
Abstract
Digital Lifestyle Medicine (DLM) is a consumer-centric model of care which elevates the importance of daily behaviors in preventing and reversing chronic disease using virtual and digital modalities to reach patients in the context where lifestyle behaviors occur and empower them to stay well. DLM is health care reimagined, designed to inspire patients to live their best life by enabling skill-building, self-efficacy, and sustainable behavior change supported by peers, scientific-evidence, and a multidisciplinary team of lifestyle medicine (LM) clinicians. Importantly, it requires insights and collaboration from healthcare experts and technology entrepreneurs to provide a profoundly different “user experience” layered with context, relevance, and scalability. Using examples from our DLM practice, we describe how key components of LM practice, including a multidisciplinary care team, behavior change support, health coaching, and peer support, are prime for digital delivery. We conclude by providing preliminary patient outcomes to date, key success factors, and opportunities for enhancement and expansion to inform the adoption and successful implementation of DLM across the collective of LM practice.
Keywords
Digital Lifestyle Medicine offers a path to supporting health
Introduction
Lifestyle medicine (LM) is a top emerging field of medicine. 1 As lifestyle-centered care is practiced more broadly, might we look toward an era of greater prevention, management, and reversal of chronic disease? However, to reach the nearly 80% percent of the US population who have chronic metabolic disease, 2 tremendous scale of LM is needed to bend the curve of disease burden and the corresponding unsustainable healthcare costs. New models of care are required to meet this urgent demand.
Leveraging virtual and digital modalities enables care transformation to a more efficient, effective, and consumer-focused model while reducing barriers to access. Of particular importance to LM is the ongoing engagement with a multidisciplinary team to support significant lifestyle change. Digital engagement makes LM relevant and effective for patients by bringing it into the context where lifestyle changes are made, in the whitespace and throughout the entire day as individuals work to adopt new patterns of eating, moving, managing stress, improving sleep, enhancing social connections, and avoiding unhealthy substances.
Designing and implementing a Digital Lifestyle Medicine (DLM) framework requires an intentional strategy and approach around care transformation that includes multidisciplinary virtual appointments, digital health coaching and programming, and peer support. Toward helping inform a scalable model of DLM for population-level impact, we describe the basic tenets of structuring and delivering DLM, share preliminary outcomes, key success factors, and opportunities for enhancement and expansion.
Implementation of a DLM Practice
Launching our LM practice during COVID provided an opportunity to build a virtual first approach. Initial steps involved the transformation of our teaching kitchen to a state-of-the-art virtual studio. Since April 2020, we have streamed over 107 virtual culinary medicine classes to the home kitchens of medical residents, patients, employees, and community members. Later in 2020, we successfully launched our specialty practice and our first LM intensive lifestyle change program, the Complete Health Improvement Program (CHIP), virtually with funding support provided by the health system for our own team members. Currently, we deliver several virtual visit types within our LM specialty practice including provider consults, shared medical appointments (SMAs), medical nutrition therapy (MNT), tobacco and nicotine consultation, and health coaching. Billing structure for virtual visits remains in fee-for-service model for SMAs and MNT with non-reimbursable health coaching applied to longitudinal programs. We offer several other ways to engage with our LM team including webinars, book clubs, and a Facebook group. While all these virtual offerings are important, most important for us was the ability to operationalize SMAs virtually, given their importance for a sustainable LM business model as well as to enable peer support critical for behavior change. 3
Digital Behavior Change Support and Health Coaching
Health coaching is a critical component to successful and sustained behavior change. 4 Supporting patients with behavior change requires ongoing and fluid communication that is not typical of patient to clinician interaction. Despite the lack of payer reimbursement, we have found creative solutions to implement individual and group-based virtual coaching. To enable efficient ongoing personalized support, we developed a library of messages based on evidence-based strategies that are designed to nudge and support the change process. These messages can be delivered on a set schedule or can be referenced by coaches to create efficiencies in personalized messaging. Meaningful, successful, and sustained behavior change requires ongoing support often beyond what a care team can offer and is most effective when patients are intentionally tracking and monitoring their own progress and data. Prescribing health apps and digital therapeutics provide an opportunity to extend behavior change support. Our team led the development of a formulary of best-in-class digital applications for our health system that are prescribed to patients to support lifestyle change. We have leveraged a mixed-payment model for the prescribing of digital apps with either the provider or payer arm of the health system paying or at times a nominal cost is passed to the patient.
