
Abstract
Despite the need for and relevance of leadership skills to the success of medical trainees and healthcare professionals, few medical schools offer formal leadership training during the preclinical years. Where such curricula exist, we have found few schools that intentionally incorporate key principles of lifestyle medicine critical to short- and long-term career development. We describe a novel relationship-centered leadership curriculum, grounded in a conceptual framework of emotional intelligence and incorporating key principles of lifestyle medicine, first piloted in 2019 and now in its fourth year of existence. In comparing pre- and post-course self-evaluations on a 5-point Likert scale, students (n = 19) reported increased competencies in Self (3.12 vs 4.20, P < .001), Teams (3.06 vs 4.00, P < .001), and System (2.55 vs 3.55, P < .001) domains. Qualitative responses demonstrated that a vital strength of the course was its direct relevance and immediate applicability to students’ personal and professional roles and goals. Results provide encouraging support for using a relationship-centered leadership framework that incorporates core elements of lifestyle medicine and emotional intelligence to facilitate medical students’ leadership development, as related to leading oneself and in dynamic relationships with others (e.g., with leaders, colleagues, patients, and within communities, teams, and systems).
Keywords
Introduction and Purpose
The purpose of this article is to describe a novel medical student leadership development curriculum that incorporates core elements of lifestyle medicine and emotional intelligence reflecting a relationship-centered leadership model. We outline the curriculum conceptual framework, program design, initial implementation, and lessons learned regarding the incorporation of lifestyle medicine into medical student leadership development.
Background
Within professional literature, leadership definitions have varied over time and by theoretical perspectives. For the purposes of our work, we started with a definition offered by Northouse 1 that is widely used in the field: leadership is working together with and influencing other people to achieve a common goal, greater than any one person themselves. This definition emphasizes that leadership is not about natural talent, skills, or titles, rather it is grounded in the work of leading. It reflects contemporary conceptions that move beyond leadership as a within-person construct and rather, as ongoing processes involving interactive and dynamic relationships between leaders and followers in varying contexts (e.g., self and others, teams, communities, and systems). That is, for leadership to be effective, there must also be effective followership; developing roles and relationships between the two are essential. 2
Leading (“doing the right thing”) is distinct from managing (“doing things right”).
3
Management produces order and consistency whereas leadership produces change and movement. A manager counts value, has a circle of power, and manages work while a leader creates value, has a circle of influence, and leads people. A leader establishes vision, aligns individuals, while motivating and inspiring them to achieve the vision. A leader achieves this through three major processes:
4
1. A vision: What is to be accomplished? 2. A team: Who is to accomplish it? 3. A strategy to motivate self and team: How to accomplish it?
In healthcare, physicians and other professionals engage at various times as leaders, managers, and as followers (e.g., team members, collaborators) in a range of interpersonal relationships (e.g., work or study groups, teams, committees) and in different contexts (e.g., education, scholarship, clinical care, administration, advocacy). Some leadership traits, skills and behaviors are already ingrained at the time of entry into the field. Many others, including realizing what leadership truly means in the context of personal and professional roles, the skills to be an effective leader, and the behaviors to decide what to do and how to act on issues that matter most to oneself can be acquired by learning, role models, experiences, and reflection.
In an ever-evolving healthcare system, future practitioners must be adept at leading in environments of uncertainty and complex change. Efforts to provide
Curriculum Conceptual Framework
Framework of Emotional Intelligence as a Foundation for Relationship-Centered Leadership.
