
Abstract
Background. Lifestyle behaviors have a significant effect on preventing and treating disease, yet there is minimal graduate medical training in lifestyle medicine (LM). LM stakeholders’ perspectives regarding components of a LM fellowship have been examined. However, the student perspective has not been studied. Methods. A cross-sectional study design analyzed medical student perceptions surrounding LM domains and educational experiences. A Kruskal-Wallis analysis of variance and a Wilcoxon Rank-Sum Test were performed for each topic. Results. In all, 21 medical students completed the survey. All domains (nutrition, physical activity, behavior change, stress resiliency, and personal health), except smoking cessation, were rated as important or very important by at least 75% of the respondents (P = .002). The 4 highest-rated educational experiences, by at least 69% of respondents, included developing LM interventions and health promotion programs, clinical experiences, and teaching other health care providers about LM. Significant differences overall were found among the educational experiences (P = .005), with research and fund raising considered the least important. Conclusions. Medical students felt strongly about including nutrition, physical activity, behavior change, personal health, and stress resiliency as part of a LM fellowship curriculum. There was significantly less interest in smoking cessation. Desired experiences of students focused on delivery of LM.
‘Furthermore, gaps in primary care residents’ knowledge, self-efficacy, and perceived professional norms regarding obesity, nutrition, and physical activity have been identified.’
Background
The United States spends 17.9% of its gross domestic product on health care, 1 and 83% of these costs are attributable to patients with at least 1 chronic disease. 2 An estimated 80% of chronic diseases and premature death can be prevented with healthy lifestyle behaviors, such as not smoking and eating healthy.3,4 Additionally, intensive lifestyle modifications may reverse heart disease and influence genetic expression.5-7
Lifestyle medicine (LM) is defined as “the evidence-based practice of helping individuals and families adopt and sustain healthy behaviors that affect health and quality of life.”8 (p. 202, para 2) Currently, there is little formal training in LM.9,10 Furthermore, gaps in primary care residents’ knowledge, self-efficacy, and perceived professional norms regarding obesity, nutrition, and physical activity have been identified. 11 Many authors have called for increased nutrition and physical activity training in medical education.12-14
The American College of Lifestyle Medicine (ACLM) was formed in 2004 to address the need for education and training in the practice of LM. Other developments have included the following: a Lifestyle Medicine Education Collaborative for undergraduate medical education,15-17 a LM 4-year combined Family/Preventive Medicine residency program at Loma Linda School of Medicine, 18 and Continuing Medical Education courses. 19 However, a LM fellowship is absent from the current training opportunities.
A study by Polak et al 20 examined attitudes of LM stakeholders with regard to content areas and educational experiences in a LM fellowship. Results showed that training should focus on clinical experiences and teaching, including content pertaining to diet, physical activity, behavior change, personal health, and stress resiliency, with less focus on smoking cessation. However, input from medical students who are interested in LM has not been sought. The purpose of this study was to identify perceptions surrounding domains and educational experiences that might be included in a LM fellowship from medical students, who would be most likely to pursue such a training opportunity. We hypothesize that this study will replicate the aforementioned findings in medical students who are interested in LM.
Methods
A cross-sectional study design was used to analyze survey data collected from January to June 2014. A previously tested Likert scale questionnaire (1 = not important; 5 = very important) that assessed the perceived importance of specific domains and educational experiences for a LM fellowship curriculum was used. 20 Six items measured attitudes regarding suggested LM domains, and 8 items addressed recommended LM educational experiences. In addition, survey participants were invited to add narrative comments to each section.
In January 2014, all 5—Harvard, Loma Linda, Stanford, UCLA, and Western—of the ACLM-recognized Lifestyle Medicine Interest Group (LMIG) medical student leaders were emailed a link to a survey that was hosted on the Survey Monkey online platform. Recipients were invited to take the voluntary survey and to email it to other LMIG student members. Data were collected and entered into an Excel spreadsheet (Excel 2010; Microsoft Corp, Seattle, WA), which was used to create a data set for statistical analysis. Harvard Catalyst provided statistical support, and the Statistical Analysis System v 9.2 (Cary, NC) was used for all analyses. This cross-sectional analysis was reviewed and determined to be an exempt study by the Duke University Institutional Review Board (Protocol ID: Pro00062363).
