
Abstract
Lifestyle Medicine Interest Groups (LMIG) have grown substantially since 2008, with 165 LMIGs established across the U.S. as of June 2024. The American College of Lifestyle Medicine (ACLM) supports LMIG establishment within academic and health system settings, providing opportunities for students, faculty, and employees to learn about and practice lifestyle medicine (LM). A cross-sectional survey containing multiple-choice and free-text questions was administered continuously to established LMIGs between March 2020 and May 2023. Descriptive statistics were generated to note the number of unique institutions, median number of events, event attendance, and frequency of event types. Thematic analysis was conducted for all free-text sections of the survey. Data from 1,062 LMIG events across 127 unique institutions with a total of 29,689 attendees was analyzed. Each institution had a median of 5 events with a median of 16 attendees. Lectures, group physical activities, and board meetings were most common. Quantitative findings reveal substantial growth among LMIG events, expansion across geographic locations, and insights into funding sources. Nutrition and physical activity were most frequently highlighted, while social connection, sleep, and avoidance of risky substances were least represented. LMIGs are growing in number and size, empowering future health professionals through LM awareness.
“Lectures, group physical activity, and board meetings occurred most frequently, and the most common event topics included nutrition and physical activity.”
Introduction
Lifestyle medicine (LM) is a medical specialty that uses therapeutic lifestyle interventions as a primary modality to treat chronic conditions, including, but not limited to, cardiovascular diseases, type 2 diabetes, and obesity.1,2 LM-certified clinicians are trained to apply evidence-based, whole-person, prescriptive lifestyle change to treat and, when used intensively, often reverse such conditions. Applying the six pillars of LM—a whole-food, plant-predominant eating pattern, physical activity, restorative sleep, stress management, positive social connections, and avoidance of risky substances—also provides effective prevention for these conditions. 3 Despite their importance, these pillars often do not receive adequate curricular focus in health professional training programs.4–7 Gaps in nutrition education, neglecting self-care, inadequate physical activity, and insufficient sleep persist among health professional students.8–12
Similar to other student interest groups, the American College of Lifestyle Medicine (ACLM) created Lifestyle Medicine Interest Groups (LMIGs) to help address the educational gaps that exist across medical and health professional curricula. 13 LMIGs serve as a starting point for academic institutions to work towards integrating LM into program curricula and ultimately support the path towards certification in the field through education, residency training programs, and professional certification by ACLM and the American Board of Lifestyle Medicine. Other types of student interest groups that are prevalent across health professional programs in North America include specialties such as dermatology, emergency medicine, family medicine, orthopedic surgery, psychiatry, radiology, and many others. Knowing that student interest groups related to other healthcare specialties, aside from the field of LM, provide additional knowledge, skills, practice, and clinical exposure, the development and expansion of LMIGs seem to be valuable next steps in exposing, supporting, and training health professional students in the six pillars of LM.14–16 As seen with many types of interest groups, LMIGs are intended to increase student engagement, understanding, interest, and even career choices based on the field of LM.17,18 Interest groups also highlight the importance of mentorship and connecting students with healthcare providers in a specific field or specialty as well as provide a means of a parallel curriculum in LM and medical education.19,20
LMIGs have emerged as vital entities within academic institutions and health systems, propelled by the growing recognition of the field of LM in healthcare. 1 LMIGs operate under the guidance of a dedicated local leadership team composed of officers and advisors, typically initiated by students, residents, or fellow trainees and supported by institutional faculty. Originally established at medical schools, support from ACLM has broadened the scope of LMIGs to encompass any academic institution or health system. Since the foundation of the first LMIG in 2008 at Harvard Medical School, there has been steady growth, and as of June 2024, an LMIG has been established at 106 of the approximately 200 U.S. medical schools, with a total of 165 LMIGs established on both academic and health system campuses. 21
The promotion and practice of LM within communities is central to the mission of the LMIGs. This involves cultivating multi-institutional LM programming, fostering connections among individuals interested in LM, and offering opportunities for professional development and leadership within the field. Education is a cornerstone, with objectives ranging from establishing or enhancing LM curricula in medical and health professions schools to providing exposure to LM practice in various settings.7,20–24
LMIGs are subject to specific requirements designed to ensure their active engagement and alignment with ACLM's objectives. A crucial component entails completing a one-time orientation facilitated by ACLM, typically held in March, July, and October. To support cross-collaboration between groups, LMIG officers are invited to participate in a dedicated leadership community on ACLM’s member engagement platform, ACLM Connect, where they contribute to group forums about LMIG success strategies, funding opportunities, and identifying key areas for growth. Additionally, LMIGs are expected to host a minimum of three events every six months, fostering community engagement and promoting LM initiatives.
