
Abstract
Background. Doctors have a special role in helping patients make lifestyle changes, and they are more credible and effective if they are role models. Yet few medical schools have incorporated lifestyle medicine into their curricula. We ascertained the influence of a lifestyle medicine curriculum during the first year of medical school. Methods. The curriculum, involving 140 students, consisted of one intensive day at medical school entry and 16 hours of teaching 8 months later. It addressed students’ own lifestyle choices and topics related to lifestyle medicine. A survey was delivered at the beginning and end of the academic year. Results. A total of 114 students completed the first survey and 64 the second. They rated the course highly for personal and professional value. At baseline, students exhibited lifestyle behaviors typical for young adults and showed an appreciation of the physician’s role in lifestyle change. However, over time they showed a significant reduction in quality of lifestyle, with increased stress, weight gain, and fast food consumption and less exercise. Conclusions. Although lifestyle medicine knowledge is valued by medical students, a 24-hour intensive lifestyle medicine curriculum delivered over 3 days appears to be ineffective in preventing worsening lifestyle behaviors over the course of the year. This is especially concerning as physicians are unlikely to provide effective guidance if they cannot sustain healthy behaviors themselves.
Keywords
‘The health behavior of medical students is crucially important not only for their own health but also for their future patients’ health.’
The greatest challenge of medicine at the beginning of the third millennium is dealing with the epidemic of chronic diseases that are caused or exacerbated by poor-quality lifestyle. The costs to society and health systems are increasing. The World Health Organization predicts that by 2020 two thirds of all diseases worldwide will be the result of unhealthy lifestyle. 1 Guidelines call uniformly for lifestyle change as the first line of therapy for prevention and treatment of chronic diseases.2,3 However, in practice physicians often fail to counsel patients about healthy behaviors. 4 The need to include lifestyle medicine teaching in undergraduate medical education is evident, yet remains a neglected area in most medical schools.5,6
The health behavior of medical students is crucially important not only for their own health but also for their future patients’ health. Research shows that healthier personal practice during medical school positively predicts physicians’ preventive counselling practices.7-9 An association has been found between physicians’ health practices and their ability to influence their patients’ lifestyle behaviors.10-12
While students appear to exhibit typical lifestyle behaviors for young adults on entering medical school in the United States, 13 these are not necessarily optimal for future health, and the heavy burden of academic requirements and high levels of stress adversely affect students’ health behaviors and status 14 further. The need for medical schools to promote student wellness is clear, yet in reality there are few initiatives aimed at encouraging healthy lifestyle behaviors.9,15,16
The Bar Ilan Medical School, established in 2011, was located in the north of Israel to promote the health status of this peripheral and disadvantaged region of the country. An emphasis has been laid on the health habits of medical students, with the aspiration that over time this would contribute to a positive wave of change toward better health for the surrounding population. To this end, a personal lifestyle behavior program was incorporated into the Public Health course, which is delivered on entry into medical school. Toward the end of the first year, teaching on lifestyle medicine is given to introduce students to their professional role and responsibilities in this area.
We studied the influence of the lifestyle curriculum on our students through a survey conducted during the first week of medical school and at the end of the first preclinical year. Our intention was to document students’ health behaviors as well as their attitudes toward the role of the medical profession in the delivery of lifestyle medicine.
Methods
Lifestyle Curriculum
An intensive lifestyle day (8 hours) is delivered within the framework of the required 3-week public health course, the first course students receive on starting medical school. The aim is to expose students to the importance of health behaviors in health and disease, the importance of lifestyle for their own health and well-being, and to encourage them to develop healthier behaviors. The formal lectures included an introduction to healthy lifestyle, exercise, nutrition and healthy eating, stress and emotional well-being, and motivation for lifestyle change. Each lecture is followed by practical and interactive exercises, including a healthy cooking demonstration, aerobic and anaerobic physical activity, and a yoga class. All sessions provide practical tools to encourage lifestyle changes for personal and professional use.
