
Abstract
“The results demonstrated that there were significant differences between males and females in their perceptions of quality of nursing care.”
Introduction
Globally, healthcare and nursing practices have undergone an ongoing transformation driven by the best available resources to enhance nursing and organizational outcomes; this ultimately improves the quality of care. The role of the healthcare system is to distribute high-quality healthcare services.1,2 Quality of care (QOC) is one of the most frequently cited in healthcare leadership and management literature because it is vital to high-performing healthcare organizations. However, as perceived by registered nurses, the QOC is the level of care provided by healthcare professionals to the population to increase the possibility of preferred health outcomes.3,4 Quality of nursing care is a crucial factor in healthcare service research and healthcare leaders’ worldwide 5 ; recognize improvements in the quality of services is a major concern. However, concerning competition between healthcare institutions, it is necessary to provide high-quality medical and nursing services to patients.6,7 The concept of quality improvement in healthcare consists of the assurance of a continuum of care over time in every aspect of healthcare prevention.8,9
There have been claims that organizational commitment10,11 and leadership behavior,1,12 were important concepts in understanding the quality of nursing care. Unfortunately, no empirical research has explored how these factors affect the quality of nursing care.
Organizational commitment is a widely studied concept of human and resource management. Organizational commitment denotes the degree of an individual’s connection to the organization’s goals, principles, rules, and norms.13,14 Meyer and Allen 15 introduced a framework encompassing 3 types of organizational commitment: affective, continuance, and normative. Affective commitment pertains to an employee’s emotional attachment; normative commitment involves feelings of responsibility towards the organization; and continuance commitment is linked to the perceived costs associated with leaving the organization. 16 A heightened level of employee organizational commitment has several implications for healthcare organizations, including the assurance of high-quality care. 17 However, poor organizational commitment increases the risk of patient safety.18,19
In healthcare organizations, leadership plays a significant role in improving the quality of nursing care. Several studies have recognized leadership behavior as a key element in the quality of nursing healthcare.20,21 Leadership is defined as “a process whereby an individual influences a group of individuals to achieve a common goal.” 22
The importance of leadership is apparent in healthcare organizations. 23 Transformational theory is the leadership theory most frequently applied in healthcare institutions is transformational theory. 22 In addition, Sfantou et al. 21 study emphasized the importance of leadership behavior in the quality of nursing care. Prior studies conducted in Jordan have not evaluated the impact of organizational commitment and leadership behavior on nurses’ perceptions of QoC. Therefore, this study aimed to investigate the impact of organizational commitment and leadership behavior on the quality of nursing care perceived by registered nurses in acute healthcare environments. The author aims to determine whether nurses with elevated levels of organizational commitment and leadership behavior perceive a higher quality of nursing care; thus, this study fills the knowledge gap in the quality of nursing care, organizational commitment, and leadership behavior in healthcare organizations and substantiates the formulation of contextually relevant decisions. Additionally, it assists leaders, managers, and policymakers in gaining a deeper understanding of fundamental issues and devising strategies that enhance the quality of nursing care and foster healthcare providers’ commitment to their organizations.
The results of the current study contribute to the body of literature by enhancing our understanding of the quality of care in the relationship between a leadership behavior, organizational commitment, and demographic variables. The findings from the current study can be applied in nursing practice, research, and education. This study is significant for future research as it aims to improve perceived nurses’ perception for quality of nursing care across healthcare institutions. This will help fill the gaps in existing nursing literature and offers a new perspective on improving nurses’ perception of quality of nursing care. In addition, this study offers valuable insights for nursing leaders, providing recommendations for developing effective strategies to improve quality of nursing care and to support its successful implementation.
This study investigates how leadership conduct and organizational commitment affect the quality of care as viewed by registered nurses. This approach seeks to direct the examination of these links by including theoretical viewpoints and filling up current research gaps. The hypothesized paradigm offers an organized method for examining the intricate connections among leadership conduct, organizational commitment, and the perceived quality of nursing care. It seeks to advance knowledge of how to promote high-quality care through organizational and leadership interventions by filling important research gaps. The model consists of organizational commitment (1) What is the relationship between the concepts (organizational commitment and leadership behavior) and nurses’ perceived quality of nursing care? (2) What are the relationships between various demographics (gender, employee age, marital status, length of time with employer, and yearly household income) and each of the study variables (perceived quality of nursing care, organizational commitment, and leadership behavior)? (3) What are the predictors of registered nurses’ perceived quality of nursing care among the study variables: demographics, organizational commitment, and leadership behavior?
Materials and Methods
Study Design
A cross-sectional correlational survey design was employed, utilizing self-reported questionnaires to collect data from registered nurses on duty between September and October 2023. This design was selected because of its ability to gather data from a substantial number of participants. The questionnaires were used to mitigate the impact of the researcher on the participants, providing them with greater freedom to respond to questions candidly and openly, as suggested by Polit and Beck. 24
Setting
According to Annual Statistical Report 25 of the Jordanian Ministry of Health, the total number of registered nurses (RNs) was 22,540. However, the Jordanian healthcare system is comprised of governmental, military, university, and private institutions. The Ministry of Health oversees 30 hospitals encompassing 3953 nurses. Two teaching hospitals, Jordan University Hospital with 534 nurses and King Abdullah Hospital with 411 nurses, were included. Military hospitals accounted for 2619 nurses, while private hospitals employed 10,008 nurses. The selection criteria for the hospitals included those equipped with medical, surgical, emergency, and critical care units. Moreover, this study specifically incorporated hospitals located in Amman, which represent the Ministry of Health, private establishments, and university-affiliated hospitals.
Population
The target population for the current research study were all registered nurses responsible for overseeing the delivery of patient care in their assigned unit/floor and those who work at Jordanian hospitals. The accessible population for the current study were registered nurses who work in the selected hospitals. The inclusion criteria were working full-time, having a minimum of one year of experience in the respective field, and holding a bachelor’s degree as the minimum educational qualification. The exclusion criteria for participants included registered nurses who would not directly provide care for the patients, such as nurse managers and directors of nurses.
Sample Size
Linear Multiple Regression: fixed model, R2 deviation from zero was conducted using G*power 3.1 26 to identify the required sample size with a two-tailed test and small effect size r = 0.10, statistical power of 0.95, and significance level of 0.05. The desired sample size was 254. Ten percent was added to cover the non-respondents; therefore, the total sample size was 280 participants.