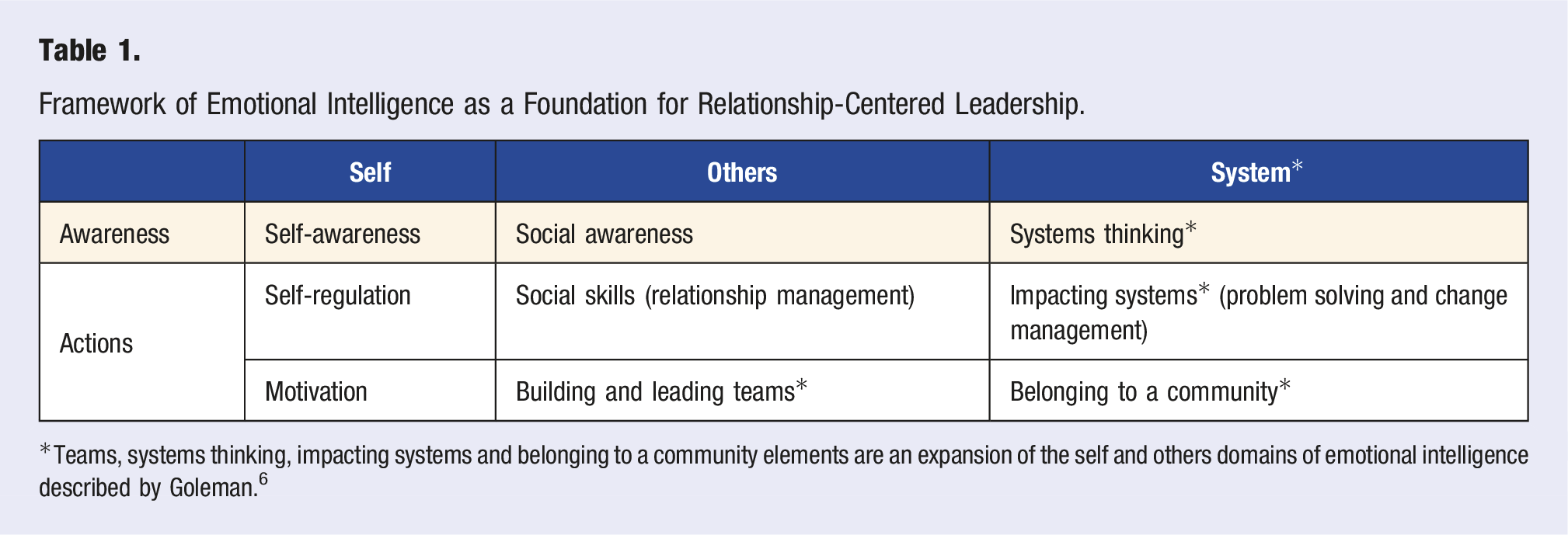
Teams, systems thinking, impacting systems and belonging to a community elements are an expansion of the self and others domains of emotional intelligence described by Goleman. 6
We refer to our framework as relationship-centered leadership that incorporates emotional intelligence and core principles of lifestyle medicine. The framework consists of three leadership domains that build sequentially and provides a sound basis for developing leadership longitudinally as medical training progresses from undergraduate to residency and practice (Figure 1): (i) being one’s best (ii) building exceptional interpersonal relationships and working in (iii) belonging to a community and impacting Relationship-centered leadership framework based on emotional intelligence.

Our framework effectively builds upon established models of leadership like situational leadership and path-goal theory. 1 Our focus is on developing oneself as a leader with strong emphasis on practicing self-care and building social connections using the pillars of lifestyle medicine to thrive long-term as a leader, follower, role model, and coach. Similarly, where teamwork literature focuses on psychological safety and accountability, 7 our model emphasizes the importance of building meaningful interpersonal relationships to build trust and manage conflict within teams in the stressful environment of healthcare. When thinking about systems improvement and change management, we emphasize social connection through engagement as a learning community defined by Wenger as a Community of Practice 8 (CoP: “a group of people who share a concern or a passion for something they do and learn how to do it better as they interact regularly”). Belonging to a CoP may also help to avoid becoming an unnecessary martyr to the cause due to loneliness, frustration, or burnout. 9 From the beginning of our curriculum, students and faculty learn with and from each other as they make meaning, solve problems, and learn through experiences and collaborative reflection.
Curriculum Program Design: Structure, Content, and Delivery
Our curriculum was co-created 10 by faculty and medical student champions using a backwards design approach, first identifying the goals, relevant conceptual frameworks, and competencies for developing medical students as leaders through literature review and structured interviews with leadership curriculum directors in leading institutions. We then used a student-led process to conduct a local needs assessment and focus groups to inform curriculum design, placement within the overall curriculum, instructional strategies, learner assessments and program evaluation.
