
Abstract
“Most participants were willing (98.1%) to change their lifestyle habits in the upcoming six months to improve their health.”
Introduction
Over the past 10 years, the epidemiological shift in stroke incidence has alarmingly transformed the stroke landscape. Stroke incidences have significantly increased (∼40%) among the working population (≤65 years of age) with approximately 15% among persons ≤50 years of age 1 and projections of prevalence rising over the next 30 years. 2 In this population, stroke has detrimental personal (e.g., identity, family, physical, mental health), professional (e.g., careers, work), societal, health care, and economic impacts.3,4 Appreciating such unique impact of stroke on younger adults, compared to older adults, and the paucity of research among this patient population, the research team conducted a needs assessment study to assesses younger adult stroke patients: (1) physical, psychological, and occupational functioning and health-related quality of life; and (2) post-stroke care preferences using patient reported outcome measures. 5 A key finding from the needs assessment study was that ≥70% of the participants (N = 85) reported the need for additional support and interventions on their physical health and preferred in-person post-stroke care led by health care providers. 5
More importantly, the rising stroke incidences among younger adults have been strongly attributed to modifiable risk factors (MRFs).6-9 Further, while the literature is emerging on the recurrence of stroke among younger adults, the risk remains significant particularly for those with unmanaged risk factors such as hypertension, diabetes, and smoking.10,11 This highlights the importance of focusing on risk factor modification and the adoption of healthy lifestyle habits,12,13 which can be achieved through lifestyle medicine (LM).14-16 LM, the cornerstone of primary and secondary stroke prevention,17,18 is an evidence-based clinical discipline that applies a root-cause approach to optimize healthy lifestyle behaviors to promote health, prevent, manage and/or treat disorders and the associated MRFs.16,19,20 LM comprises of six pillars—nutrition, physical activity, sleep health, stress management, substance use, and social connectedness. 19 There are countless studies supporting the positive effect of LM on reducing chronic disease (e.g., type 2 diabetes), and cerebrovascular disease (stroke) risk and reoccurrence.16,21-23 The strength of the LM research is underscored by numerous evidence-based clinical guidelines from the American Heart Association24,25 and the Heart and Stroke Foundation of Canada 26 on risk factor modification through positive and healthy lifestyle behaviors.
According to several behavioral change theories (e.g., health belief model, knowledge attitude practice model, social cognitive theory) and empirical evidence, a precursor to behavior change is knowledge.27-29 While knowledge is essential to promote healthy behaviors, it is insufficient on its own 30 and often does not translate into the adoption and sustainment of healthy behaviors. 31 This highlights the importance of understanding the contextual facilitators and barriers to behavior change 32 as this influences the adoption of positive and healthy behaviors. Such information is vital to apprise the design (e.g., content, mode of delivery) and successful implementation of evidence-based behavioral interventions that support, equip, as well as adequately address the contextual and influencing factors, needs and preferences of younger adults; all of which supports brain health which is vital for healthy aging, functional independence, and predicting quality of life. 33 However, to date, lifestyle-related knowledge, behaviors and influencing factors are not well understood among younger adult stroke and high-risk patients. This study aimed to fill this gap by attaining an understanding of younger adult stroke and high-risk stroke patients’ lifestyle-related knowledge and behaviors as well as influencing factors for the adoption of healthy lifestyle behaviors with attention to also sex, age and stroke status differences.
Methods
Study Design and Ethical Consideration
A cross-sectional study was conducted. The study was part of a larger explanatory sequential mixed methods quality improvement (Know Brain Embrace Care) investigation of younger adult stroke patients’ knowledge around health risk factors, brain health and LM concepts, facilitators and barriers with the adoption of healthy lifestyle habits as well as recommendations for preferred LM-related interventions to support brain health prevention. The findings for this study are reported using guidelines of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) for cross-sectional studies. 34 The study was approved by the UHN Quality Improvement Committee (QIRC#23-0518). Verbal consent was attained by the research coordinator.
Setting and Participants
The study was conducted at the Toronto Western Hospital (TWH), University Health Network (UHN) located in Toronto, Canada, which is one of the largest stroke centers in the province (Ontario), affiliated with the University of Toronto. A consecutive sampling method was employed. Specifically, patients attending the Stroke Prevention or Neurovascular Clinics at TWH were approached from June 2022-September 2023. Patients who met the inclusion criteria were approached and recruited by a research coordinator. The study population encompassed younger adult patients who at the time of participation: (1) had an ischemic or hemorrhagic stroke >90 days prior to recruitment or were at higher risk for stroke (no stroke, but a diagnosis of TIA, unruptured aneurysm or vascular malformation); (2) were of working age (≤65 years of age); (3) were receiving care at either the Stroke Prevention (stroke or TIA) or Neurovascular (aneurysm or vascular malformation) Clinic at TWH; and (4) were able to communicate in English. Patients were excluded if they had a known brain injury that resulted from trauma and had known advanced cognitive impairment (defined as a diagnosis of dementia and/or mRS >(4) that would preclude them from providing informed consent. Patients were considered for inclusion, based on assessments by members of the health care team (e.g., Neurologists, Nurse Practitioners) during clinic visits and proceeded to inform the research coordinator. Following this, potential participants were approached by the research coordinator to explain the study, provide a letter of information, and answer any study-related questions.
Data Collection
Data were collected from the consented participants through a survey, which was either hard copy or electronic (based on the preference of the participant).
Sociodemographic and Clinical Characteristics
Participant’s sociodemographic and clinical characteristics were collected through a REDCap survey. Sociodemographic characteristics were assessed with questions pertaining to sex, gender, age, level of education, ethnicity, language, marital status, employment status, family structure, and household income. Clinical characteristics were assessed with questions about stroke status, number of strokes, time since stroke (in months) and diagnosis of any other neurological condition.
Variables and Instrumentation
The study variables were: (1) lifestyle knowledge; (2) lifestyle status and associated facilitators and barriers; and (3) health behavior motivation.
Lifestyle Knowledge
Data were obtained through questions on lifestyle knowledge using an investigator-developed questionnaire that was guided by the Life’s Essential 8 recommendations 24 and the Brain Care Score (BCS).35,36 All participants received multiple-choice questions with different cut-off values as options and were asked to select the recommended guidelines on blood pressure, physical activity, nutrition, substance use, sleep health, and alcohol use, with definitions and examples provided when necessary. The correct recommendations included: (i) a blood pressure of 120/80 mmHg or below; (ii) at least 150 minutes of moderate exercise per week—for example, brisk walking or activity that makes one breath harder, but can talk; (iii) consuming at least 4.5 servings of fruits and vegetables per day—for example, one serving equal to a handful or one cup and does not include fruit juice; (iv) 2 servings of lean protein per day—for example, an adult portion equivalent to about a palm size; (v) 3 servings of whole grains per day—for example, brown rice, whole wheat pasta/bread, quinoa, whole oats—unprocessed with one adult portion equivalent to one cup or one slice; (vi) 1500 mg of sodium intake per day—for example, one teaspoon of table salt has 2300 mg of sodium; (vii) a sleep duration of 7-8 hours per night; and (viii) 1-2 alcoholic drinks per day. We assessed the level of knowledge by the number of correct recommendations, ranging from 0 to 8.
