
Abstract
Aging is a lifelong process, and many chronic diseases and geriatric syndromes are influenced by lifestyle factors. Here, we discuss the benefits of integrating education in geriatrics and lifestyle medicine to not only improve competency of health professions learners in each area, but also so that learners can promote healthy aging in the clinical care of their future patients. We review the current state of geriatrics education, the role of lifestyle medicine in aging, and strategies to bridge the gaps between geriatrics and lifestyle medicine.
“Lifestyle medicine promotes healthy aging and can help prevent or manage multiple geriatric syndromes.”
The U.S. population is aging and the prevalence of geriatric syndromes, such as frailty and dementia, is anticipated to increase. Despite these trends, medical trainees often receive limited education in both geriatrics and lifestyle medicine, specialties essential for preventing and managing geriatric syndromes. Addressing this gap through an integrated healthy aging curriculum can better prepare learners to care for the growing population of older adults.
Current State of Geriatrics Education
Most medical trainees receive insufficient training and exposure in geriatrics. The Licensing Committee on Medical Education (LCME) does not mandate training in geriatrics, though does specify that the curriculum should cover “each phase of the human life cycle.” 1 Internal Medicine residents, who typically care for older adults, often receive less than 4 weeks of geriatric-specific clinical instruction in a three-year program.2,3 In addition, less trainees are choosing fellowships in Geriatric Medicine. 4 As a result, there are challenges in delivering adequate care to older adults. Integrating healthy aging education through the lens of lifestyle medicine may be a strategy to prepare health professions learners to care for older adults.
The Role of Lifestyle Medicine in Aging
Aging is a lifelong process, and many chronic diseases and geriatric syndromes are influenced by lifestyle factors. At a population level, up to 45% of dementia risk can be attributed to potentially modifiable lifestyle factors including physical inactivity, obesity, excessive alcohol intake, and social isolation. 5 A multi-modal and comprehensive lifestyle approach is likely more efficacious for preserving cognitive function than one single factor alone. In the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER), a multidomain lifestyle intervention including exercise, cognitive training, and nutritional guidance (n = 1260), performance on neuropsychological testing was 25% higher in the intervention group as compared to a health education control at 2 years. 6 In a recent randomized controlled trial of intensive lifestyle changes in patients with mild cognitive impairment or early dementia due to Alzheimer’s disease (n = 51), the intervention group experienced either small improvement or slower progression in cognition and function as compared to a waitlist control group at 20 weeks. 7 The study’s lifestyle modifications included a whole-food plant-based diet with micronutrient supplementation, aerobic exercise, strength training, stress management, and social support.
Similarly, lifestyle interventions, especially exercise and nutrition, are first-line interventions for frailty. 8 Resistance training is important for both frailty prevention and management given age-related loss of muscle mass. Multicomponent exercise that includes aerobic and balance training appears to be particularly effective. 9 Yoga and tai chi are emerging as effective multicomponent interventions for frailty.10,11 A Mediterranean-style diet and increased protein intake are evidence-based dietary strategies to combat frailty.12,13 Other geriatric syndromes, such as falls, urinary incontinence, depression, and insomnia similarly benefit from a lifestyle medicine approach, which can additionally help prevent geriatric syndromes such as polypharmacy.
In Figure 1, we describe the relationship between the “4Ms” of geriatrics and the six pillars of Lifestyle Medicine. The 4Ms was developed by the Age-Friendly Health System initiative to guide healthcare systems to become “age-friendly,” providing high-quality care across the evidence-based “4Ms” domains of What Matters (implementing patient-centered care that accounts for the individual’s priorities and desires), Medication (addressing polypharmacy, potential drug interactions, and adverse effects), Mentation (evaluating and treating cognitive impairment and mental health concerns), and Mobility (assessing and maintaining physical function and independence).