Our curriculum aims to enable students to develop their knowledge, attitudes, and skills in the three major domains of leadership development, namely, self, teams, and systems: a. Self: Being one’s best self personally and professionally by: i. Developing one’s own leadership mission statement that aligns well with one’s personal values, professional identity, and a sense of meaning and purpose ii. Incorporating lifestyle medicine into leadership by conducting a whole health assessment, identifying actionable areas (in the pillars of healthful eating, activity, sleep, managing stress, forming and maintaining relationships, avoiding risky substances), and setting Specific, Measurable, Achievable, Relevant, Time-bound (SMART) goals to work on during the program b. Interpersonal and Teams: i. Navigating interpersonal relationships by developing emotional intelligence skills in the self and relationship domains (e.g., self-awareness, self-regulation, empathy, relationship management) ii. Working effectively in teams by demonstrating the skills necessary to be an effective member and leader of a team, building high performing teams characterized by a culture of psychological safety and effective decision-making
7
iii. Developing communication skills (active listening, speaking, writing) and applying feedback, negotiation, and conflict resolution skills c. Systems: Impacting systems by i. Developing systems thinking and problem solving skills through identification of health systems components and developing a toolkit for impacting health systems using change management, high-value care, and advocacy ii. Belonging to a learning community (CoP) dedicated to leadership development in medical training and bringing about change in medical education
The foundational preclinical course is delivered in a small group setting weekly for two-to three-hour long sessions over 16 weeks for a full semester. The course intentionally applies adult learning theory 11 using the full learning cycle: (1) learn core concepts and principles, (2) use guided initial practice, (3) reinforce with hands-on, realistic practice, (4) reflect on learning, feelings, insights, future learning, (5) give, receive, and use feedback for continued learning.
Teaching methods include case studies, workshops, guest faculty and student role models, movies, simulations, book clubs, reflections, and one-on-one coaching by students who are course alumni. Early in the curriculum, an entire session is devoted to incorporating lifestyle medicine principles to leading oneself. This includes formulating one’s mission statement, conducting a whole health assessment, identifying actionable areas and developing SMART goals. Students also interact with lifestyle medicine role models who share their stories on discovering meaning and purpose and how they have stayed authentic to their life stories when making professional choices. An end-of-course “Taste of Lifestyle Medicine” celebration marks the transition from a student in training to course alumni ready to coach incoming junior students in the next course iteration. Emphasis on building a learning community among course students, alumni, and faculty expands support networks and enhances a culture of psychological safety. Course alumni continue their leadership development through an elective in their final year of medical school encompassing monthly knowledge and reflection sessions with a team project. Building a CoP of students and faculty within the institution facilitates application of relationship-centered leadership in improving personal well-being, developing each other and professional practice.
Curriculum Evaluation
To evaluate the curriculum, we designed a multi-dimensional program evaluation for formative and summative purposes. A full description of methods and results are beyond the scope and purpose of this article. Therefore, we focus here on the pre-post student self-assessment questionnaire (24 items targeting course competencies in the self, teams and systems domains of leadership, 5-point Likert scale: 1 = strongly disagree to 5 = strongly agree) and the student narrative responses in course closing reflection activity specific to leadership and lifestyle medicine principles within the course context. Standard data screening procedures and reliability estimates were used prior to applying paired t-test statistical analysis. Descriptive statistics included means and statistical significance was set at an alpha level of .05.
Student narrative responses from end-of-course reflection activity and student-led debriefing sessions were examined to further understand students’ key takeaways in the self, teams and systems domains of the course, and whether and how they applied what was learned to activities outside of the course.
