
Abstract
A systematic review and meta-analysis investigated randomized clinical trials (RCTs) of mindfulness-based interventions (MBIs) targeting lifestyle behaviors commonly associated with brain health in adults. Data sources included Ovid Medline, Ovid PsycINFO, CINAHL [EBSCO], Embase, Cochrane Library [Ovid], Web of Science, and https://ClinicalTrials.gov. Studies were screened using Covidence 2.0. A total of 79 published RCTs of MBIs for adults (18+, patient and non-patient populations) targeting one or more lifestyle behavior (physical activity, sleep, diet, alcohol use, tobacco cessation, and social and mental activities) met eligibility criteria. MBIs were associated with reduced sleep disturbance (40/54 RCTs; 3537 participants; SMD = −.53; 95% CI = −.74 to −.32; I 2 = 78%), increased physical activity (9/17 RCTs analyzed; 685 participants; SMD = .72; 95% CI = .04 to 1.40; I 2 = 89%), improved tobacco cessation (8/12 RCTs; 1234 participants; OR = 2.11; 95% CI = 1.12 to 3.97; I 2 = 55%), and lowered alcohol use (4/6 RCTs; 261 participants; SMD = −.39; 95% CI = −.45 to −.32; I 2 = 0%). This review found moderate to high-quality evidence for MBIs targeting sleep, physical activity, alcohol use, and tobacco cessation. Heterogeneity for these outcomes and insufficient data to analyze diet, mental activities, and cognitive functioning limit our ability to draw definitive conclusions about the effects of MBIs on brain health.
“Mindfulness increases self-awareness, decreases impulsivity, and allows individuals to make intentional lifestyle choices rather than be on automatic pilot.”
Introduction
A large and growing body of research suggests that lifestyle behaviors are critical for brain health. 1 Rather than the absence of illness, recent biopsychosocial definitions of brain health emphasize optimal brain functioning at all ages through the integration of the mind, brain, and body. 2 Physical activity, sleep, diet, alcohol use, tobacco cessation, and social and mental activities have been consistently identified by meta-analyses,3,4 population-based studies,5-7 and public health institutions,8,9 as lifestyle “Pillars of Brain Health.” Engaging in these lifestyle behaviors promotes brain health in many ways, such as reducing the rate and burden of neuropsychiatric illness, slowing cognitive decline, and preserving brain structure with aging,10–15 even in at-risk populations.16,17 Modifiable lifestyle behaviors of brain health are a public health priority because neuropsychiatric illnesses are leading causes of disability and death worldwide, affect >100 million Americans, and cost the US healthcare system over $800 billion annually.18,19 In addition to brain health, lifestyle behaviors are equally critical for the prevention and management of other conditions, such as cancer and cardiovascular disease.20,21 The benefits of modifying lifestyle risk factors begin in midlife or earlier10–14 and accumulate with aging,15,22 underscoring the importance of adopting healthy behaviors across the lifespan.
Mindfulness practices have direct brain health benefits and may promote lifestyle behavior change. Mindfulness is commonly defined as a practice of non-judgmental awareness of the present moment. 23 Mindfulness recruits emotion regulation, attentional and cognitive control, and self-related processes (e.g., monitoring, efficacy) that enhance one’s ability to make healthier choices and cope with stressors that derail lifestyle goals (e.g., urges to overeat or avoid exercise).24-27 Positive associations between mindfulness and brain structure,28-30 cognitive function,28,31-34 and neuropsychiatric illness risk reduction (e.g., chronic stress, depression, cardiovascular disease)35-37 have been observed even through brief practice. 38 Mindfulness training interventions offer a feasible and potentially cost-effective approach to promoting behavior change and brain health.24,39,40
Mindfulness-based interventions (MBIs)—secular, manualized, group-based intervention programs 41 —have had a growing presence in lifestyle medicine and medical settings over the past 20 years. 26 Two of the most validated MBI are mindfulness-based stress reduction (MBSR) and mindfulness-based cognitive therapy (MBCT), which are standardized protocols that consist of 8 weeks of group sessions (2-2.5 hours) that provide education and training in various mindfulness practices (e.g., mindful breathing, body scan).26,42 Researchers have adapted MBSR and MBCT for specific populations (e.g., Mindfulness and Relaxation Training for Insomnia, MRTI) 43 and developed analogous mind-body programs that promote engagement in healthy lifestyle behaviors (e.g., The Stress Management and Resiliency Training, SMART). 44 Systematic reviews and meta-analyses conducted on individual lifestyle outcomes have shown a positive relationship between MBIs and physical activity, 45 sleep, 46 weight loss,26,47 and substance use48,49; however, other studies provided low quality or inconclusive evidence.50,51 To date, no systematic review and meta-analysis has comprehensively examined the effects of MBIs on multiple lifestyle behaviors linked to brain health. Also, there is limited understanding of how design choices—for example, MBIs practices, format, duration—impact lifestyle outcomes.
