
Abstract
Background:
The Complete Health Improvement Program (CHIP) is effective in improving cardiovascular disease risk via the original live recorded DVD (DIS) and a revised studio recorded video versions (VIS), both presented in-person synchronously. The studio version was also presented in-person asynchronously (VIA) and virtually asynchronously (VVA).
Objective:
Assess the comparative effectiveness of four delivery methods of CHIP.
Methods:
Participants had biomarkers measured at baseline and after the 11th session: blood pressure (SBP, DBP), body mass index (BMI), fasting blood glucose (FBG), and lipid panel (TC, TG, LDL-c, HDL-c). ANCOVA was utilized to evaluate the interaction over time by group.
Results:
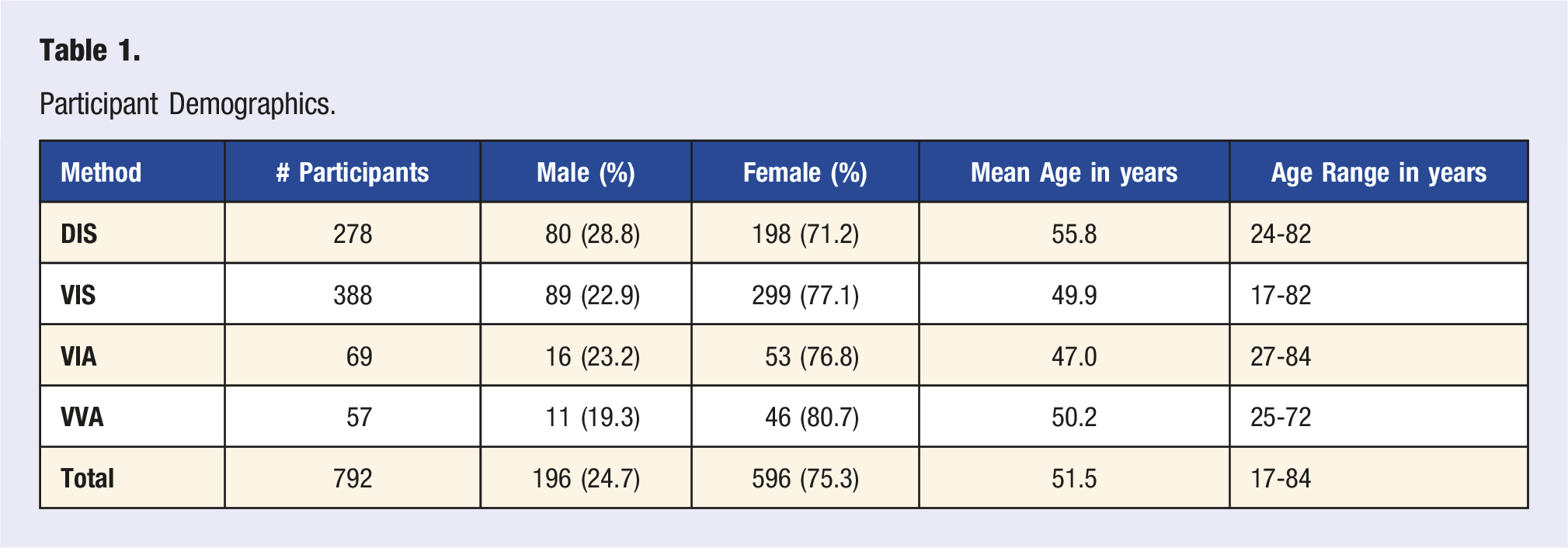
Of 792 participants, the majority female in all groups (71.2-80.7%), mean age ranged 47.0–55.8 years. All methods showed significant changes in all biomarkers measured over time except for TG and SBP in VIA, TG in VVA and DBP in VIS. The time by delivery method interaction was significant for HDL-c (F value = 6.33, P = .0003), BMI (F value = 4.04, P = .007), systolic BP (F value = 4.33, P = .004). DIS was most effective in reducing HDL-c, BMI and systolic BP.