Sample and Sampling
The sampling aims to select the most suitable participants to enable the focus of the study to be researched. The participants recruited for this study were nurses working in the departments of the selected hospitals. An important consideration is the type of sampling, as this can ensure a more rigorous sample, resulting in a more representative sample that enables researchers to generalize the findings. In this study, a multistage sampling technique was employed. In the first stage, we employed a simple random technique to select hospitals from 2 healthcare sectors in Amman, Jordan. The selected hospitals included a private hospital, a government hospital, and a teaching hospital. In the second stage, nurses were recruited from different departments in a systematic sampling technique (medical, surgical, critical care, emergency, obstetrics, and pediatrics) of each hospital. Systematic sampling technique was used to select nurses from different hospital departments. Systematic sampling is a probability sampling method in which sample members from a larger population are selected according to a random starting point but with a fixed, periodic interval and is one of the most popular sampling methods utilized in research. The authors systematically ask every 10th number on the nurses’ list for participation in the study. However, there is a hidden pattern in the population, for example, nurses work 3 shifts per days, the authors made sure to visit nurses on 3 shifts for data collection.
The head nurses in the hospitals were contacted. Copies of ethical approval, instrument, and summary of the study were given to head nurses, seeking for approval of data collection. The researchers contacted the nurses to participate in the study voluntarily who met the inclusion criteria, describing the purpose of the study, method of data collection, and the time required to answer the questionnaire. Participants who agreed to participate were asked by the researcher in nursing station to fill out the questionnaires.
Ethical Consideration
Prior to commencing data collection and gaining access to registered nurses, approval was obtained. The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Jordanian Ministry of Health. Requested letter on (5/7/2023) number (6737) with Code number 11962 issued on (6/8/2023) and the University of Jordan Ethics Committee Approval Code number (223000296), Approval Date (30/6/2023). Participation in the study was voluntary and the researcher ensured the anonymity of the participants by refraining from recording any personal identification. A cover letter attached to the questionnaire provided detailed information regarding the objectives of the study. Nurses who agreed to participate implicitly provided consent by returning the completed questionnaire, indicating their willingness to participate in the study.
Data Collection
Data were collected in September and October 2023 using a questionnaire consisting of 4 parts: (1) background questionnaire, (2) nurses’ perceived quality of care, (3) nurses’ organizational commitment questionnaire, and (4) leadership behavior. The instrument was pre-tested with a group of registered nurses from a single hospital to ensure its content validity and language clarity in the English version. The researcher explained the study objectives and procedures to nurse administrators and department heads at the participating hospitals. Upon obtaining permission, the researcher invited participants to a lecture room in each department, distributed questionnaires, instructed them to complete the questionnaires, and returned them once they finished.
Instrumentation–Measurements of Variables
This study used the Jordanian-Registered Nurses’ Perceived Quality of Care Instrument, which is a modified 71-item survey. The statements were carefully tested to align with the intended construct, avoiding obvious similarities with other items covering the same construct. All statements, except for leadership behavior, were closed using a seven-point Likert scale. The Likert scale was chosen for its explicit understandability by the respondents and ability to effectively discriminate between their perceptions and degrees of agreement or disagreement. The Likert-scale format is straightforward and flexible. Notably, some measures were negatively worded, whereas others were positively worded to minimize agreement bias. The dependent variable was perceived quality of nursing care, with leadership behavior and organizational commitment as independent variables. Intervention demographic variables included sex, age, marital status, educational level, monthly income, and length of time with an organization. The researcher adapted 3 existing scales for this study: quality of care, leadership behavior, and organizational commitment. Six demographic questions were included in this study.
The Korean English version of the SERVQUAL instrument, consisting of 20 items, was used to measure nursing care service quality. The SERVQUAL instrument was developed by Parasuraman et al.27,28 in English and adopted questions without modification by the researchers. The English version of the SERVQUAL instrument includes 5 dimensions with 4 items each. The instrument is designed to measure service quality by capturing respondents’ expectations along 5 dimensions of service quality: tangibility, which is directed to the physical environment; and Reliability, Responsiveness, Empathy and Assurance, which are assumed to measure the human aspect of service delivery. The scoring system used a seven-point Likert scale ranging from 1 strongly disagree to 7 strongly agree. Abuosi and Atinga 29 reported Cronbach’s alpha coefficients for the 5 dimensions as follows: 0.80, 0.84, 0.83, 0.83 for responsiveness, assurance, and 0.84 for empathy. Moreover, the current study reported that Cronbach’s alpha coefficients for the 5 dimensions of tangibles, reliability, responsiveness, assurance, and empathy were 0.80, 0.85, 0.83, 0.86, and 0.88, respectively.
The independent variable, organizational commitment, was measured using the Organizational Commitment Questionnaire (OCQ) by Mowday et al. 30 It is a 23-item instrument that assesses affective, continuance, and normative commitment with an estimated Cronbach’s α of 0.70. 31 In this study, the instrument demonstrated Cronbach’s alpha coefficient of 0.82. Perceptions of leadership behavior were assessed using 21 descriptive elements from the Multifactor Leadership Questionnaire (MLQ) Form 6S by Bass and Avolio. 32 The MLQ covers 4 factors of transformational leadership: idealized influence behaviors, inspirational motivation, intellectual stimulation, and individualized consideration. Two factors of transactional leadership, contingent rewards and active and passive management-by-exception, and the final factor, indicate a lack of leadership (or laissez-faire leadership). Respondents rated their current immediate supervisor’s behavioral frequency on a five-point scale. The items were rated on a 1-5 rating Likert scale. The scale points were 1 = not at all, 2 = once in a while, 3 = sometimes, 4 = fairly often, and 5 = frequently if not always. Every subscale-factor consists of 3 items. The internal consistency for leadership behavior in the current study ranged from 0.90 for transformational leadership, 0.86 for transactional leadership, and 0.83 for laissez-faire.
Data Analysis, Screening, and Cleaning
Data were analyzed using the Statistical Package for Social Science (SPSS)-version 26. Descriptive statistics (means, percentages, and standard deviations) were used to describe the demographics of the study sample. Other statistical tests, such as the forward stepwise multiple linear regression test, were used for data analysis. It examines whether the independent variables (demographics, organizational commitment, and leadership behaviors) under study explain a statistically significant amount of variance in the Dependent Variable, after accounting for all other variables. Pearson’s correlation test was used to test the correlations between study variables. 24
The data were screened and cleaned by running frequencies on every variable and carefully examining the frequencies for invalid values, unusual values, large amounts of missing data, and adequate variability. When dealing with missing data, the researcher examined both the quantity and pattern, distinguishing between random and systematic. For the demographic data questionnaire, if a participant had less than 10% of the research instrument left unanswered, missing data were substituted with the group’s mean score for that particular item. To assess the quality of the data, the study variable scores for normality, extreme skewness, and kurtosis were examined using frequency tables, histograms, and scatterplots. It is worth noting that the variables are measured at the continuous (interval and ratio) level.