Results
Results are reported for all students completing the first two course implementations (n = 19, 100% response). All three leadership domain subscales demonstrated good reliability (Cronbach’s alphas: self = .82, team = .81, system = .90). As seen in Figure 2, in comparing pre- and post-course self-evaluations on a 5-point Likert scale, students reported increased confidence in performing competencies in self (3.12 vs 4.20, P < .001), team (3.06 vs 4.00, P < .001), and systems (2.55 vs 3.55, P < .001) domains. Students self-assessment competency scores across 3 leadership domains. Students self-assessed their competencies on a Likert 5-point scale across three leadership domains (Self, Team, and System). The mean scores are shown ± standard error. Blue corresponds to pre-course scores; green corresponds to post-course scores.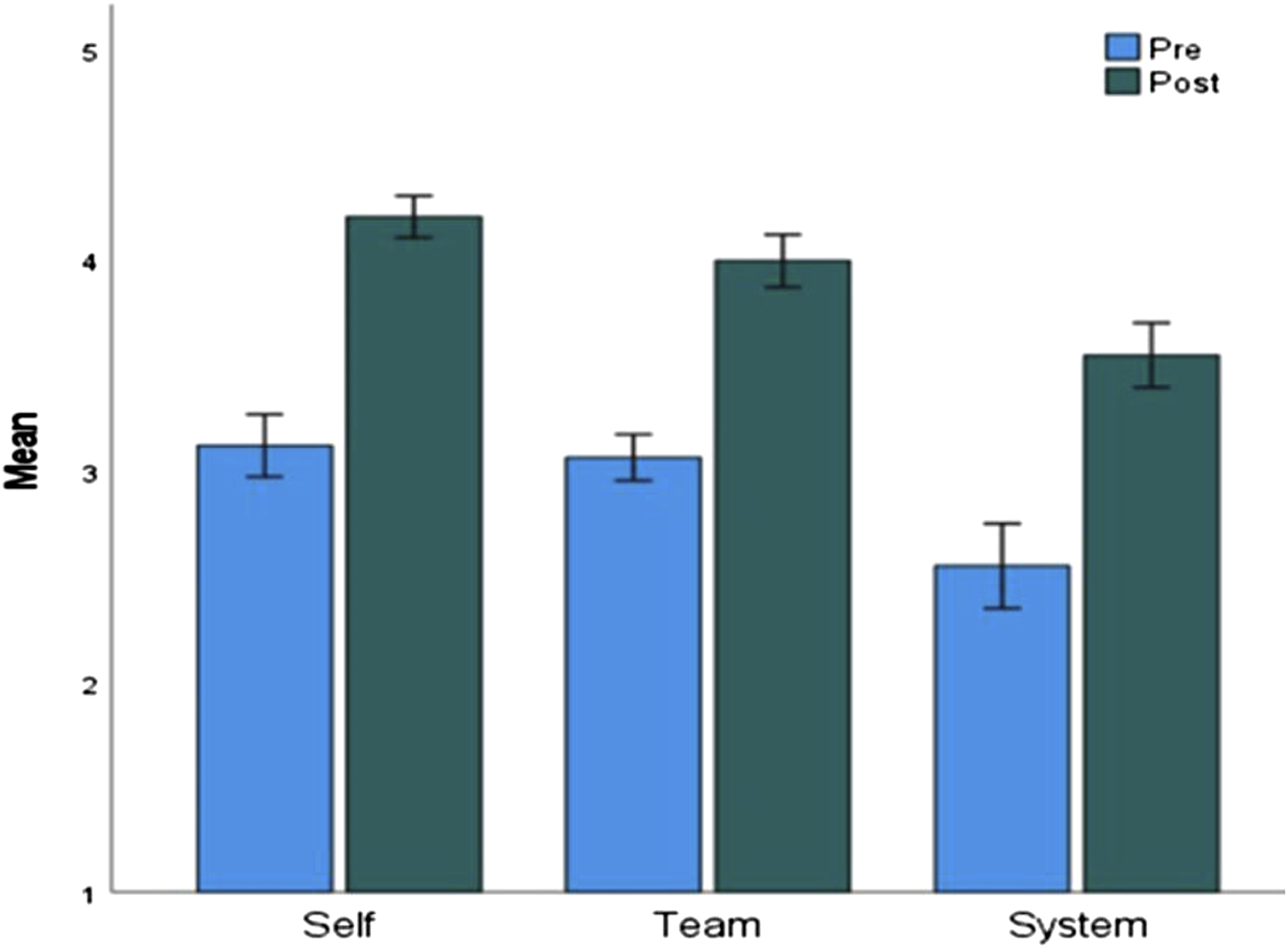
Reviews of post-course qualitative reflections revealed that a vital strength of the course was its direct relevance and immediate applicability to students’ ongoing daily activities across multiple environments, such as personal wellness and relationships, interest group leadership roles, and team-based learning activities. All students agreed the course impacted their behaviors outside the course and reflected on using behaviors or skills learned during the course in small groups or team-based activities or in modifying their own lifestyle. Selected representative quotes from closing reflections are included to illustrate examples of relationship-centered leadership from the course (each quote is labeled by domain of leadership and core principles in leadership and lifestyle medicine in parenthesis): “Take care of yourself so you can take care of others… I think that our conversations surrounding Lifestyle Medicine were a spark that had me thinking more about what it means to both care for ourselves holistically and care for our patients holistically.” (self; lifestyle medicine) “I think that because of this course, I am able to be more deliberate and self-aware in my relationships, teams, and organizations. A big portion of this class consisted of sharing your individual perspective, which is something that I was not necessarily comfortable with or accustomed to at the beginning of the course. Through the course, I became a lot more comfortable with my own voice and perspective.” (self, teams; emotional intelligence) “In my mission statement, I included my relationships with my parents, sisters, partner, and patients. While my mission statement will be evolving as I grow older and gain more insightful and powerful experiences, I do think that I will check in on myself and think to myself, are my actions consistent with the mission I want for myself? At the end of the day, I want to ensure that my actions are true to myself and my values.” (self, interpersonal; lifestyle medicine and leadership) “Trust in your teammates and in your methods. While there may be room for improvement, have faith that you will achieve success if everyone has the same mentality and supports one