
Abstract
Understanding how lifestyle factors impact psychiatric well-being is essential for supporting recovery in COVID-19 survivors, yet their influence on long-term outcomes remains underexplored. This cross-sectional study evaluates associations between depression, generalized anxiety disorder (GAD), post-traumatic stress disorder (PTSD), suicidal ideation (SI), and syndromic common mental disorder (CMD) with lifestyle factors in 730 moderate to severe COVID-19 survivors. Lifestyle factors included physical activity, alcohol and substance use and during COVID-19 infection, and dietary intake, with assessments conducted 6 to 11 months post-hospitalization. Multiple logistic regression was employed for each of the five dependent variables. Of the participants, 51.9% were male, with a mean age of 55. Previous COVID-19 sedative use and the severity of alcohol use were correlated with increased depression (sedative, OR = 2.43, P = .011; alcohol OR = 1.09, P = .017), GAD (sedative, OR = 2.13, P = .007; alcohol OR = 1.08, P = .009), PTSD (sedative, OR = 2.10, P = .008; alcohol OR = 1.08, P = .004), and sedative for CMD (OR = 1.97, P = .005). Opioid use was linked to increased GAD (OR = 2.23, P = .042), and “fruits and vegetables” consumption 2-3 times/week was associated with lower odds for depression (OR = 0.19, P = .021). No lifestyle behaviors were found to be associated with suicidal ideation. These results underscore the importance of lifestyle-specific behaviors in mitigating psychiatric symptoms during the extended recovery period from COVID-19. This is particularly pertinent with respect to minimizing the consumption of sedatives and alcohol in the context of depression, GAD, and PTSD, as well as the use of opioids for GAD and the increased intake of fruits and vegetables to depression. These findings may have substantial implications for the formulation of lifestyle strategies aimed at the prevention of mental health disorders subsequent to severe acute viral infections.
Introduction
Symptoms persisting for 12 weeks or longer after recovery from SARS-CoV-2 infection have been recognized as “long COVID.” 1 Among its most common manifestations are fatigue, dyspnea, sleep disturbances, and cognitive and psychiatric symptoms. 2 Psychiatric conditions are particularly prevalent in long COVID, with a systematic review reporting depression in approximately 32% and anxiety in 29% of affected individuals. 3 Longitudinal studies further underscore the mental health burden, with 22.5% of ICU survivors experiencing post-traumatic stress 6 months post-hospitalization 4 and 6.7% of patients with long COVID reporting suicidal ideation 17 months after their initial infection. 5 This highlights the significant and enduring psychiatric challenges faced by individuals recovering from COVID-19.
Pre-pandemic research supports the critical role of lifestyle factors in mental health. High-quality diets, such as the Mediterranean diet, have been associated with lower risks of depression through their anti-inflammatory and neuroprotective effects,6-9 mainly driven by the high concentration of polyphenols. 10 Regular physical activity is also linked to improved psychological outcomes and represents a modifiable factor with therapeutic potential.11,12 In contrast, substance use, including alcohol and opioids, has been associated with suicide risk. 13 Although these associations are well-established, most COVID-19-related studies have focused on short-term impacts of lifestyle habits, such as immediate psychological distress or symptom exacerbation during the pandemic.
Lifestyle behaviors prior to infection appear to play a protective role in mitigating these outcomes. Higher adherence to healthy lifestyle habits—such as engaging in at least 150 minutes per week of moderate to vigorous physical activity, maintaining a balanced diet, and obtaining 7 to 9 hours of sleep—was associated with lower odds of long COVID symptoms in a dose-dependent manner. 14 A recent meta-analysis underscores that significant disruptions in daily routines during the pandemic—including irregular physical activity, eating patterns, disrupted sleep, and reduced social and leisure activities—were associated with heightened psychological distress, anxiety, and depression. 15 Additionally, alcohol and drug use rose significantly during the pandemic, 16 often as coping mechanisms for stress and emotional challenges, further exacerbating psychiatric vulnerabilities. 17
Previous research within our study cohort demonstrated that physical inactivity was associated with persistent COVID-19 symptoms, including memory impairments, depression, anxiety, and loss of taste and smell. 18 Expanding our work, this study examines a broader range of lifestyle factors—substance use, dietary habits, smoking, and physical activity—as predictors of five psychiatric outcomes: depression, generalized anxiety disorder (GAD), syndromic common mental disorder (CMD), post-traumatic stress disorder (PTSD), and suicidal ideation (SI) in individuals with long COVID. Using a multivariate regression framework, this work aims to address critical research gaps and provide actionable insights to guide interventions targeting the long-term mental health burden of COVID-19.
Methods
Study Design and Population
This research is derived from a cohort study conducted at the Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (HCFMUSP). The hospital focuses on treating moderate to severe COVID-19 cases, particularly during the pandemic’s onset. Moderate cases were defined by the need for hospital care, while severe cases required intensive care unit (ICU) support. The establishment of the “HCFMUSP post-COVID-19 cohort” facilitates research on long-term medical, functional, and neuropsychiatric effects of moderate and severe COVID-19 in adults and older individuals. 19 A comprehensive description of our methodology, along with an accompanying flowchart, is detailed in Busatto et al. 20 Research protocol was approved by the Ethics Committee at HCFMUSP (Capes-HC) and is registered at the Brazilian Registry of Clinical Trials (ReBEC) under the registration number 4.270.242 (RBR-8z7v5wc). All participants provided informed consent before being enrolled in the study.