Lifestyle medicine teaching is incorporated toward the end of the first year in the bioenergetics course, which covers different aspects of chronic diseases. In this component of the lifestyle curriculum, the relevance of lifestyle behaviors to health and disease and the central role of the medical profession are addressed. The 2-day program includes more in-depth knowledge of nutrition (4 hours), sports medicine (4 hours), motivational interviewing (4 hours), smoking (2 hours), and sleep medicine (2 hours).
Study Population
All medical students enrolled in 2012 and 2013 at Bar Ilan University Faculty of Medicine. The program is a 4-year graduate program with students commencing following a first degree and 3 years compulsory military service.
Outcome Measures
An anonymized survey was administered during the first week of medical studies and again 8 months later at the end of the lifestyle medicine teaching sessions. Students were questioned on demographic data, perceived health status, body weight, stress levels, and personal health behaviors including smoking, exercise, sleep, and diet. The survey was a composite of the Israeli Ministry of Health National Survey of Knowledge, Attitude and Practices (KAP) 2011 17 with further questions relating to diet and eating behaviors adapted from the UK HENRY obesity prevention program. 18 Attitudes toward physicians’ role in relation to lifestyle medicine were ascertained using 3 items. These were selected from a validated instrument developed to assess physicians’ attitudes to lifestyle counseling. 19 The 3 items focused on the perceived role of the physician. Items in this scale are ranked on a Likert-type scale from 1 = strongly disagree to 4 = strongly agree.
Students also completed an online questionnaire at the end of the Public Health course, evaluating the intensive lifestyle day, using a Likert-type scale of 1 to 5, anchored with descriptors. They were given space to freely comment on the course.
Data Analysis
Initial checks compared participants who completed questionnaires at both time points with those who only completed the baseline measure. Continuous variables were tested using independent groups t tests, and categorical variables using χ2 or Mann-Whitney U tests, as appropriate.
Changes in continuous outcomes (eg, dietary consumption, frequency of physical activity) were analyzed using repeated measures t tests. Due to the level of data provided, changes in perceived weight and health status, eating habits, and sleep quality were analyzed using the nonparametric paired-sample Wilcoxon signed rank test. Change in smoking status was analyzed using McNemar’s test for paired nominal-level data.
Results
A total of 140 students were enrolled in the medical school between 2012 and 2013, of whom 114 completed the surveys on entry and 64 eight months later. Mean age was 27 years (SD 3.4); 54 were male and 60 female; 22 were immigrants; 111 were Jewish, 3 Arab; 42 were married of whom 11 had children.
Students who provided data at both time points did not substantially differ from those who only completed the first measure. The groups were comparable in terms of gender, age, weight (reported weight and perceived weight status), body mass index (BMI), lifestyle, and perceived health and stress level (all P > .05).
Medical Students’ Perceptions of Health and Reported Health Behaviors on Entry to Medical School
Medical students’ perceptions of their health status and their reported health behaviors are shown in Table 1. At the start of medical school they perceived their health to be good, and the mean BMI was in the healthy range. Almost 1 in 5 reported smoking but only one student smoked more than 10 cigarettes daily; alcohol consumption was low. Using consumption of vegetables and sweet drink consumption as markers of diet, their nutrition was satisfactory, and most students engaged in physical activity regularly. Stress levels were moderate and they slept on average 6 to 7 hours each night, with reasonable quality sleep.
Medical Student Lifestyle Behaviors on Entry to Medical School and Their Attitudes to Lifestyle Medicine (n = 114).