another.” (teams; CoP) “Build with others – remember you are part of a larger team in medicine, and you can always reach out and learn from others.” (teams, systems; CoP) “Take time to connect with others – building your network can help you grow and envision where you want to be in the future and who you want to be.” (teams, systems; CoP) “Some of my most memorable interactions with fellow students occurred in this class. I had the opportunity to get to know my peers in a different way and learn from their experiences.” (interpersonal; CoP) “Know that you are part of a larger system and can use this to continue to learn and gain confidence from the experiences of others.” (self, systems; CoP) “After this course, I think I’ve realized that changing the system can come in many ways, and that you can contribute towards change in smaller ways, with the help of a team, or as a follower. Making a difference doesn’t always come at the expense of personal well-being.” (self, systems; lifestyle medicine) “Overall, I feel less overwhelmed, and more confident in myself. One way in which I feel more confident is in my ability to lead specific change in the healthcare system. Prior, I often felt as though there was so much that needed to change, and I had no idea where to begin or how. Now, I feel that I can actually initiate change. Having a framework of how to approach leading change while belonging to a community of like-minded individuals contributed to that increased confidence.” (self, systems; lifestyle medicine, emotional intelligence, CoP)
Ongoing engagement with course alumni serving as coaches to current students revealed these interactions helped them feel like valued members of the community. Beyond contributing to the learning and well-being of juniors, they were developing their own coaching skills by serving in these roles and felt more likely to offer and ask for help because of this service to the CoP.
Discussion
Lessons Learned From Leadership Curriculum Development
We describe key lessons learned from our experience developing a leadership curriculum for medical students founded in the novel framework of relationship-centered leadership and incorporating various aspects of lifestyle medicine. 1. Our curriculum and outcomes demonstrate that leadership competencies can be developed early during medical training and adult learners are keen to apply these skills right away to their personal and professional lives. 2. A relationship-centered leadership framework within the context of a CoP facilitates a psychologically safe learning environment by allowing participants to be vulnerable as they build trust with each other and show up as their real self, guided by their core values and mission. 3. These curriculum design features, along with the intentional incorporation of sessions focused on lifestyle medicine, may further explain the perceived positive impact on personal wellness and relationships noted by students at course conclusion. Importantly, this holistic approach to leadership development may have the potential to reduce stress and burnout long-term.