Lifestyle Behaviors
Data were obtained through questions on participants’ lifestyle status using investigator-developed questions guided by the American Heart Association and Centres for Disease Control and Prevention recommendations and the American College of Lifestyle Medicine (ACLM) validated tools. 37 Questions focused on all six pillars of LM and inquired about the extent to which participants engaged (e.g., frequency, duration, amount) with the various pillars. For example, (e.g., if asked about moderate physical activities, participants were given a simple definition: moderate physical activity is an activity that takes physical effort and makes you breathe somewhat harder than normal but able to talk, examples: brisk walking, carrying light load, biking at regular pace). Physical activity, specifically for walking, was converted into daily steps. 38
Health Behavior Motivation
The Health Behaviour Motivation Scale (HBMS) was used. The HBMS is based on the Self-Determination Theory and measures persons’ motivation towards pro-health behaviors. The tool comprises of five dimensions: (1) intrinsic regulation; (2) identified and reintegration regulation; (3) introjected regulation; (4) external regulation; and (5) amotivation. The tool is anchored on a 5-point Likert scale ranging from 1 (statement not suiting me at all) to 5 (statement suits me very well). The HBMS is psychometrically robust, Cronbach’s α = 0.91-0.94. 39
Statistical Methods
Descriptive and inferential statistics were conducted using SPSS (Version 29) 40 and R software v4.1.0. 41 The sample was described using descriptive statistics. Lifestyle knowledge-related variables, which were categorical, were described using counts and percentages. Lifestyle status-related variables, which were continuous and categorical, were described using means and standard deviations (SDs) and counts and percentages, respectively. We employed Linear Model ANOVAs for continuous data that followed normal distribution, while Pearson chi-square tests were applied for categorical data. Descriptive subgroup analysis was also performed for sex, age (≤45 year and ≥45 years) and stroke history. All analyses used a significance level of P < 0.05.
Regression Models
We performed univariable and multivariable logistic regression models with the primary outcome being the level of knowledge based on the correct number of lifestyle knowledge answers. We dichotomized the level of knowledge at the median, resulting in two groups: (i) lower level of knowledge (≤3) and (ii) higher level of knowledge (≥4).
Variables for univariable logistic regression were selected a priori, driven by past literature shown to associate with knowledge of risk factors for brain disease.8,42-44 These variables included age, sex, marital status, education, employment, income level, ethnicity, history of stroke, and Canadian or foreign-born status. For the multivariable analyses, we based our choice of confounders on variables which were significantly associated with lifestyle knowledge in the univariable analysis and previously published epidemiological data.8,42,45 We presented our logistic regression results as odds ratios (OR) with corresponding 95% confidence intervals (CI) and P-values. A two-tailed P-value of <0.05 was considered statistically significant. We evaluated multicollinearity in each model through the variance inflation factor, while model fit was assessed using McFadden’s Pseudo-R squared. A McFadden’s R2 value between 0.2 and 0.4 indicates excellent model fits. 46
Results
Participants
A total of 260 patients were screened for eligibility by a member of the health care team and of those, the research coordinator could not reach 66 to inquire about their interest to take part in the study. Of the 194 participants approached, 90 declined to take part for various reasons (e.g., no response after three attempts, lack of time and/or interest, language barrier). A total of 104 participants comprised the study sample (Figure 1). STROBE flow chart.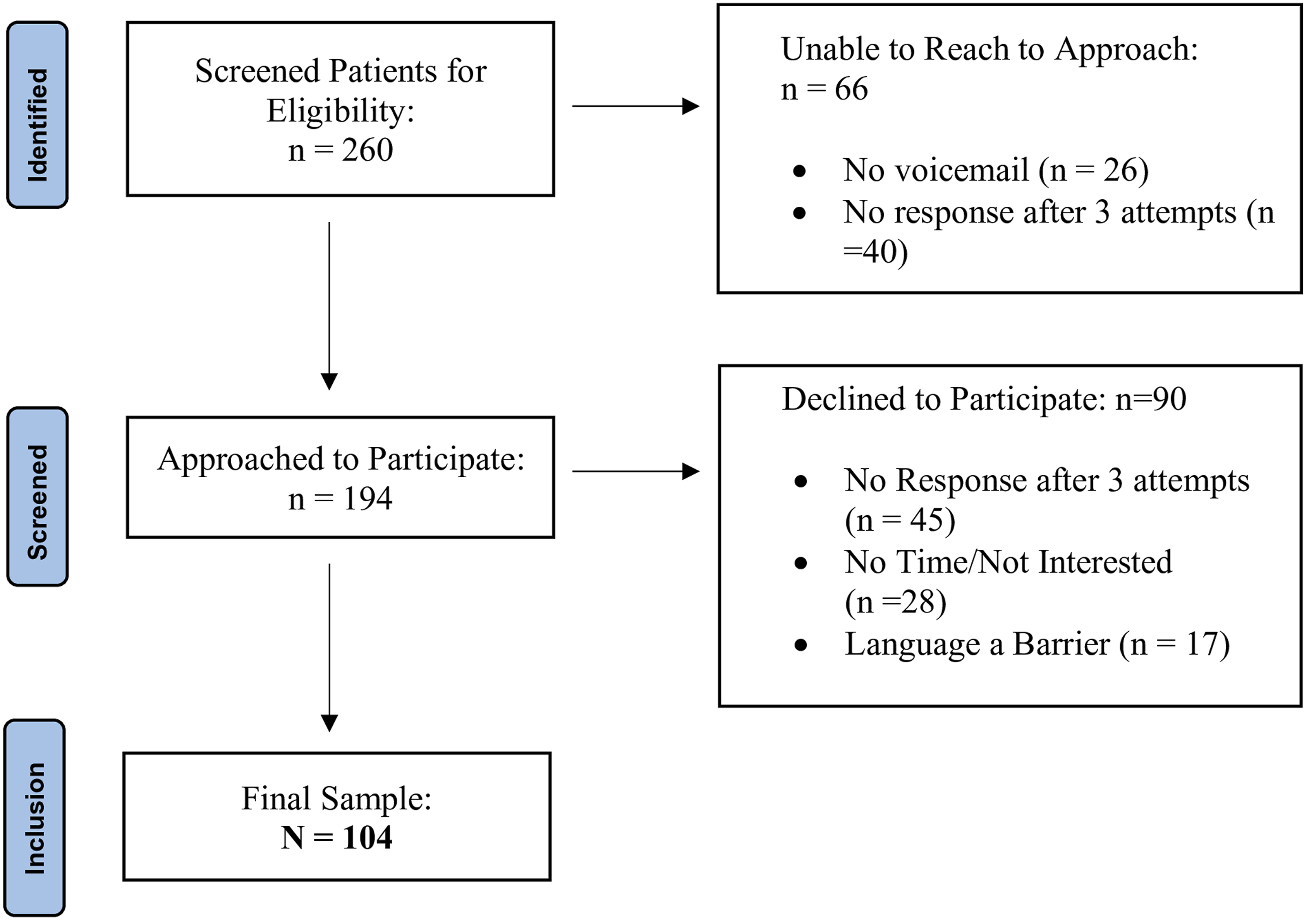
Sociodemographic Characteristics
Sociodemographic Characteristics.