Results
Demographic Characteristics
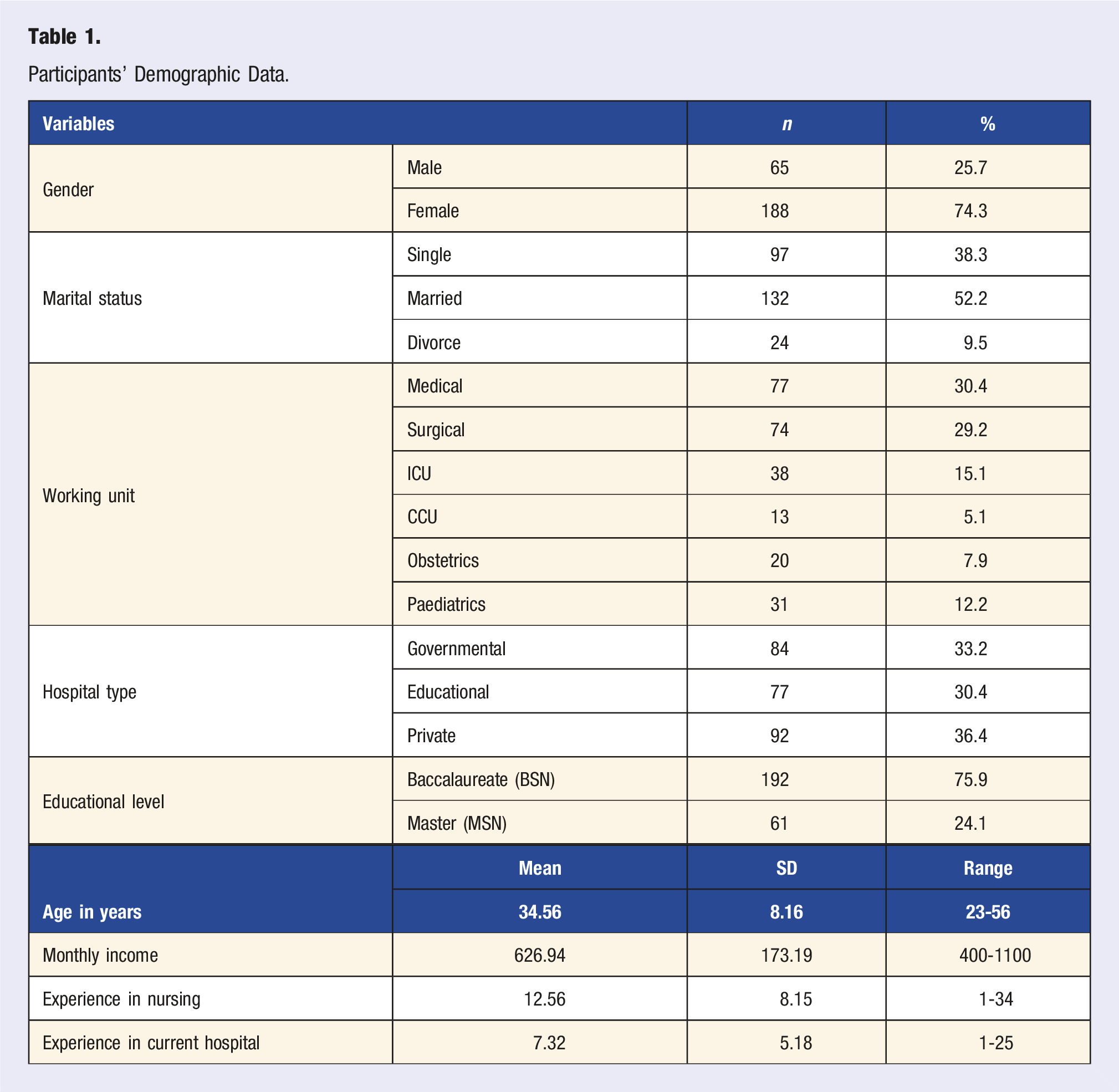
Participants’ Demographic Data.
Nurses’ Perceptions of Quality of Nursing Care
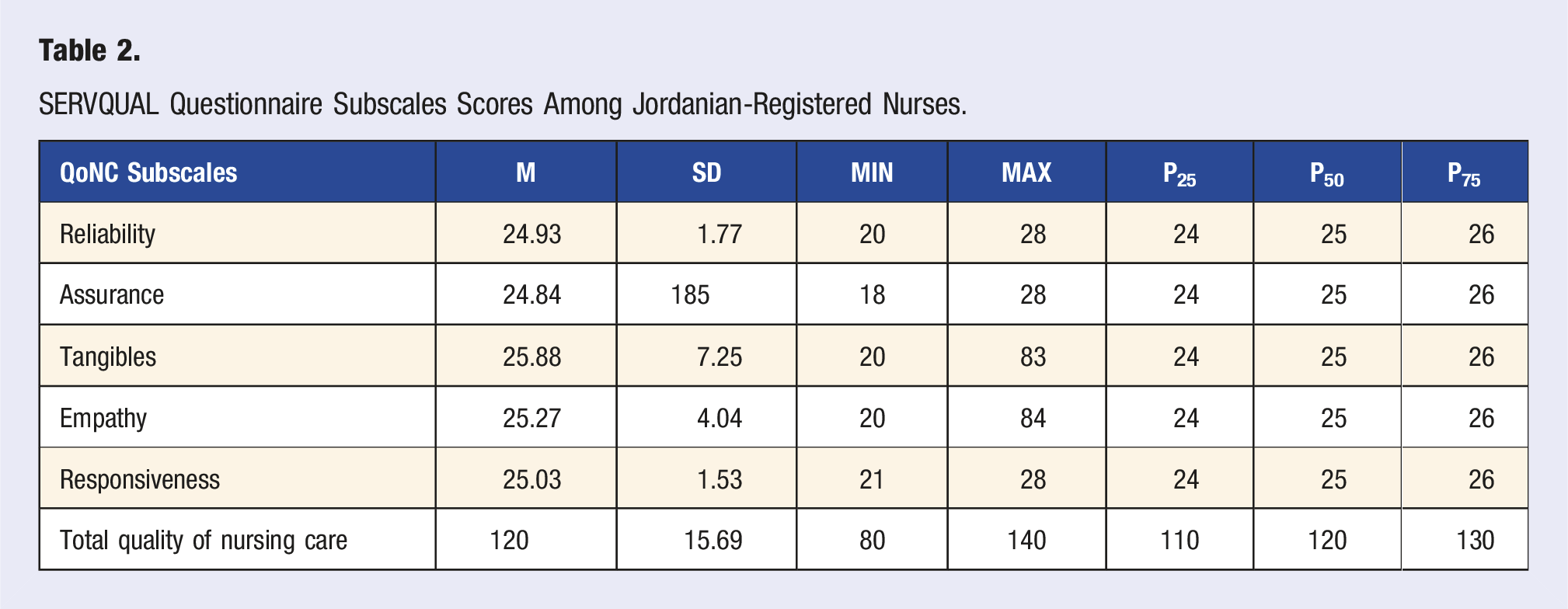
SERVQUAL Questionnaire Subscales Scores Among Jordanian-Registered Nurses.