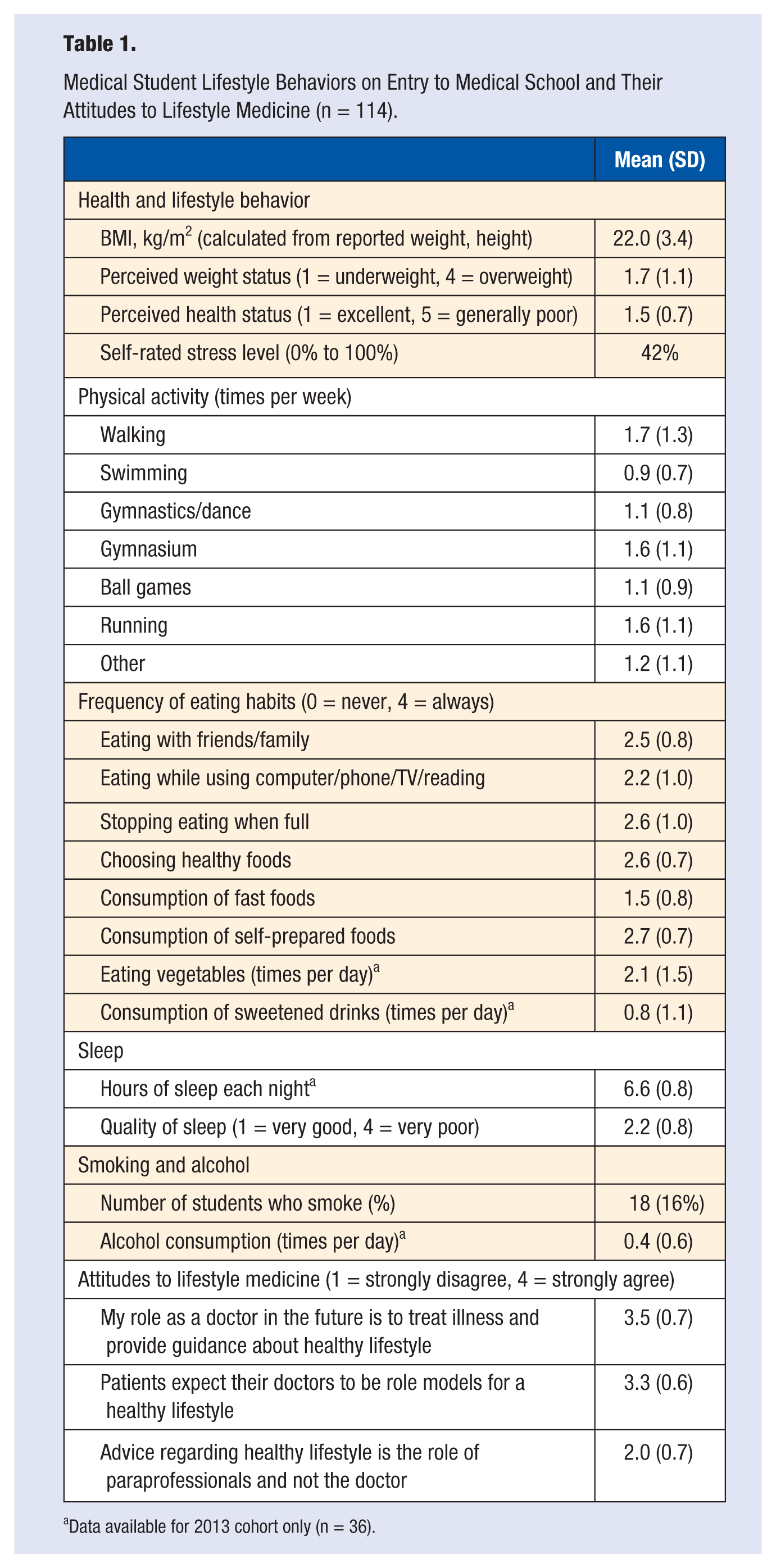
Data available for 2013 cohort only (n = 36).