To maintain transparency and accountability, LMIG leadership must submit documentation, including officer information surveys, event reports, and annual reports from LMIG advisors and leaders, ensuring ACLM remains informed of their activities. These requirements serve to uphold the standards of LMIGs and reinforce their commitment to advancing LM principles within their respective communities. 25
These resources and requirements have been implemented since 2020 and have supported the growth and scalability of LMIG establishment and support. Between 2020 and 2023, the number of LMIGs tripled from 46 to 140 established LMIGs (Figure 1). ACLM has continuously collected event reports since March 2020 and provides important data about LMIG events. A better understanding of LMIGs and their events can provide important insight into their reach and inform how ACLM can best structure appropriate support moving forward. Established LMIG growth chart.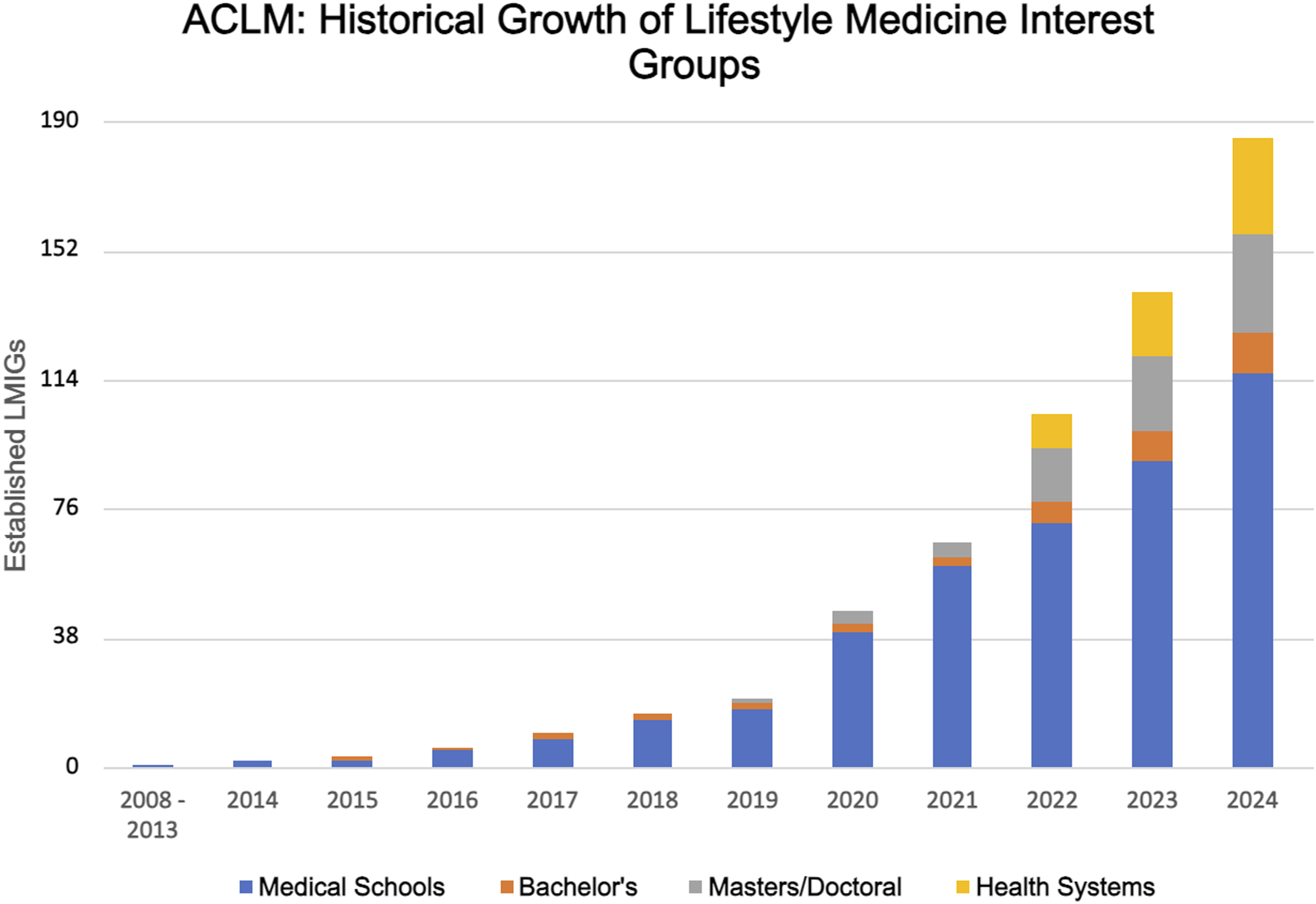
Objectives
Using data from event reports regularly collected by ACLM, the objectives of this study are to (1) describe the scope, reach, and key elements of LMIG events, (2) demonstrate the geographic distribution of LMIG events, (3) analyze the type of funding used to host LMIG events, and (4) determine needed resource categories.