Leadership Behavior and Organizational Commitment
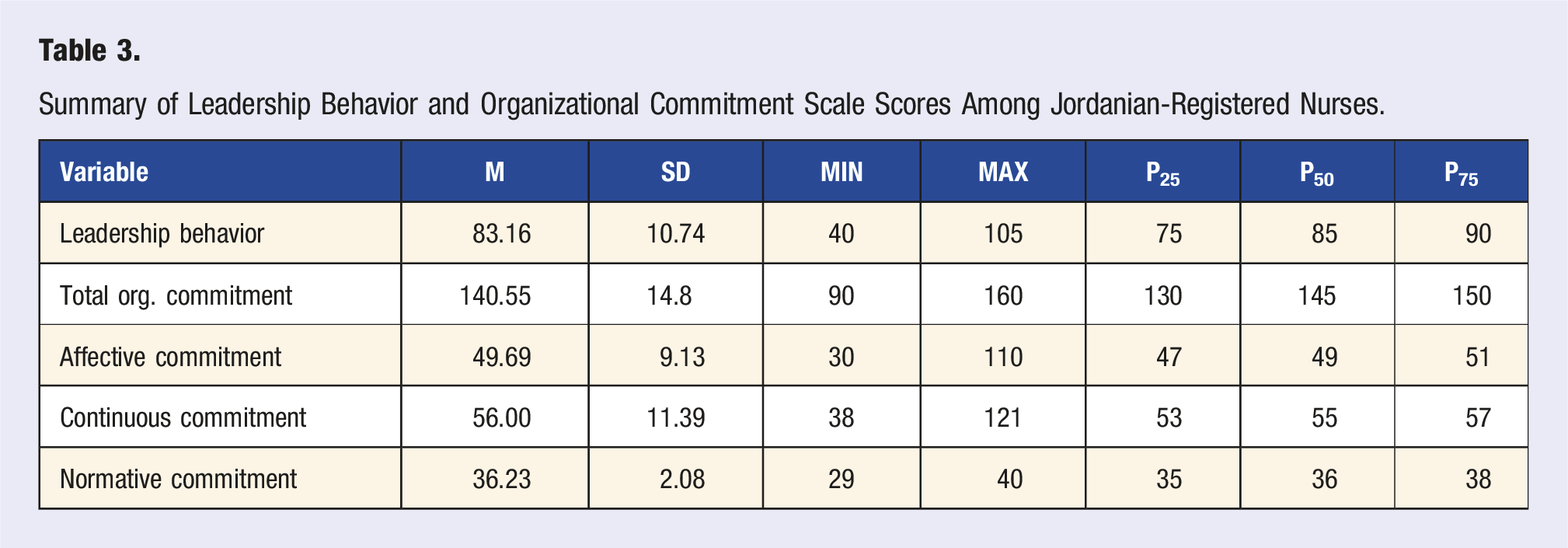
Summary of Leadership Behavior and Organizational Commitment Scale Scores Among Jordanian-Registered Nurses.
Differences/Relationships Between Selected Demographic Variables and Nurses Perceived Quality of Nursing Care
To answer the first research question, “Is there a relationship between nurses’ demographic variables and nurses’ perceived quality of nursing care?” The independent t test and one-way ANOVA were used, with significance set at α < 0.05. Following the examination and confirmation of all parametric test assumptions, it was ensured that sample observations were random, all variables exhibited a normal distribution (with skewness values falling within the range of −2 to +2 and kurtosis values within the range of −7 to +7), and there was equality of variances across all variables. Results of the independent t test revealed that there were significant differences (t251 = 13.22, P < 0.001) between males and females in their perception of quality of nursing care scores. Similarly, there was a significant difference (t251 = 12.26, P= < 0.001) between males and females in leadership behavior scores. Similarly, there was a significant difference (t251 = 8.98, P= < 0.001) between males and females in their organizational.
Difference in Nurses Perceived Quality of Care Scores, Leadership Behavior, and Organizational Commitment Based on Gender.
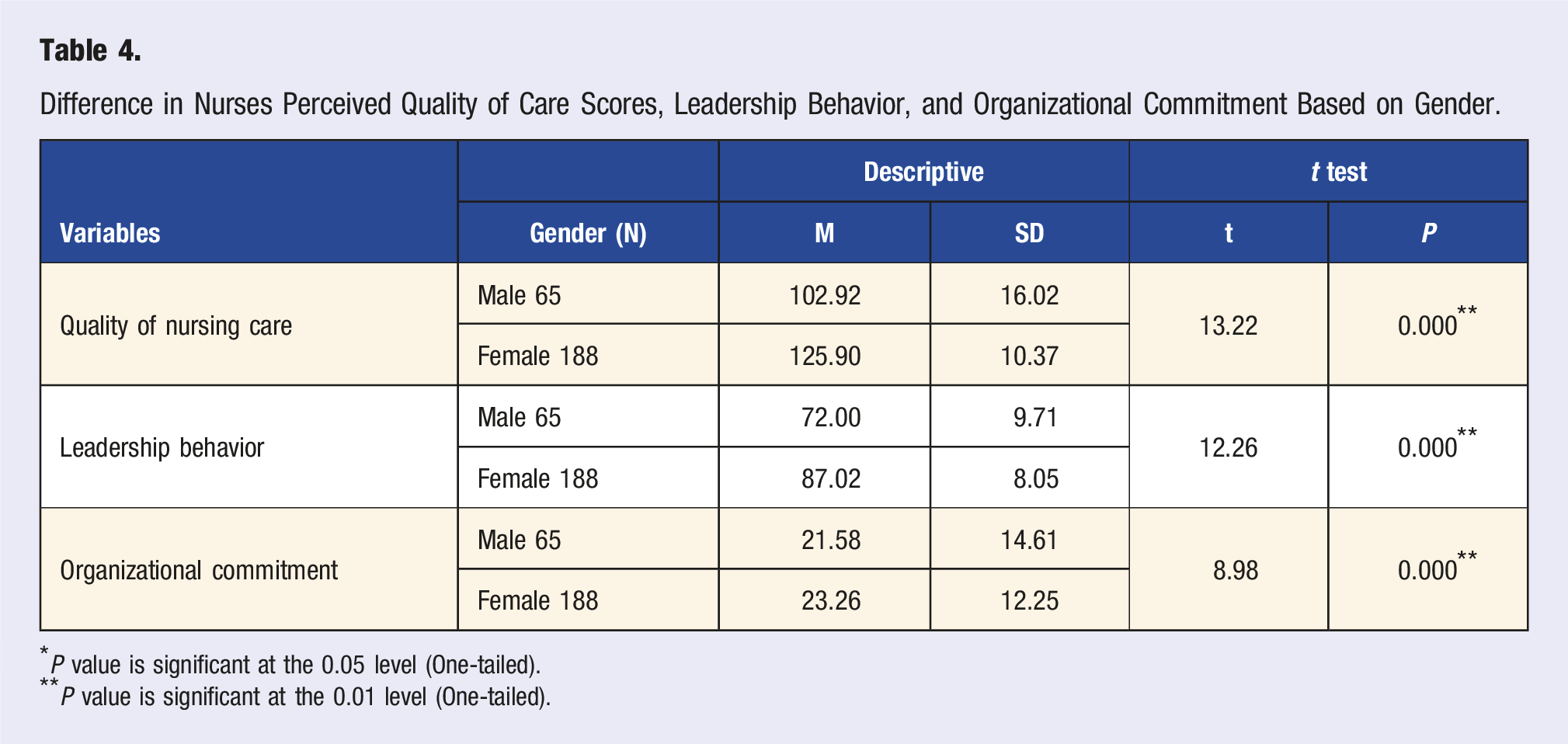
*P value is significant at the 0.05 level (One-tailed).
