
Abstract
Lifestyle medicine is a patient-engaged field that has grown in tandem with our increasing knowledge of the importance of lifestyle factors and modifiable health behaviors for disease prevention, health promotion, and the management of chronic illness. Stress is at the epicenter of many negative behaviors that contribute to unhealthy lives, such as smoking, overeating, and unhealthy diets, and lack of activity. Mindfulness meditation is a stress reduction practice that teaches awareness, appreciation, and nonjudgmental acceptance of one’s present experience, thereby short-circuiting reactive, automatic stress reactions. Our systematic review and meta-analysis focuses on the application of randomized controlled mindfulness intervention studies across a broad range of populations and conditions that are relevant to lifestyle medicine. In addition to organizing and highlighting mindfulness research studies that are relevant to the field of lifestyle medicine, we also empirically examine the impact of study design issues (eg, use of different controls, intervention length and duration, sample size, primary outcomes) on the magnitude of effect of mindfulness interventions in lifestyle medicine. Overall, this systematic review and meta-analysis found partial evidence for mindfulness-based interventions to provide short-term benefits across a wide range of lifestyle medicine–relevant populations and study outcomes, particularly focusing on the areas of diet and weight management and symptom burden. Numerous outcome measures were used; however, the most common were the Perceived Stress Scale and the State Trait Anxiety Inventory. This analysis also provides evidence for mindfulness-based interventions that have fewer than 20 individuals per group, as well as partial support for interventions that are less than the standard 8 weeks in duration.
Keywords
‘Mindfulness is a multisensory, contemplative meditative tradition that is formally practiced while sitting, lying, eating, walking, or engaging in gentle yogic postures.’
Lifestyle medicine is an approach to medical care that focuses on the adoption and maintenance of positive health behaviors to prevent the development or worsening of disease, promote healthy living and wellness, and optimally manage existing chronic medical conditions and related burden. 1 This field has evolved considerably over the past decade as an adjunct to conventional medical care and often consists of leveraging evidence-based interventions in exercise/physical activity, diet/nutrition, smoking cessation, and stress management to prevent or reduce lifestyle-related health problems such as obesity, 2 cardiovascular disease, 3 hypertension, 4 type 2 diabetes, 5 and other chronic conditions. 6 Lifestyle medicine is a patient-centered practice that relies greatly on the engagement of patients themselves to be active agents of their own health and wellness. 7
Given the pivotal and accumulative role of psychological and physiological stress in the onset, continuation, and outcomes of chronic disease,8-10 one particularly important lifestyle medicine–based intervention is stress management and reduction. An increasingly studied type of stress reduction involves the cultivation of mindfulness, or the practice of paying attention on purpose, in the present moment, without judgment. 11 Mindfulness is a multisensory, contemplative meditative tradition that is formally practiced while sitting, lying, eating, walking, or engaging in gentle yogic postures. It has been operationally defined as a bivariate mode or state of consciousness, involving (a) the self-regulation of sustained attention and attentional shifting, which subsequently fosters the inhibition of secondary elaborative cognitive processing (rumination); and (b) an orientation toward internal and external experiences characterized by openness, curiosity, and acceptance. 12
Over the past 2 decades, a structured intervention called mindfulness-based stress reduction (MBSR) has become one of the most commonly evaluated and empirically supported treatments for helping people reduce stress and manage disease and treatment related sequelae in both healthy and chronic disease samples.13-15 Based primarily on the instruction of mindfulness meditation and gentle yoga, MBSR is a group-based, 8-week program that was developed at the University of Massachusetts Stress Reduction Clinic under the direction of Jon Kabat-Zinn. 11 As a nonreligious practice, MBSR facilitates the cultivation of nonjudgmental, moment-to-moment awareness through a process of attentional single-mindedness (eg, mindfulness). MBSR is composed of a systematic, developmentally sequenced curriculum that uses a group format to experientially instruct participants in the practice of mindfulness meditation and Hatha yoga. Each session includes different forms of meditation practice, such as cultivating awareness of thoughts, feelings, and bodily sensations, and learning to incorporate this awareness during stressful emotional and/or physical life situations. 16
Several other related mindfulness-based interventions have been adapted from MBSR for other patient groups or conditions, including Mindfulness Based Cognitive Therapy (MBCT),17-19 Mindfulness-Based Relapse Prevention (MBRP), 20 Mindfulness-Based Eating Interventions (MB-EAT 21 and MEAL 22 ), and so on. Recent systematic reviews have been conducted on mindfulness-based interventions focusing on substance-use disorders, 23 lower back pain, 24 eating disorders, 25 cancer survivors,26,27 and anxiety disorders. 28 Overall, these reviews suggest that MBSR, MBCT, and their adaptations have demonstrated promising results in the reduction of emotional distress (depression, anxiety) and pain, improvements in sleep, and overall health-related quality of life. 29 Mindfulness-based interventions may also have an important role in reducing the physiological effects of stress on the body and have been associated with reestablishing normal patterns of cortisol secretion, 30 decreases in pro-inflammatory cytokines, and possible beneficial changes in HPA axis functioning in cancer patients. 31 Despite these reviews, little empirical evidence exists on whether modifications to MBSR (eg, implementing it less than 8 weeks, adding additional tailored content to the lessons) or study design differences (eg, having relatively smaller group sizes, using a wait-list control vs an active control) significantly affect primary outcomes of mindfulness randomized controlled trials (RCTs) that are relevant to lifestyle medicine. We were also curious about what study outcomes relevant to lifestyle medicine would see the greatest or most significant change as a result of mindfulness training. The purpose of this study was to (a) systematically review published mindfulness-based RCTs with relevance to lifestyle medicine (eg, those that focused on adopting and/or maintaining mindfulness practices as a means of preventing or managing existing medical conditions and symptoms or promoting health and wellness among the general population) and (b) utilize meta-analytic procedures to determine whether study design characteristics, intervention modifications, and choice of specific outcomes meaningfully affect variability of effect size magnitude across studies.
Methods
We followed guidelines from the Preferred Reported Items for Systematic Reviews and Meta-Analyses (PRISMA) 32 and the Cochrane Collaboration 33 for this study.