Conclusion:
While all four methods yielded significant changes in biomarkers, the in-person, synchronous delivery method produced the largest improvements.
Keywords
“A preponderance of evidence exists in the scientific literature showing the efficacy of the Complete Health Improvement Program (CHIP) in improving biomarkers relevant to lifestyle-related chronic diseases.”
Introduction
Approximately six in ten adults in the United States have at least one chronic disease including heart disease, cancer, lung disease, stroke, diabetes, Alzheimer’s disease, and kidney disease. 1 Several therapeutic lifestyle modification programs (TLMPs) show positive effects on chronic disease status, including lowering cardiovascular risk,2-7 improving mental health,8,9 controlling body weight9,10 and lowering mortality from kidney disease. 11 In the age of COVID-19, many programs needed to alter the method of delivery to accommodate governmental regulations and CDC recommendations. TLMPs delivered online were already successful at reducing the HbA1c biomarker to below pre-diabetes level,12,13 and promoting greater weight loss compared to traditional face-to-face programs.14,15 There are practical benefits of online content delivery, including increased convenience and access.
Content delivery models and efficacy of online learning have been examined over time, but little is known specific to online learning and TLMPs. This study compares the effectiveness of different methods of delivery of a well-established TLMP, The Complete Health Improvement Program (CHIP). The original live recorded version of CHIP (DIS) and a revised studio recorded version (VIS) were initially both presented in an in-person synchronous (all participants viewing at the same time) class setting. The studio recorded version more recently has also been presented in an in-person asynchronous (participants viewing at their own selected time) (VIA), and virtual asynchronous (VVA) method.
Live online content delivery, or synchronous learning, provides immediate content feedback, support of social processes, and interaction amongst the group. Evidence shows positive associations between health outcomes and social support. 16 Synchronous delivery poses some implementation challenges including scheduling, acquiring classroom space, audio-visual equipment and technology support to address live technical issues, travel time, and locating skilled facilitators. Such challenges contribute to the cost of program delivery and can constrain class size as well as frequency of program delivery.17-24
Asynchronous, online content delivery allows learners to view material at their own selected time, and review materials in a repeated manner for a longer duration allowing more time to reflect on content. This mode of delivery is ideal for content that is constant or permanent. Drawbacks noted in the literature include misinterpretation of content, and lack of spontaneous interaction and immediate feedback which can translate into procrastination, reduced performance, and low engagement.
As the field of lifestyle medicine continues its rapid expansion, and the pandemic reshapes our culture, there is an anticipated increase in the number of online TLMPs. This study seeks to contribute to the discussion regarding effective approaches to TLMP content delivery.
Methods
CHIP participants were asked to consent to use of their de-identified data, aggregated for analytical purposes. Nonconsenting individuals for this data collection were still eligible to participate in CHIP but were excluded from this study. Approval was obtained from the Ohio University Institutional Review Board (16-X-44) and registered with ClinicalTrials.gov (NCT03025451).
CHIP Intervention
CHIP has been utilized in clinics and communities for over 25 years to empower participants to choose healthy lifestyle habits to prevent, arrest, and reverse chronic lifestyle-related disease. Over the years, the program has undergone modifications in methods of delivery (described below); however, the core concepts have remained the same. 9 Prerecorded videos and live activities have been used for instruction, consisting of discussions, physical exercise, and cooking demonstrations.9,10 Participants were instructed to follow a minimally processed, predominantly plant-based, whole foods diet, focused on consumption of vegetables, fruits, cooked whole grains, legumes and limited nuts and seeds. Daily dietary objectives of CHIP were fat less than 20% of calories, less than 10 teaspoons of added sugar, less than 2000 mg of added salt, cholesterol less than 50 mg, and 35-40 g of fiber. 10 CHIP also promoted at least 30 minutes of moderate physical activity or 10,000 steps daily. Strength training exercises with a duration of 20-30 minutes, 2-3 days a week were also advised. 10
Data Collection
Retrospective data were evaluated from consenting CHIP participants in 37 CHIP classes, provided by Live Healthy Appalachia, a local nonprofit organization in Athens, Ohio, which promotes healthy eating and active lifestyles in the region. These classes were delivered in 16-18 sessions over 2 to 4 months, from 2011-2021.