Students’ Views Regarding the Lifestyle Curriculum
All 114 students participated in the lifestyle day over the 2 academic years. Students rated the lifestyle day highly and found it valuable (see Figure 1). They saw the day as being of professional (4.0 ± 1) and personal value (4.1 ± 1). Overall, it was ranked as a positive learning experience (4.2 ± 0.9), and rated higher than the public health course overall. Comments indicated that the session was excellent and should be extended in length and breadth. They also noted that the combination of lectures with practical experience was enriching and fascinating and gave motivation to put into practice what was learned.
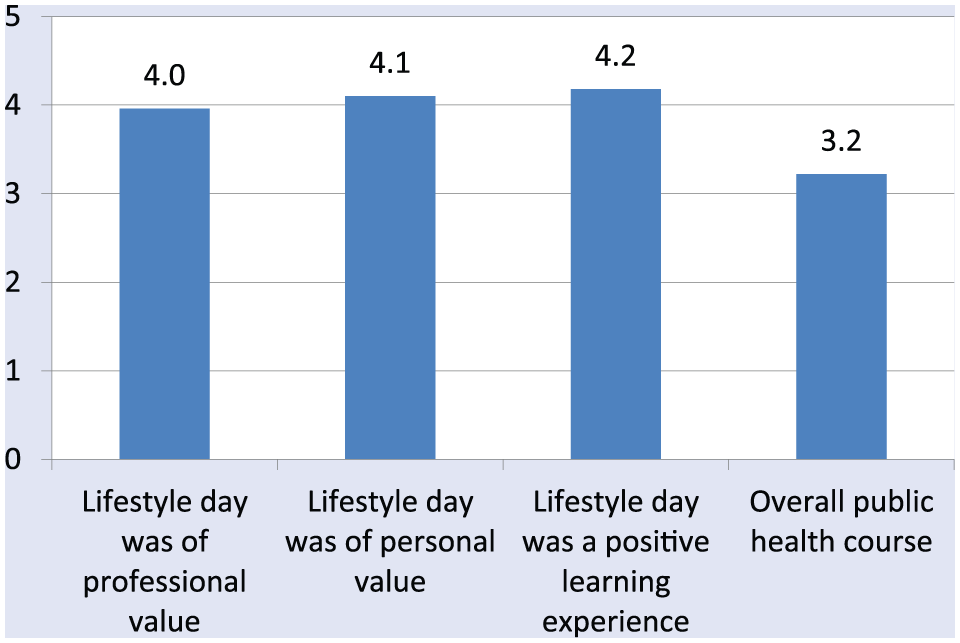
Students’ perceptions regarding the lifestyle day*.
Change in Health Behaviors Over the First Year of Medical School
Sixty-four of the 114 students (56%) completed the survey again 8 months later at the end of the lifestyle teaching curriculum; 28 were from the 2012 cohort and 36 from the 2013 cohort. Students who failed to complete the second survey (n = 50) did not differ at baseline in terms of age, gender, reported weight/BMI, perceived health and stress levels, smoking, exercise, eating habits, or dietary intake.
As shown in Table 2, there was a significant increase in self-reported weight (and hence BMI) with a mean gain of 1 kg. Perceptions of weight status did not change, but there was significant deterioration in perceived overall health status. Self-reported stress levels were also significantly higher at follow-up, with reduction in the use of exercise in response to stress.
Change in Medical Student Weight and Health Status During Their First Year at Medical School (n = 64).
