guidelines such as the American Heart Association 75 and the American Diabetes Association 76 ; (iii) the American College of Lifestyle Medicine (ACLM) which has established undergraduate medical education courses, certifications, residencies and fellowships 36 ; and (iv) the Resolution 959 (I-17) supporting policies that incentivize and provide funding for the inclusion of LM and social determinants of health in medical education in the United States. 71
The LM educational interventions within the respective programs were also predominately delivered in-person and through lecture format. This finding is aligned with reviews on culinary medicine and LM in medical curricula.30,74 While the delivery of content through lectures is a commonly used approach in health professional’s curricula, alternative and more innovative pedagogical approaches can be easily integrated in existing courses. For instance, simulation provides health professional trainees with an authentic clinical environment that supports enhancement in knowledge, refinement of skills (e.g., communication, counseling, teaching) as well as the ability to bridge the gap from knowledge acquisition (theory that is commonly attained in the classroom, didactic learning) to knowledge application (e.g., interactive workshops).77,78 Such innovation was illustrated in a LM educational intervention that integrated clinical simulation for nursing students to address social isolation and loneliness among older adults. 77 In the quasi-experimental study that encompassed a simulation program (asynchronous theoretical training and synchronous practicing training using an online platform) among nursing students (N = 25, 27.44 years, 76% women), statistically significant improvements (P < 0.05) with knowledge and attitudes as well as their ability to address loneliness and social isolation towards older adults was reported. 77 Likewise, simulation is being used for educating nursing, psychology, social work, medical trainees and dietitians on the substance use 79 and nutrition 78 pillars.
The pace of advancement and discoveries in science to improve patient health outcomes and clinical practice requires continued integration of new material in existing health professionals curricula.
18
Such programs often have long-standing education models and processes,
18
causing curricula tensions and challenges. However, a solution to such challenges is a tailored approach to the respective health professional’s programs through several ways (Figure 4). First, is through curriculum mapping, which is instrumental to identify patterns, overlaps, and gaps in a strategic way to enhance curricula
80
afforded to health professional trainees as future HCPs. As an illustrative example, the authors conducted a content analysis of LM curriculum in Canadian UGME to identify the current state and gaps with the intent of informing future educational interventions to enhance medical trainee’s LM-related knowledge, skills and competencies in Canada.
81
Second, is the use of existing and established modules, materials, courses and professional development opportunities that can be integrated rather than added to minimize curriculum overload. For example, the ACLM has developed an introductory LM course with the curriculum delineated along with the slide decks and teacher’s manual.
82
Further, the Institute of Lifestyle Medicine through Harvard Medical School’s Department of Continuing Education and the American College of Preventive Medicine deliver a 2-day workshop with online materials
83
as well as a 30-h comprehensive LM course through webinars,
84
respectively. Finally, is the use of available LM-related frameworks and competencies that are currently geared towards UGME that can be easily adapted to guide health professional school deans and program directors on systematic and strategic ways to integrate learning objectives and content. Examples of core LM-related frameworks and competencies include the American Heart Association general framework for US medical schools,
18
LM competencies published in the American Journal of Lifestyle Medicine,
85
and nutrition competencies published in the Journal of the Medical Association.