At the beginning of the course, and again after the 11th session, fasting venous blood samples were collected and analyzed for total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-c), high-density lipoprotein cholesterol (HDL-c) and fasting blood glucose (FBG) with CLIA-waived analyzers. For participants in Athens, this was generally done at the local hospital. For remote virtual participants, data was self-reported, having been obtained from a medical facility of their choice, or was collected in a corporate setting and results provided to Live Healthy Appalachia. Body mass index (BMI), and blood pressure (BP) were recorded or self-reported near the time of the blood draws. Data was stored in a password-encrypted database located at Live Healthy Appalachia.
Delivery Methods
Four methods of delivery were utilized: • • • •
Data Analysis
Descriptive statistics were performed to describe and summarize the data. The corresponding frequency, percent distribution, mean and standard deviation were reported (Table 2). Bivariate analysis was performed. A P value < .05 was considered statistically significant.
To account for baseline differences between groups, ANCOVA using general linear model approach was performed with a within subject’s factor time and between subject’s factor group to evaluate the interaction of time by group. Adjustments were also made for age and gender. Such an analysis allows for the dynamic or autoregressive nature of the data and overcomes limitations in the assumptions underlying the univariate models. All analyses were conducted using SAS 9.4.
Results
Participant Demographics.
Mean (±standard deviation) change in study variables across time among the study groups. Column 5 demonstrates the P value of variable change within the delivery method.
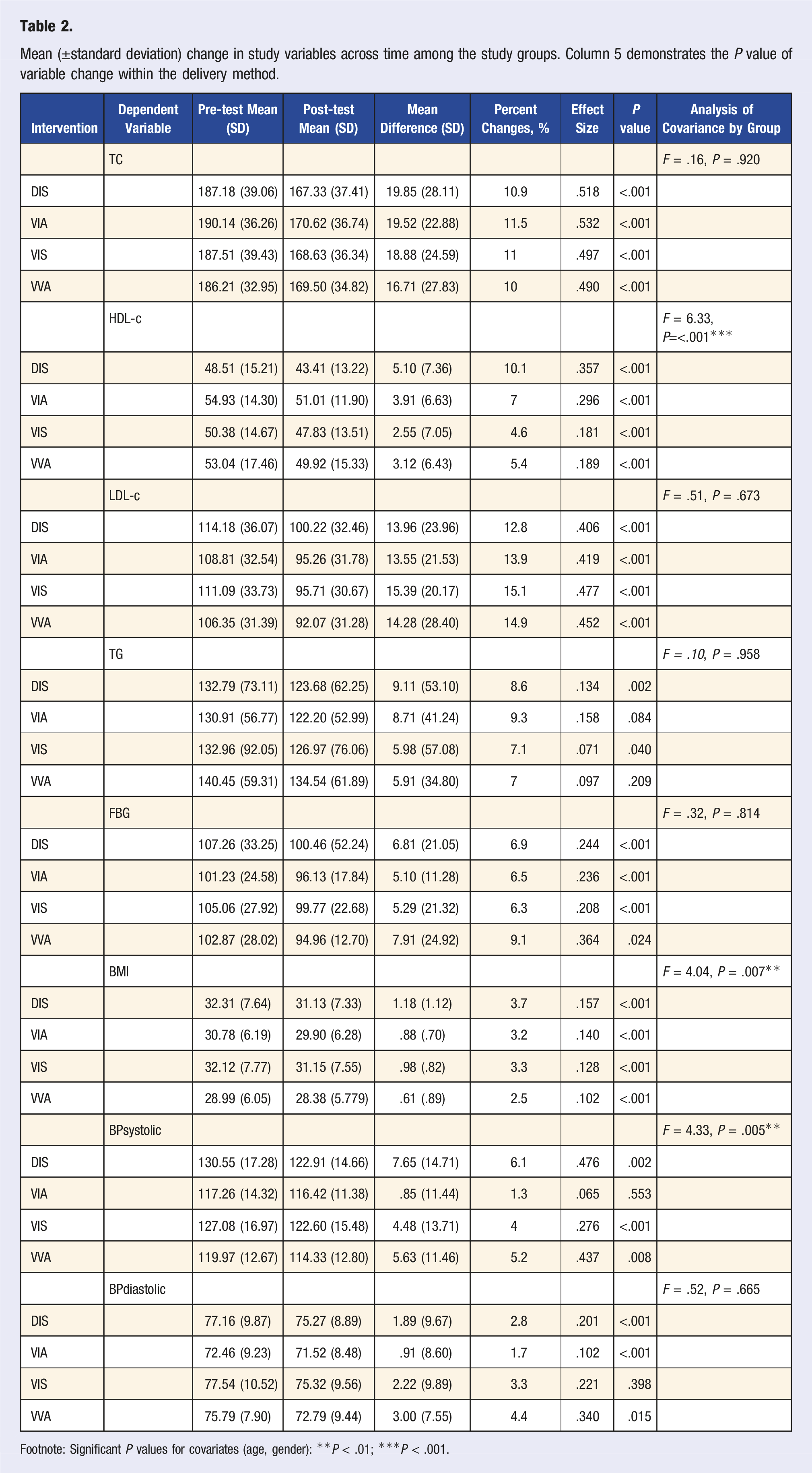
Footnote: Significant P values for covariates (age, gender): **P < .01; ***P < .001.
Statistical analysis showed that the time by method interaction was not significant for TC (F value = .16, P = .920), LDL-c (F value = .51, P = .672), TG (F value = .10, P = .957), FBG (F value = .32, P = .813), nor DBP (F value = .52, P = .665) indicating that there was no statistically significant difference between methods on the values of these parameters in the participants across the two time periods. There was significant change in these parameters over time, but "group/method" didn’t matter. All program delivery methods yielded statistically significant results (Table 2).