To address these research gaps, we conducted a systematic review and meta-analysis of published randomized clinical trials (RCT) that evaluated the effects of MBIs on one or more lifestyle behavioral outcomes linked to brain health in adult (age 18 and older) samples. We focused on lifestyle behaviors that could be modified by MBIs (physical activity, sleep, diet, alcohol use, tobacco cessation, and social and mental activities) instead of non-modifiable risk factors that are associated with brain health and disease (e.g., history of dementia or traumatic brain injury). Our first aim was to investigate, following the PICOS framework, 52 the range of research methods used in the RCTs. Our second aim was to estimate the effect size of MBIs on lifestyle behavior outcomes, explore whether the effects differ by study characteristics (patient status, age, sex, MBIs type, control type, intervention duration, risk of bias), and assess RCT quality (Cochrane Collaboration Risk of Bias tool version 1.0 53 and Grading of Recommendations Assessment, Development and Evaluation; (GRADE). 54 The results will identify directions to improve the quality of future studies and provide evidence-based conclusions to guide the use of MBIs to promote brain health.
Online Methods
Literature Search
Our systematic review was conducted according to a pre-registered protocol (PROSPERO# CRD42020193780). We searched the following databases using tailored search strategies for each database: Ovid Medline, Ovid PsycINFO, CINAHL via EBSCO, Embase, Cochrane Library via Ovid, Web of Science, and https://ClinicalTrials.gov. Our literature search was developed and conducted by a medical librarian (author initials LLP) at our academic medical center with experience in systematic reviews and meta-analysis of MBIs. We limited our search to RCTs published from inception to 2020 to ensure that our study on 7 lifestyle outcomes of brain health was feasible. The Supplement contains the full search strategy (eTables 1-6). Our methodology followed the Preferred Reported Items for Systematic Reviews and Meta-Analyses (PRISMA) 55 and Cochrane Handbook for Systematic Reviews of Interventions guidelines. 53
Eligibility Criteria
Study Design
We included published RCTs of MBIs targeting one or more modifiable lifestyle behavior for brain health (see Outcomes section). The comparison condition included active, waitlist, no intervention, or a combination of these groups. We excluded studies that were: (1) not peer-reviewed (manuscripts, abstracts, presentations, book chapters, protocols, dissertations), (2) not original RCTs that reported quantitative outcomes (secondary analysis, follow-up, observational, qualitative, cases studies, non-randomized open pilots), (3) incomplete trials (protocol papers), (4) narrative and systematic reviews, and (5) not published in English due to lack of resources for translation.
Population
We included studies of adults (age 18 and older) because lifestyle behaviors are important for brain health across the adult lifespan.1,56 We included both patient and non-patient samples to compare the effects of MBIs and to inform the primary and secondary prevention of brain health risk factors. We included cardiac diseases, cancer, and other chronic conditions because they are impacted by lifestyle behaviors and MBIs and can affect brain health.20,21,26 We excluded treatment studies for serious medical (e.g., medically unstable or declining, requiring hospitalization) or psychiatric illness (e.g., substance use, suicidal and homicidal ideation, psychotic disorders) that would require a higher level of care than an outpatient MBIs. 26
Intervention