Methods
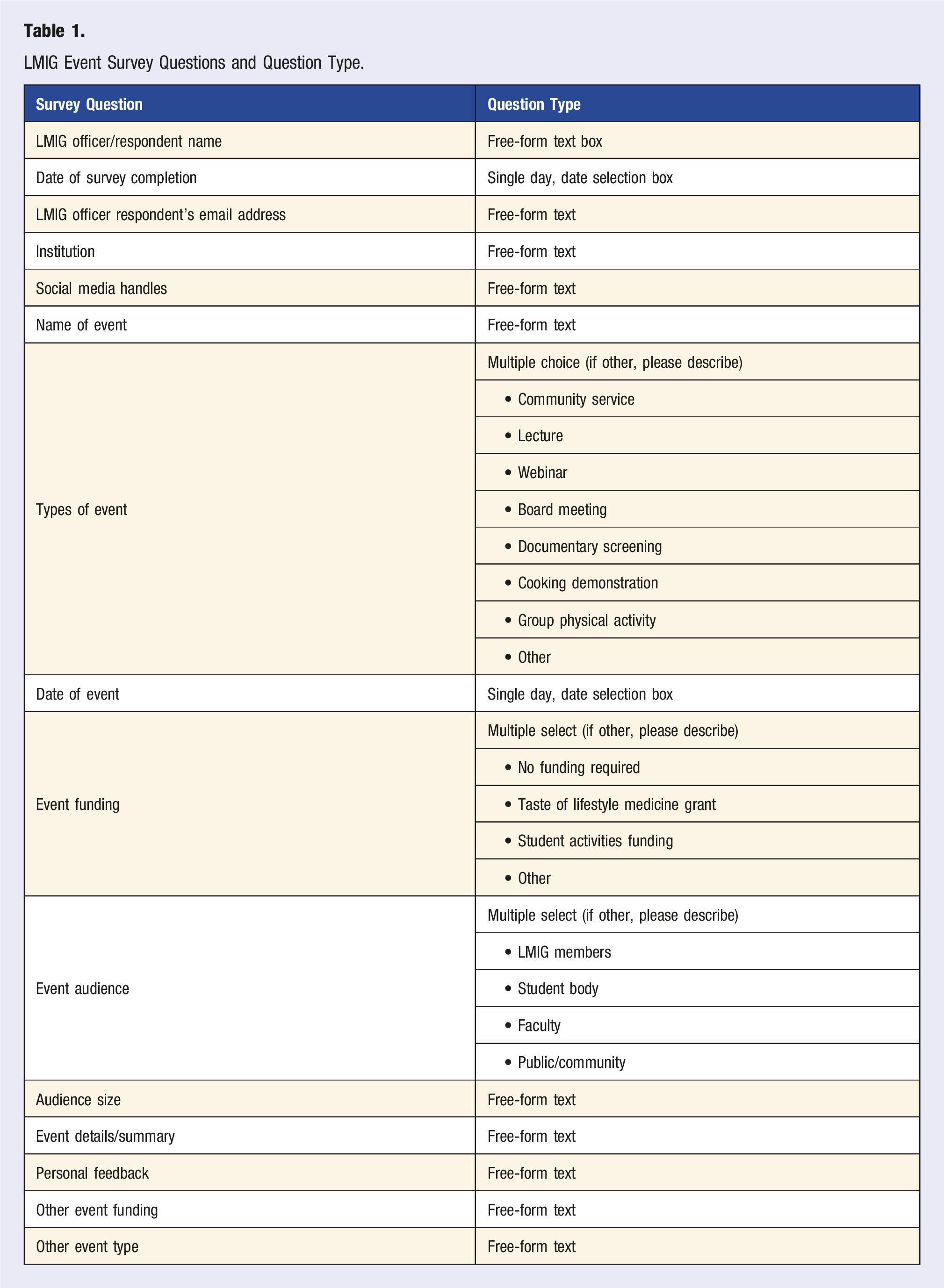
The LMIG event report was developed by members of the ACLM education and research team to track LMIG requirements, highlight their reach, and identify resources needed to improve the quality of LMIG activities. The report link was provided to LMIG leaders during their initial LMIG orientation, accessible within the LMIG toolkit and ACLM Connect LMIG Leader Community, as well as included in quarterly LMIG officer update emails sent from ACLM. The aforementioned LMIG toolkit was created to make the process of starting and maintaining an LMIG as easy as possible for students and practicing health professionals alike. 25 LMIG leaders and advisors were provided access to submit a 5-10 minute cross-sectional LMIG event report to fulfill a portion of the annual ACLM LMIG reporting requirements. The submission of these LMIG event reports is mandatory. The report was administered in English, and responses were collected via ACLM’s project management platform, Asana.