Eligible participants were patients hospitalized at HCFMUSP for at least 24 hours with moderate or severe COVID-19 between March 30 and August 30, 2020, during the height of the initial wave of the pandemic in Brazil, when HCFMUSP functioned as a fully dedicated facility for COVID-19 treatment. For the present study, participants were excluded if they did not complete neuropsychiatric assessments 7 to 11 months after hospitalization, were reinfected during follow-up based on clinical signs and symptoms suggestive of SARS-CoV-2 reinfection, or had incomplete data on psychiatric outcomes due to the inability to compute results on the CIS-R. Reporting will conform to The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement. 21
Assessment Protocol and Data Collection
Hospital records and databases were utilized to obtain clinical and sociodemographic data, including hospitalization length, ICU care duration, the need for orotracheal intubation, smoking status, and the severity of acute illness as classified by the World Health Organization (WHO) criteria. 22 Participants’ socioeconomic status was categorized according to the Brazilian Association of Research Companies (ABEP) 23 score and classification, which assign households to categories from Class A (highest) to Class E (lowest) based on household characteristics and ownership of consumer goods.
Follow-up in-person assessments were conducted by a team of trained psychiatrists, neuropsychologists, and medical students. These evaluations, which included questionnaires on psychiatric outcomes, lifestyle factors, and overall well-being, were administered approximately 6 months after hospitalization (mean of 6.9 months; range 1.3 to 12.3 months). The Clinical Interview Schedule-Revised (CIS-R), 24 a structured instrument that assesses 14 psychiatric diagnoses, was used to diagnose syndromic common mental disorder (CMD), generalized anxiety disorder (GAD), and depression. According to CIS-R, syndromic CMD (named below only as CMD) is the sum of 12 or more symptoms irrespective of diagnosis. We utilized this as a distinct entity to encompass a group of individuals not classified under other diagnoses yet still experiencing functional impairment related to symptoms. The psychiatric assessment also included an adapted version of the Ask Suicide-Screening Questions (ASQ), 25 which evaluated suicidal ideation using the third question: “In the past 4 weeks, have you had thoughts of killing yourself?” Responses were categorized as never, rarely, frequently, or very frequently/daily. Post-traumatic stress disorder (PTSD) was evaluated utilizing the Post-Traumatic Stress Disorder Checklist (PCL-C). 26 Raters assigned scores to symptoms contingent upon the participants’ disclosures regarding the extent to which they were affected over the preceding month while only accounting for symptoms that emerged subsequent to the onset of the COVID-19 infection.
Physical activity levels were measured using the International Physical Activity Questionnaire (IPAQ). 27 The Alcohol Use Disorder Identification Test (AUDIT) 28 was utilized to evaluate alcohol consumption risk levels, with scores ranging from 0 to 40, where higher scores suggest a possible dependence. Dietary habits and substance use were assessed through targeted interview questions, detailed in the Supplemental Material. For dietary habits, participants reported the frequency of their consumption over the past 12 months of meat, processed meat, fish, chicken, pork, and “fruits and vegetables,” with responses categorized as never, once a week, two to three times a week, once a day and more than once a day. Comparisons were made between frequency categories within this same 12-month period.
Statistical Analysis
Statistical analyses were conducted using Stata. 29 The patient cohort was described using frequencies, means, and standard deviations for demographic and clinical variables. The psychiatric outcomes assessed included depression, CMD, GAD, PTSD, and suicidal ideation. Diagnoses were based on the criteria and questionnaires described in the “Assessment and Data Collection” section. For suicidal ideation, comparisons were made between individuals with and without suicidal thoughts.
The lifestyle variables included in the analysis were: (1) physical activity levels as measured by IPAQ; (2) substance use, including cannabis, tobacco, opioids (tramadol, morphine, codeine, heroin), sedatives—calming medications or sleep aids like benzodiazepines or Z-drugs—and the AUDIT score for alcohol consumption; and (3) dietary intake, the frequency of consumption of meat (referring to any type, including red meat, pork, chicken, and fish), red meat, processed meat (e.g., sausage, ham, salami), pork, fish, chicken, and “fruits and vegetables.” Each substance’s usage and dietary variables were examined independently for correlations with psychiatric outcomes. Sedative and opioid use was assessed based on participant-reported use before and after COVID-19 hospitalization, without distinguishing between prescribed and non-prescribed use. Questionnaire variables with fewer than 10 responses were aggregated to improve events per variable and reduce bias. 30 Lifestyle variables were selected due to their established links to depression, anxiety, PTSD, and suicidal ideation in prior studies, underscoring their theoretical relevance to long COVID.31-33
We performed a selection of lifestyle variables for inclusion in the models using univariate tests for each psychiatric outcome using a P-value threshold of 0.2. This threshold was to avoid prematurely excluding variables that may be relevant in this exploratory analysis. 34 Collinearity was assessed using Variance Inflation Factor (VIF), and predictors with VIF ≥10 were excluded. Multiple logistic regression models were employed to jointly assess the association between lifestyle factors and each psychiatric outcome. The models were adjusted for the potential confounders: age, sex, WHO severity classification, BMI at admission, and ABEP score. To control for the false discovery rate and to reduce the risk of Type 1 errors associated with multiple comparisons, the Benjamini-Hochberg (BH) correction was applied to the P-values generated in the multiple logistic regression models.