Peer Support in a Digital and Virtual World
Social and peer support are other critical components to successful and sustained change. 5 Not all patients have a robust social network that is supportive of their lifestyle changes. We believe that LM practices should support creating opportunity for scalable and ongoing connectivity to peers who also are adopting and sustaining transformative lifestyle change. Digital and virtual modalities enable patients and community members to connect with each other in an ongoing basis, in real-time, and without requiring physical proximity. Virtual SMAs and groups are a cornerstone to how we foster peer group support. We extend the ability for peers to connect by adding channels for ongoing peer messaging such as moderating the chat feature with Microsoft Teams or suggesting the app GroupMe, recommending groups utilize apps that foster social connectivity around health behaviors such as Strava for physical activity, supporting a private Facebook group for our patients and consumers of LM, and sponsoring virtual monthly reunions upon graduation from longitudinal programs.
Conclusion
Lifestyle Medicine brings health to the forefront of care and consequently a nontraditional and innovative model of care is required to keep the patient’s lifestyle behaviors at the front and center. Core requirements include a multidisciplinary team approach, evidence-based behavior change and health coaching support, and robust peer support. DLM offers a path to supporting health that offers key characteristics that enable transformation and meaningful population-level impact.
We refer to this as the RISE philosophy of DLM:
Relevant: brings the care into the everyday life of patients and into their whitespace, where the behavior change occurs.
Inspirational: leverages peer support and patient goal setting to empower meaningful behavior change; encourages patients to discover their “why.”
Sustainable: Utilizing a digital and virtual delivery method reduces the cost of delivering LM while increasing the number of patients that can be reached.
Effective: utilizes evidence-based behavior change science to support lifestyle change through LM professional and peer support.
Average Biometric Improvements for Patients Enrolled in CHIP (n = 31).
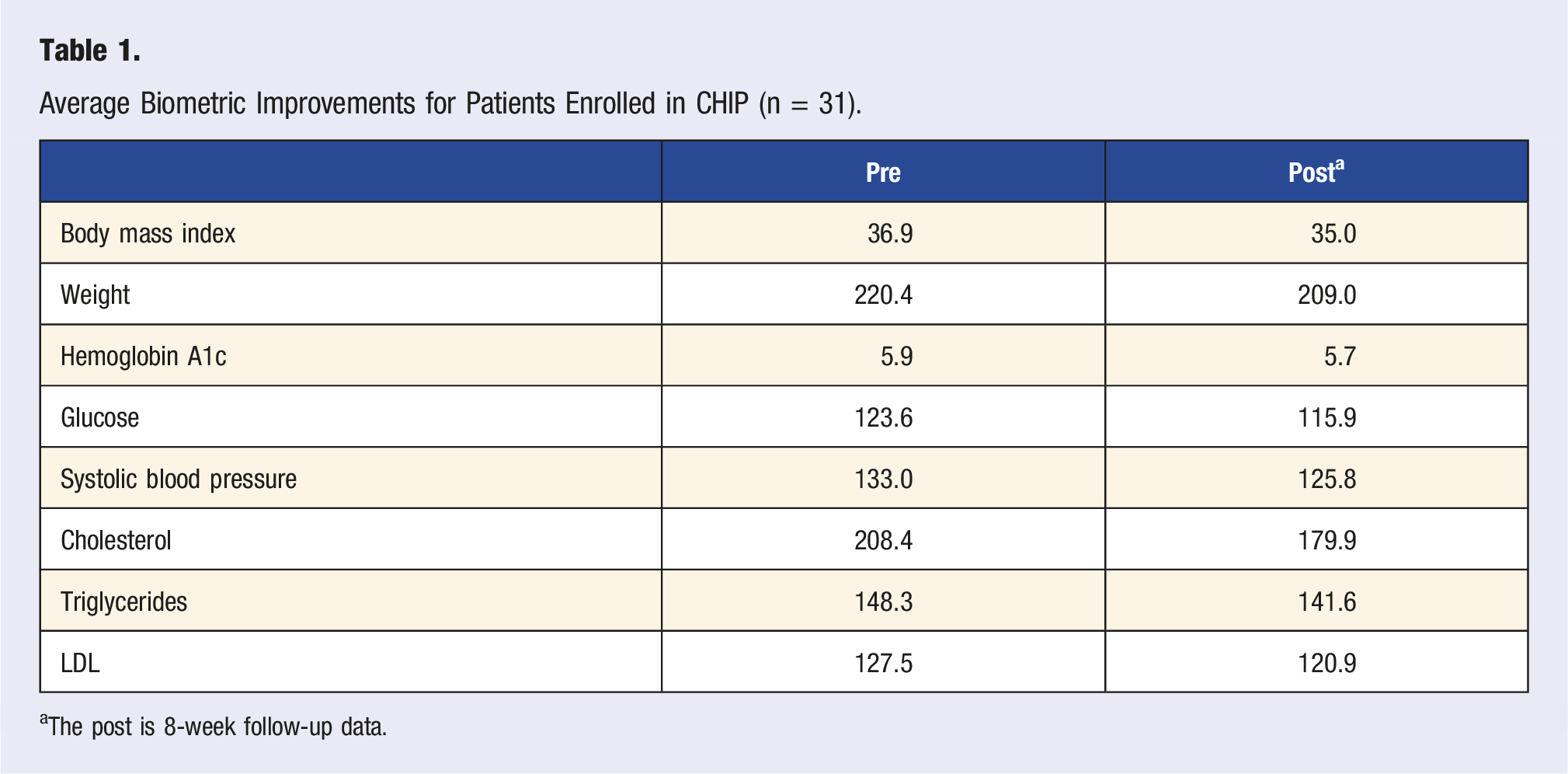