The time by delivery method interaction was significant (F value = 6.33, P = .0003) for HDL-c indicating that there was significant difference in methods on participants HDL-c across the two time periods. The mean adjusted HDL-c reduced by 6.9% in VIA, by 4.6% in VIS, by 5.4% in VVA, and by 10.1% in DIS. There was a significant change in HDL-c over time across all four groups. DIS was most effective in reducing HDL-c.
There was a statistically significant difference between the delivery methods on participants BMI across the two time periods (F value = 4.04, P = .007). The mean adjusted BMI reduced by 3.2% in VIA, by 3.3% in VIS, by 2.5% in VVA, and by 3.7% in DIS. There was a significant change in BMI over time across all three groups. DIS was most effective in reducing BMI.
The time by delivery method interaction was significant (F value = 4.33, P = .004) for systolic BP indicating that there was significant difference in methods on participants systolic BP across the two time periods. The mean adjusted systolic BP reduced by 1.3% in VIA, by 4% in VIS, by 5.2% in VVA, and by 6.1% in DIS. There was a significant change in systolic BP over time across all three groups. DIS was most effective in reducing systolic BP.
Discussion
A preponderance of evidence exists in the scientific literature showing the efficacy of the Complete Health Improvement Program (CHIP) in improving biomarkers relevant to lifestyle-related chronic diseases. This study examines four content delivery methods of CHIP with the aim to identify which delivery method induces the greatest effects in related biomarkers. Participants in each group were self-selecting volunteers. Eight outcome variables were analyzed from each delivery method. All four delivery methods yielded statistically significant improvements in most biomarkers evaluated; however, DIS was significantly more effective in reducing SBP, BMI and HDL-c as compared to the other three delivery methods.