Literature Search and Strategy
Our literature search included the following databases and sites over the past 10 years (between 2002 through 2012): PUBMED, OVID/MEDICINE, PROQUEST, PSYCHINFO, MINDFULNET.ORG, and Mindfulness Research Monthly (http://www.mindfulexperience.org/). We adapted the following complete key word search strategy as necessary per database: Lifestyle Medicine, Mindfulness Meditation, Mindfulness Based Stress Reduction, MBSR, Mindfulness Based Cognitive Therapy, MBCT, Mindfulness Based Relapse Prevention, Mindfulness Based Intervention, Mindfulness Based Eating Awareness Training, and Mindful Eating and Living. We also filtered results by the following criteria: published in English, between 2002 and 2012, peer reviewed journal, clinical trial, randomized trials, systematic review, review, meta-analysis, human. All initially retrieved abstracts were read by 2 reviewers (DV and MK). We reviewed all articles in their entirely that contained sufficient information to calculate effect sizes. Once all eligible studies were identified, each article was reviewed in full and abstracted accordingly.
Eligibility Criteria
Interventions
Given our study questions, we included group-based clinical mindfulness intervention studies of at least 2 weeks or longer such as MBSR, MBCT, MB-EAT, and so on, or modified derivatives where similar mindfulness training was the primary focus of the intervention.
Study Type
We only included published RCTs (including wait-list control designs) and excluded observational or nonrandomized studies or published abstracts. We excluded follow-up studies of previously published original trials as well as laboratory-based experiments that did not involve intensive group-based mindfulness training as a means of improving a lifestyle medicine–relevant outcome or goal (eg, emotional regulation, smoking cessation).
Patients Populations and Relevance to Lifestyle Medicine
In view of the broad focus and applicability of lifestyle medicine practices that span disease prevention, health promotion, and chronic disease management, we kept this category broad in our search strategy to allow for as many lifestyle medicine relevant studies as possible where the primary purpose of the mindfulness intervention was to facilitate wellness, improve quality of life, or promote health and well-being. With regard to psychiatric and substance use studies, we limited the types of publications to less severe, community-based populations (vs intensive programs or inpatient facilities) where symptomatology (eg, depressive symptoms, cannabis use) could be widely generalizable to others without psychiatric problems or diagnoses. In the end, we included patient populations highlighted in the American College of Lifestyle Medicine’s Evidence Review, 1 including cancer, cardiovascular disease, metabolic syndrome, musculoskeletal and joint problems, neurological disorders, pain disorders, and psychiatric and respiratory illness.
Data Extraction
We followed published recommendations to establish meta-analytic decision rules34,35 and the PICOS framework (Population, Interventions, Comparators, Outcomes, Study Design) 36 to abstract relevant articles. Our research team (all study authors) engaged in a systematic and iterative data identification, review, and indexing process. Following the initial creation of the study database (MK and DV), article reviewers (all coauthors with individually subdivided reviewing/abstracting assignments) independently coded study characteristics, including the following: study title, authors, and publication year; population under study; clinical issue addressed and primary outcome; study type; characteristics of the intervention (eg, number of weeks, modifications); control group characteristics; sample size; adult or pediatric focus; gender, age, study outcomes, and measures; study quality; and relevance to lifestyle medicine.
Authors CM and DV abstracted means and standard deviations for primary study outcomes from the baseline and immediate follow-up assessments. When standard deviations were not reported but standard errors or confidence intervals of the intervention means were, we obtained standard deviations by multiplying the standard error by the square root of the sample size
We selected each study’s stated primary outcome on which to calculate effect sizes, which could include psychological constructs such as anxiety or stress, as well as other lifestyle medicine–relevant outcomes such as systolic blood pressure, or number of cigarettes smoked per day. Studies that included multiple experimental arms (eg, mindfulness interventions vs usual care vs active control condition) were coded so that each treatment was included as a separate unit of analysis. We used Hedge’s g as a standardized measure of effect size, which is very similar to Cohen’s d; however, it is less prone to positive bias, especially when smaller sample sizes are included. The formula for calculating Hedge’s g is the following:
Effect size estimates can be interpreted in similar ways to correlation coefficients (eg, Cohen’s criteria: small = .20; medium = .50; large = ≥.80). 37
Study Quality and Risk of Bias
We assessed study quality and risk of bias by having at least 2 coders per article provide numeric quality ratings (1 = low quality, 2 = medium quality, 3 = high quality) at 2 separate reviews (based on the Cochrane criteria) followed by a third round of bias risk examination (DV) where Cochrane Risk of Bias criteria were applied to each publication that was ultimately selected. The Cochrane Risk of Bias Assessment tool examines selection bias, performance bias, detection bias, attrition bias, reporting bias, and other bias. 38
Data Summary and Analysis
We used SPSS version 22 and publically available meta-analysis software from Durham University (see http://tinyurl.com/ntu94ns)). Using a random effects model, we pooled and tested effect sizes for homogeneity to determine whether individual study variation estimates are true population parameters. Given that studies varied widely in intervention, population, and outcomes, we also weighted study effect sizes by sample size. 34 Next, we examined effect size variation between study characteristics and intervention conditions. Homogeneity assumptions were tested using Levine’s test. Planned comparisons were conducted using the least squared difference statistic on significant F tests.