Within-item responses were analyzed categorically using a χ2 test for homogeneity (Figures 1 and 2). Equity in variance within each educational item (eg, LM domains and educational experiences) was calculated using a Kruskal-Wallis analysis of variance (ANOVA), given the nonparametric distribution of the data (Figures 1 and 2). Pairwise comparisons were conducted using Wilcoxon rank-sum tests. The Bonferroni correction was used with P values ≤.008 and ≤.006, considered statistically significant for the LM domains and educational experiences, respectively.
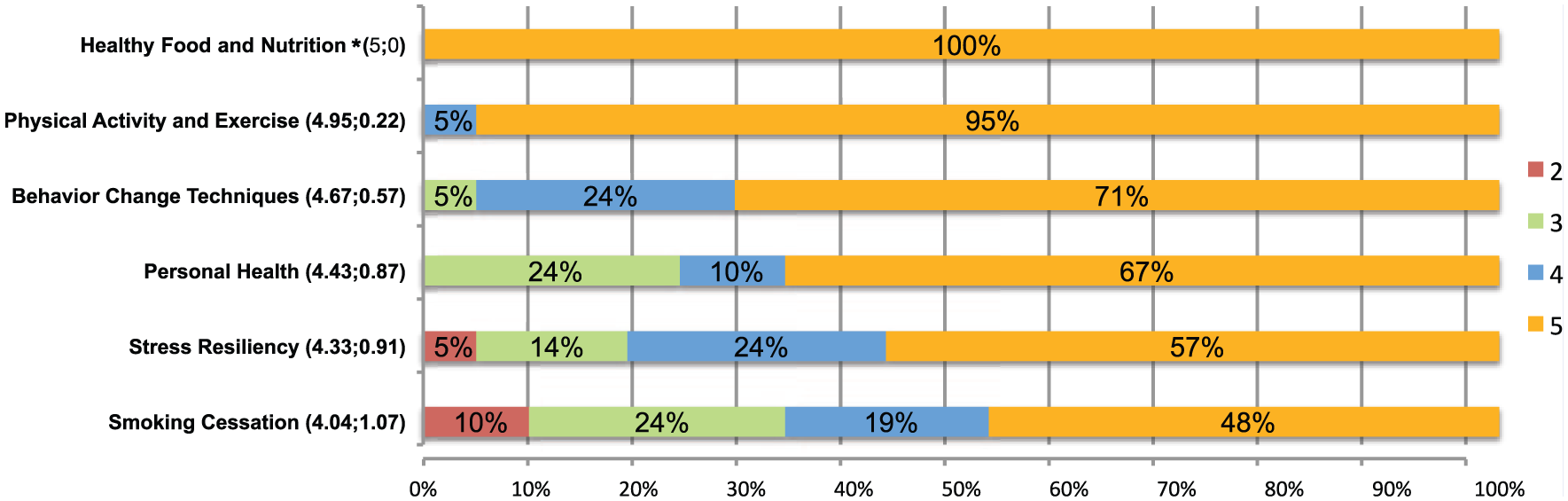
Lifestyle medicine (LM) domains: Percentage of responders’ perceived importance of specific LM domains to include in LM fellowship curricula (1 = not important; 5 = very important).