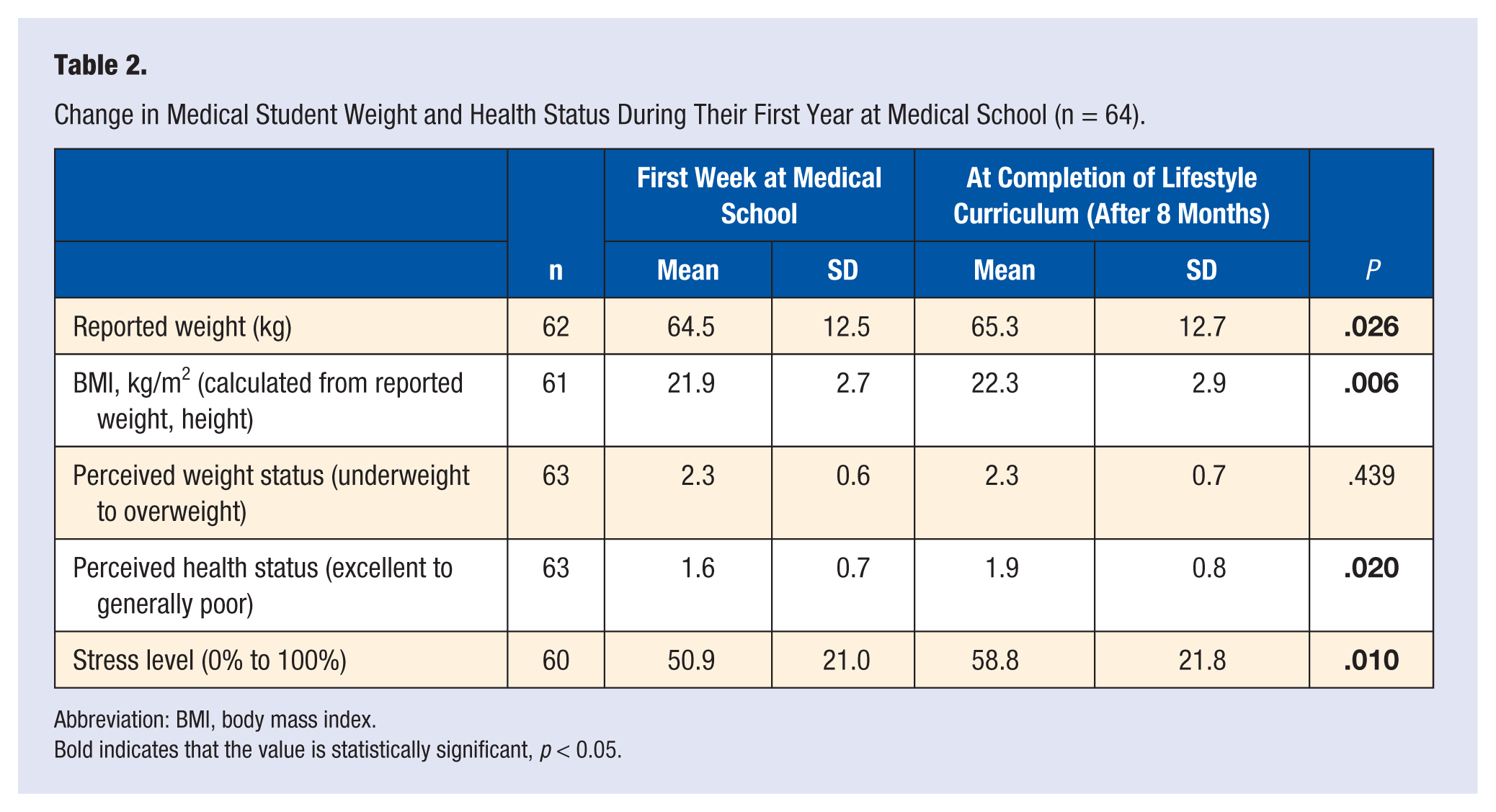
Abbreviation: BMI, body mass index.
Bold indicates that the value is statistically significant, p < 0.05.
More detailed analyses of health behaviors are shown in Table 3. A significant reduction was found in all forms of physical activity except for walking. When asked about the support they would find helpful to increase their physical activity (data not shown in table), 35 responded at baseline that group activities would be helpful but only 14 felt this was a good idea later (P = .001). Eating habits changed little over time except for reported consumption of fast foods, which increased significantly (P = .041). Questions relating to sleep and smoking were only introduced for the second cohort. Students showed no change in quantity or quality of sleep. Smoking and alcohol consumption also showed no change.