Results
Literature Search
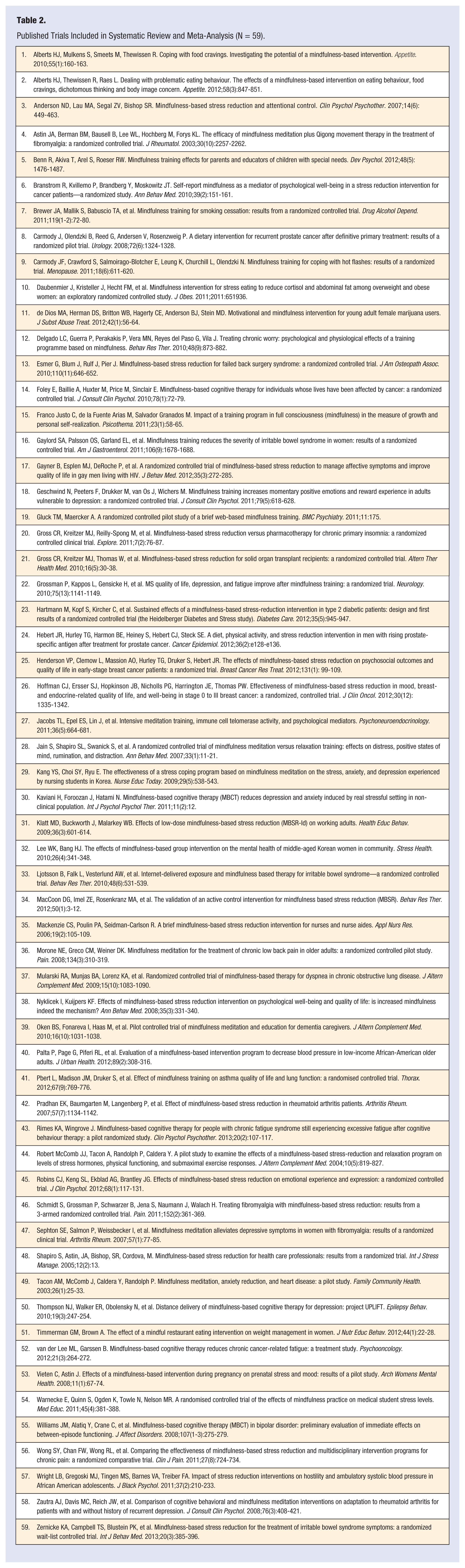
Our initial search yielded 973 articles, which after reexamination and removal of duplicates and nonrelevant papers was reduced to 600 articles for full abstract review and a first round of coding. Following training, each coauthor reviewed and coded roughly 75 articles each, which subsequently led to the reduction of our pool of studies to 184. The primary reason for removal was due to nonrandomized studies. Following another round of discussion and training, each coauthor reviewed and abstracted the remaining articles in full. This lead to a final review, reduction, and reorganization of 59 fully abstracted articles, which were selected for analysis and presentation in this current systematic review.
Study, Setting, and Patient Characteristics
We classified the 59 studies into 13 general categories based on population-specific details. Most categories were also subdivided into specific populations or foci. Cardiovascular relevant studies were the most frequently categorized (n = 10), which included specific areas such as smoking cessation/substance use, weight management, diabetes, blood pressure, and heart disease. See Tables 1 and 2 for included studies and population classifications.
Overview of Included Studies by General Category and Specific Population.
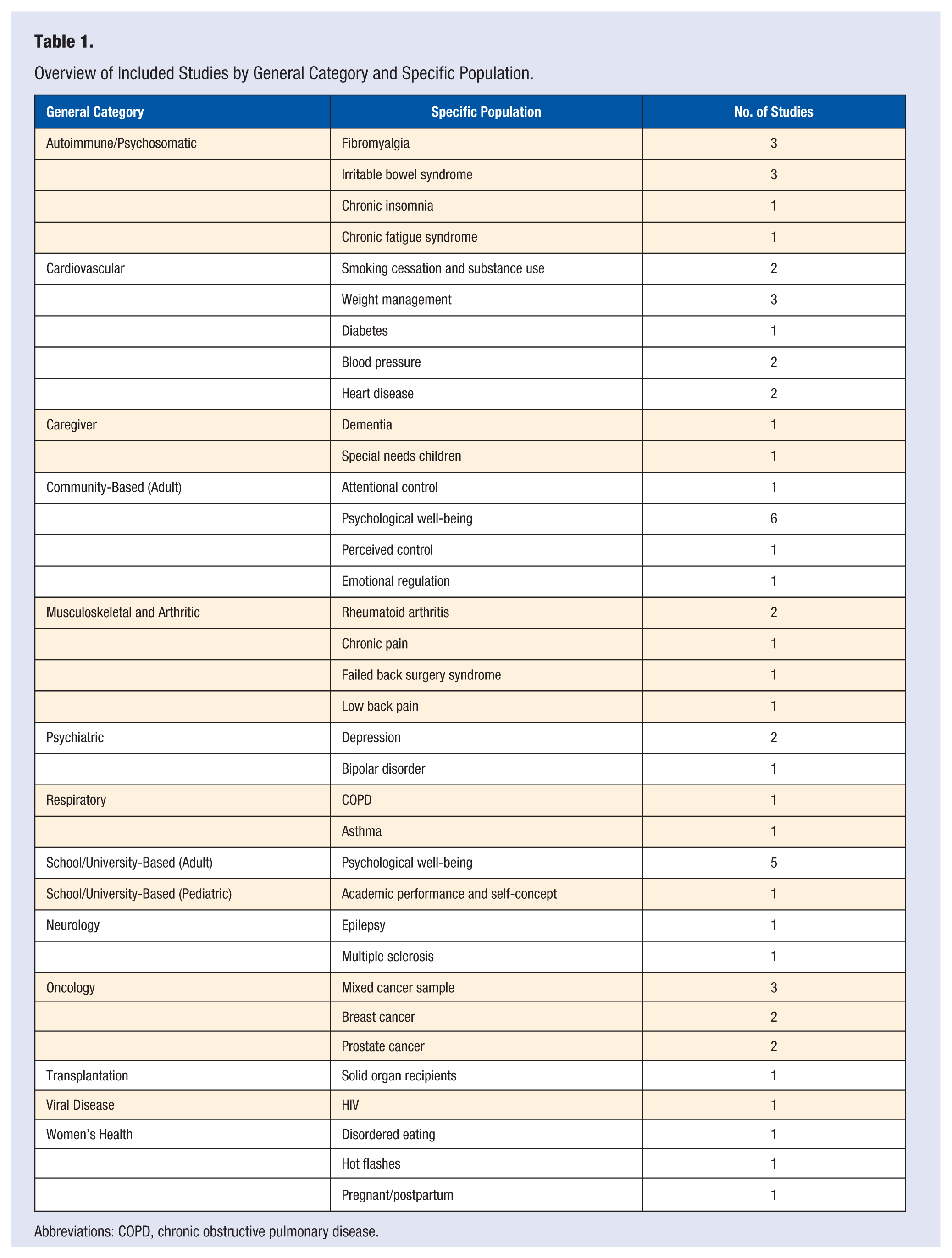
Abbreviations: COPD, chronic obstructive pulmonary disease.