We defined MBIs as programs that teach the practice of non-judgmental awareness of the present moment as the primary treatment mechanism. We included secularized MBIs because they are more likely to be integrated into standard clinical practice, have a growing tradition in medicine, and allow for a broader appeal to more patients than religious practices (e.g., prayer). 57 We included MBSR, MBCT, and other MBIs that lasted at least two weeks (or a minimum of two sessions) to ensure a sufficient dose. 26 This criteria also allowed us to distinguish MBIs from non-clinical laboratory studies of mindfulness. 26 We excluded interventions that do not use formal mindfulness meditation as the primary intervention component (i.e., occurring in less than half of the sessions), such as cognitive behavioral therapy, dialectical behavioral therapy, acceptance and commitment therapy, stress/resiliency programs, Pilates, Tai Chi, yoga, progressive muscle relaxation, or deep breathing (i.e., as a stand-alone intervention).26,58 We excluded studies that combined mindfulness with medication to prevent treatment confounds. 59
Outcomes
Our co-primary outcomes are self-reported “Lifestyle Pillars” of brain health consistently identified in literature: physical activity, diet, sleep, alcohol use, tobacco cessation, social and mental activities.60,61 We extracted and analyzed each lifestyle outcome separately because (1) there are no single instruments that assess all of the lifestyle behaviors, 62 (2) existing multidomain instruments 63 are not widely used, and (3) analyzing the effects of MBI on individual lifestyle outcomes has utility for informing behavioral targets in clinical practice. In addition to lifestyle outcomes, we extracted cognitive functioning as an exploratory outcome given our focus on the effects of MBIs brain health. The Supplement includes full MeSH terms to define the lifestyle (primary) and cognitive (exploratory) outcomes in our search strategy. We prioritized analyzing the most commonly reported measure among the included trials when studies reported two or more lifestyle measures of the same type (e.g., two physical activity questionnaires). 58
Study Selection and Data Extraction
Two trained reviewers independently screened all studies for inclusion and exclusion criteria in three stages (title, abstract, and full text) using a standardized protocol and forms in Covidence version 2.0. 64 The principal investigator (author initials RAM) resolved disagreements at each stage to determine the final studies included in the review. We contacted corresponding authors when necessary to request full texts, pertinent unpublished data, and clarify methods or results. We extracted the following data: age, sex, population, MBIs and control type, duration, and outcome measures (sample size, mean, and standard deviation). When the outcomes data were incomplete, we imputed them using available data65-67 and conducted sensitivity analyses. 68
Risk of Bias and Quality Assessment
We evaluated all studies included in the review with the Cochrane Collaboration Risk of Bias tool version 1.0 53 and analyzed them in R 69 with RStudio 70 and the robvis 71 package. Two trained raters independently assigned each of the following domains (sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting, and other sources of bias) as low, unclear, or high risk using standardized forms in Covidence. The first author (RAM) resolved disagreements between the raters or consulted with the overall team to reach a consensus. We evaluated the quality of the evidence for each lifestyle outcome using the GRADE criteria 54 in the GRADEpro GDT software. 72
Meta-Analysis