**P value is significant at the 0.01 level (One-tailed).
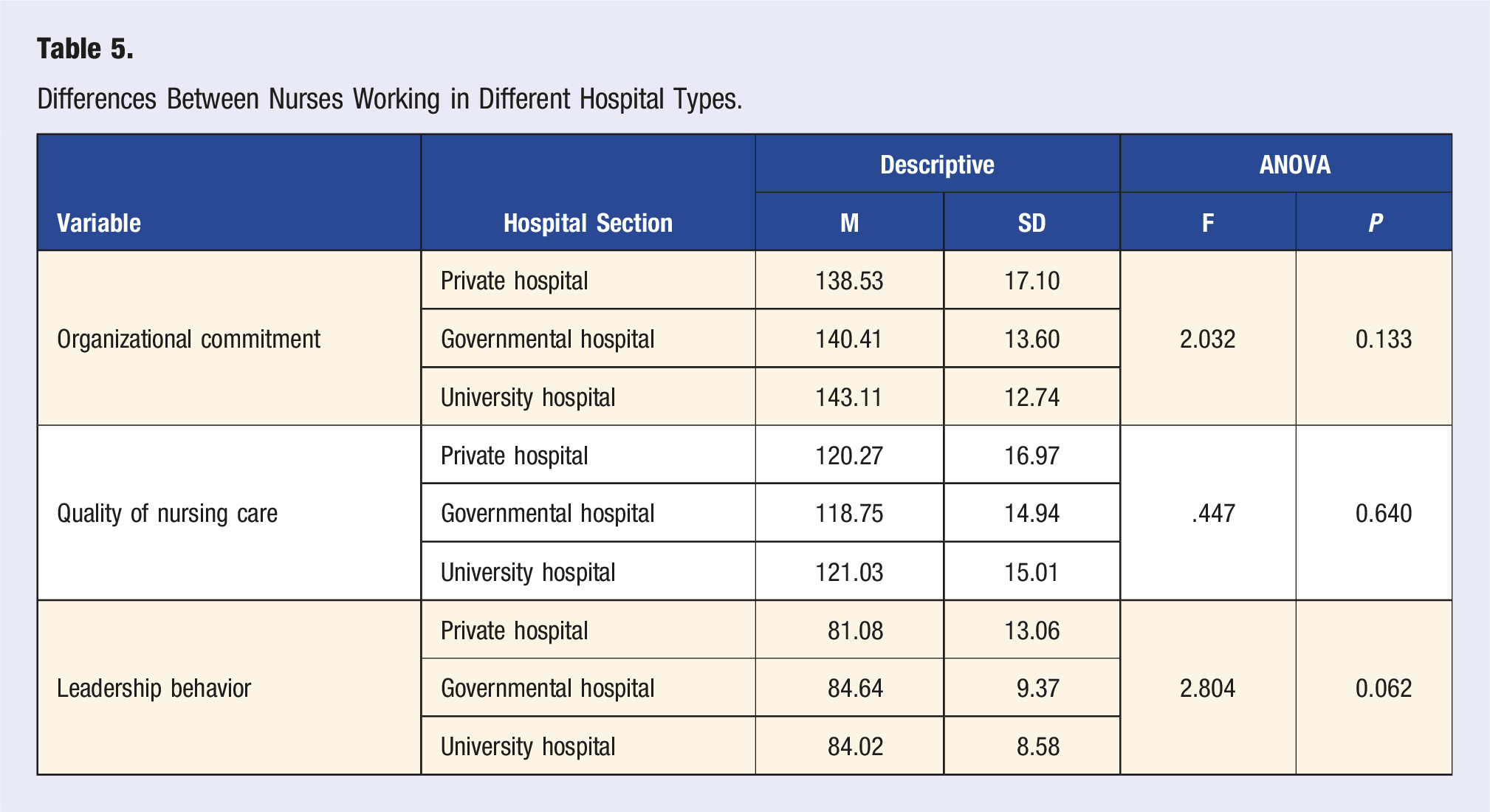
Differences Between Nurses Working in Different Hospital Types.
Correlation Between, Leadership Behavior, Organizational Commitment, Age, General Nursing Experience, Current Organization Experience, Monthly Income and Perceived Nurses Quality of Nursing Care
To answer the research question, “What are the correlations between the independent variables (leadership behavior, organizational commitment, age, nursing experience, current organizational experience, and monthly income) and the dependent variable (perceived nurses’ quality of nursing care)?” The Pearson’s correlation test was employed, with the significance level set at α < 0.05. Furthermore, following the examination and confirmation of all parametric test assumptions, it was ensured that all variables exhibited a normal distribution (with skewness values falling within the range of −2 to +2 and kurtosis values within the range of −7 to +7), and there was equality of variances across all variables.
Correlation Between Leadership Behavior, Organizational Commitment, Age, General Nursing Experience, Organization Experience, Monthly Income and Perceived Nurses’ Quality of Nursing Care.