Published Trials Included in Systematic Review and Meta-Analysis (N = 59).
The majority of studies focused on adults (average age = 46.6), and the average total sample size per study was 67.7 (18-229). Females were included in roughly 75% of all studies, whereas males were included in roughly 25%. See Table 3 for full study characteristics.
Study Characteristics.
Abbreviations: MBSR, mindfulness-based stress reduction; MBCT, mindfulness-based cognitive therapy.
Intervention and Control Condition Characteristics
See Tables 3 and 4 for details on intervention and control condition characteristics. The majority of studies reported using the original 8-week MBSR intervention 11 (44.6%) and a wait-list control condition (57%). Among weekly interventions (whether MBSR, MBCT, or an offshoot), the average course length was 7.8 weeks (2-12 weeks), with an 8-week or longer intervention being used in 83.1% of all studies. Outside of adjusting the course length, other components that were added to MBSR included things like qigong, 39 mindful parenting or teaching, 40 diet/exercise,41,42 and mindful mothering, 43 and 2 studies relied on the Internet as a means of delivering the intervention.44,45 Active controls consisted of things such as social support or support groups, 46 pharmacotherapy, 47 smoking cessation education, 48 life skills education, 49 health education, 49 massage, 50 relaxation training, 51 stress and coping psychoeducation, 52 and nutrition education. 53 In 70.8% of the studies, the mindfulness intervention was reported to be superior to controls (eg, significantly different in the hypothesized direction). In 22% of studies, both mindfulness and control conditions reported significant improvements, and in 8% of studies, neither mindfulness nor control reported significant changes in the primary outcomes.
Characteristics of Included Studies.
Abbreviations: MBSR, mindfulness-based stress reduction; MBCT, mindfulness-based cognitive therapy; MB-EAT, mindfulness-based eating awareness training; IBS, irritable bowel syndrome; COPD, chronic obstructive pulmonary disease.
Risk of Bias