14
A conceptual model that illustrates the interconnectedness of the six pillars of Lifestyle Medicine—nutrition, stress management, sleep, exercise, social connection, and avoidance of risky substances—and their impact on the 4Ms of an Age-Friendly Health System: What Matters, Medication, Mentation, and Mobility. For example, physical activity promotion in childhood and mid-life can reduce future risk of dementia and falls. Integrated education in lifestyle and geriatric medicine better prepares learners to support healthy aging across the lifespan.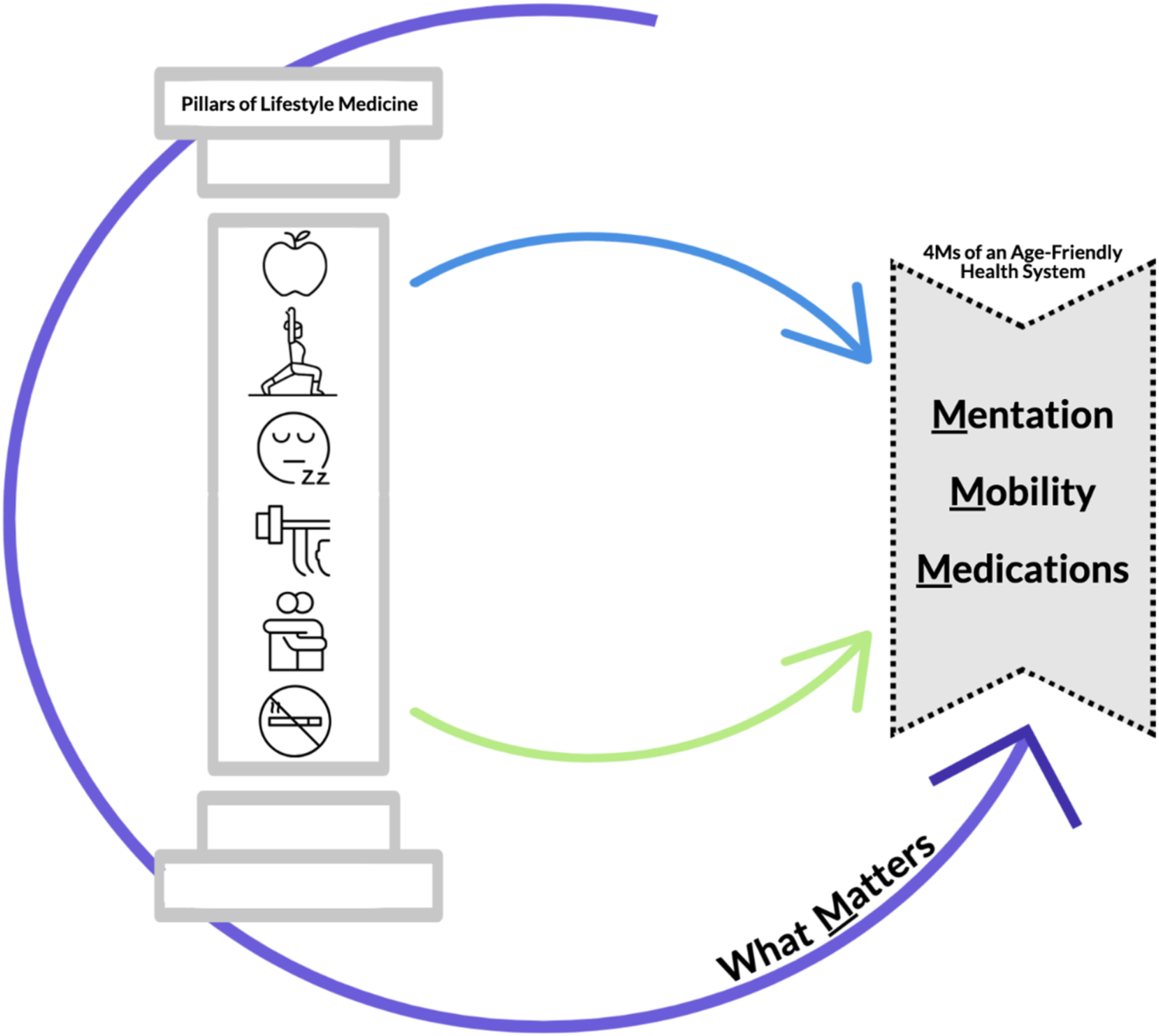
Bridging the Gap: Integrating Geriatrics and Lifestyle Medicine
Traditionally, geriatrics and lifestyle medicine have been treated as separate disciplines within medical education, potentially competing for limited curriculum space. As described above, lifestyle medicine promotes healthy aging and can help prevent or manage multiple geriatric syndromes. An integrated curriculum will prepare learners across health professions to provide better care across the lifespan.
The benefits of robust education in aging and lifestyle medicine extend beyond those specializing in geriatrics. Primary care clinicians care for patients of all ages and are adept at health screenings and preventive counseling. Thus, they are well-equipped to intervene in early- to mid-life to prevent chronic disease and geriatric syndromes. For pediatricians, early injury prevention, dietary and physical activity counseling, and screening for a safe home environment sets the stage for healthy habits in children and reduces dementia risk and other age-related issues in the future. Future surgeons and physiatrists will be equipped to prepare their older patients for surgery through “prehabilitation” programs 15 and assess for caregiver support to promote better recovery for their patients.
Educators can teach healthy aging in creative and innovative ways. Harvard Medical School (HMS) has two major Curricular Themes that have begun to collaborate on this integrative topic. The Aging and End-of-Life Care Theme is a longitudinal curriculum based on the Geriatric 4Ms model 16 while the Nutrition and Lifestyle Medicine Theme focuses on the six pillars of lifestyle medicine. The themes developed a case-based collaborative learning session that covers elements of lifestyle medicine essential for healthy aging, such as strength training and protein requirements to mitigate age-related declines in muscle mass and frailty. The Third Edition of the textbook Lifestyle Medicine began including the section “Lifestyle Medicine in Geriatrics” for the first time, a significant advancement in bridging these fields. 17 During training, learners can be incorporated into settings that promote healthy aging through lifestyle approaches, such as senior centers, home visits, and medical group visit programs.18,19
Ultimately, an integrated curriculum that combines geriatrics with lifestyle medicine can better prepare learners to care for older adults across the lifespan and is a strategy for educational programs to enhance their training in both areas. By doing so, we can ensure that healthcare professionals are not only prepared to address the immediate needs of their patients but are also equipped to promote long-term health and well-being as people age.
Footnotes
Author Contributions
J.V.L. and S.P. drafted the manuscript, created figures, and edited and approved the final version.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS, or the U.S. Government.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of an award (GACA 6 K01HP49053-01-01 to J.V.L.) totaling $86,978 with 0% financed with non-governmental sources. The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS, or the U.S. Government.