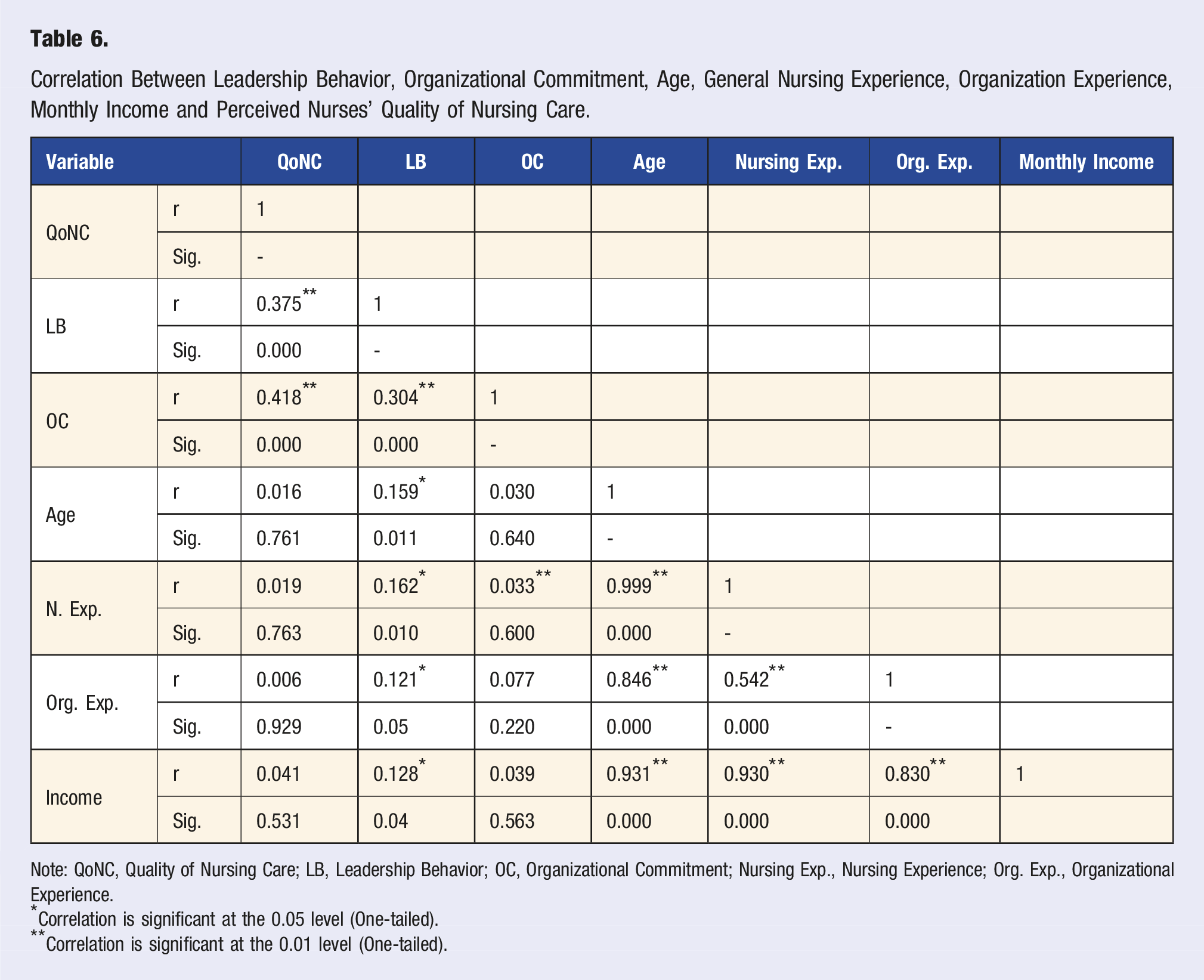
Note: QoNC, Quality of Nursing Care; LB, Leadership Behavior; OC, Organizational Commitment; Nursing Exp., Nursing Experience; Org. Exp., Organizational Experience.
*Correlation is significant at the 0.05 level (One-tailed).
**Correlation is significant at the 0.01 level (One-tailed).
The results indicate a significant positive relationship (r = 0.304, P < 0.001) between organizational commitment and leadership behavior. This means that nurses with higher scores on leadership behavior are more likely to have higher organizational commitment. In addition, there was a significant positive relationship between organizational commitment and nursing experience (r = 0.333, P < 0.001). This means that nurses with more years of experience are more likely to be committed to their organizations. Likewise, there was a significant positive relationship (r = 0.162, P < 0.001) between leadership behavior and nursing experience. This means that experienced nurses had higher scores for leadership behavior, as shown in Table 6.
Predictors of Nurses’ Perception of Quality of Nursing Care
Collinearity Analysis of Perceived Quality of Care Among Jordanian-Registered Nurses.
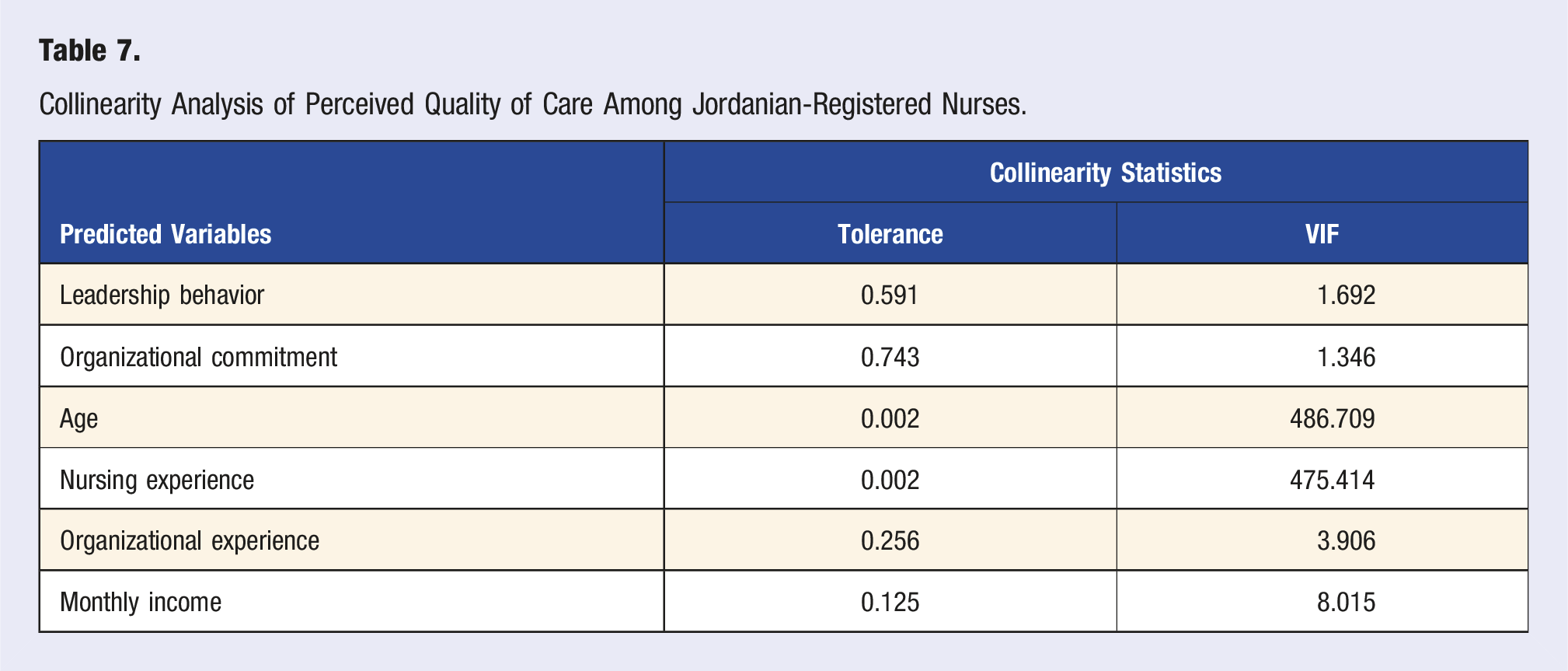
Also, Multicollinearity was confirmed through checking the values of the correlation coefficient (r) between the predictors, and it was observed that the highest value between “nursing experience” and age (r = −.999, P < .001), which showed that predictors chosen are measuring different things and there is an absence of multicollinearity (See Table 7).