Change in Reported Health and Lifestyle Behaviors Following 8 Months at Medical School and After Completion of the Lifestyle Medicine Curriculum.
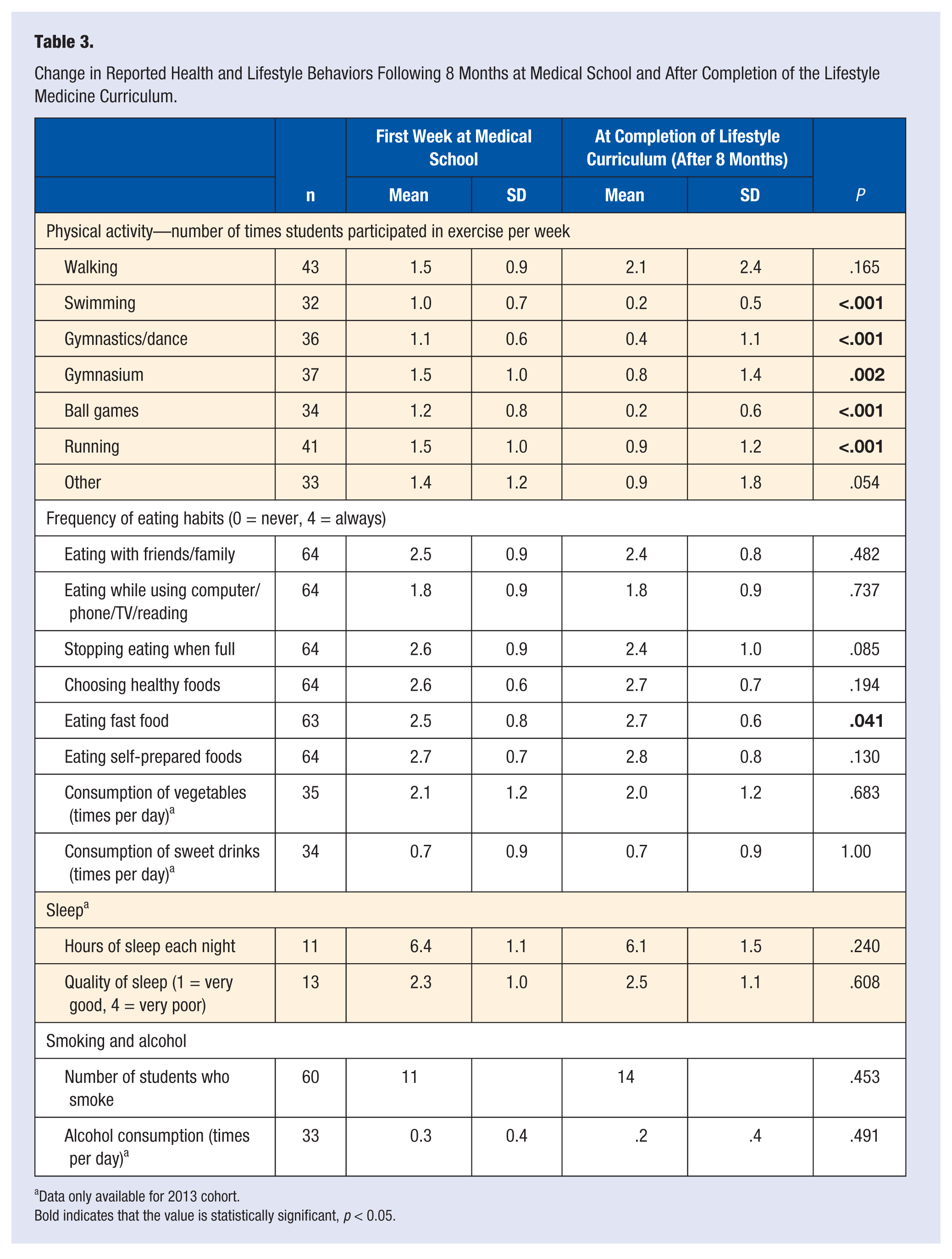
Data only available for 2013 cohort.