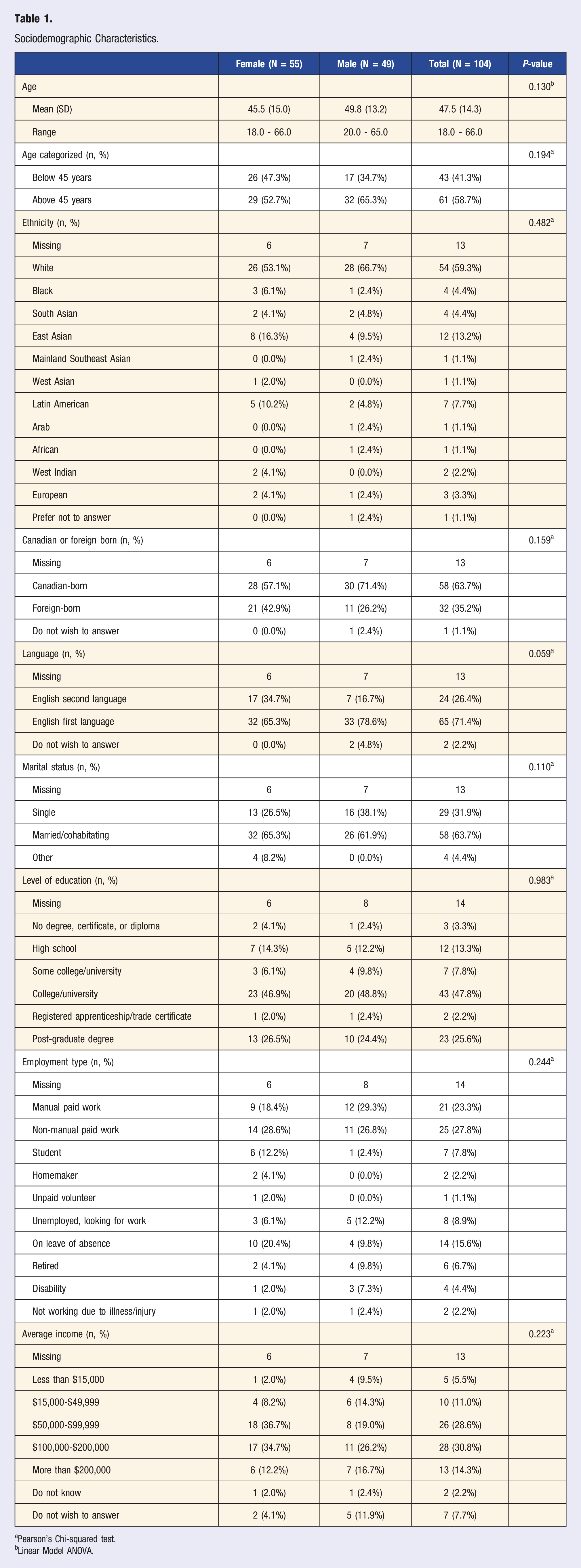
aPearson’s Chi-squared test.
bLinear Model ANOVA.
Clinical Characteristics
Clinical Characteristics.
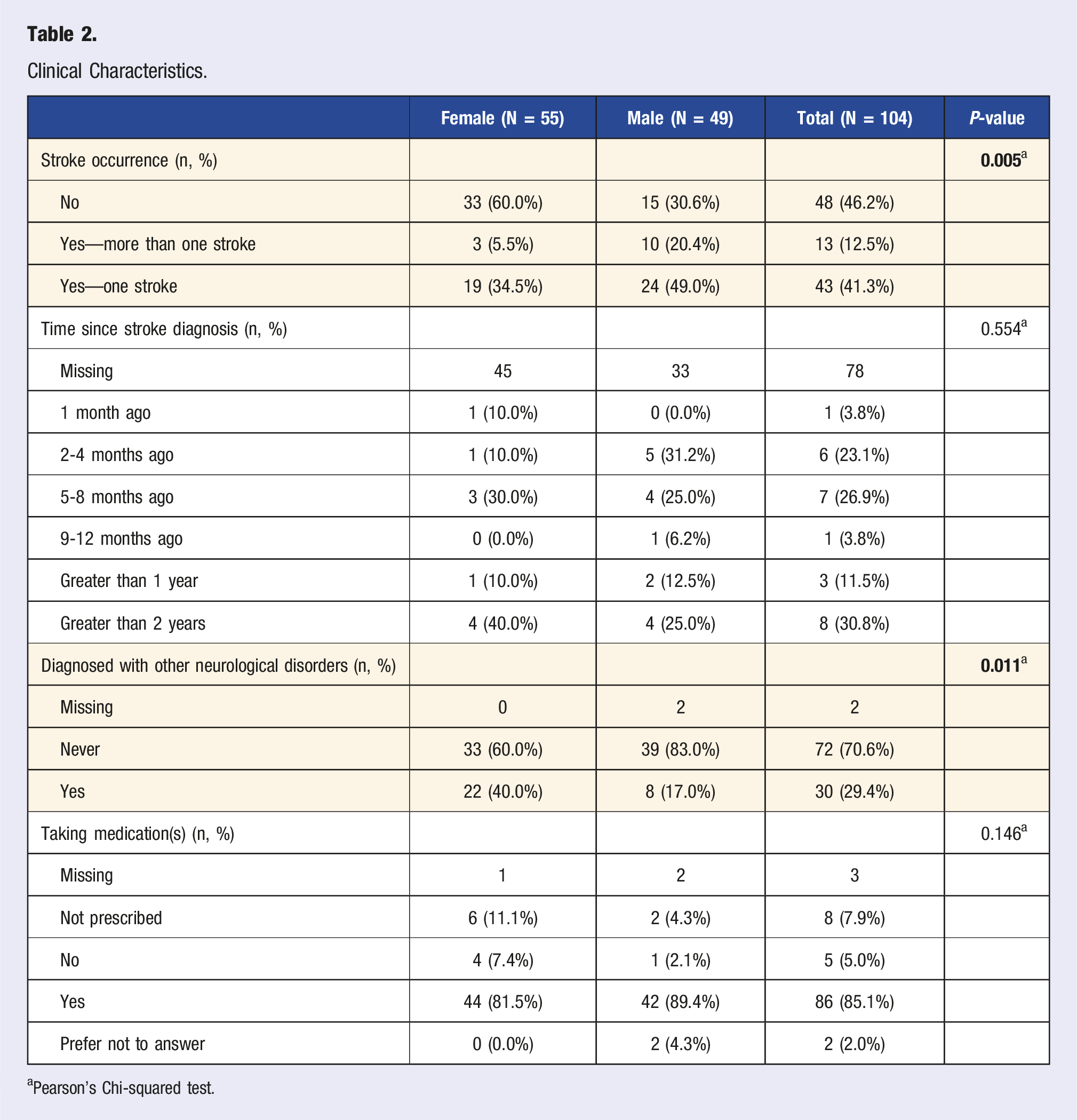
aPearson’s Chi-squared test.