Results
A total of 730 participants were included in the multivariable analysis. The average age was 55 years, and participants were predominantly male (51.9%). In terms of ethnicity, most participants identified as white (65.3%), followed by brown (23.3%), black (7.8%), and yellow (0.4%). The largest proportion of our sample, 32.5%, belongs to Class C1 of the ABEP classification. This class represents a middle socioeconomic segment in Brazil, typically including families that are somewhat comfortable economically but not affluent. The mean ABEP score was 25.14 (SD: 8.09), ranging from 7 (lower socioeconomic status) to 65 (higher socioeconomic status). The mean duration of hospitalization in our sample was 17.49 (SD: 18.99), with 53.6% of the patients requiring intensive care. Additionally, 40.9% underwent orotracheal intubation, with a mean duration of 10.8 days, and 41% were classified as having the highest clinical severity during the acute phase, according to WHO criteria. Moreover, 39.2% were sedentary according to IPAQ classification.
Regarding dietary habits, 95.9% of the sample reported no dietary restrictions. In general, 87.8% of participants reported consuming meat (referring to any type, including red meat, pork, chicken, and fish) two or more days per week, and 53.5% reported avoiding processed meat. Additionally, about 73% of respondents stated that they ate fruits and vegetables at least once daily.
The mean AUDIT score was 1.55 (SD: 3.41), indicating low-risk alcohol consumption according to WHO guidelines. Among participants, 94% reported no previous use of opioids, including tramadol, morphine, codeine, or heroin. Additionally, 95% were identified as non-current smokers, although 22% reported previous smoking. Furthermore, 17% had a history of sedative use (i.e., calming medications or sleep aids like benzodiazepines or Z-drugs) prior to hospitalization. Lastly, 97% of participants stated they had never used cannabis before their COVID-19 hospitalization. In our sample, the prevalence of psychiatric diagnoses was 7.26% for depression, 14.79% for generalized anxiety disorder, 29.86% for CMD, and 14.52% for PTSD. Notably, 15.06% of patients had two or more diagnoses, according to the CIS-R, and 6.1% of participants reported suicidal ideation.
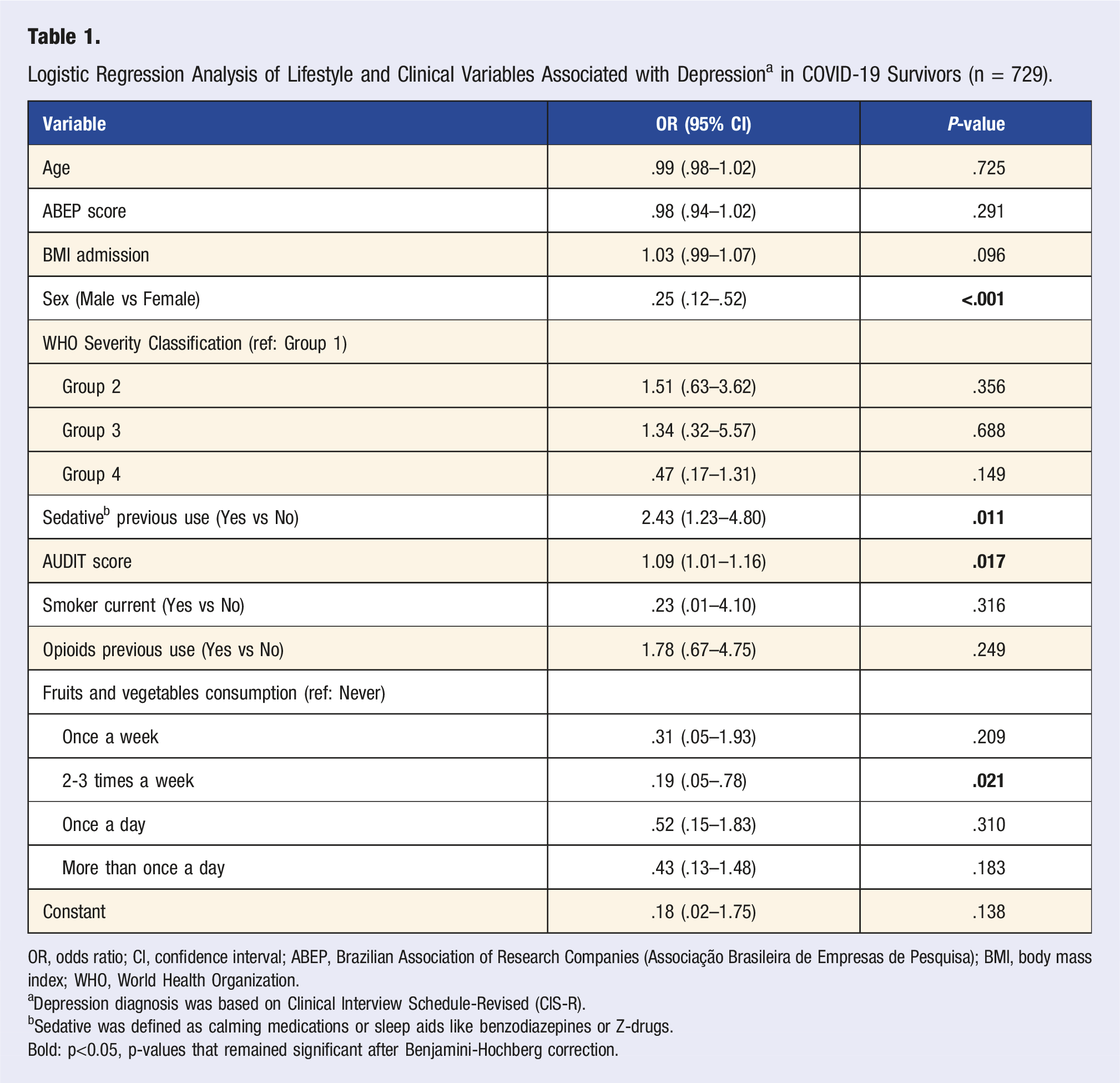
Logistic Regression Analysis of Lifestyle and Clinical Variables Associated with Depression a in COVID-19 Survivors (n = 729).