See Figure 1 for risk of bias assessment for each study. In all studies, risk of selection bias (based on allocation to the intervention), selective bias, or incomplete outcomes data was generally low. All included studies reported utilizing a random component in the sequence generation process. While a small number of studies reported allocation concealment and blinding of participants, personnel, and outcomes, it was not clear in the majority of studies whether these measures were taken. Using the Cochrane tool’s criteria, an unclear rating is suggested when insufficient information does not permit judgment of low risk or high risk. Considering that the majority of studies utilized a wait-list control group where blinding participants is not feasible, the majority of studies likely fall within the high-risk category; however, insufficient information is available.
Risk of Bias Assessment
Outcome Measures and Domains
A variety of different outcome measures were used in the included studies; however, the most common were measures to assess self-reported anxiety (33.8%) and perceived stress (20%) (see Tables 4 and 5).
Study Measurement Tools and Domains Assessed.
Effect Size Variability Across Studies and Study Characteristics
See Table 6 for the average effect size variation across study characteristics and Figure 2 for effect sizes and 95% confidence intervals by primary outcome and population. Within the different mindfulness interventions delivered, we first examined the total effect of allocation to study condition (mindfulness, wait-list/usual care, or active control) on effect size variability in primary outcomes. Overall, mindfulness interventions were significantly different to all other conditions (P < .01) with a large pooled effect size compared to weak effects for waitlist and usual care groups (.1 and .2, respectively) and moderate effects for active control conditions (.5). The active control condition effect size was also significantly stronger compared to the waitlist/usual care. The assumption that all effect sizes were estimating the same population mean (eg, homogeneity) was not met however, indicating heterogeneity of variance within these studies.
Average Effect Size Variation Across Study Characteristics a .
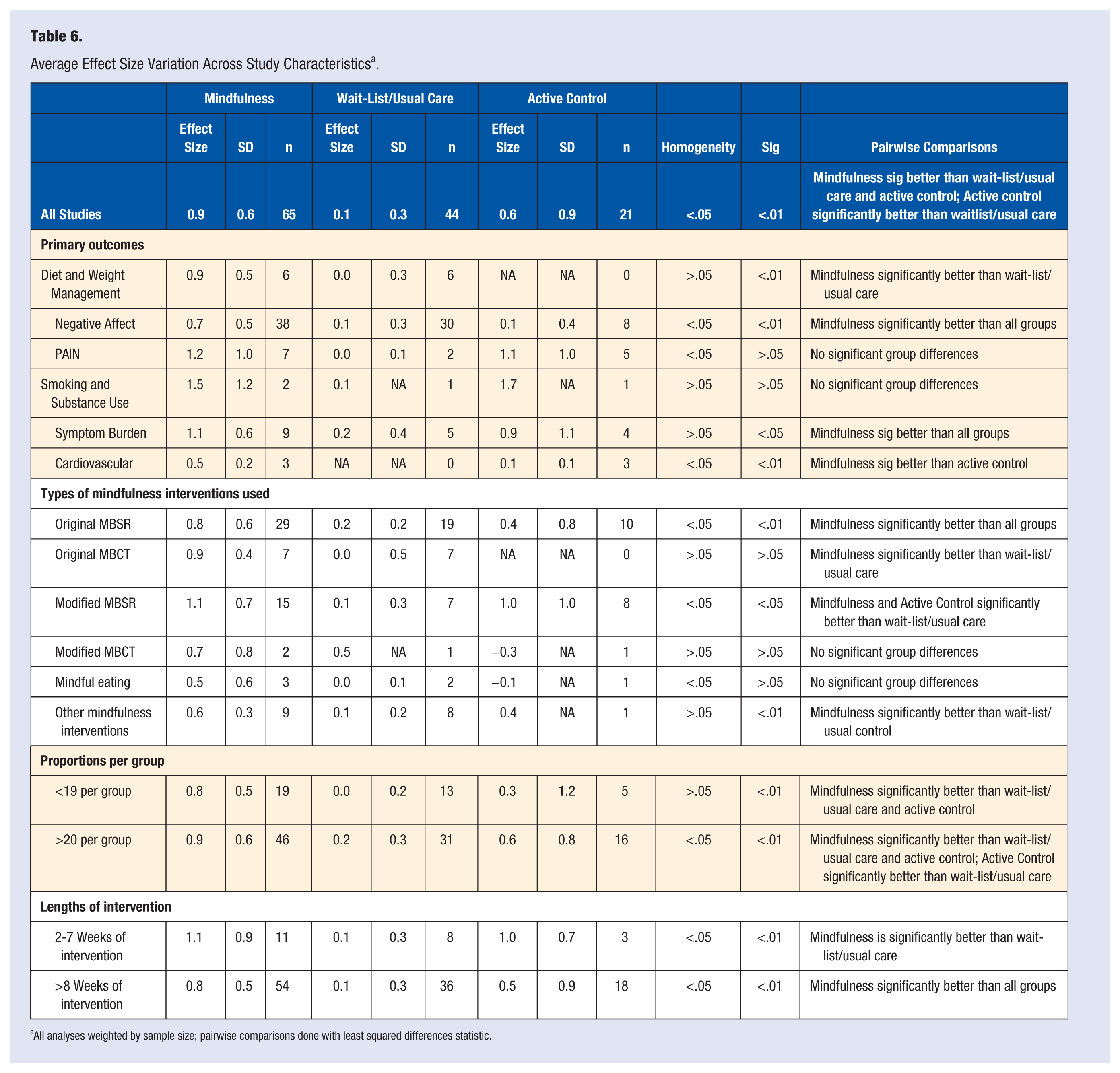
All analyses weighted by sample size; pairwise comparisons done with least squared differences statistic.
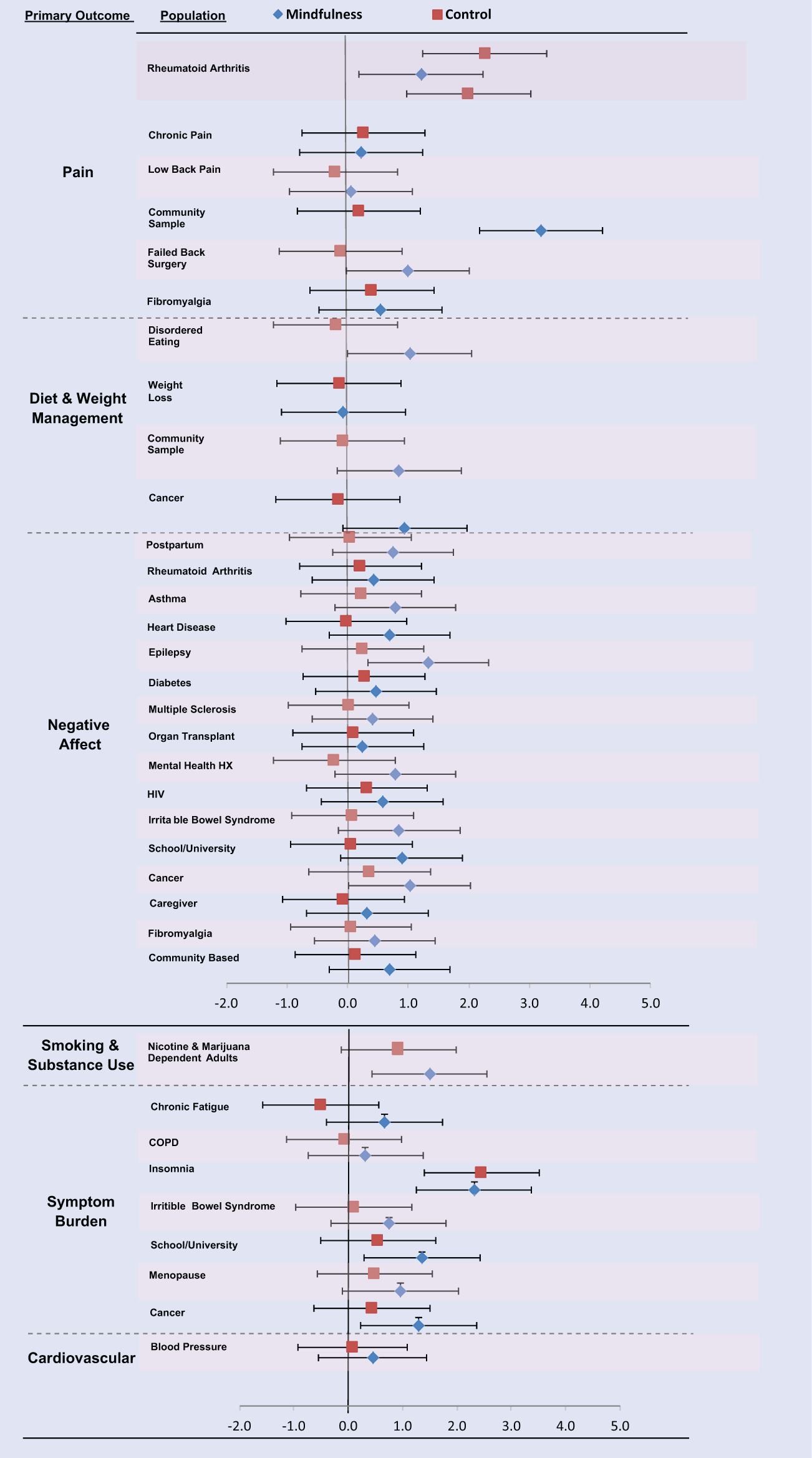
Effect Sizes and 95% Confidence Intervals by Primary Outcome and Population.