Lifestyle Knowledge
Healthy Lifestyle Knowledge.
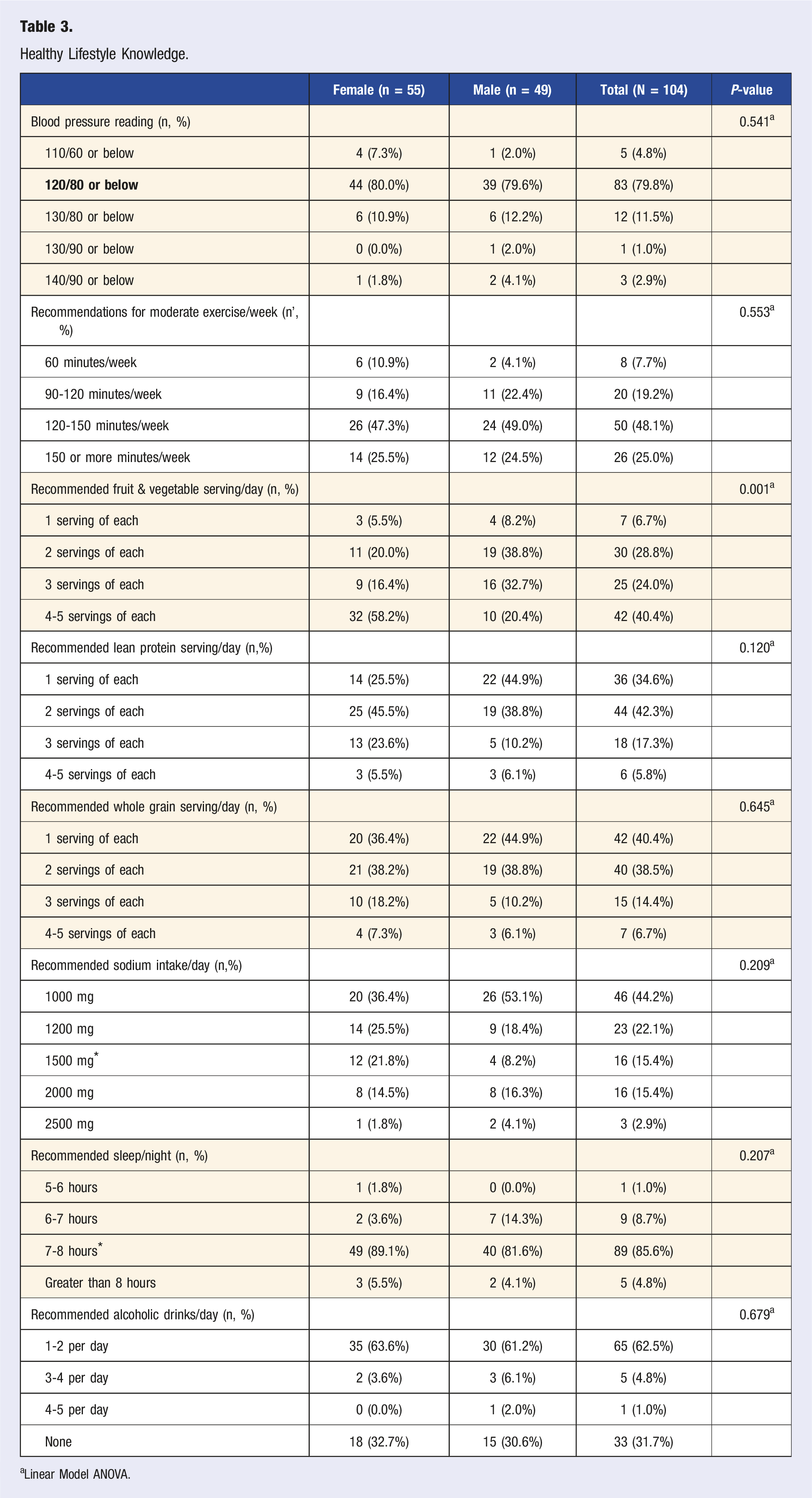
aLinear Model ANOVA.
Level of Knowledge
The distribution of knowledge levels was as follows: 0 participants had only 1 correctly answered recommended guideline questions, 9 (9.7%) participants had 2 correct, 26 (25.0%) had 3, 32 (30.8%) had 4, 25 (24.0%) had 5, 10 (9.6%) had 6, 1 (1.0%) had 7, and 1 (1.0%) had 8. The median level of total knowledge was 4 (IQR 3-5).
Lifestyle Behaviors
Nutrition
Eating Lifestyle Status.