LMIG Event Survey Questions and Question Type.
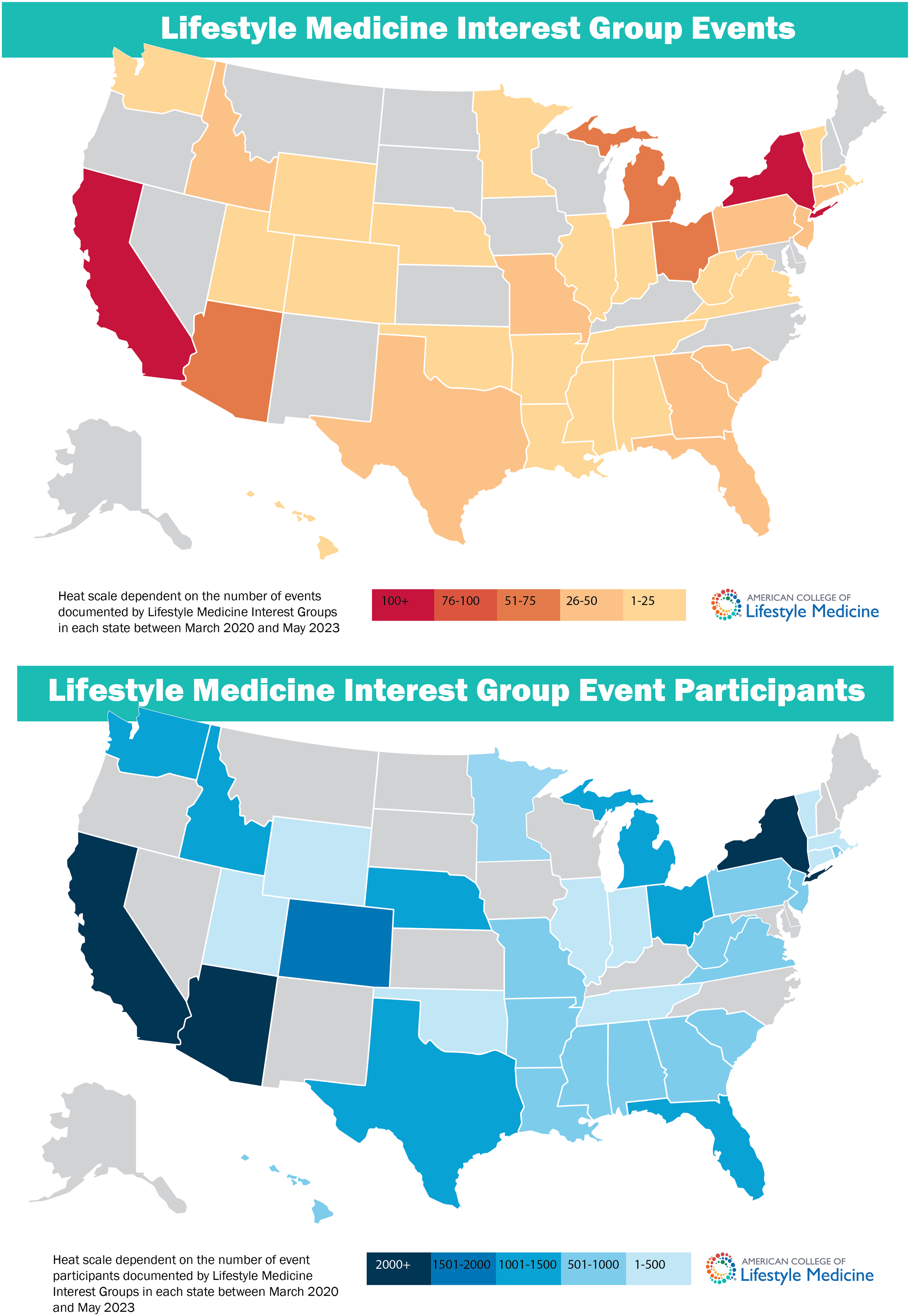
Geographic distribution of LMIG events and participant distribution of LMIG events.