Bold indicates that the value is statistically significant, p < 0.05.
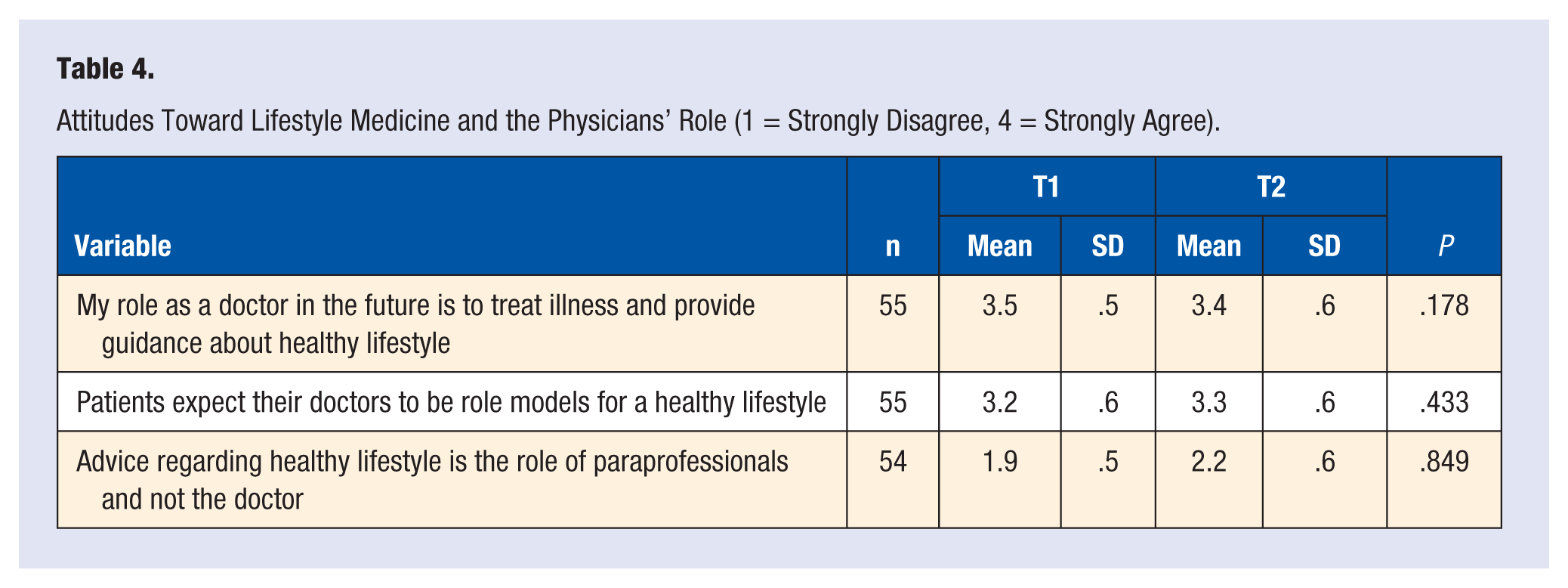
On questioning students regarding the role of the doctor in lifestyle medicine, there was little change, with most continuing to see that they had a role as providing guidance to patients and that this area was not only the role of paraprofessionals (see Table 4).
Attitudes Toward Lifestyle Medicine and the Physicians’ Role (1 = Strongly Disagree, 4 = Strongly Agree).
Discussion
In light of the recognition that doctors have a significant role in the prevention and management of lifestyle-related diseases, we introduced a lifestyle curriculum into the first year of medical studies, based on our successful experience of training family physicians. 20 The program consisted of 24 hours of teaching delivered in 2 concentrated blocks—as much as could be negotiated into an already stretched and demanding curriculum. We determined to ascertain students’ views regarding the program and to see if it affected their health and lifestyle over the course of the following year. We hoped that the program would reinforce healthy behaviors and help them realize the importance of role modeling these behaviors in their career as physicians.