OR, odds ratio; CI, confidence interval; ABEP, Brazilian Association of Research Companies (Associação Brasileira de Empresas de Pesquisa); BMI, body mass index; WHO, World Health Organization.
aDepression diagnosis was based on Clinical Interview Schedule-Revised (CIS-R).
bSedative was defined as calming medications or sleep aids like benzodiazepines or Z-drugs.
Bold: p<0.05, p-values that remained significant after Benjamini-Hochberg correction.
Table 1 displays the regression analysis of the associations between lifestyle measures and depression. Previous use of sedative substances was associated with 2.43 times higher odds of depression (OR = 2.43 [95% CI 1.23-4.80], P = .011), and higher alcohol consumption also reaching significance (OR = 1.09 [95% CI 1.01-1.16], P = .017). For dietary habits, consuming fruits and vegetables 2-3 times a week was associated with an 81% reduction in odds of depression compared to those not consuming them in the last 12 months (OR = 0.19 [95% CI .05–.78], P = .021). Sex was the only covariate that demonstrated a significant association and the only variable that remained significant after adjustment for multiple comparisons, with males exhibiting significantly lower odds of depression (OR = 0.25 [95% CI .12–.52], P < .001).
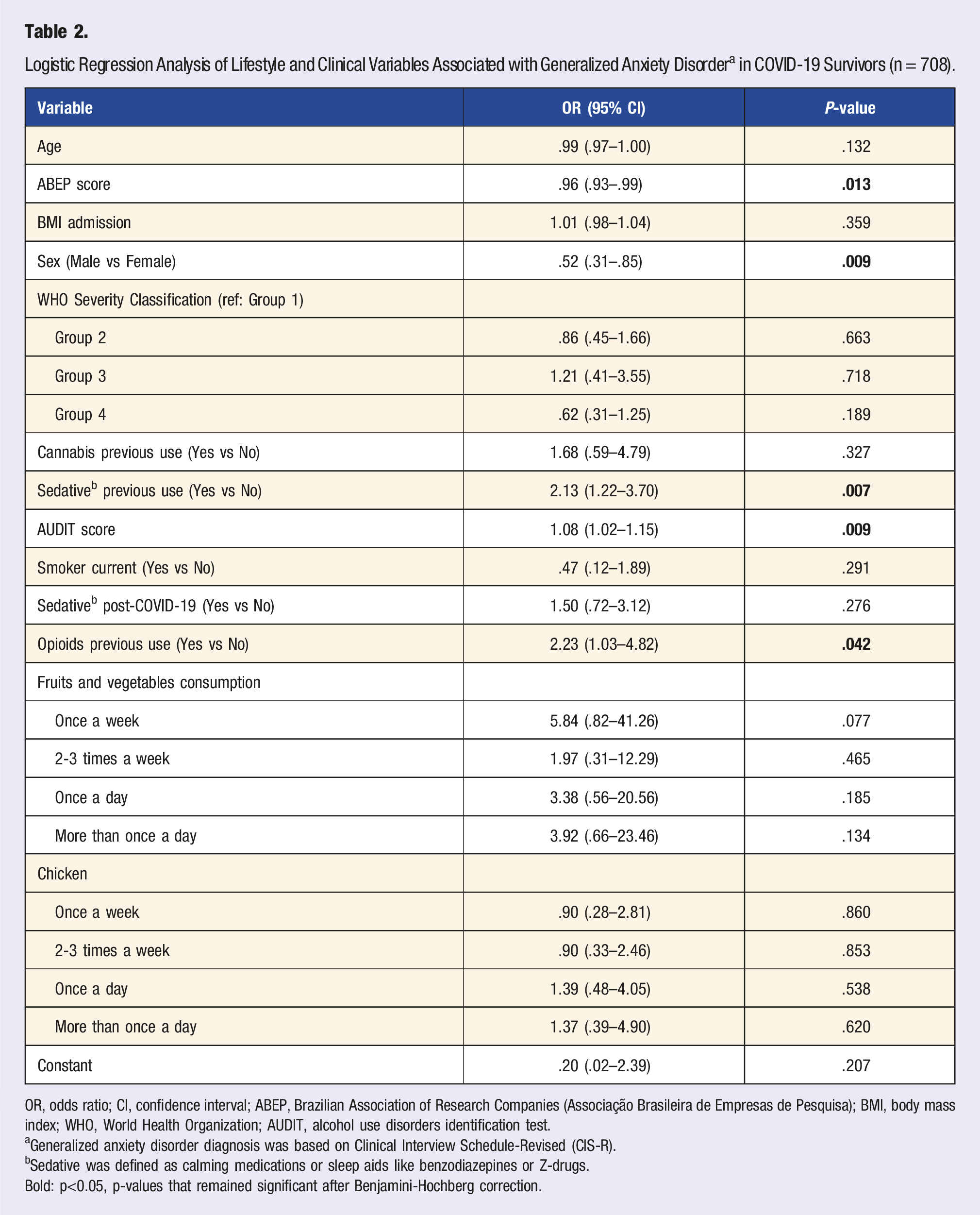
Logistic Regression Analysis of Lifestyle and Clinical Variables Associated with Generalized Anxiety Disorder a in COVID-19 Survivors (n = 708).