Additionally, an examination of the histogram of standardized residuals indicated that the data contained approximately normally distributed errors. This was further supported by the normal P-P plot of standardized residuals, which displayed points that were not precisely on the line but in close proximity. Furthermore, the scatterplot of the standardized predicted values confirmed that the data satisfied the assumptions of homogeneity of variance and linearity.
To determine the predictors, forward stepwise linear regression was performed by setting the significance point at α < 0.05. Four variables were predictors of the quality of nursing care. These variables were leadership behavior, organizational commitment, organizational experience, and monthly income. The results revealed that the best prediction model consisted of the following predictors: leadership behavior, organizational commitment, and monthly income.
The forward stepwise multiple linear regression was conducted to identify predictors of perceived quality of nursing care. However, acknowledging the statistical concerns raised regarding stepwise selection—such as overfitting, unstable variable selection, and biased standard errors—we reanalyzed the data by entering all theoretically relevant variables simultaneously in a multiple linear regression model. Additionally, we applied k-fold cross-validation (k = 10) to assess the model’s generalizability and reduce the risk of overfitting. Model fit was evaluated using the Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) to allow for model comparison and to support the robustness of the regression results. A revised regression model was tested by including all theoretically relevant predictors simultaneously. The model yielded an R2 = 0.236. To evaluate model performance, AIC and BIC were calculated: AIC = 712.3, BIC = 745.9. The 10-fold cross-validation revealed minimal difference between the training and validation errors, supporting model generalizability and robustness.
Predictors of Perceived Quality of Care Among Jordanian-Registered Nurses.
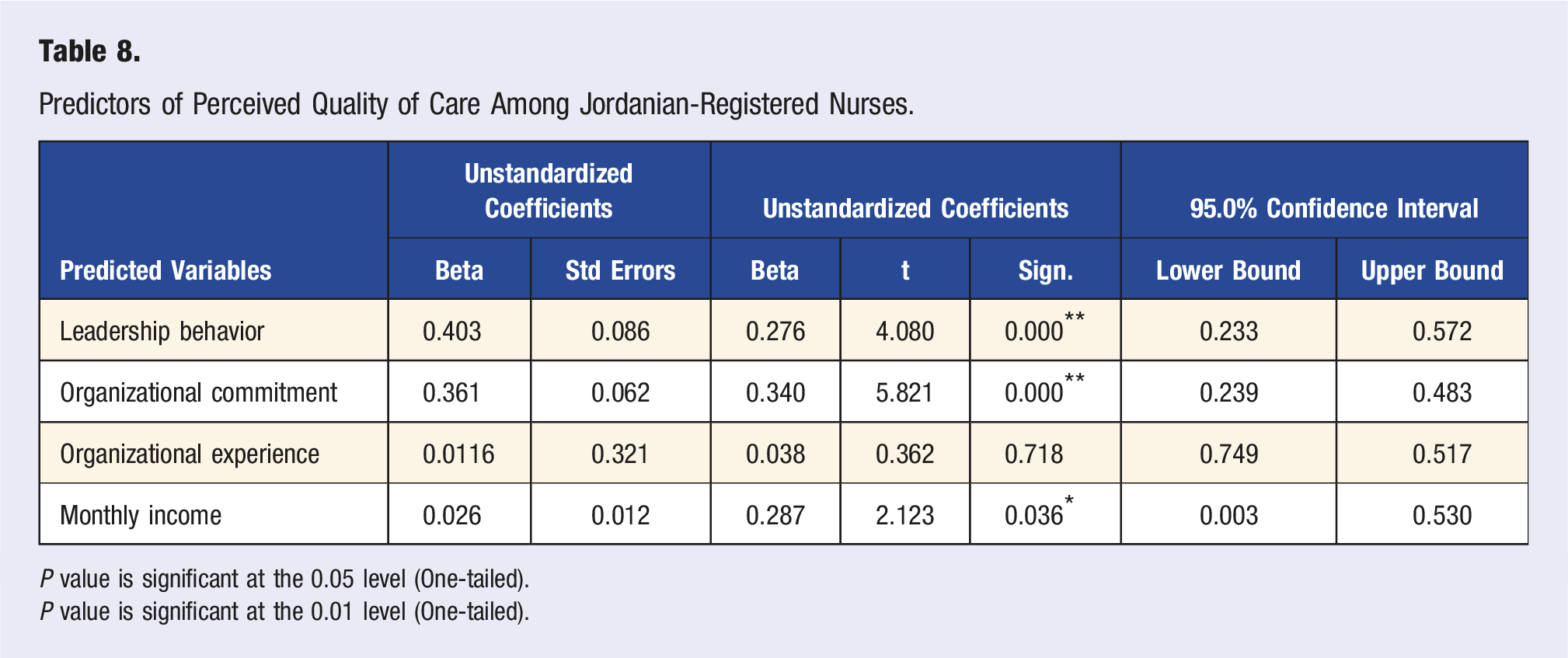
P value is significant at the 0.05 level (One-tailed).
P value is significant at the 0.01 level (One-tailed).