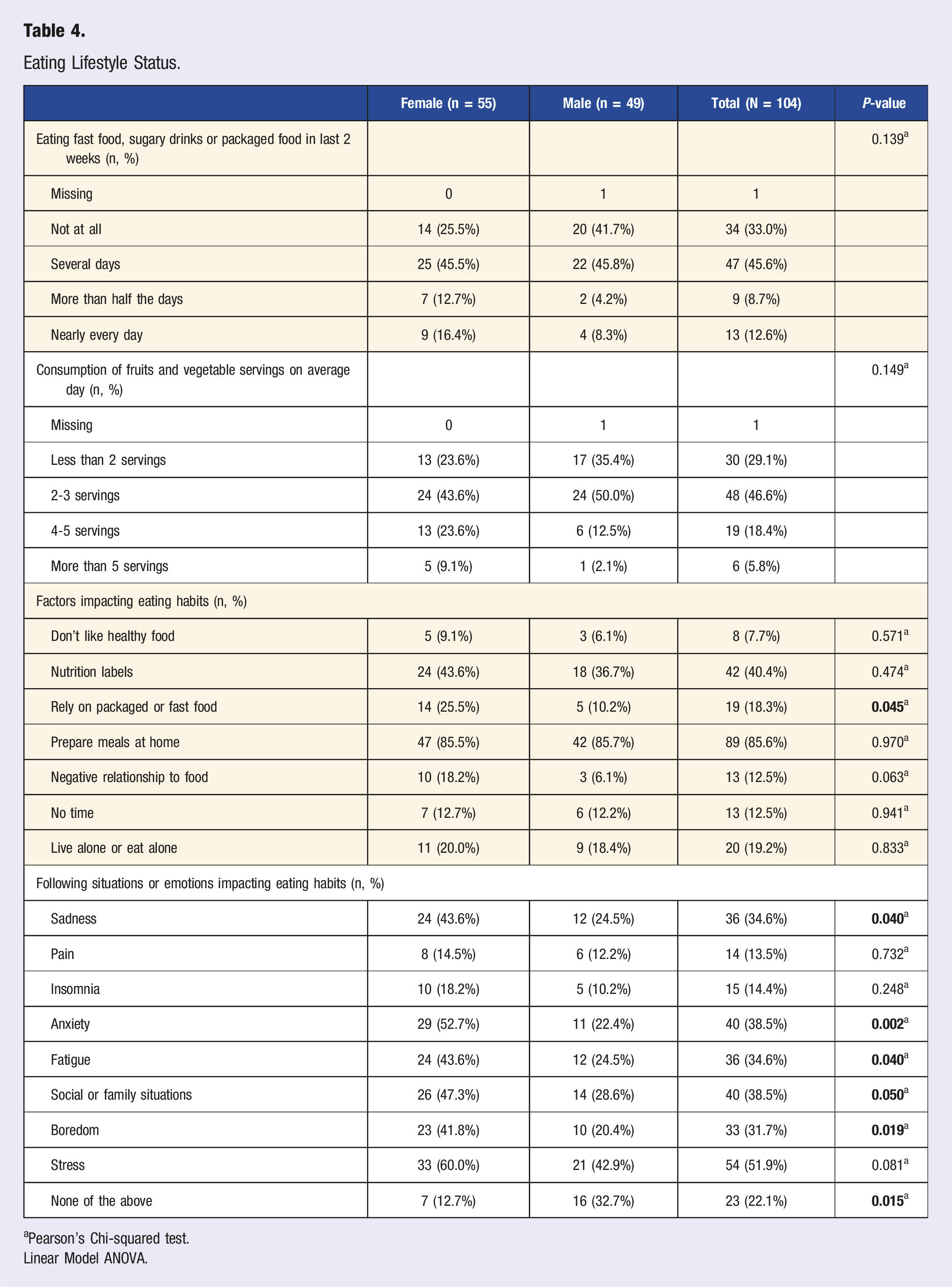
aPearson’s Chi-squared test.
Linear Model ANOVA.
Physical Activity
Physical Activity Lifestyle Status.
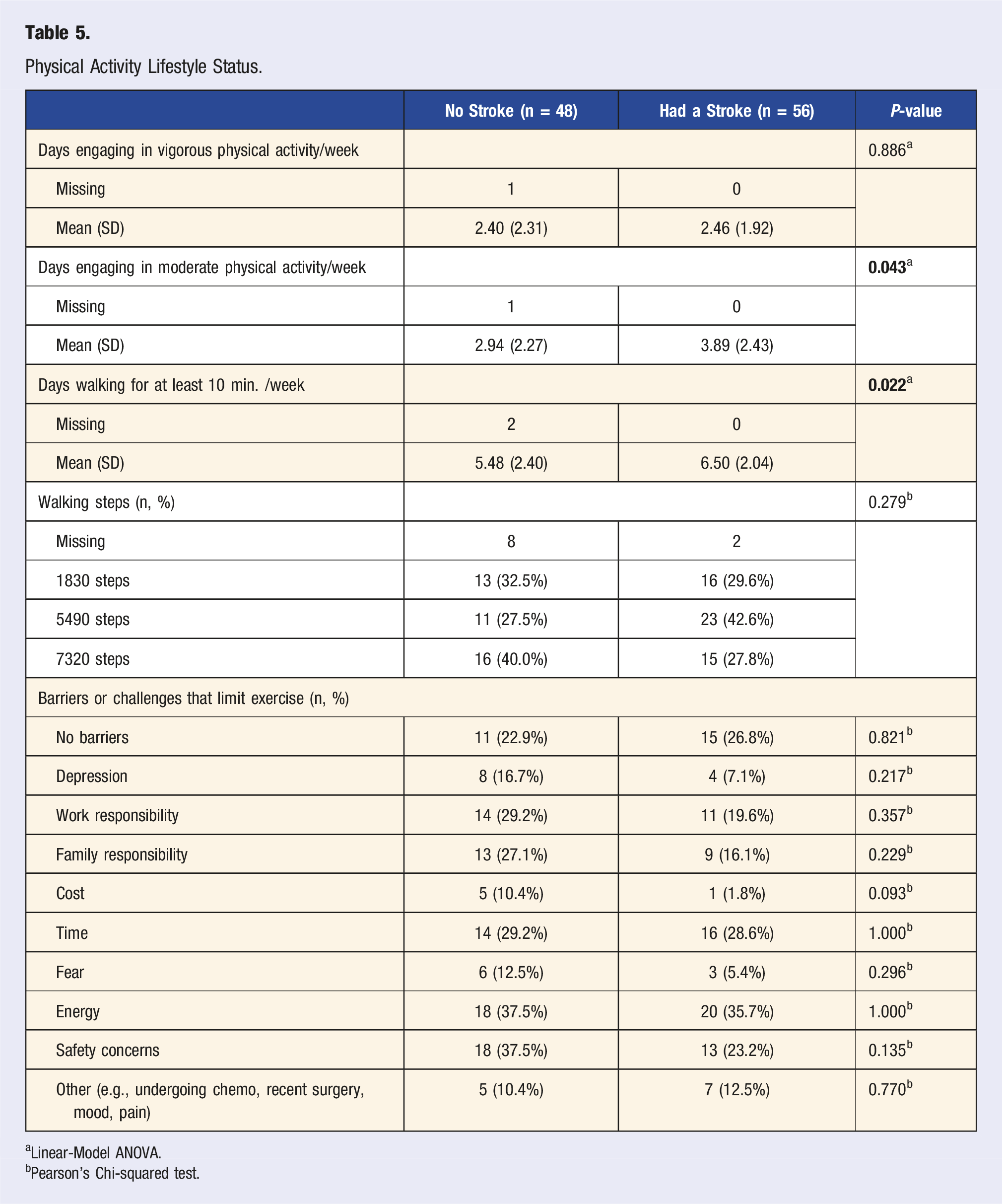
aLinear-Model ANOVA.
bPearson’s Chi-squared test.