86
Appreciating the intersection of lifestyle and health care, LM is integral in health professionals curricula to equip trainees and the future generation of HCPs with the knowledge, skills and competencies to meaningfully and effectively integrate in practice as an antidote
36
for the prevention, management and treatment of NCDs, and consequential complications such as stroke, heart disease, cancer or dementia. Study implications.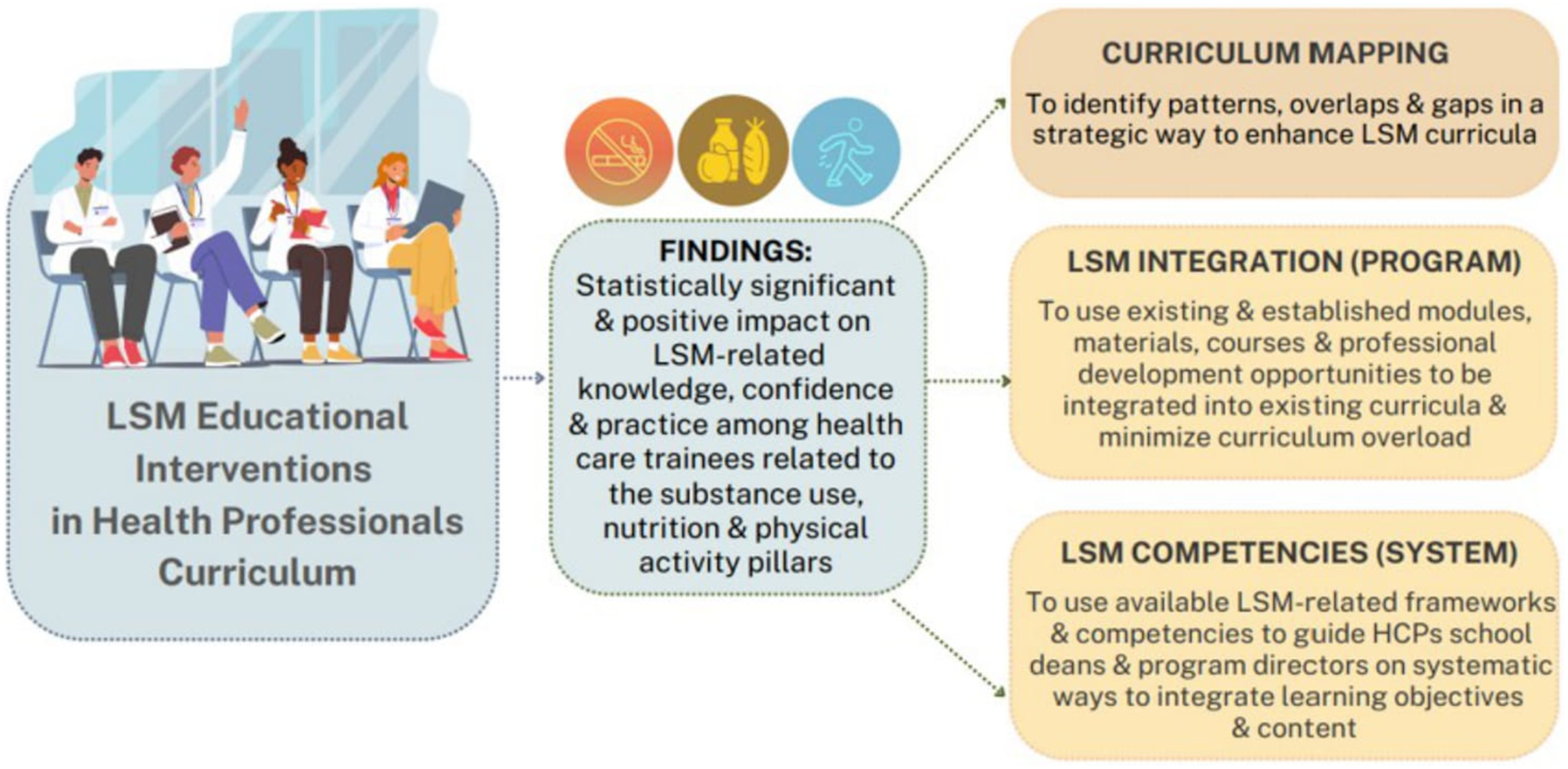
Limitations
This systematic review and meta-analysis have several limitations. First, the findings from meta-analyses should be interpreted with caution due to the high level of heterogeneity and wide prediction intervals. Differences in study populations, interventions, and outcome measures contributed to this variability. This may make the results more suitable for providing an overall overview rather than definitive conclusions as well as identifying gaps in the literature to be addressed in future research studies. Due to the limited number of studies, meta-regression was not deemed feasible. Influence diagnostics identified Arthur (2001) as a key driver of heterogeneity across all outcomes, despite similar study characteristics. The remaining heterogeneity, particularly from Whitehead (2014), Butler (2009), Schwindt (2016), and Sejr (2002), remains unexplained, suggesting unmeasured methodological differences. However, removing these studies reduced heterogeneity while maintaining effect size directionality, statistical significance, and yielding narrower prediction intervals. These sensitivity analyses strengthened the robustness of the study findings. Second, sensitivity analysis showed lower levels of heterogeneity among participants receiving lecture-based or single-session interventions compared to those in multi-session or course-based formats for the knowledge outcomes. This might suggest that the more streamlined and less complex interventions yield more consistent outcomes. However, we did not observe a similar trend for confidence and practice. Third, while we followed the terminology used in the original articles to categorize outcomes (e.g., labeling a questionnaire as measuring “practice”), there may be arbitrariness in these classifications. Specific definitions for the outcomes were not uniformly applied, which may affect the consistency and interpretation of the results. Fourth, while we tested a limited number of hypotheses, with additional analyses conducted solely to assess robustness, we acknowledge that multiple comparisons may introduce a potential risk of Type I errors. Finally, there was insufficient power to obtain reliable estimates for the attitude outcome. Future studies should aim to include larger, more homogeneous samples and utilize standardized outcome measures to enhance the power and precision of meta-analytic estimates in this domain.
Conclusion