We conducted the meta-analysis with R packages73,74 informed by similar studies.26,58 We calculated the standardized mean difference (SMD; Hedges’ g) between the MBIs and control at the post-intervention endpoint in a random-effects model for each lifestyle outcome using restricted maximum likelihood (REML). 53 We were unable to analyze secondary endpoints due to a lack of follow-up data reported by included studies. We pooled the means, standard deviations, and sample sizes of studies that included more than one control group. We assessed statistical heterogeneity between trials using the I 2 statistic. 75 We weighted the effects using the generic inverse variance method. We assessed bias in the meta-analysis results using both visual inspection (funnel plots) and statistical (Egger’s regression test) methods. 76 We interpreted statistical significance using the conventional two-tailed α < .05. After assessing the main outcomes, we examined whether the heterogeneity in MBIs effects significantly differed by the following subgroups: (1) patients vs non-patients, (2) age (sample mean), (3) sex (sample percent female), (4) MBIs type (e.g., MBSR, MBCT, or other), (5) control type (i.e., active, waitlist, usual care), (6) intervention duration, and (7) risk of bias (high vs low).
Results
Literature Search
Figure 1 presents the PRISMA of RCT identification and selection. Our initial search resulted in 7985 potential articles, 199 of which met our eligibility criteria. A total of 79 articles (9233 total participants) met full-text eligibility criteria and were included in the systematic review and meta-analysis (eTable 7). The most common reasons for exclusion were: study did not meet set criteria for MBIs (n = 30), study was non-RCT (n = 19), and study lacked lifestyle outcomes (n = 14). Table 1 PRISMA diagram of trial identification and selection. Full Details of Included Participants and Studies.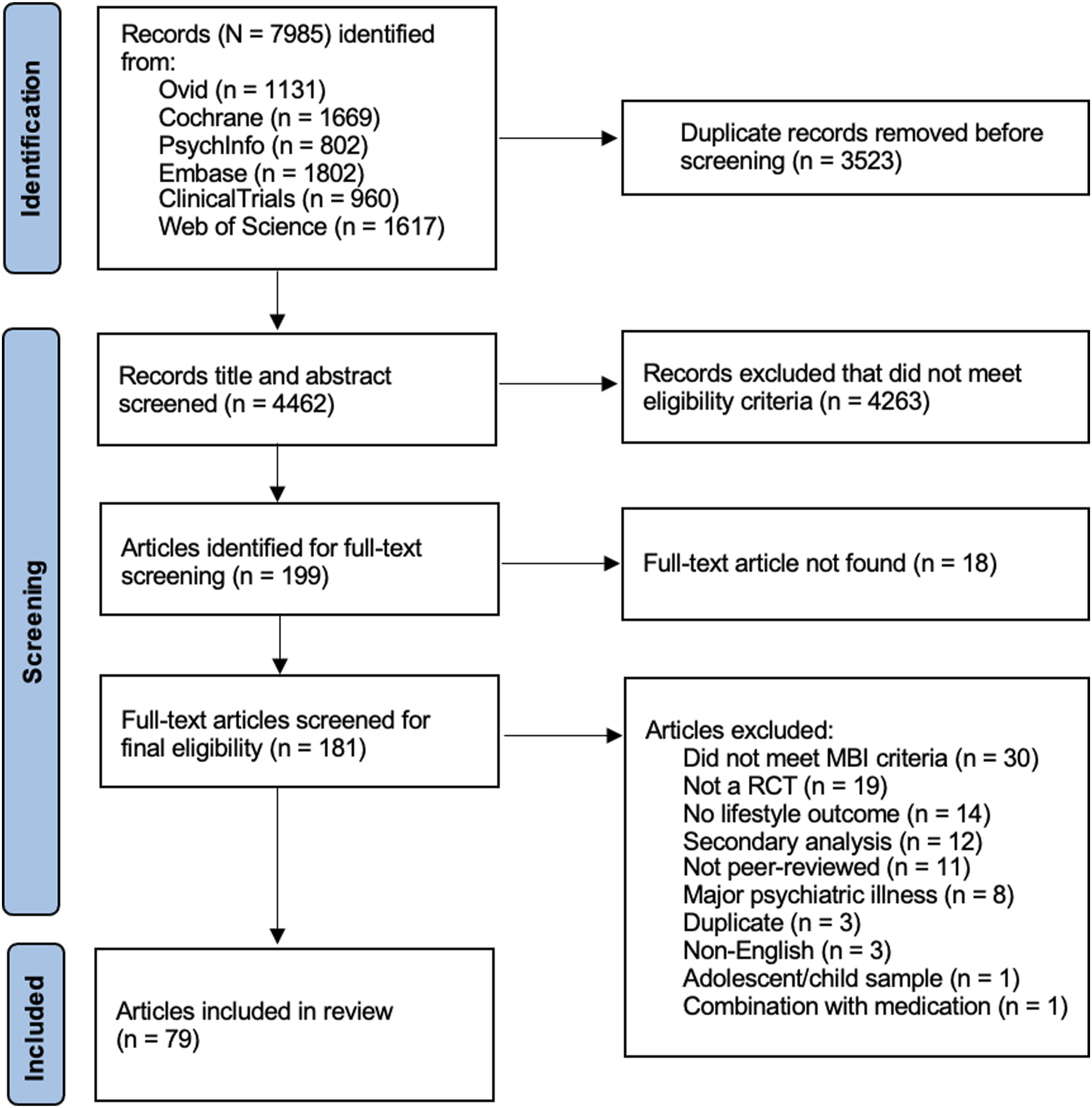

Included Studies
The characteristics of included participants and studies are summarized in eTable 8 and are fully listed in eTable 9. Included studies were published between 2009 to 2020 with an increase over time (min = 2 in 2009, max = 12 in 2019). The average sample size was 116.87 (SD = 152.83, min = 21, max = 1255) and the average age was 46.75 (SD = 11.58, min = 20.16, max = 78.57). The samples were predominately Female (76.71%). There was even representation of both patients (n = 46, 58%) and non-patient (n = 33, 42%) samples. The most common MBIs were to promote general health and wellbeing in healthy adults (n = 24, 30%, e.g., increase social connection in a non-clinical sample), followed by MBIs for lifestyle behaviors in medical populations such as cancer (n = 17) and tobacco cessation (n = 10, 13%) (see eTable 8 for all categories).
eTable 9 reports the intervention and control characteristics. The most common form of MBIs were programs developed by the researchers to promote lifestyle behaviors in specific populations. MBSR and MBCT were used in 25 (32%) and 4 (5%) studies, respectively. The majority of MBIs were in-person (n = 66, 84%), delivered in a group format (n = 65, 82%), and lasted approximately 8 weeks on average (M = 7.89, SD = 4.22, min = 2, max = 24). Nearly half of the studies (n = 36, 46%) used an active control. The majority of studies (n = 56, 71%) reported that the MBIs group was superior to the control at post-intervention (19% both improved, 6% neither, 3% control improved, 1% unclear).
The greatest source of bias was incomplete outcome data due to attrition at the post-intervention assessment (over 25% of included RCTs). There were some concerns regarding allocation concealment, blinding of outcome assessors, and blinding of participants and personnel. This is likely attributed to insufficient reporting about these procedures and the challenge of blinding in behavioral interventions. See eFigure 1 for risk of bias assessment summary plots, which were similar when analyzed with and without accounting for sample size.