Sleep Health
Overall, half of the participants (51.9%) reported having <7 hours of sleep/night. Few participants (39.8%) reported always being on their screen two hours before sleeping time, and most participants (75.7%) reported never using a sleeping aid to fall asleep.
Social Connectedness
Most participants (80.6%) described their social relationships as having at least two persons, other than their family members, that they were close with and most (63.1%) indicated always having persons who care about them. Most participants (84.5%) reported feeling that their life has a meaning and/or purpose.
Stress Management
Participants reported having varying levels of stress with most being manageable (48.5%) and moderate (36.9%). Sometimes (39.8%) participants felt unable to control important things in their life yet, felt fairly confident (31.1%) and very confident (31.1%) in handling personal challenges. Sometimes (38.8%) participants felt overwhelmed, most (56.3%) had little interest doing things, and feeling down, depressed or hopeless (56.3%). Few (44.7%) felt nervous, anxious or on edge on several days as well as bothered by worrying too much (46.1%) in the past two weeks. Participants employed various coping strategies: meditation (23.1%), PA (58.7%), counseling (25%), socializing with friends and family (62.5%), eating too much or too little (41.3%), and TV and/or video games (59.6%).
Substance Use
Most participants drank zero to one drink per week (79.6%) and never smoked (73.8%) or used recreational drugs (97.1%) and marijuana (79.6%). Few participants (14.4%) reported receiving counseling on nutrition.
Lifestyle Adoption Around Brain Health and Motivations
Overall, most participants were willing (98.1%) to change their lifestyle habits in the upcoming six months to improve their health. The priority areas identified by participants to improve their health centered around exercise, nutrition, mental health, and sleep (Supplemental Table 2). Participants rated various reasons for engaging in a healthy lifestyle such as feeling of happiness, overall importance, guilt or remorse if health is neglected, and to make others happy (Supplemental Table 3).
Sex, Age and Stroke-Related Differences
Lifestyle Knowledge
There was a statistically significant sex difference in nutrition-related knowledge. Specifically, females had more knowledge of recommended fruit and vegetable servings (P = 0.001) compared to males. There was also a statistically significant age difference in knowledge of recommended lean protein servings/day (P = 0.048): ≤45 years had more knowledge compared to persons ≥45 years. Likewise, a statistically significant difference was found related to physical activity (PA)-related knowledge (P = 0.022): those who had a stroke understood the current PA recommendations more compared to those that did not have a stroke.
Lifestyle Status
Nutrition
There was a statistically significant age difference with the frequency of processed food consumption (P = 0.045): participants ≤45 years consumed more processed food than those ≥45 years. There was also a statistically significant sex difference with factors influencing eating habits: more females relied on packaged or fast food and had a significantly negative relationship with food compared to males (P = 0.045) (Table 3). There were also notable sex and age-related differences with situations or emotions influencing participants’ eating habits. Of note, sadness (P = 0.040), anxiety (P = 0.002), fatigue (P = 040), social and family situations (P = 0.050) and boredom (P = 0.019) influenced female’s eating habits more than males (Table 3). Similarly, sadness (P = 0.004), anxiety (P = 0.040), and boredom (P = 0.032) influenced the eating habits of participants ≥45 years compared to ≤45 years.
Physical Activity and Sleep Health
Participants who had a prior stroke engaged in more moderate PA days/week (P = 0.043) and walked more (days/week) for at least 10 minutes/week (P = 0.022) compared to those without a stroke. Also, participants ≤45 years reported always having screen time two hours before sleeping compared to ≥45 years (P = 0.002).
Stress Management and Substance Use
Sex, age, and stroke status-related differences were found with coping strategies. For sex, more females used counseling/psychotherapy (P = 0.017) as a coping strategy compared to males. For age, those ≤45 years used counseling (P=< 0.001), eating too much or too little (P = 0.044), and substance use (P = 0.031) compared to ≥45 years to cope with stress. Whereas participants ≥45 years used spirituality/faith (P = 0.054) as a coping strategy compared to ≤45 years. For stroke status, those who had a stroke used more exercise (P = 0.005) to cope with stress compared to those who did not have a stroke. Age differences were also found with alcohol consumption per week (P = 0.039): those ≥45 years consumed 2-3 drinks/week compared to ≤45 years; and participants ≤45 years consumed four or more drinks/week compared to ≥45 years.
Regression Analysis on Knowledge Level
Multivariable Logistic Regression and Level of Lifestyle-Related Knowledge.