Leadership Curriculum Development Principles Applicable to the LM Community
Some of the lessons learned from medical student curriculum development are generalizable to lifestyle medicine practitioners. While it is ideal to begin developing leadership skills early in medical training, the reality is that most practitioners do not receive any formal leadership or teamwork training in their undergraduate or graduate medical education. These key principles can be useful to keep in mind when developing continuing medical education programs for lifestyle medicine practitioners. 1. All lifestyle medicine practitioners are leaders; the need for leadership development applies to all and highlights a tremendous gap in currently available educational offerings within lifestyle medicine forums. Needs assessment surveys of members can be helpful in identifying this gap, and in finding out the skills and competencies, as well as learning methodologies members need to develop these skills. 2. The key domains of relationship-centered leadership are self, teams, and systems—any leadership development needs to incorporate skill building in all three domains, ideally in this sequence such that participants can use self and social awareness to build better teams and meaningfully impact systems together. 3. Role of experiential learning in a supportive Community of Practice (CoP)—Leadership development needs to be longitudinal and experiential to allow for knowledge acquisition, skill development, application, and reflection over a variety of experiences. Belonging to a CoP allows for a safe space, network effects, and social learning for collective problem solving, peer coaching and support, and celebrating small wins and even bearing losses together to stay alive in the demanding and risky practice of leadership.
Leadership is ultimately about the work of leading, not innate leadership abilities or the development of tools of the toolkit. Anecdotally, many lifestyle medicine practitioners are drawn to this field after leaning into their own experiences of burnout and may benefit from organizational and community support when embarking on risky leadership journeys in a system resistant to change. Existing communities of practice in lifestyle medicine focused organizations are promising forums in this regard and can be leveraged for leadership development.
Future Plans
We are guided by our original vision of: (1) identifying what competencies are most essential for medical students to be their best self personally and professionally, build meaningful relationships, lead teams, and impact the system while belonging to a community of practice; and (2) developing and implementing curriculum to develop those competencies in the most efficient and effective way.
Our relationship-centered leadership curriculum has expanded from an elective taught in the fall semester of second year of medical school, to a longitudinal elective program beginning in the first year of medical school with the opportunity to continue in the CoP throughout medical training culminating in a reflective, collective experience that runs throughout the final year of training.
While identifying space within the medical school core curriculum remains challenging, students and course directors alike are most receptive to curricular change when relationship-centered leadership curriculum is integrated into the existing events in medical training allowing participants to be more engaged, effective, and less stressed in their personal and professional roles. Events such as practice-based learning, team-based learning, and student interest groups are areas where task-focused structure can be improved by intentionally setting the stage with relationship-centered frameworks that build interpersonal relationships and teams while accomplishing shared goals.
Conclusion
Relationship-centered leadership is not about pursuing a task, title, position, or reward, it is about being your best self personally and professionally, building meaningful interpersonal relationships, working in teams, belonging to a community, and impacting systems in areas that matter most to oneself.
Our medical student leadership curriculum shows encouraging results from multiple angles that developing these competencies is possible and leads to direct and immediate impacts in personal and professional roles and relationships. Relationship-centered leadership in healthcare is a relatively novel concept that will only benefit from further refinement in concept, program design and assessment as it is applied to broader contexts. Its strength lies in its integration of emotional intelligence with principles of lifestyle medicine and its potential for improving the effectiveness and well-being of leaders and followers, their relationships, teams, communities, and systems.
Footnotes
Acknowledgments
We are indebted to the course participants for their dedication and time with the pilot Leadership for Medical Students curriculum and would further like to express our gratitude towards the supporting course faculty: Dr Ilene Rosenberg, Dr Lisa Coplit, Dr Listy Thomas and Dr Lyuba Konopasek.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author RA has had equity ownership in the following companies in the last 24 months (but does not have any financial conflict related to this publication): Moderna, Regeneron, Paratek, Aurinia, Progyny.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Albert Schweitzer Institute at Quinnipiac University and the AIMES grant at Frank H. Netter MD School of Medicine at Quinnipiac University.
Ethical approval
This project Leadership for medical students curriculum development, protocol #10219 has been approved by Quinnipiac University Institutional Review Board