A small (N = 14) but notable body of literature describing LM educational interventions embedded within health professional’s curricula were identified and evaluated based on the effectiveness on improving LM-related knowledge, skills, competence, and practice. Findings from the systematic review and meta-analysis showed that LM educational interventions when delivered have a statistically significant and positive impact on health care trainee’s LM-related knowledge, confidence and practice particularly related to the nutrition, physical activity and substance use pillars, while there was insufficient power for the attitude outcome. Significant gaps continue to exist on the sleep health, social connectedness and stress management pillars. Study findings highlight several notable implications: (i) curriculum mapping to support the systematic identification of patterns, overlaps and gaps for LM-related content within health professionals’ programs; (ii) use of existing and established modules, courses and materials to integrate within existing health professional’s programs; and (iii) adapting existing frameworks and competencies that are geared towards UGME towards health professionals. Recognizing the rising global prevalence of NCDs and the associated increase in concordant health care expenditure, LM is strategically poised in a unique point in time to rethink and redesign health professionals’ curricula to better prepare future generations of HCPs to support the health and well-being of persons, communities and populations.
Supplemental Material
Supplemental Material - Lifestyle Medicine Education in Health Professionals Curricula: A Systematic Review and Meta-Analysis
Supplemental Material for Lifestyle Medicine Education in Health Professionals Curricula: A Systematic Review and Meta-Analysis by Sarah Ibrahim, RN, MN, PhD, CHSE, Jasper R. Senff, MD, Janani Sivakumar, BSc(Hons), Matthew Ventresca, MSc, MBA, CHE, CCRP, Judith Coulson, MSN, NP, Sanjula Singh, MD, PhD, and Aleksandra Pikula, MD, DipABPN, DipABLM in American Journal of Lifestyle Medicine
Footnotes
Author Contributions
SI supervised the study conception, design, data collection and led the manuscript preparation. JRS assisted with the study conception, led the data analysis of the study and advised on all components of the study methods, interpretation of study findings, reviewed and approved the manuscript. JS and MV assisted with the data screening and extraction as well as reviewed the manuscript. SS assisted with the study conception and advised on the data collection and analysis as well as reviewed and approved the manuscript. AP provided funding through the center and advised on the study conception and design, data collection, manuscript preparation, and reviewed and approved the manuscript. All authors approved the submitted version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work is supported by the Jay and Sari Sonshine Centre for Stroke Prevention & Cerebrovascular Brain Health.
Ethical Considerations
This article does not contain any studies with human or animal participants. There are no human participants in this article and informed consent is not required.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.