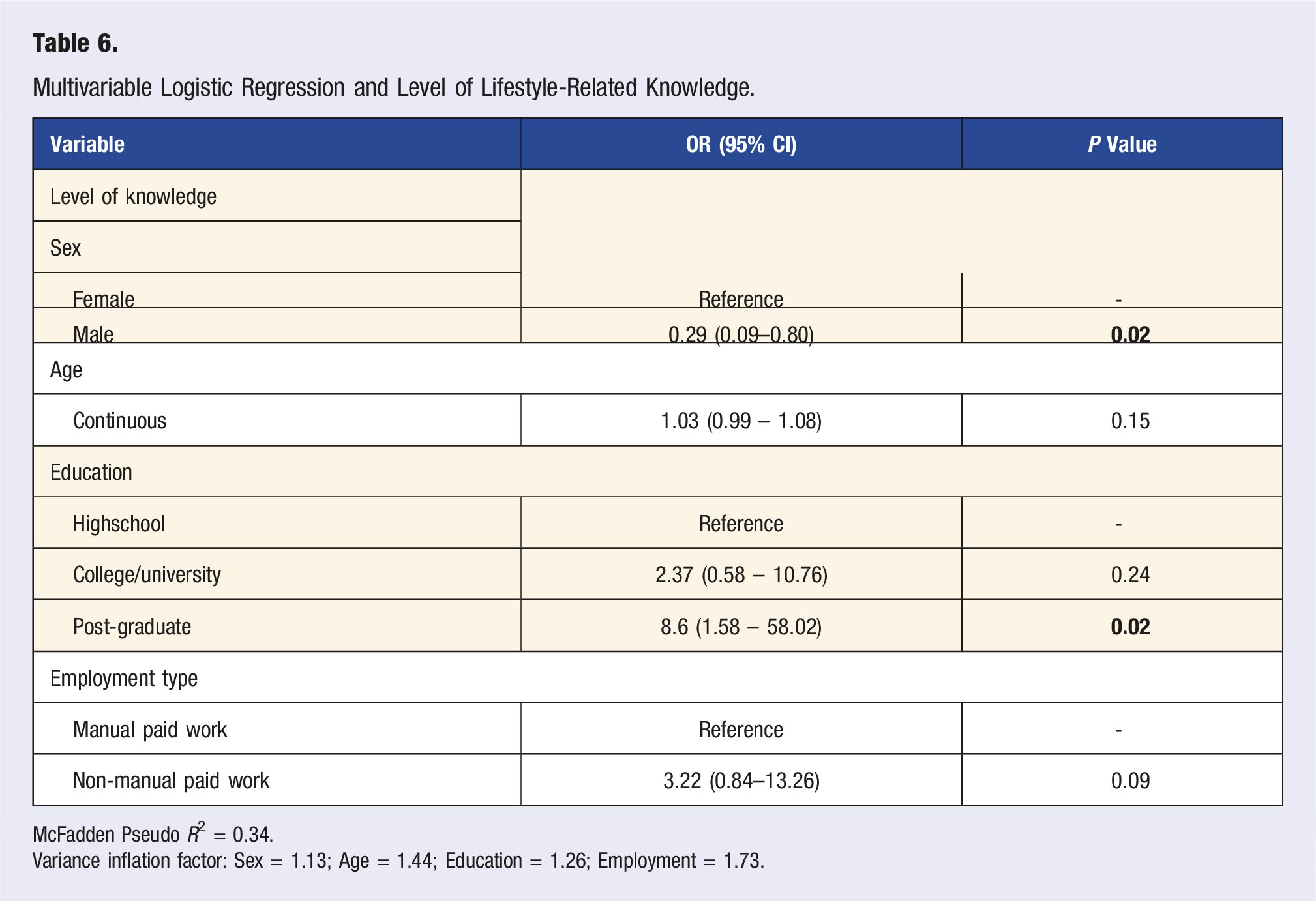
McFadden Pseudo R2 = 0.34.
Variance inflation factor: Sex = 1.13; Age = 1.44; Education = 1.26; Employment = 1.73.
Discussion
Understanding the health-related knowledge and behaviors of younger adult stroke patients is warranted as its adoption and adherence is a greatest challenge. 48 The findings from this study, the first to our knowledge conducted in Canada for this unique patient population, highlight variable levels of lifestyle-related knowledge and the complexity of adopting such behaviors, with apparent and variable facilitators and barriers.
Lifestyle Knowledge
In general, most study participants understood the current recommendations for blood pressure, sleep and alcohol consumption, while only few were aware of nutrition and exercise-related recommendations as the two most impactful lifestyle pillars relevant to stroke prevention. Importantly, the variation in lifestyle-related knowledge is consistent with the general and stroke literature.49-53 As illustrated in a cross-sectional study (N = 411, mean age: 52.4. SD:7.3, range 40-74 years) of Singaporean Chinese, 49 most (88%) participants identified one correct stroke risk factor, however, 20% were unable to name ≥1 established stroke risk factor. 49 Similarly, in a study that was part of a prospective Norwegian Stroke-Paths of Treatment cohort, 52 participant’s (N = 282, mean age: 71.8, 57.1% men) self-reported symptom-related knowledge increased at three months (P < .001) and continued at 12 months post-stroke, however there were variations in participant’s stroke risk factor-related knowledge. 52 This is in parallel with findings from a cross-sectional study of 101 participants in Saudi Arabia (50% ≤ 65 years old, 58.4% men, two thirds overweight or obese), 53 where only 50% of participants correctly identified stroke risk factors; while 67.4% did not think it was important to maintain a healthy weight; 66.3% did not think exercise was important; 47.8% (of those who smoked) did not feel it was important to quit, and in contrary, 63.4% felt it was important to eat healthy. 53 Variability with lifestyle knowledge may help explain the globally emerging evidence of the rising prevalence of stroke among younger adults with attributions to MRFs such as diet and physical inactivity. 54
A potential explanation for the variability in lifestyle-related knowledge could be explained by the public health campaigns55,56 that may be different in various geographic regions and/or interventions with a strong focus on some risk factors (substance use, smoking and hypertension)57-59 and little focus on others (nutrition, sleep, stress, physical activity, and social connectedness). These campaigns, which are delivered through different platforms (e.g., websites, social media, mass media campaigns, mobile applications), are used to reach wider audience in diverse settings (community, workplace, and hospitals, clinics) 60 to enhance knowledge about risk factors, and non-communicable diseases. 61 However, such campaigns are not necessary sustainably geared towards a high-risk population or for patients with prior strokes, and certainly not delivered in consistent form via clinical practice or formal medical education.16,62 Further, as seen in this study, having the knowledge about healthy lifestyle does not necessary translate into practicing such behaviors. 30
Lifestyle Behavior
In this study, we also observed inconsistent levels of healthy lifestyle behaviors among the younger adult stroke participants, although most reported willingness to change their lifestyle. These findings are consistent with the general and stroke-related literature.50,51 For instance, in a cross-sectional study of 333 stroke patients (mean age 62.43, SD: 10.45) in Canada, 51 only 38% (n = 128) had intention to exercise post-discharge with living situation (F = 5.416, P = 0.001), monthly income (F = 49.711, P < 0.001), subjective norm (r = 0.613, P < 0.001), attitude (r = 0.739, P < 0.001) and behavioral control (r = 0.765, P < 0.001) being significant predicators of such intention. 51 Similar findings were found in the National Health and Nutrition Examination Surveys that explored trends of unhealthy lifestyle factors among persons who had a stroke in the United Stated from 1999 to 2018. 50 There was an overall increase in unhealthy lifestyle habits among participants (N = 2017; grouped as 20-44, 45-64 and ≥65 years), with significant increase in alcohol consumption (39.3% (95% Confidence Interval (CI): 29.8, 48.7) to 57.4% (CI: 45.7, 69.0) P = 0.008) and obesity (39.2% (CI: 28.3, 50.2) to 49.4% (CI: 38.9, 59.8) P = 0.029). 50 Of note, participants who were separated, divorced, widowed or unemployed reported overall higher risks of multiple unhealthy lifestyle behaviors. 50 Similarly, the consumption of unhealthy eating habits (e.g., ultra-processed food) is linked with prolonged screen time (e.g., 3 hours/day) 63 and replacing 30 minutes of socializing, streaming or gaming with 30 minutes of physical activity was associated with a lower follow-up Body Mass Index z-score. 64
In this study, we observed some sex and stroke-status related differences, specific to adoption of healthy lifestyle behaviors. Such variances were also noted in chronic disease-related literature. Specific to sex, lack of time due to competing demands of family and domestic responsibilities as well as low energy were found to influence lifestyle changes in women (N = 32, 20-50 years of age) with gestational diabetes mellitus. 65 Similar findings were found in a qualitative study that explored motivations and barriers on healthy lifestyle among middle-aged Iranian women. 66 One of the themes pertained to women’s responsibilities in both the family and society was time for, that interfered with their ability to adopt healthy behaviors despite having the knowledge and motivation to do so. 66 Specific to stroke status, compared to non-stroke patients, stroke patients are also exposed to more lifestyle-related education and interventions as part of post-stroke rehabilitation or discharge programs, which has been found to positively influence their lifestyle knowledge and behaviors (e.g., reducing MRFs such as blood pressure, weight, and cholesterol).67,68
Implications