Thematic analysis of key elements of LMIG events was conducted for all free-text questions, including event details, personal feedback, other event funding, and other event type. Two team members independently inductively coded free-text data into categories to identify emergent categories of responses. Discrepant coding was resolved through discussion with a third member of the research team to modify codes as needed and achieve consensus. The overall frequency of codes and themes of the LMIG events was determined and ranked.
Results
Participants reported 1062 LMIG events held at 127 unique institutions, with a total of 29,689 attendees from the years 2020-2023. During this timeframe, the number of established LMIGs tripled from 46 to 140 LMIGs. Each institution reported a median of 5 events (range 1-38) with a median of 16 attendees (range 2-500). The most frequently held events were lectures (26%), group physical activity sessions (15%), and board meetings (11%) (Figure 3 and Table 2). Quantitative findings reveal a 259% growth of established LMIGs across geographic locations, a 163% increase in LMIGs among medical schools, a 400% increase in LMIGs among masters/doctoral-level programs, 350% growth for bachelors-level programs, and the new development of LMIGs for health systems from March 2020 through May 2023. This growth has led to increased LMIG events and helpful insights related to sources of LMIG event funding. Heatmaps were created to visualize the geographic distribution of LMIG events across the United States, highlighting that institutions in the states of California and New York held the highest number of LMIG events, with over 100 LMIG events held in both states. There are 16 U.S. states that do not yet have a formal LMIG at any institution. As for LMIG event funding sources, the majority of events (45%) did not require funding, 24.2% of events were funded by their respective institution’s student activities funds, 14.8% of events were funded by an ACLM Taste of Lifestyle Medicine Grant, and 16.2% of events were funded by other sources, including private funds from institutional staff, faculty, or students (Table 2). Distribution of LMIG event type and representation of the ACLM pillars. Type of Event, Event Funding Sources, Representation of the Six Lifestyle Medicine Pillars, and Distribution of In-Person and Online LMIG Events.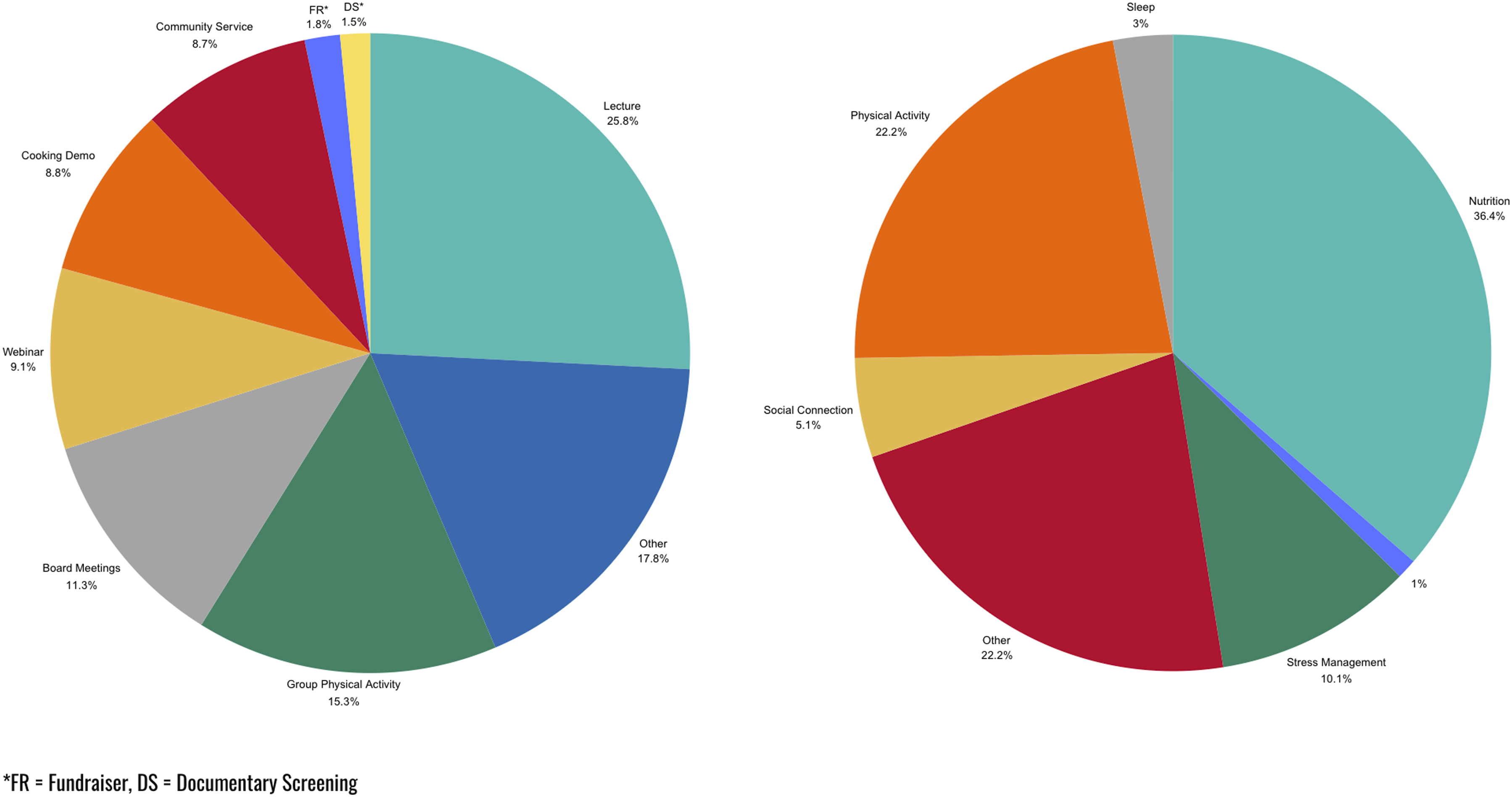