Lifestyle Outcomes (Co-Primary)
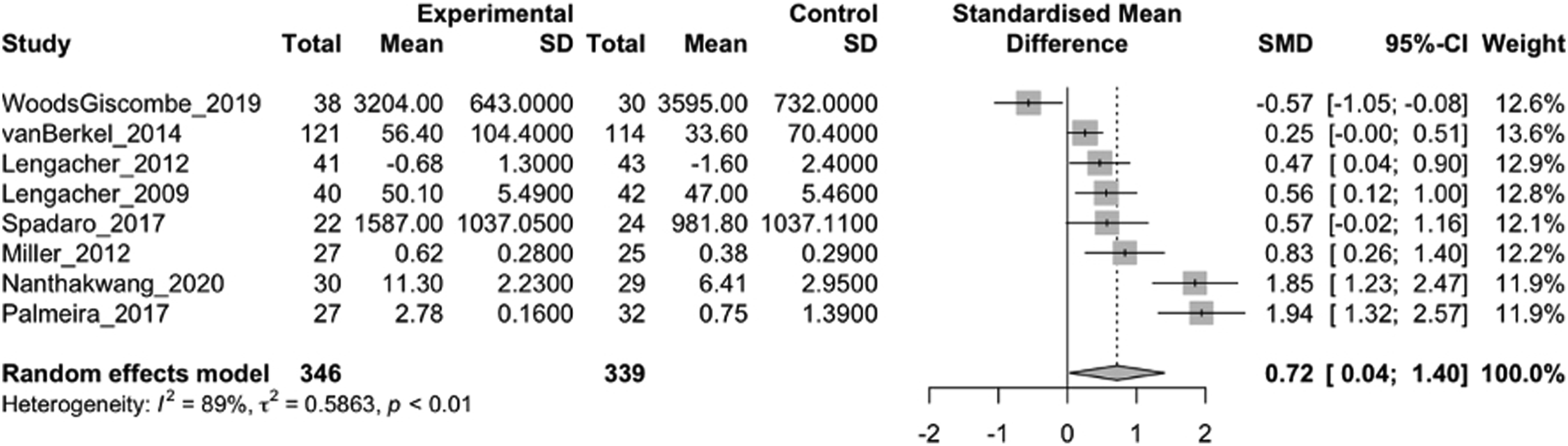
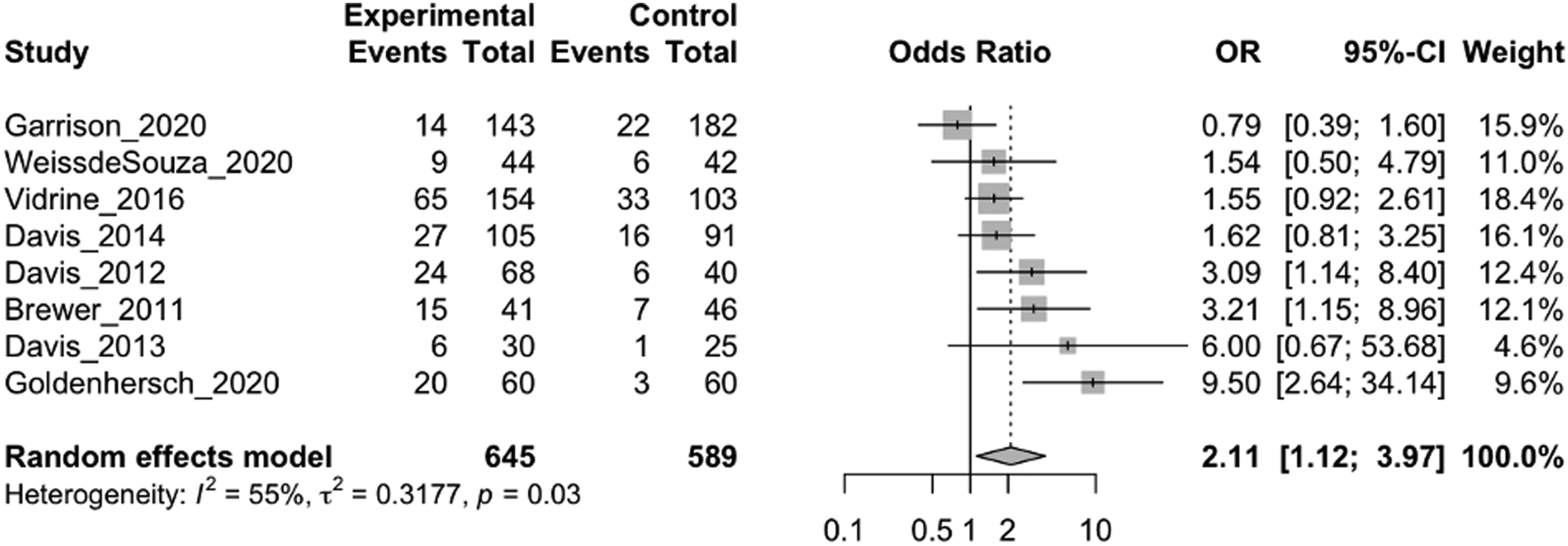
eTable 10 reports the lifestyle outcome measures. MBIs were associated with post-intervention reductions in sleep disturbance (40/54 RCTs analyzed; 3537 participants; SMD = −.53; 95% CI = −.74 to −.32; I
2
= 78%), increases in physical activity (9/17 RCTs analyzed; 685 participants; SMD = .72; 95% CI = .04 to 1.40; I
2
= 89%), greater odds of tobacco cessation (8/12 RCTs analyzed; 1234 participants; OR = 2.11; 95% CI = 1.12 to 3.97; I
2
= 55%), and lower alcohol use (4/6 RCTs analyzed; 261 participants; SMD = −.39; 95% CI = −.45 to −.32; I
2
= 0%). MBIs were not significantly associated with social activity (7/9 RCTs analyzed; 552 participants; SMD = .46; 95% CI = −.36 to 1.28; I
2
= 87%). See Figures 2–4 and eFigures 2-3 for lifestyle outcome forest plots. Inspection of the funnel plots and Eggar’s test (t = −2.58, P = .02) suggested that sleep outcomes were asymmetrical. This distribution was likely driven by heterogeneity in two studies with high SMD in favor of MBIs (see Supplement).43,77 We were unable to analyze diet due to the lack of consistent outcome measures between studies. No studies tested mental activities as a lifestyle outcome. Forest plot of sleep outcomes generated in the meta R package. MBIs were associated with reductions in sleep disturbance (40/54 RCTs analyzed; 3,537 participants; SMD = −0.53; 95% CI = −0.74 to -0.32; I2 = 78%). Forest plot of physical activity outcomes generated in the meta R package. 