OR, odds ratio; CI, confidence interval; ABEP, Brazilian Association of Research Companies (Associação Brasileira de Empresas de Pesquisa); BMI, body mass index; WHO, World Health Organization; AUDIT, alcohol use disorders identification test.
aGeneralized anxiety disorder diagnosis was based on Clinical Interview Schedule-Revised (CIS-R).
bSedative was defined as calming medications or sleep aids like benzodiazepines or Z-drugs.
Bold: p<0.05, p-values that remained significant after Benjamini-Hochberg correction.
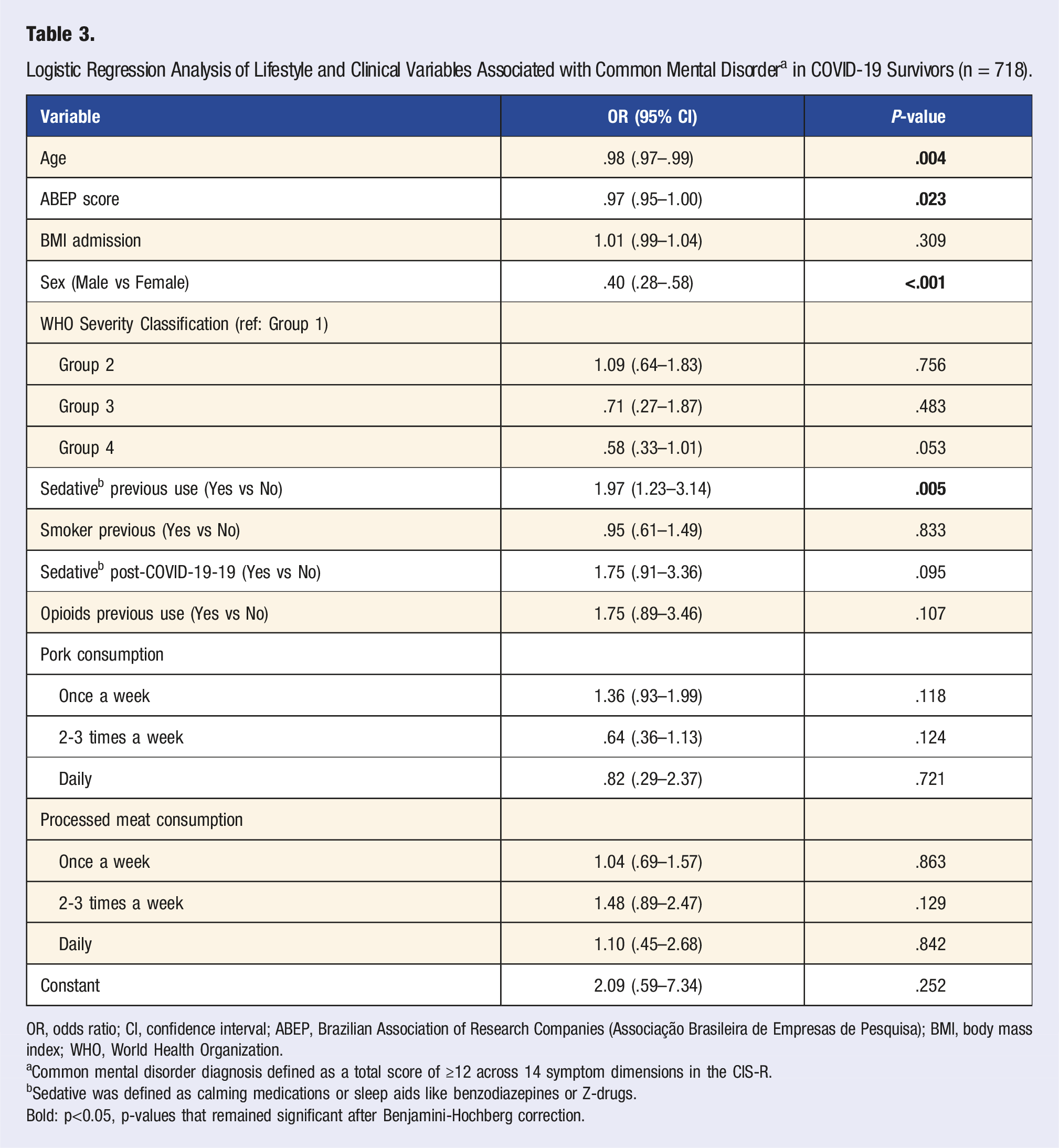
Logistic Regression Analysis of Lifestyle and Clinical Variables Associated with Common Mental Disorder a in COVID-19 Survivors (n = 718).
OR, odds ratio; CI, confidence interval; ABEP, Brazilian Association of Research Companies (Associação Brasileira de Empresas de Pesquisa); BMI, body mass index; WHO, World Health Organization.
aCommon mental disorder diagnosis defined as a total score of ≥12 across 14 symptom dimensions in the CIS-R.
bSedative was defined as calming medications or sleep aids like benzodiazepines or Z-drugs.