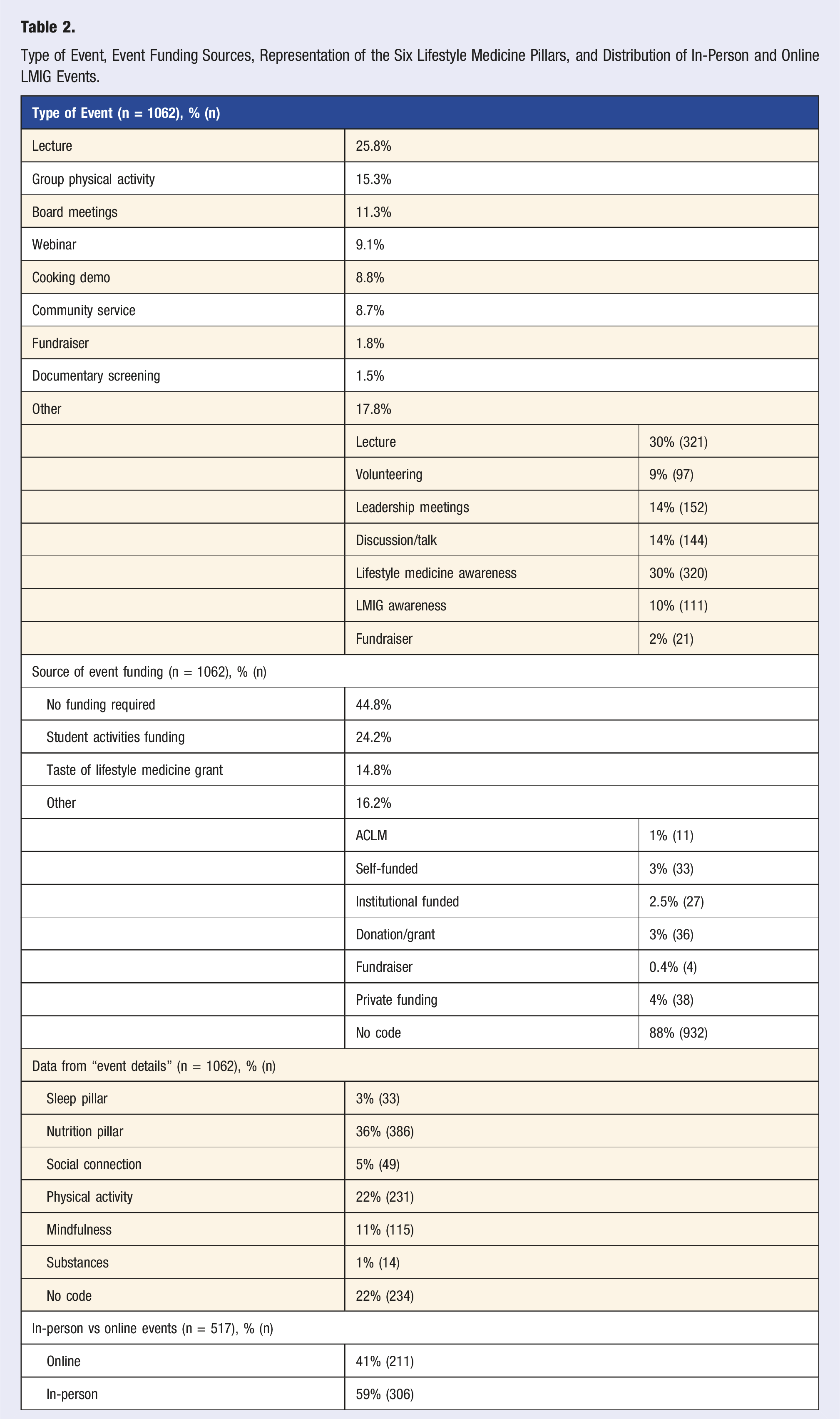
Analysis of LMIG report free-text responses revealed further insights pertaining to the key elements of the 1062 LMIG events being evaluated. Categorization of responses yielded 17 codes for event details, 13 for personal feedback, 7 for other event types, and 7 for other event funding sources. Of the six ACLM pillars, nutrition (36%) and physical activity (22%) were the most frequently noted topics among all LMIG events. Stress management through mindfulness and well-being practices was the focal point of 11% of LMIG events. Conversely, the ACLM pillars of social connection (5%), sleep (3%), and avoidance of risky substances (1%) were least represented among LMIG events (Figure 3 and Table 2). As for the format of LMIG events, lecture and/or discussion-style events were most prevalent compared to documentary viewings, community volunteering, and fundraising events (Figure 3 and Table 2). A total of 41% of LMIG events promoted LM awareness and/or LMIG awareness to prospective LMIG members, the community, and other audiences. Of the responses that noted a specific LMIG event location, 59% were held in person, while 41% were held over a virtual platform (Table 2). Areas of improvement among LMIG events, such as event promotion, increased event attendance, and improved event logistics, should be noted and further explored.
Discussion
The growth trajectory of LMIGs from 2008 to 2024 highlights the value of these student interest groups across medical schools, bachelor’s and graduate degree programs, and health systems. 21 The 127 unique institutions, 1062 events, and 29,689 event attendees represented in this analysis exemplify the rapid growth of LMIGs and their respective events from 2020 to 2023. 6 Student interest groups provide many valuable opportunities for health professional students of all types, including increased exposure to specialty fields, in-depth training and workshops, collaborative and interdisciplinary learning, networking, leadership, advocacy, and research, among others. From the importance of developing professional identity to increasing student professionalization in health professional research and education, many types of student interest groups are increasing opportunities for medical