70 MBIs were associated with improvements in physical activity (9/17 RCTs analyzed; 685 participants; SMD = 0.72; 95% CI = 0.04 to 1.40; I2 = 89%). Forest plot of tobacco smoking outcomes generated in the meta R package. MBIs were significantly associated with greater odds of tobacco smoking cessation (8/12 RCTs analyzed; 1,234 participants; OR = 2.11; 95% CI = 1.12 to 3.97; I2 = 55%).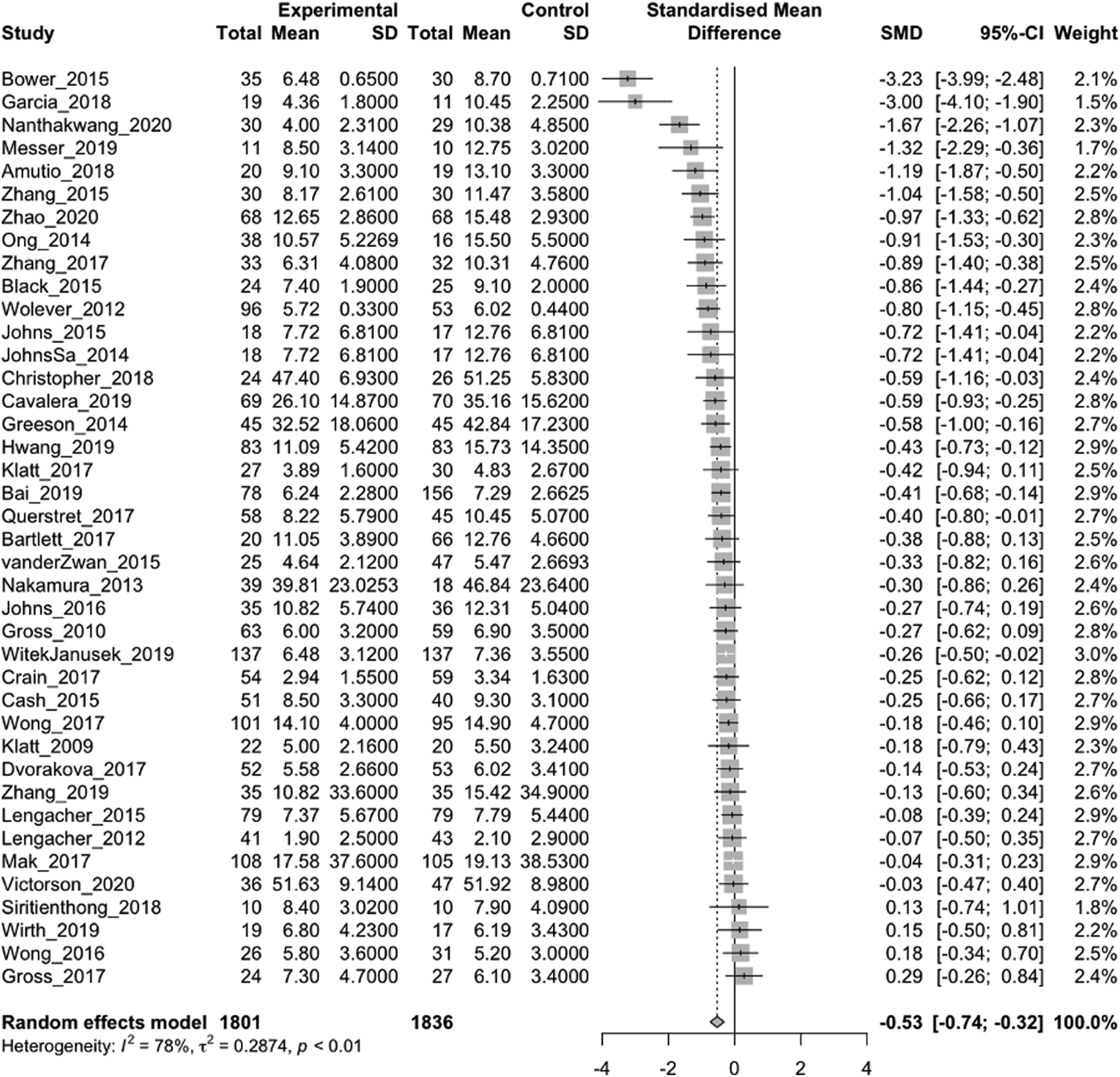
Subgroup Analyses of Lifestyle Outcomes
A-priori subgroup analyses indicated that the effects were greater in RCTs of adapted MBIs (15 RCTs; SMD = −.61; 95% CI = −.95 to −.26) than MBSR (14 RCTs; SMD = −.28; 95% CI = −.45 to −.10) on sleep disturbance; however, MBSR had lower heterogeneity (I 2 = 42% vs 74%). The effects of MBIs on sleep disturbance were greater against waitlist, treatment-as-usual, and empty control arms (25 RCTs; SMD = −.64; 95% CI = −.90 to −.37, I 2 = 79%) and were lower and not significant against active controls (15 RCTs; SMD = −.32; 95% CI = −.65 to .01, I 2 = 69%). Longer MBIs (e.g., 12 vs 5 weeks) were associated with greater improvements in social activity (estimate = .34, 95% CI = .14 to .53, P = .007). The remaining subgroup analyses (patient status, age, sex, control type, risk of bias) were not significant.