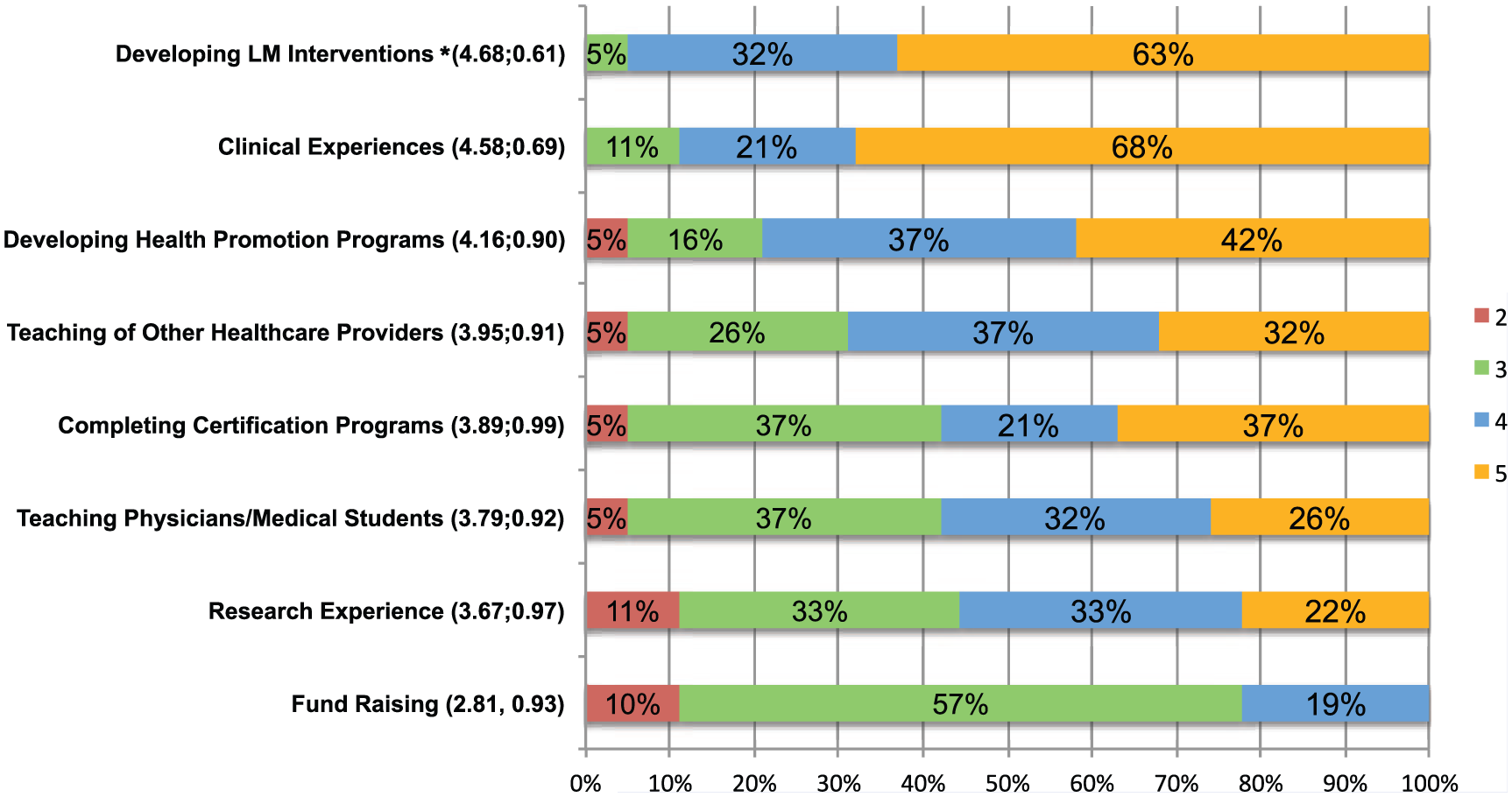
Lifestyle medicine (LM) educational experiences: Percentage of responders’ perceived importance of specific LM educational experiences to include in LM fellowship curricula (1 = not important; 5 = very important).
Results
A total of 21 medical students completed the survey. However, 3 of these students only completed the domain portion of the survey. It was not possible to calculate an accurate response rate because the total number of email addresses the link was sent to was not tracked.
Lifestyle Medicine Domains
The distributions of attitudes and average mean regarding the importance of including specific domains in a LM fellowship curriculum are presented in Figure 1. All domains except smoking cessation (eg, nutrition, physical activity, behavioral change techniques, stress resiliency, and personal behavior) were rated a 4 or 5 from at least 75% of the responders.