students, nursing students, public health students, and so many others.26,27 The contribution of this analysis was to examine the growth of LMIGs since 2020 and determine existing gaps that can be improved upon as ACLM continues to grow and expand its LMIG initiatives. The results of this cross-sectional survey analysis provide valuable insights into specifically how LMIGs can play a role in integrating LM educational and experiential opportunities into healthcare education and training and how LMIG efforts can be improved for the future. 7
Student interest groups also fill in gaps and areas of weakness within the medical and health professional fields. Whether it be high levels of stress, poor dietary habits, too little sleep, not enough physical activity, or the need for social support, a wide variety of health professional education and training efforts are aiming to increase opportunities for student learning and health behavior modification.28–30 LMIGs are bridging many gaps in health professionals’ and students’ training and education,14–19 including an integral role in the implementation science and RE-AIM/PRISM approaches to encourage the uptake of evidence-based LM education, research, and practice. 31
This analysis highlights the predominant types of events and event topics of all 1062 LMIG event surveys. Lectures, group physical activity, and board meetings occurred most frequently, and the most common event topics included nutrition and physical activity. While opportunities exist to increase the number of events focused on social connection, stress management, and avoidance of risky substances, the focus on nutrition and physical activity events is promising, as unhealthy dietary habits and decreased physical activity have been identified as major concerns contributing to increasing levels of stress and burnout for medical students.32,33 Recent research suggests that students who maintain schedules that balance studying with healthy habits and self-care are less likely to experience burnout and more likely to optimize their academic performance.32,34–38 Participation in LMIG events should be considered as a potential strategy to help combat the academically rigorous medical school environment and the associated perception of medical students that healthy lifestyles must be sacrificed for academic achievement.