Cognitive Outcomes (Exploratory)
Only two articles included cognitive outcomes. In an older adult sample (N = 59), Nanthakwang et al. (2020) found that deep breathing and body scan combined with music was associated with significant improvements on the PTQL Cognitive Domain vs the routine care control (P = .001). In a sample of healthy adults (N = 80), Grensman et al. (2018) found that MBCT was associated with improvements on the Swedish health-related quality of life survey (P < .001) cognitive functioning subscale but was not superior to the CBT control. However, we had insufficient data to include cognitive outcomes in the meta-analysis (see eTable 11).
Discussion
In this systematic review and meta-analysis of RCTs, MBIs were associated with significant post-intervention improvements in sleep quality, physical activity, reduced alcohol use, and tobacco cessation compared to control conditions. The moderate effect size and heterogeneity for these outcomes were generally consistent with similar studies.26,57,58 We found the quality of the evidence to be high for tobacco cessation, moderate for sleep quality and physical activity due to heterogeneity, and moderate for alcohol use due to imprecision (see eTable 12 for GRADE criteria). Our systematic review and meta-analysis adds to the published studies of MBIs for lifestyle medicine26,58 because it is the first to investigate multiple lifestyle outcomes consistent with recent initiatives to understand the biopsychosocial determinants of brain health. The RCT designs, relatively low risk of bias, and large proportion of active control groups were methodological strengths of the included studies.
Mindfulness increases self-awareness, decreases impulsivity, and allows individuals to make intentional lifestyle choices rather than be on automatic pilot. MBIs have been shown to decrease negative patterns of ruminative thoughts, emotional reactivity, and judgmental self-evaluations that contribute to sleep disturbance.78-81 These mindfulness processes may also promote the tolerance of uncomfortable thoughts and sensations that are experienced through exertion (e.g., pain, fatigue), thereby promoting sustained physical activity.82-84 The substance use literature has focused on the potential for MBIs to enhance emotion regulation towards aversive experiences that contribute to alcohol and tobacco cravings and urges.85,86 Future studies are needed to test mindfulness mechanisms that drive lifestyle changes for brain health.
The subgroup analyses provide evidence that study design choices significantly affect outcomes in RCT of MBIs. It is possible that adapting MBIs to specific lifestyle behaviors or populations can increase potency, such as integrating specific behavioral techniques for sleep restriction and hygiene. 87 Importantly, RCT of MBSR for sleep had the lowest heterogeneity, which is likely by design because it follows a highly standardized protocol that emphasizes consistent training and therapist fidelity. 88 Consistent with prior research, 89 the effects of MBIs on sleep disturbance were greater when compared to waitlist, treatment-as-usual, or empty conditions than active controls. We encourage researchers to provide a clear rationale for the control condition that is appropriate for the stage of intervention development. Finally, the effects of MBIs on lifestyle outcomes were independent of participants’ age, sex, and patient status suggesting that MBIs could be broadly implemented to promote brain health. Based on the subgroup results, we encourage future research to explore whether adaptations to MBIs could improve outcomes, and fully report decision choices so that their associations with outcomes can be further studies in future meta-analyses.
Our findings suggest that MBIs have broad applications in clinical contexts. “Brain Health Services” offers a promising model for integrating MBIs into primary and preventative care to promote brain health.90,91 In this model, patients are triaged to brain health interventions after a comprehensive assessment of individual lifestyle profiles. MBIs can be offered in combination with education on brain health and individualized coaching in the form of shared medical visits.92,93 Shared medical visits are cost-effective and sustainable because they are delivered to groups of patients with similar risk factors and can be billed to insurance. To promote scalability, clinical integration could begin with MBSR and MBCT because they are commonly recognized and follow a standardized protocol with high therapist fidelity, demonstrating a model for effective and replicable intervention. Ultimately, MBIs must be adapted to be successfully offered in outpatient clinics or community health centers, targeting diverse populations across the adult lifespan. To be successful, healthcare systems must overcome the documented barriers to implementing brain health care, such as limited time and resources for prevention. 94 Overall, our study positions MBIs as a versatile and effective approach within lifestyle medicine, offering valuable insights for clinicians and healthcare systems seeking to enhance brain health and patient quality of life.