Next, we examined whether effect sizes differed by type of primary outcome. To organized this varied literature, we first grouped study outcomes into the following 6 thematic categories: Diet and Weight Management (body image concern, emotional food cravings, emotional eating, saturated fat intake, and weight loss); Negative Affect (anxiety, perceived stress, hostility, tension, neuroticism, emotional exhaustion, and worry); Pain (general pain, fibromyalgia pain, and low back pain); Smoking and Substance Use (number of tobacco cigarettes smoked and number of marijuana cigarettes smoked); Symptom Burden (hot flash bother, irritable bowel syndrome symptoms, insomnia, global symptom severity, dyspnea, and fatigue); and Cardiovascular (systolic blood pressure). The homogeneity assumption was met for 3 categories (Diet and Weight Management; Smoking and Substance Use; and Symptom Burden), of which 2 demonstrated statistically significant differences. Diet and Weight Management (P < .01) and Symptom Burden (P < .05) effect sizes were each significantly more robust for mindfulness (.9 and 1.1, respectively) compared with all other groups (see Figure 3).
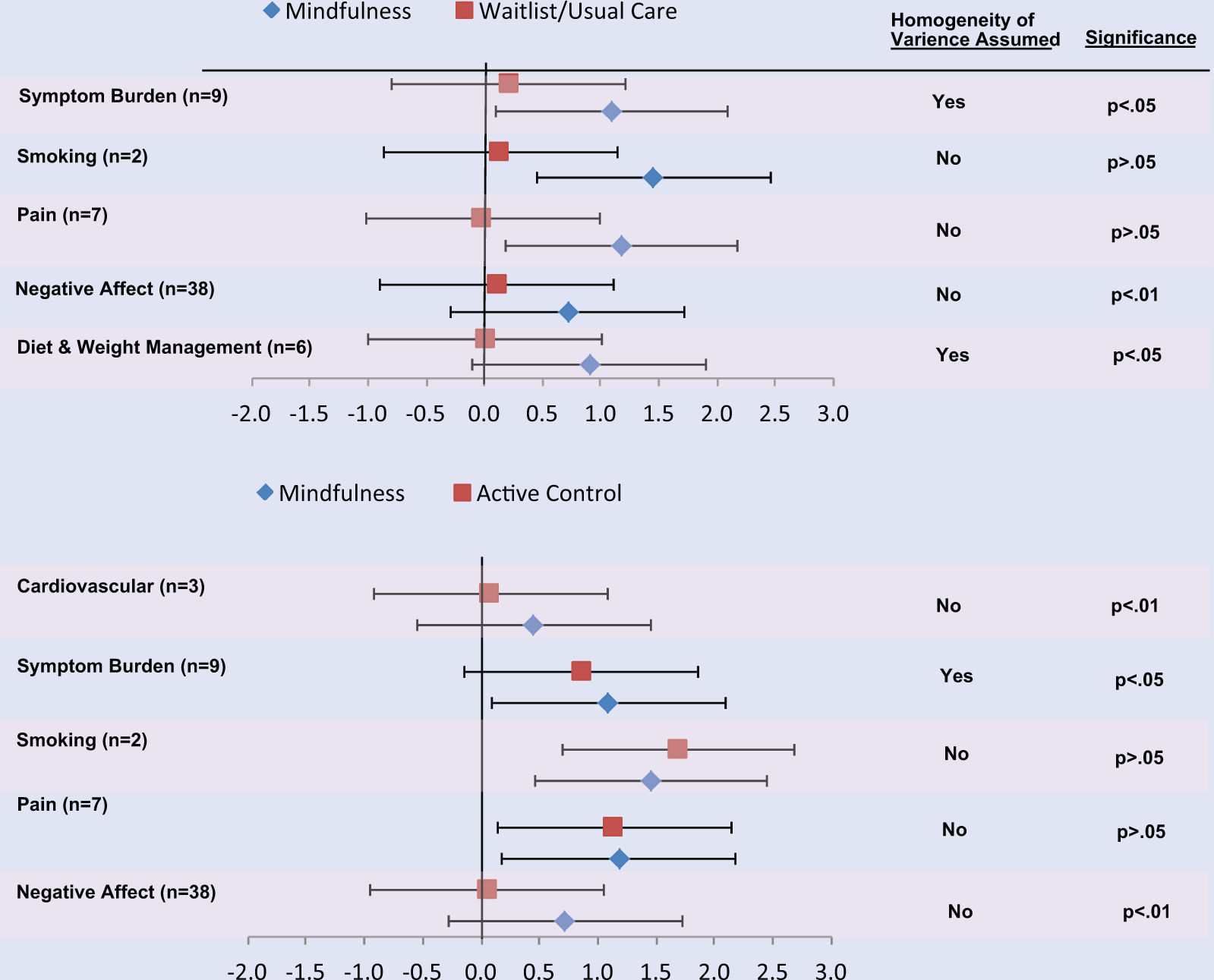
Effect Size Differences Between Condition and Primary Outcome.
When comparing different types of mindfulness interventions delivered, the original MBSR group effect size (g = .8) was significantly larger compared to wait-list/usual care (g = .2) and active control (g = .4); however, homogeneity of variance assumptions were not met. Of all types of mindfulness interventions delivered, the only group where the homogeneity assumption was met and demonstrated a significant difference was in “other mindfulness interventions” where mindfulness had significantly larger effect sizes (g = .6) compared with the wait-list/usual care condition (g = .1). This “other” category was made up of studies focusing on diet and weight management (22%), negative affect (67%), and smoking and substance use (11%) (see Figure 4).