ACLM further supports LMIGs by facilitating a free, virtual LMIG lecture series to reduce time and access barriers to applicable, evidence-based LM content from board-certified professionals. The virtual LMIG lecture series is made available bi-monthly via Zoom and hosted by LMIGs across the country. Virtual lecture topics have ranged from “Finding a path to healthy and sustainable diets for all,” presented by Dr Walter Willet, “The Power of Sleep,” presented by Dr Param Dedhia, to “Cultivating Resilience: Life lessons from the longest lived,” presented by Dr Meagan Grega and “Collaboration and Negotiation: The Key to Therapeutic Lifestyle Change,” presented by Dr Beth Frates.
Another notable strength related to reducing barriers to LMIG events is that 44% of all events did not require funding. Furthermore, 24% of LMIG events were provided student activities funding from their respective institutions, while only 14.8% of LMIG events used the Taste of Lifestyle Medicine (TOLM) grant provided by ACLM. The TOLM grant is available to U.S. medical and health professional students and faculty who are “interested in hosting a non-commercial LM educational event”; the grant funds are specifically available for the reimbursement of whole-food plant-based foods and ingredients. 39 This is an area of improvement and opportunity for the future growth and expansion of LMIGs as funding is often a barrier reported by those hosting LMIG events and other interest group-style events in academic and healthcare institution settings.23,40
Limitations of this study include the self-reported nature of the data on the LMIG report. For parameters such as number of participants, some answers were an estimate or a range. Furthermore, survey dropout limited data captured. Some responses were left blank and coded as “no code,” limiting the ability to draw conclusions from the data set. A majority of participants did not complete the survey section related to LMIG event sources of funding. Given that this data encompassed events held during the height of the COVID-19 pandemic, LMIGs were required to adapt their events to comply with regulations. For example, some LMIGs planned in-person events but had to cancel or shift to an online meeting style. Prior to 2020, there was no formalized data collection process for analyzing LMIG events. Although it is not possible to draw comparisons to LMIG events before 2020, LMIGs and their respective events have notably grown in number, frequency, and size since 2020, demonstrating the rise in LM awareness.
Despite the limitations, this is a summary of how the objectives were met to describe the scope, reach, and key elements of LMIG events, demonstrate the geographic distribution of LMIG events, analyze the type of funding used to host LMIG events and determine needed resource categories. Between March 2020 and May 2023, 127 LMIGs collectively held over 1000 events, demonstrating continued LMIG growth. These events were held in all but 16 states in the US. Based on the findings of this LMIG event analysis, it is worth noting that over 44% of these events did not require funding. Seeing continued growth among LMIGs while often mitigating the cost barrier is powerful for further growth and expansion of LMIGs and their associated events.
Looking ahead, the new standardized method for documenting LMIG events will help illustrate the trajectory and development of LMIGs and their associated events. Making sections of the survey mandatory will bolster future data to prevent non-responses. Given that the data from this 3-year period included COVID-19, it will be of interest to see if there is a shift in the mode of delivery of events from virtual platforms to in-person gatherings. 23 The overall frequency of themes helps demonstrate the ACLM pillars on which LMIGs tend to focus, while additional resources for LMIGs to host events on sleep and avoidance of risky substances should be considered. Completion of the LMIG survey also allowed for LMIG leadership to reflect on their event and identify areas for improvement. Noted areas of improvement include event promotion, logistics, and increased attendee participation. The identified areas of improvement can be integrated into resources such as the LMIG Toolkit and orientations so LMIG leaders can anticipate challenges and see how their peers have adapted. Finally, analyzing data from the surveys gave rise to changes to the survey questions and overall survey structure to enhance data collection for the future.
This project’s objective is to determine the key elements of successful LMIG events, as well as their overall scope and reach. These results document the impact that LMIGs have had over the past 3 years. Seeing the evolution of LMIGs through these event records not only documents the influence LMIGs have in their communities but also underscores the overarching goal of increasing LM awareness at institutions to promote evidence-based, LM-driven healthcare.
Conclusion
This analysis reveals robust growth and great value provided by existing LMIGs and their respective events. In response, this summary has led to new paths for growth and improvement for LMIGs and serves as a call to action to include schools from every state in the US and focus on areas of improvement for LMIGs, such as event promotion, increased event attendance, and improved event logistics. This analysis indicates that marketing, communication, and pre-event planning efforts may be helpful in expanding the scope and reach of LMIG events in the future.
Footnotes
Declaration of Conflicting Interests
GOG, SFH, KLS, and MCK are employees of the American College of Lifestyle Medicine. The other author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the American College of Lifestyle Medicine.
Ethical Statement
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.