The limitations of included RCTs must be weighed against the findings of our systematic review and meta-analysis. First, visual inspection of the funnel plots and Eggar’s regression test revealed asymmetry in the sleep outcomes. Although publication bias cannot be ruled out, asymmetry was likely driven by two RCTs with small sample sizes that reported large SMD in favor of the MBI. Second, there were several threats to generalizability. RCTs had an overrepresentation of female participants. Data on race, ethnicity, and socioeconomic status could not be extracted and analyzed due to reporting inconsistencies between studies. Additionally, we excluded non-English studies due to a lack of translation resources. Third, incomplete data and reporting inconsistencies between studies limited our ability to draw conclusions about the effects of MBIs on brain health. We were unable to analyze the effects of MBIs on diet, mental activities, and cognitive functioning outcomes due to insufficient data and heterogeneity in outcome measures. Fourth, there was wide variability in authors’ descriptions of MBIs, and some of the included studies may not be universally considered an MBI (e.g., transcendental meditation). Fifth, incomplete outcome data, blinding of participants and personnel, outcome assessors, and allocation concealment were the most common risks of bias and studies often lacked sufficient details to provide definitive ratings. Despite our attempts to impute missing data, several studies were excluded from the meta-analysis because essential outcomes data (sample size, mean, and standard deviation) were not reported (see Supplement). Finally, our intention was to evaluate the emerging evidence of MBIs to modify lifestyle “Pillars of Brain Health,” but acknowledge that these behaviors widely impact other health conditions.
Our study is the first systematic review and meta-analysis to investigate the range of research methods used in RCTs and estimate the effects of MBIs on multiple lifestyle outcomes for brain health. Our findings provide empirical evidence that MBIs, as a feasible and efficacious psychosocial intervention, may offer a broad and robust lifestyle medicine approach for promoting brain health across the adult lifespan. Yet, the heterogeneity in outcomes and insufficient data to analyze diet, mental activities, and cognitive functioning limit our ability to draw definitive conclusions about the effects of MBIs on the broad range of lifestyle behaviors commonly linked to brain health. Future studies should address the methodological limitations documented in our review and test whether MBI-related improvements in lifestyle behaviors can reduce other risk factors for poor brain health (e.g., chronic stress, depression, cardiovascular disease) and promote quality of life in diverse populations.
CME/CE Article Quiz
American College of Lifestyle Medicine (ACLM) members can earn FREE CME/CE credit by reading this approved CME/CE article and successfully completing the online CME/CE activity. Non-members can earn CME/CE for $40 per article. Visit lifestylemedicine.org to join the ACLM.
AJLM CME/CE Articles and Quizzes are offered online only through the American College of Lifestyle Medicine and are accessible at lifestylemedicine.org/store. ACLM Members can enroll in the activity, complete the quiz, and earn this CME/CE for free. Non-members will be charged $40 per article.
A Passing score of 80% or higher is required in order to be awarded the CME/CE credit.
Supplemental Material
Supplemental Material - Mindfulness-Based Interventions Targeting Modifiable Lifestyle Behaviors Associated With Brain Health: A Systematic Review and Meta-Analysis
Supplemental Material for Mindfulness-Based Interventions Targeting Modifiable Lifestyle Behaviors Associated With Brain Health: A Systematic Review and Meta-Analy0073is by Ryan A. Mace, PhD, Matthew J. Stauder, MS, Sarah W. Hopkins, MS, Joshua E. Cohen, Malvina O. Pietrzykowski, MS, Lisa L. Philpotts, BSN, MSLS, Christina M. Luberto, PhD, and Ana-Maria Vranceanu, PhD American Journal of Lifestyle Medicine.
Supplemental Material
Supplemental Material - Mindfulness-Based Interventions Targeting Modifiable Lifestyle Behaviors Associated With Brain Health: A Systematic Review and Meta-Analysis
Supplemental Material for Mindfulness-Based Interventions Targeting Modifiable Lifestyle Behaviors Associated With Brain Health: A Systematic Review and Meta-Analy0073is by Ryan A. Mace, PhD, Matthew J. Stauder, MS, Sarah W. Hopkins, MS, Joshua E. Cohen, Malvina O. Pietrzykowski, MS, Lisa L. Philpotts, BSN, MSLS, Christina M. Luberto, PhD, and Ana-Maria Vranceanu, PhD American Journal of Lifestyle Medicine.
Footnotes
Acknowledgments
The authors thank Sim Uppal, Mira Reichman, Juliana Wagner, Julia Oppenheim, and Anna Yaggi for their contributions to the planning, abstract screening, and data extraction phases of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.