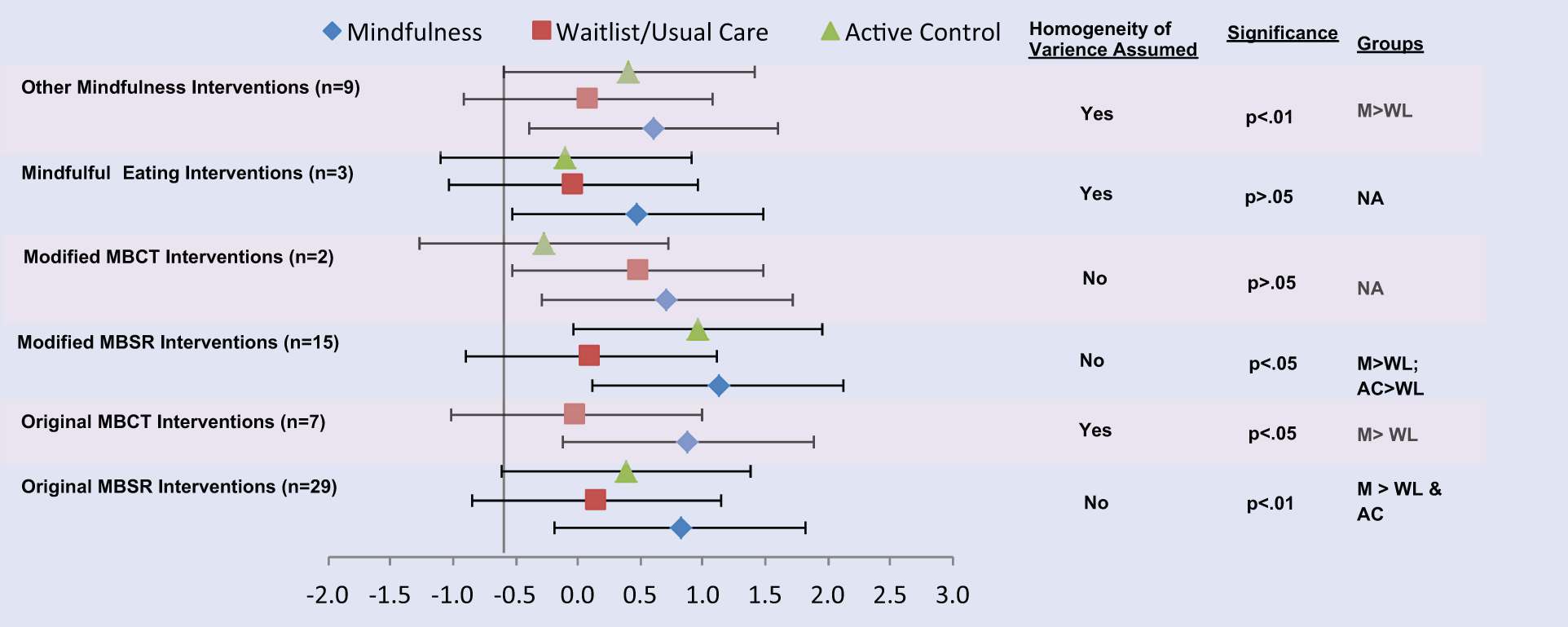
Effect Size Differences Between Condition and Type of Mindfulness Intervention.
Next, we compared effect size differences between studies with 19 or less participants in a group with those that had 20 or more per group. In both the “19 or less” and “20 or more” groups, the mindfulness condition had significantly larger effect sizes (P < .01) compared with the wait-list/usual care and active control groups; however, the homogeneity assumption was only met in the “19 or less” group (g = .8). In addition, the active control also had significantly higher effect sizes (P < .01; g = .6) compared to the wait-list/usual care group in the “20 or more” group; however, the homogeneity assumption was not met (see Figure 5).
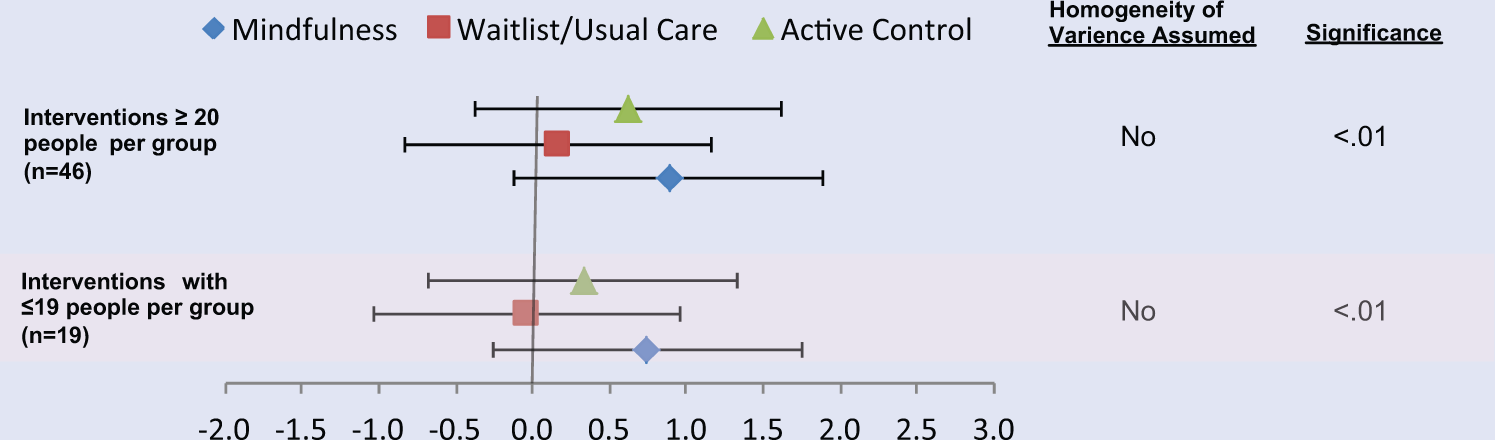
Effect Size Differences Between Condition and Group Size.
Finally, we compared the possible effect size differences when the number of weeks of the mindfulness intervention was relatively less (eg, between 2 and 7 weeks) or more (eg, 8 weeks or more). The mindfulness condition had significantly larger effect sizes than the wait-list/usual care groups (P < .01; g = 1.1) in both intervention periods and was also significantly larger than the active control conditions in the “8 weeks or more” (P < .01; g = .8). The homogeneity assumption was not met for either the “2 to 7 week” or “8 weeks or more” comparisons (see Figure 6).