The study findings have several notable implications. First, it is imperative to integrate LM educational interventions as part of “standard of care” for all patients, and specifically post-stroke. Integrating such interventions as “standard of care” would support the much needed and overdo paradigm shift from reaction to prevention in health care systems.48,69 Such interventions should also account for various barriers that negatively impact healthy lifestyle behavior changes (e.g., time, fear, personal and professional responsibilities) and integrate strategies accordingly (e.g., making exercise or physical movement a family activity). Second, although most of this study population identified as White, it is essential to ensure educational and behavioral interventions are culturally tailored. This is because stroke is a condition of disparities with ethnic, racial, sex, and gender inequities in prevalence, incidence, treatment, health care access and outcomes.70,71 This is further coupled with a decrement in the translation of evidence-based preventive interventions to specific communities and structurally marginalized populations72,73 and this may negatively impact lifestyle-related knowledge and the adoption of healthy behaviors. Third, although not fully explored in this study, it is important to focus on mental-emotional health of younger adults in clinical practice, assessments, and LM interventions as it can impact lifestyle habits (e.g., eating habits and coping strategies) and in turn, the risk of chronic conditions. 74 Finally, the importance for integrating LM prescriptions by physicians and/or nurse practitioners to support and encourage enactment of healthy lifestyle behaviors (e.g., physical activity, healthy eating habits, reducing substance use) 75 among younger adult stroke patients. Simply, informing patients to engage in healthy lifestyle behaviors is often too vague and unhelpful 76 for patients. As such, providing prescriptions that are customized by accounting for the patients’ preferences and circumstances as well as designed using the elements of the SMART (Specific, Measurable, Achievable, Realistic, Timebound) objectives better supports younger adult stroke patients in achieving real, practical and incremental lifestyle changes. 76
Limitations
The study has several limitations. First, this was also a cross-sectional study so no causal interference can be made given that exposure and outcome are measured at the same time. Second, the inclusion criteria were limited to persons who were able to communicate in English. Third, most participants identified as being White and were of higher socioeconomic status (based on their reported income). This may limit our ability to generalize the study findings to other younger adult stroke patients who are unable to communicate in English, are of diverse cultural and ethnic background and lower socioeconomic status who may have varying level of healthy knowledge and behaviors. Fourth, one participant (0.009%) identified as non-binary. As such, a sex analysis was performed to minimize the risk of Type 1 errors with conducting a gender analysis. Fourth, the study was conducted in a single academic health science centre in Toronto, Canada and this may impact the generalizability of the study findings. Finally, self-reported surveys in stroke and identified risk(s) have limitations compared to objective measurements, as they may have risk information. 77
Conclusion
The global burden of stroke and its risk factors landscape has considerably changed. Increasing stroke incidences among younger adults are commonly attributed to MRFs. Abating MRFs can be achieved through, which requires lifestyle-related knowledge and the adoption of positive and healthy behaviors. However, the current lifestyle-related knowledge, behaviors and influencing factors among younger adults is not well understood. Variability in LM-related knowledge (particularly for nutrition and PA) and the adoption of healthy habits was observed in this study with sex, age, and stroke-status related differences. The study findings have implications to clinical practice and the development of fast emerging LM interventions and prescriptions to support the adoption of healthy lifestyle behaviors to support brain health and reduce the risk of stroke and/or its reoccurrence (Figure 2). Graphic abstract of study and findings.
Supplemental Material
Supplemental Material - Lifestyle Knowledge and Behavior Among Stroke and High-Risk Younger Adult Patients Through Sex, Age and Stroke Status Differences: A Cross-Sectional Study
Supplemental Material for Lifestyle Knowledge and Behavior Among Stroke and High-Risk Younger Adult Patients Through Sex, Age and Stroke Status Differences: A Cross-Sectional Study by Sarah Ibrahim, Jasper R. Senff, Troy Francis, Aleksandra Stanimirovic, Sharon Ng, Lindsey Zhang, Akshaya Ravi, Leanne K. Casaubon, Keithan Sivakumar, Joanathan Rosand, Sanjula, Singh, Valeria E. Rac, and Aleksandra Pikula in American Journal of Lifestyle Medicine.
Footnotes
Author’s Note
The senior author receives support from the Jay and Sari Sonshine Chair in Stroke Prevention and Cerebrovascular Disease at University of Toronto/University Health Network.
Acknowledgments
We would like to thank all the participants that took part in the study and Mrs. Shoba Singh for assisting with the participant recruitment process. Further, we would like to also thank Dr Joanna D. Schaafsma for helping us in high-risk patient recruitment from the Neurovascular Clinic at the University Health Network, Toronto.
Author Contributions
SI, JRS, and TF led the data analysis and preparation of the manuscript. VR led and advised on all components of the study methods, interpretation of study findings, and reviewed and approved the manuscript. SN and LZ contributed to the data collection and reviewed and approved the manuscript. AP secured the funding, supervised the study conception and design, data collection, interpretation of the study findings, manuscript preparation, and reviewed and approved of the manuscript. All authors contributed to the overall study design as well as reviewed and approved of the manuscript.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the University of Toronto Division of Neurology (The Slamen-Fast New Initiatives in Neurology).
Ethical Statement
Data Availability Statement
Available upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.