While the lifestyle curriculum amounted to only a relatively small proportion of their preclinical studies, survey of the literature indicates that lifestyle medicine receives more attention in our medical school than the subject is given elsewhere.5,6,15,16 We were gratified that the students received the program well, and their comments indicated that they took the subject seriously and were intending to lobby for healthier opportunities within their student union and the medical school itself. The results of our survey of health behaviors toward the end of the first year of medical training were therefore disappointing to say the least.
On entry to medical school, students’ lifestyle was satisfactory in terms of weight, stress levels, and perceived health and was comparable to medical students in the United States 13 and other individuals of their age in Israel. 20 Most reported participating in active sport at least once per week, their daily vegetables consumption was adequate, and consumption of sweet drinks was moderate. While they commonly ate fast foods, they also prepared home-cooked food for themselves. They appeared to be a population who would be receptive to the lifestyle curriculum, especially as they saw the relevance of lifestyle as part of the doctor’s role in caring for patients.
However, after only 8 months of medical school, their lifestyle had deteriorated considerably. They reported an increase in weight, poorer health, increased stress, and a reduction in exercise to counter stress. They changed from being active to reducing their physical activity across a range of activities. Their consumption of fast foods increased (although eating habits appeared to change little in other ways). As they are mature students, this change cannot be explained by a move from sheltered home life. While reports on this sort of deterioration over the course of medical studies is not new, 14 our findings indicate that greater efforts are needed to reduce the stress and burden of medical studies, provide a healthier medical school environment, and incorporate lifestyle medicine more effectively into the medical curriculum. Medical schools must take responsibility to consider ways to reduce stress and support students to cope with it, especially as stress is likely to be inherent in the study of medicine.
Changing lifestyle behaviors is difficult and requires time and continued efforts. Our results suggest that more substantial resources and time need to be allocated to lifestyle medicine. A more effective way may be to incorporate it into the entire medical curriculum, across both the preclinical and clinical years. Individual help for students is also a necessary component. We are presently seeking resources to design an integrated curriculum that provides students with the competences doctors require to effectively deliver lifestyle medicine.
There are limitations to our study. The lifestyle program amounted to only a limited proportion of the medical curriculum; with a “single dose” addressing their own lifestyle at the start of their studies followed by 2 days of academic study relating to lifestyle medicine. We were perhaps naïve to imagine that, however well received, it could counteract the well-acknowledged burden of medical studies. The response rate to the second survey was less than 60%, although we saw this as something of an achievement given the students’ weariness of teaching satisfaction surveys to which they are often subjected. The finding that responders did not differ from nonresponders in their personal characteristics and lifestyle behaviors provides some reassurance that our findings have validity.
Tackling the issue of lifestyle goes beyond the health and well-being of medical students. Health behaviors during medical school are important as they predict physicians’ later preventive counselling practices.7-9 There is also evidence that physicians who lead healthier lifestyles are more able to influence their patients’ lifestyle behaviors for the good.10-12 Appropriate investment in the medical school years and instilling “healthy” policies into the medical school environment are essential to maximize the chances of overcoming the epidemic of lifestyle-related diseases, which is dominating health across the world. No doubt this requires inclusion through a longitudinal curriculum with frequent “touch points” emphasizing the importance of personal health behaviors and professional skills in supporting lifestyle change. Given the inevitability of stress during medical studies, medical schools must also take responsibility to help students cope with their stress, as well as focusing on how to help future patients.
Footnotes
Acknowledgements
The authors thank Unilever for financially supporting the cooking demonstration part of the lifestyle course.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This research protocol was approved by the Ohio University Institutional Research Board.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.