Discussion
Descriptive data on the participants’ demographic variables revealed that the majority of registered nurses were female. This result is consistent with other studies in Jordan,33,34 the United States,35,36 China,37,38 and Canada, 39 implying that the majority of nursing workforce in Jordan is females due to the policy implemented by the Ministry of Higher Education regarding the student acceptance in nursing colleges, which states that 70% of the admissions to nursing colleges are females. 40
Regarding marital status, most participants were married. This result is consistent with other Jordanian studies,34,41,42 China 38 and Canada. 39 In addition, the majority of participants were young, reflecting that the young workforce in the nursing discipline is consistent with the results of Dwyer et al 35 results in the United States and Liu et al 37 in China.
With regard to the educational background in the current study, the level of education for participants was mostly a bachelor’s degree, in agreement with results in Jordan33,34,41,43; and in the United States35,36,44 reflecting that the majority of the working force in the nursing discipline holds a bachelor’s degree. Whereas, the nursing experience background showed that the average for years of nursing experience was 12.6 years while it was 1-5 years in the study by Alfuqaha and Alsharah, 33 Alfuqaha et al 34 . In addition, it has been less than 5 years in China. 38
The results demonstrated that there were significant differences between males and females in their perceptions of quality of nursing care. The results indicated that female nurses had a higher perception of QoC than male nurses. This indicates that nurses of different genders perceive nursing care as recognizing and respecting the uniqueness and value of each individual. The present findings are consistent with other studies such as Tong et al 45 and Wei et al. 46 However, the results of this study differ from those of previous studies such as Albougami 47 and Trinidad et al. 48
The findings of this study indicated no significant difference in perceived QoC scores between nurses with bachelor’s and master’s degrees, aligning with the results of a study by Peršolja. 49 This may be due to the nature of nurses’ work, which does not necessarily depend on their educational level. In addition, the results revealed that there was no significant difference between nurses with different marital statuses and hospital types in their nurses’ perceptions of the quality of nursing care, which is consistent with Yusefi et al. 50
Analyses were conducted to determine if any relationships existed between the independent study variables (Leadership Behavior, Organizational Commitment, Nursing Experience, Age, and monthly income) of registered nurses and their perceptions of the quality of nursing care. The majority of the results indicated a statistically significant low-to-moderate positive correlation between the independent and dependent variables (Quality of Nursing Care).
Moreover, the results provide further evidence of the perception of the quality of nursing care among Jordanian-registered nurses. This study demonstrated that the total level of perception of nursing care among Jordanian-registered nurses was moderate, as reflected by their moderate reliability, assurance, tangibles, empathy, and responsiveness. This is consistent with previous studies in Jordan by Salahat and Al-Hamdan 51 and Alharbi et al, 52 which shed light on nurses’ perceptions of quality of care as a significant issue in Jordan and urges administrators in the healthcare industry to enhance the hospital environment to increase the quality of nursing care.
Additionally, the results indicated a significant positive relationship between age, monthly income, leadership behavior, organizational commitment, and quality of nursing care. Leadership behavior as perceived by RNs was assessed in this study. Numerous studies have recognized leadership behavior as a key element in the quality of nursing care.12,53 The results of this study revealed a significant positive relationship between nurses’ perceived quality of nursing care and leadership behavior. An explanation could be that nurses who work in good leadership context have higher levels of quality of nursing care than those who work in contexts with a lack of leadership. Moreover, the present study showed a significant positive relationship between nurses' organizational commitment and the perceived quality of nursing care. This finding was in line with the results of a study by Elserogy et al, 54 however, it contradicted those of a study by Seyedoshohadaee et al. 55
Finally, the third research question was “What are the predictors of registered nurses’ perceived quality of nursing care among the study variables: demographics, organizational commitment, and leadership behavior?” Analyses for the third research question were used to determine if predictors for quality of nursing care, were present using forward stepwise multiple linear regression.
The current results revealed that leadership behavior, organizational commitment, and monthly income were predictors of nurses’ perceived quality of nursing care. Moreover, the results of this study indicate that leadership, organizational commitment, and monthly income are key to enhancing the quality of nursing care. This is supported by Kibret et al,
56
Havaei et al,
57
and Lee and Yom.
58
Moreover, a study conducted by Nikjooy et al
59
stated that nurses’ organizational commitment was a predictor of the quality of nursing care in addition to other work-related factors.
60
The results revealed that leadership was a predictor of quality of nursing care. Similar to the present study, Foss
61
found that leadership was a predictor of nurses’ perceptions of the quality of nursing care. Furthermore, other independent variable, sex, was not a predictor in this study for quality of nursing care. In Summary
Limitations and Implications of the Study
This study has certain limitations, notably, its reliance on self-reporting, which is susceptible to various response biases. The instruments that were used in this study may be susceptible to social desirability responses because some items may be viewed as either intrusive, or more socially desirable than others. Nurses who were engaged, and felt a commitment to the organization may were more likely to participate. Measurement of the staff nurse’s perception of leader behaviors and the nurse’s own level of quality of nursing care a one-time session may be a limitation because participants may answer questionnaire based on their selective memory. However, the use of anonymity may help to reduce the possibility of social desirability.
Despite these limitations, the results of this study have the potential to contribute to the ongoing professional development in the nursing discipline. These findings augment the limited knowledge base of this specific area of research. Further research should be conducted to examine the quality of nursing care throughout undergraduate nursing education and continue monitoring throughout the new graduate period especially within 2 years of graduation. In addition, the results of this study could be used by nursing leadership and healthcare authorities to assess current working conditions and to develop and appropriately implement effective policies and interventional strategies that consider nurses’ and organizational needs. Nursing educators may find it useful to apply the study’s outcomes to identify new practice roles for nursing students, better prepare them to assume effective leadership roles, and advocate for nurses. Additionally, the results may inform the development of professional training programs, the establishment of formal and informal support networks, and the allocation of resources, all of which contribute to enhancing the overall quality of nursing care.
Conclusion
This study marked an inaugural investigation into the primary determinants of nursing care quality among registered nurses in Jordan, utilizing a validated and extensive measure of organizational commitment and leadership behaviors. This study was the first to examine the relationships between Jordanian-registered nurses’ perceptions of the quality of nursing care and their perceptions of nurses’ organizational commitment and leadership behavior in Jordan, and shed light on important results for administration, clinical practice, and future research. The study revealed significant insights and identified gender, organizational commitment, monthly income, age, and nursing experience as key predictors of nurses’ perceived quality of nursing care. Therefore, there is an urgent need to improve the overall quality of nursing care.
Footnotes
Acknowledgments
Mahmoud Al-Hussami acknowledges that this research was conducted during the sabbatical leave of the University of Jordan, school of nursing for the academic year 2023/2024. We sincerely thank the participants and directors of nursing at the participating hospitals.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.