Bold: p<0.05, p-values that remained significant after Benjamini-Hochberg correction.
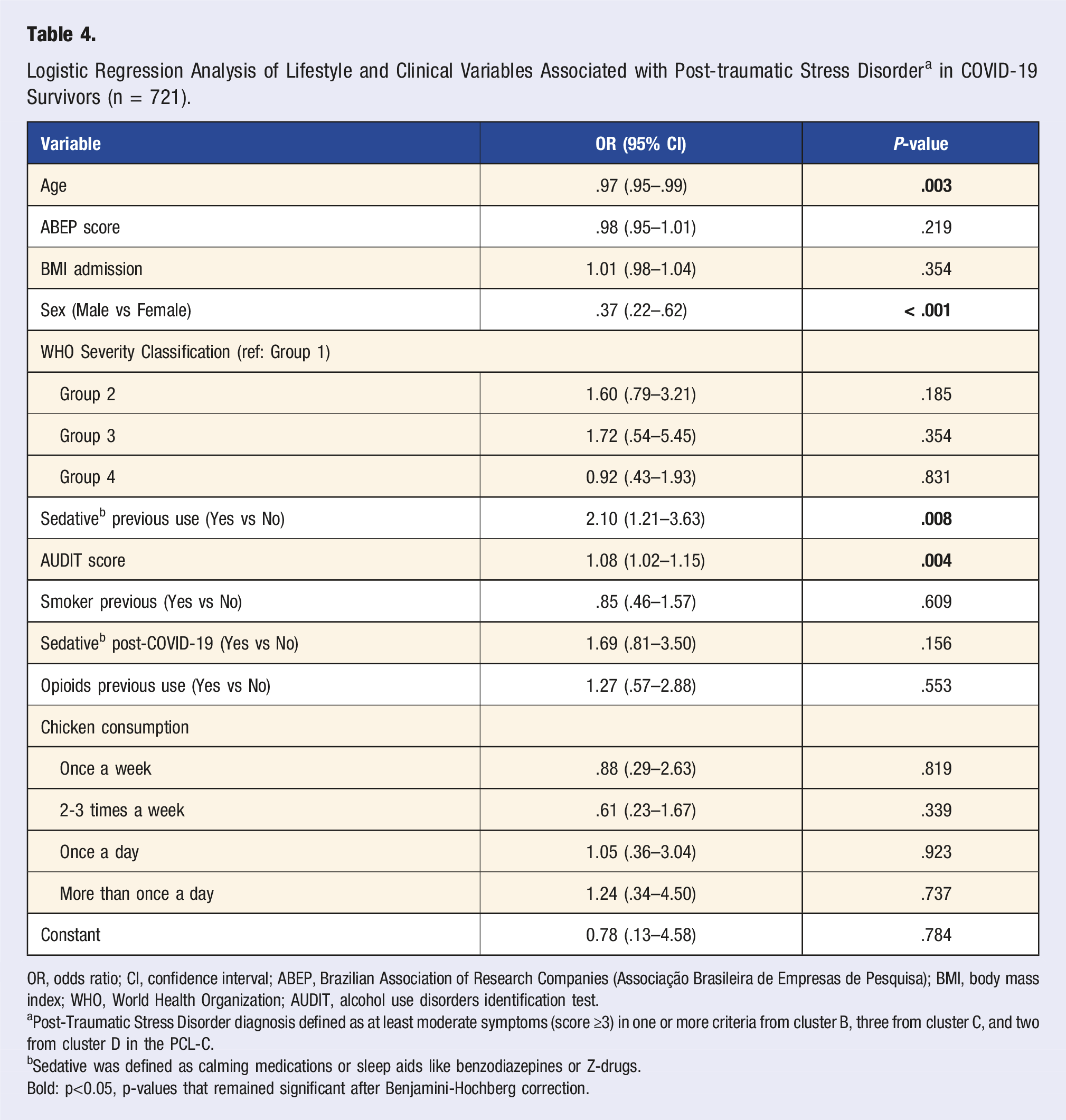
Logistic Regression Analysis of Lifestyle and Clinical Variables Associated with Post-traumatic Stress Disorder a in COVID-19 Survivors (n = 721).
OR, odds ratio; CI, confidence interval; ABEP, Brazilian Association of Research Companies (Associação Brasileira de Empresas de Pesquisa); BMI, body mass index; WHO, World Health Organization; AUDIT, alcohol use disorders identification test.
aPost-Traumatic Stress Disorder diagnosis defined as at least moderate symptoms (score ≥3) in one or more criteria from cluster B, three from cluster C, and two from cluster D in the PCL-C.
bSedative was defined as calming medications or sleep aids like benzodiazepines or Z-drugs.
Bold: p<0.05, p-values that remained significant after Benjamini-Hochberg correction.
Logistic Regression Analysis of Lifestyle and Clinical Variables Associated with Suicidal Ideation a in COVID-19 Survivors (n = 710).