A Kruskal-Wallis ANOVA revealed significant differences overall across all the domains (P = .002). Pairwise comparisons showed that nutrition was endorsed more frequently than the following domains: smoking (z = 0.002), stress resiliency (z = 0.001), and personal health (z = 0.004). There were also significant differences with physical activity being endorsed more frequently than smoking (z = 0.006) and stress resiliency (z = 0.004). There were no other significant differences between the other domains.
Lifestyle Medicine Educational Experiences
Attitudes distribution and average mean regarding the importance of including specific educational experiences in the fellowship curriculum are presented in Figure 2. Four educational experiences, including clinical experience, teaching other health care providers, developing lifestyle interventions, and developing health promotion programs, were graded a 4 or 5 from at least 69% of the responders.
A Kruskal-Wallis ANOVA revealed significant differences overall among the educational experiences (P = 0.005). Pairwise comparisons showed that research was endorsed less often than clinical experiences (z = 0.003) and developing lifestyle interventions (z = 0.003); teaching physicians was endorsed less often than clinical experiences (z = 0.006) and developing lifestyle interventions (z = 0.003); and fund raising was endorsed less often than teaching physicians (z = 0.004), clinical experiences (z < 0.0001), developing lifestyle interventions (z < 0.0001), and obtaining certifications (z = 0.003). There were no other significant differences within the other educational experiences.
Qualitative Comments
A total of 10 responders (47.6%) wrote narrative suggestions in the “other domain” field and 1 responder (4.8%) in the “other educational experience” field; 2 responders (9.5%) wrote general comments. Major LM domain suggestions included social/emotional factors, mindfulness, business, and sleep. Epigenetics, biofeedback, and knowledge of local disease and cultural norms were also mentioned. The only comment regarding educational experiences suggested adapting health practices to suit the target community and population. The 2 general comments encouraged a patient-centered approach and expressed the desire for a 1.5-year, as opposed to a 1-year, fellowship experience.
Discussion
This study offers a medical student perspective on the perceived importance of LM domains and educational experiences that could be included in a LM fellowship curriculum. The results suggest that medical students similarly value the same educational domains as key LM stakeholders. 20 Greater than 75% of students rated all domains (eg, nutrition, physical activity, behavioral change techniques, stress resiliency, and personal behavior), except smoking cessation, as a 4 or 5 on the Likert scale, which was very similar to the stakeholder perspective. 20 Both students and stakeholders perceived smoking cessation as a significantly less important component of a LM fellowship. This is notable because cigarette smoking is the leading preventable cause of death and disease in the United States. 21 Additionally, the ACLM specifically denotes the domains of diet, exercise, stress management, and smoking cessation as components of LM. 22
It is unclear why both medical students and stakeholders view smoking cessation as less important. It is possible that the declining smoking rates in the United States and lack of exposure in day-to-day experiences have resulted in a perception that smoking cessation skills may be less important or useful in practice. 23 Medical students may also recognize that numerous tobacco cessation programs and resources already exist24,25 and feel comfortable referring patients to those resources, rather than provide intensive treatment themselves. Alternatively, medical students and stakeholders may already feel competent and comfortable with their previous training. Further research is needed to examine the necessity of including smoking cessation in a LM fellowship.
This study supports inclusion of the educational experiences of developing LM interventions, clinical opportunities to practice LM, developing health promotion programs, and teaching other health care providers about LM as part of a LM fellowship. These results were similar to LM stakeholders’ attitudes. 20 Both groups agreed on the importance of engaging in LM interventions, clinical experiences, health promotion programs, and teaching other health care providers about LM. Medical students and stakeholders alike rated obtaining certifications, fundraising, and research as less-important educational experiences. 20
The only notable difference between medical students and stakeholders was the student attitude surrounding the importance of educating other physicians/medical students. This educational leadership experience of training colleagues was rated as a 4 or 5 in importance by 91% of stakeholders, whereas only 58% of students felt this way. 20 Medical students may view themselves as learners in the early stages of training and, therefore, not at the competency level required to teach others in the profession. Experienced clinicians have a greater fund of knowledge and may appreciate the importance of and feel more comfortable with teaching. Further investigation is needed on the importance of including teaching medical students and other physicians about LM as part of a formal fellowship.