Why did the DIS method perform better in reducing several biomarkers? Live in-person content delivery provides immediate feedback, support of social processes and interaction amongst the group. The DIS content delivery method further speaks to existing knowledge regarding the positive associations between health outcomes and social support. Participants who chose to participate in an in-person program may have been more motivated to change compared to participants who chose a more convenient (e.g., no travel requirement to intervention) program delivery method. This may account for the variation in biomarker outcomes seen between the different content delivery groups. Other delivery methods evaluated lacked the same level of in-person engagement, and the ability to “check-out” (e.g., turn off video camera, engage with distractions) during the intervention.
The uniqueness of this method may have been in presenting Dr. Hans Diehl, the founder and developer of CHIP, filmed in front of a live audience. His interaction with the audience and the camera frequently panning the audience showing intent faces, nodding heads, and laughing at Dr. Diehl’s quips, may play a role in the appeal. This appeal may have been especially powerful for an audience that is skewed toward the geriatric age range, having grown up with television programs filmed in front of a live audience. In addition to this, DIS, though not uniquely so, had the added layer of watching the presentation as a group and providing time as a group to discuss and process the content material.
The benefits associated with synchronous live learning include behavior modeling: observing and imitating others and self-evaluation of behaviors against instructors. 20 Immediate feedback in the form of praise, the attention of others and two-way communication, and learners taking on a participatory role play a key role in cognitive learning and behavior change.25-27 Factors such as extrinsic and intrinsic motivation, influence participation level, uptake of program materials, and outcomes. 18 If extrinsic motivation is present, synchronous program delivery may garner the greatest level of participation. 28 Future studies may consider including participant screening questions to inform on which factors are present before choosing a delivery method.
COVID-19 has driven a dramatic change in society, creating increased isolation and increased reliance on online technology for social interaction and education. It is still early to determine all the positives and negatives of these changes. CHIP was positioned to address these changes without too much difficulty, already having a virtual option in place. It is difficult to adjust for all variables related to COVID, but CHIP, in whatever method delivered, appeared to consistently produce positive changes in multiple biometrics.
Limitations
The findings expressed in this study derive from a population sample which is predominantly female. Although many studies involving TLMPs have a similar sample population,8-10 generalization of study findings beyond the described demographic segment should be considered with caution. This study is non-randomized, consisting of self-selected participants with various incentives to participate, including corporate incentive in some cases. This limits the generalizability of these findings. CHIP as a program, evolved throughout the time studied, which may cloud some of the comparisons, and consisted of subcategories of delivery methods and populations which were not individually stratified for this analysis. It is also difficult to account for the impact of the COVID pandemic on participant engagement and results. There was no measurement of “attendance” either viewing the videos asynchronously, nor of attendance in person. Some of the data utilized was self-reported, which would generally amplify the effect (favor more favorable responses). Participants could have reported false information out of embarrassment, or from some other motivation. The second data collection occurred after the 11th session, which depending on the class, could have been as little as 3 weeks after onset of intervention, or up to 12 weeks. This could affect the magnitude of change. No account was taken of change in medication, which could affect the magnitude of change in results.
Conclusion
CHIP was effective in producing improvements in multiple lifestyle-related chronic disease risk factors in all four delivery methods; however, DIS was significantly more effective in reducing SBP, BMI, and HDL-c as compared to the other three methods.
Further study to determine which method best serves participants’ individual learning styles would be helpful in finding optimal personal success.
Footnotes
Author’s Note
All communications regarding manuscript and reprint requests should be directed to David Drozek.
Acknowledgments
Live Healthy Appalachia, the regional administrator of CHIP provided administrative support and access to participant data. Janet Simon, PhD, Ohio University, reviewed the statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.