aThe post is 8-week follow-up data.
Drawing upon our experience to date, we believe key success factors in delivering DLM include • Utilizing an EMR to facilitate clinical documentation and tracking of patient outcomes. • Assessing the competency of patients with technology. • Increasing staff resources for virtual groups to moderate the chat, handle technology, and assist with documentation. • Offering program options to accommodate varying levels of readiness to change, varying schedules, and different payment models. • Supporting team members with group facilitation, motivational interviewing, health coaching, implicit bias, and design thinking training. • Fostering a spirit of innovation, transformation, patient centeredness, and consumer excellence. • Supporting DLM implementation with a clear strategic plan, business plan, and success metrics. • Executive level support for both LM and a digital first approach to health care.
While this article provides guidance for implementing DLM, this should be considered a starting point. We imagine a future in which layered upon these concepts is greater payer support for LM, a shift from ineffective employee wellness programs toward LM disease-reversal strategies, seamlessly integrated health coaching with remote patient monitoring, secure yet scalable ways of empowering peer support, and uniform standardization in data collection and evaluation such that reporting the population-level impact is visible. We are actively contributing toward these ideas both within our own integrated health system, as a corporate partner of ACLM, and through innovation with entrepreneurs. We believe the full realization of DLM occurs at the intersection of the science, technology, entertainment, and social health. It is at that intersection when the power of DLM truly can transform the future of medicine and inspire communities to stay well. This transformation will require aligned efforts and the diverse thinking and creativity of the collective passion and purpose-driven LM professional community.
Footnotes
Acknowledgments
The authors would like to thank Ryan Hampton and Kara Tibbe for their contributions to the program development and data analysis. Gratitude is also extended to Claire Cavarretta for assistance with preparing the manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.