Narrative comments provided additional insight into what areas might be missing from a LM curriculum. Areas that appeared in both the stakeholder study and in this study included sleep, mindfulness, and behavior change techniques (eg, biofeedback, culture of change). Interestingly, multiple medical students commented on business models, whereas the stakeholders emphasized experience with implementing already existing LM programs (eg, Dean Ornish Program or Coronary Health Improvement Program [CHIP]).26,27 Future studies should assess the necessity and feasibility of providing the type of fellowship experience that medical students are seeking and may also want to gauge the interest level of including additional domains such as sleep or mindfulness.
There is clearly a strong interest in additional training in LM, and the creation of a LM fellowship could meet this need. A natural fit for this proposed fellowship could be within the family medicine or preventive medicine academic curriculum. Family medicine, in particular, has identified a lack of balance between research and clinical fellowships. 28 A LM fellowship could help translate some of these essential skills in providing evidence-based lifestyle treatment. This would also help address a significant gap in primary care residents’ knowledge, self-efficacy, and perceived professional norms regarding obesity, nutrition, and physical activity counseling. 11
A critical piece of a LM fellowship would be to provide the education and clinical experiences medical students are seeking. The results of this study support previous findings and offer further evidence reinforcing that a LM fellowship curriculum should include education in the domains of nutrition, physical activity, behavior change, stress resiliency, and personal health and focus on the delivery of LM. Importantly, this evidence came from medical students who expressed an inherent interest in LM. This study specifically targeted these individuals because of their familiarity with LM and ability to provide informed opinions on what skills a LM fellowship should address.
Limitations
This was a voluntary self-reported study of medical students who were members of a LMIG in a US medical school. Although the survey had been tested previously, it had not been fully validated. The survey was emailed to LM interest group leaders to distribute to the LMIG members. This resulted in an inability to determine how many people actually received the survey to calculate a response rate. The survey was sent to medical students who were clearly interested in LM, likely resulting in the high rankings on the Likert scale for many of the items. However, this study was not intended to generalize fellowship attitudes across all students. Furthermore, medical students who are interested in LM are the most likely individuals to seek a LM fellowship. This study was designed to explore the values and preferences of interested students because any LM fellowship program would need to appeal to and be valued by those pursuing the additional training.
Although the sample size of 21 respondents was small (with 3 medical students completing only half of the study), it provided sufficient power to detect significant differences across the domains and educational experiences examined. It is possible that further differences could be detected with a larger sample size. Results largely replicated findings from the prior study involving 35 stakeholders. 20
Conclusion
Medical students interested in LM felt strongly about including nutrition, physical activity, behavior change, personal healthy, and stress resiliency as part of a LM fellowship curriculum, with significantly less interest in smoking cessation. The desired educational experiences of medical students focused on the delivery of LM through developing lifestyle interventions, clinical experiences, developing health promotion programs, and teaching other health care providers. Notably different in this study of medical students, as compared with LM stakeholders, was the lack of emphasis toward teaching other physicians and medical students as part of a LM fellowship curriculum.
Footnotes
Acknowledgements
This work was conducted with support from Harvard Catalyst, The Harvard Clinical and Translational Science Center (National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health Award UL1 TR001102), and financial contributions from Harvard University and its affiliated academic health care center. The content is solely the responsibility of the authors and does not necessarily represent the official views of Harvard Catalyst, Harvard University and its affiliated academic health care centers, or the National Institutes of Health.
Authors’ Note
This cross-sectional analysis was reviewed and determined to be an exempt study by the Duke University Institutional Review Board (Protocol ID: Pro00062363).