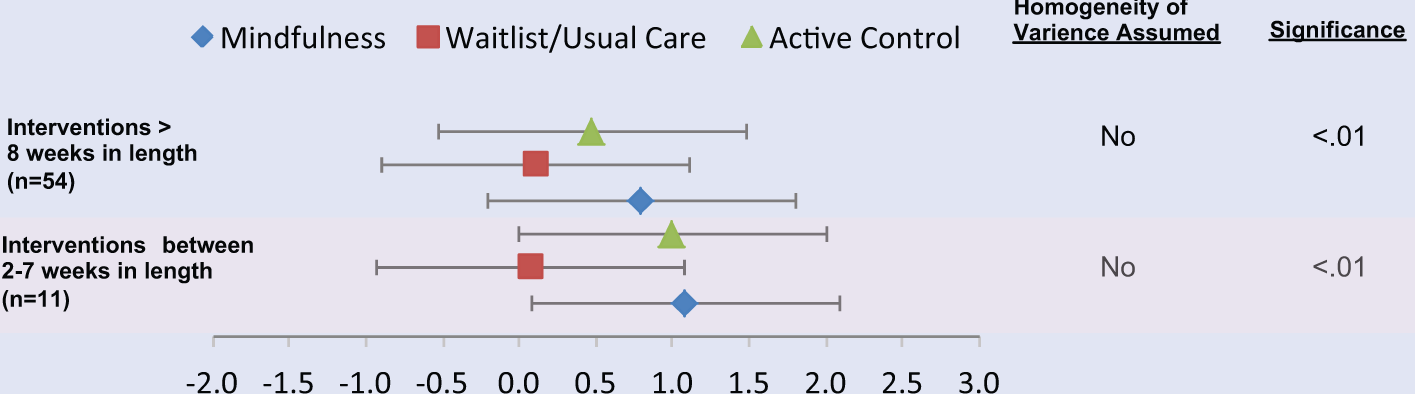
Effect Size Differences Between Condition and Weeks.
Discussion
Overall, this systematic review and meta-analysis found partial evidence for mindfulness-based interventions to provide short-term benefits across a wide range of lifestyle medicine–relevant populations and study outcomes, particularly focusing on the areas of diet and weight management and symptom burden. Mindfulness-based interventions are inherently lifestyle medicine interventions that have the potential to address a wide range of issues, from disease prevention and health promotion to chronic disease management.
Wait-list conditions were the predominant control group in the included studies, and our meta-analytic findings suggest that mindfulness interventions are superior to no treatment at all, or simply the passage of time. Being placed on a wait-list may be demoralizing for the person who does not want to wait (possibly influencing their outcome scores negatively), or create a positive expectancy effect knowing that their turn is coming (possibly influencing their outcome scores positively). Using wait-list controls is understandable in behavioral medicine research, especially in the early, pilot testing of an intervention where the primary aim is feasibility, acceptability, and safety. However, given the apparent viability and tolerability of mindfulness interventions, as evidenced by their widespread application across numerous different populations and conditions, continued efforts should be made to develop, test, and use good active control conditions (eg, MacCoon et al.’s 54 Health Enhancement Training) to mirror the social-emotional and educational components of MBSR and similar courses. While these multiweek mindfulness courses are not intended to be “support groups,” they are undoubtedly “supportive” to many, and therefore a formidable placebo condition would allow the unique effects of mindfulness training to be more exquisitely examined.
While relatively small sample sizes can be observed across many of the included studies, our empirical findings suggest that this has not affected the power to detect statistically significant findings or risk type II errors, nor has it contributed to comparably smaller effect sizes. Similarly, modifying MBSR in different ways to the original 8-week course continued to produce large effect sizes across studies.
Compared to other medical social science disciplines, the use of eHealth as a tool for the delivery of mindfulness interventions was comparatively small in our review. Provided current trends in the use of technology-based self-management interventions,55,56 this delivery method will undeniably increase over time. Instead of applying a one-size-fits all design/development/delivery approach from other fields such as behavioral or preventive medicine, mindfulness researchers will benefit from exploring novel informatics applications that parallel the specific intricacies and mechanisms of the mindfulness construct itself, so that intervention and method of delivery go hand in hand.
We also observed that the vast majority of studies conducted with US patient samples were with English-speaking, Caucasian, female participants. Mindfulness interventions have tremendous potential to affect real change in health disparities that involve modifiable, lifestyle medicine-relevant outcomes. Continued efforts should be made to further develop, refine, culturally tailor, validate, and empirically examine the effects of mindfulness interventions with non-English-speaking patient groups to address these issues.
This study is not without limitations. First, publication bias was not examined across included studies. Second, as can be seen in Figure 1, many studies failed to report important risk of bias criteria, specifically allocation of concealment, blinding of participants, and blinding of outcomes. While these are important factors for mindfulness researchers to include, it is also understandable that given the unique qualities of a mindfulness intervention, concepts such as blinding do not necessarily apply when the control group is a wait-list, which several of these studies utilized. Future mindfulness RCTs that utilize active or matched controls will add rigor to the body of empirical evidence on these interventions by continuing to abide by and improve on design and reporting standards. A third limitation is that for several of the analytic comparisons, the homogeneity of variance assumption was not met, which indicates that more variation may have been present in the comparison of combined effects than from mere chance alone. For this reason, we used a random effects approach; however, caution should be taken when interpreting results from significant comparisons where the assumption was not met.
Conclusion
This systematic review and meta-analysis found partial evidence of the short-term effectiveness of largely wait-list-controlled mindfulness-based interventions applied to a variety of lifestyle medicine–relevant contexts. Examples including the benefits of mindfulness interventions in managing symptom burden and affecting important modifiable health behaviors such as smoking and eating practices. This analysis also provides evidence for mindfulness-based interventions that have fewer than 20 individuals per group, as well as partial support for interventions that are less than the standard 8 weeks in duration.
Based on our findings and the overall characteristics of these studies, recommendations for future mindfulness intervention trials include the following: (a) utilizing reliable, active control conditions when appropriate; (b) providing greater transparently of Cochrane risk of bias criteria as it allows; (c) actively shaping how intervention delivery will be the most effective for mindfulness trials, whether in face-to-face or eHealth modes, and (d) increasing enrollment and participation of non-White/English speaking samples, and (e) working to make mindfulness interventions more accessible and culturally relevant for ethnically diverse and non-English speaking samples of individuals affected by lifestyle-perpetuated health disparities.