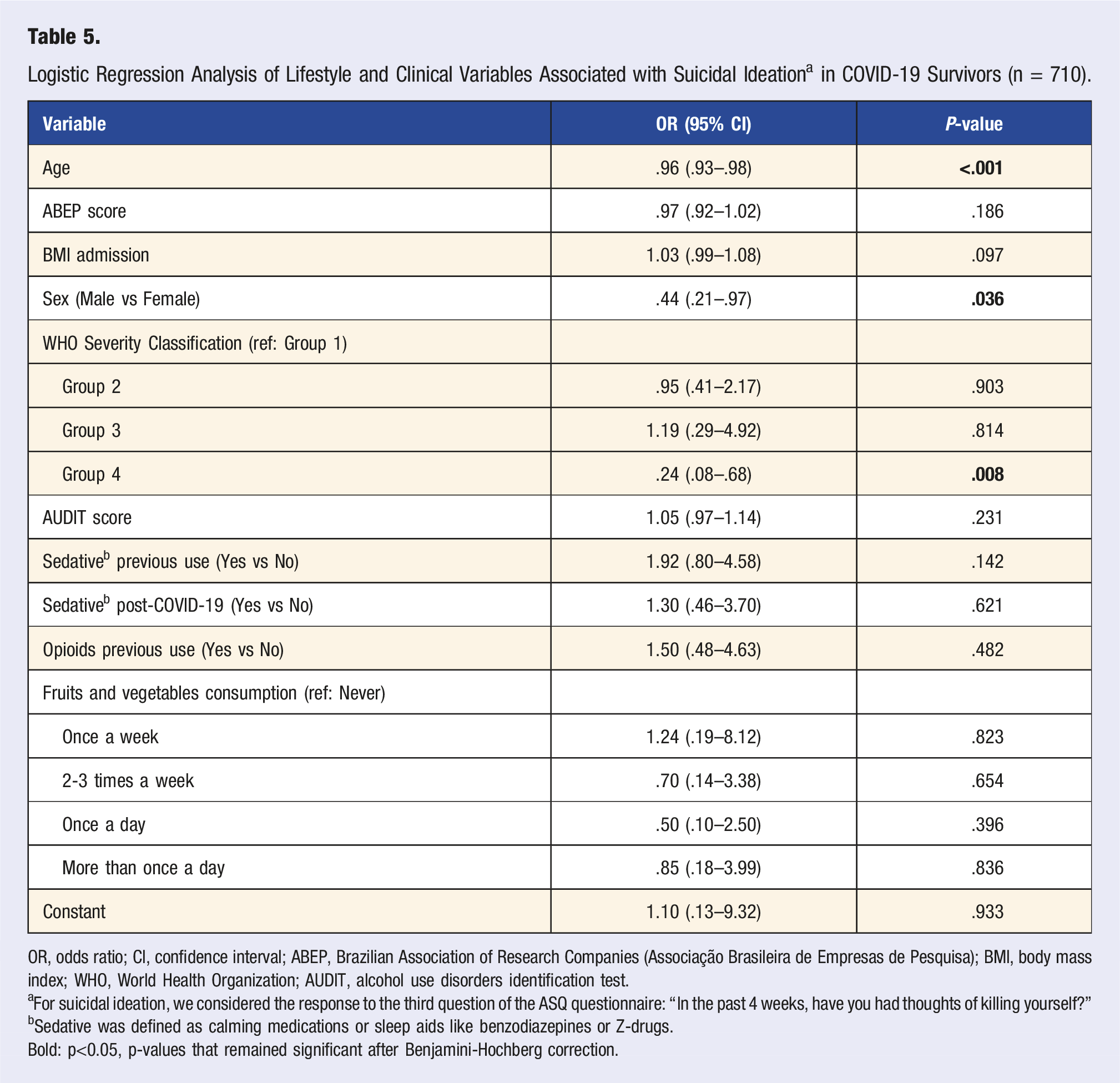
OR, odds ratio; CI, confidence interval; ABEP, Brazilian Association of Research Companies (Associação Brasileira de Empresas de Pesquisa); BMI, body mass index; WHO, World Health Organization; AUDIT, alcohol use disorders identification test.
aFor suicidal ideation, we considered the response to the third question of the ASQ questionnaire: “In the past 4 weeks, have you had thoughts of killing yourself?”
bSedative was defined as calming medications or sleep aids like benzodiazepines or Z-drugs.
Bold: p<0.05, p-values that remained significant after Benjamini-Hochberg correction.
Discussion
In this study, we investigated the relationships between lifestyle factors and psychiatric outcomes in a cohort of 730 post-COVID-19 patients 7 to 11 months after acute infection. It is noteworthy that various lifestyle factors have been correlated with the symptoms of long COVID. Our results indicated that substance use and misuse were associated with several mental health disorders in the long-term of COVID-19 infection. The use of sedatives before hospitalization due to COVID-19 was associated with more than twice the odds of depression, GAD, PTSD, and CMD. Alcohol consumption has also been linked to an increased prevalence of depression, PTSD, and GAD, and previous opioid use was associated with more than twice the odds of developing GAD. Conversely, the consumption of “fruits and vegetables” was associated with a decreased likelihood of developing depression. Following the adjustment for multiple comparisons, only previous sedative use remained significantly associated with a higher risk of PTSD and CMD, and alcohol misuse with PTSD. These results provide valuable insights into the role of lifestyle factors in psychiatric outcomes following COVID-19.
One of the primary findings of our research indicates that previous medical and non-medical usage of sedatives, such as benzodiazepines or Z-drugs, was correlated with nearly all observed outcomes. The prevalence of benzodiazepine usage identified in our study (17%) corresponds with one-year prevalence rates reported in a Brazilian longitudinal study (15%). 35 This rate is markedly higher than those documented in the United States (5.2%) 36 yet lower than the rate observed in Spain (22.3%). 37 Throughout the pandemic, there was a notable increase in the prescription of sedatives for conditions such as anxiety, depression, and sleep disturbances.38,39 Although these prescriptions may provide temporary relief, their prolonged use raises significant concerns regarding dependency and the potential exacerbation of psychiatric conditions.40,41 Misuse of sedatives, particularly among populations with histories of abuse or dependence, has been linked to an increase in agoraphobia, panic symptoms, 42 and also a higher risk for developing mood and substance use disorder. 43 The robust associations identified within our study suggest that previous sedative usage may act as both an indicator of pre-existing mental health conditions and a contributing factor to psychiatric outcomes post-COVID-19.44,45 This dual role underscores the necessity for diligent monitoring and deprescribing strategies to alleviate the risks associated with long-term sedative use, thereby positioning sedative misuse as a critical target for intervention to facilitate psychiatric recovery in individuals suffering from long-term COVID-19 syndrome.
Our study revealed a significant association between increased AUDIT scores, reflecting more severe alcohol use, with depression, GAD, and PTSD. This is in line with several studies pointing out a bi-directional association between alcohol abuse and depressive and anxiety disorders. While higher alcohol intake increases the likelihood of developing depressive symptoms, 46 it can also precipitate heavier drinking habits. 47 Less quality data is seen for anxiety-related disorders, possibly due to the paucity of research regarding this topic. 48 For PTSD, studies have shown that individuals might use the substance as a coping behavior, in a hypothesis called “self-medication.” 49 Moreover, alcohol misuse exacerbates PTSD symptoms by disrupting emotional regulation and reinforcing avoidance behaviors, hindering treatment progress. 50 Even though our sample demonstrated a low use of alcohol in general, our data pointing to these individuals with a more heavy drinking behavior might also be explained to the lockdown, where, for some individuals, substance use increased driven by boredom, loss of daily structure, and loneliness. 51 This use pattern heightened anxiety, depression, and loneliness during the COVID-19 pandemic. 52 Therefore, routine screening for alcohol consumption in individuals with severe clinical illnesses could be particularly beneficial in individuals with long COVID conditions.
Opioid use was associated with 2.23 higher odds of GAD, though this did not remain significant after adjustment for multiple comparisons. Our sample reported very low opioid consumption, with 94% of participants indicating no use, consistent with Brazil’s mid-level opioid consumption. 53 These findings may not be generalizable to populations with higher opioid use prevalence, such as the U.S., where there was a significant increase in opioid-related emergency service utilization and overdose rates during the pandemic, 54 raising concerns about potential consequences in the context of the post-pandemic era.
Regarding dietary habits, our analyses revealed that participants who consumed fruits and vegetables regularly (2-3 times per week) had lower odds of depression compared to those who had not consumed fruits and vegetables in the past 12 months. However, this association was not observed at higher consumption frequencies, possibly due to the limited sample size in these categories, which may have reduced the statistical power needed to detect significant differences. Other potential explanations include the possibility that individuals consuming larger quantities of fruits and vegetables may rely on a limited variety, thereby restricting the range of nutrients obtained. Additionally, the benefits of nutrient intake may plateau at moderate consumption levels. Furthermore, residual confounding from unmeasured variables, such as differences in nutrient absorption, food preparation methods, or mental health-related behavioral changes influencing dietary choices (reverse causality), could also contribute to the observed patterns. Despite methodological differences, numerous large cohort studies emphasize a significant association between fruit and vegetable consumption, with the most prominent studies particularly highlighting berries, citrus fruits, and green leafy vegetables, and a reduced risk of depression and improved mental health.55,56 Notwithstanding, our study found no significant association between processed meat consumption and any assessed psychiatric outcomes, despite previous research linking processed meat to depression.45,46,57,58 Discrepancies in findings may arise from variations in the frequency and quantity of processed meat consumption within our study population, the duration of exposure that was assessed, or disparities in dietary reporting methodologies. Furthermore, unmeasured confounders, such as sodium or preservative content in the specific processed meats consumed, as well as differences in the integration of these foods into the wider diet, could have had an impact on the results.
Our study revealed no significant associations between levels of physical activity and broad psychiatric diagnoses, including depression and post-traumatic stress disorder (PTSD). These findings align with those of a prior study conducted within the same cohort, which similarly reported no associations between physical activity and anxiety or depression, but identified fatigue and dyspnea as notable predictors of physical inactivity. 18 This suggests that physical inactivity associated with long COVID may be more closely related to physical symptoms rather than having a direct impact on psychiatric outcomes, or it may manifest in the future. The assessment of physical activity levels in our study was conducted using a self-reported questionnaire that reflected the week preceding follow-up evaluations, a methodology that is prone to inaccuracies such as recall bias, social desirability bias, and the propensity to over or underestimate activity levels, 59 which may have limited the accuracy of our findings. Future studies could mitigate these limitations by incorporating objective measures, such as accelerometers or fitness trackers, to provide more reliable assessments of physical activity. Despite this, the significance of physical activity in mental health is well-established, with comprehensive evidence underscoring its protective benefits against depression and anxiety.12,60,61 A systematic review and meta-analysis have illustrated the advantages of exercise-based rehabilitation—encompassing aerobic, resistance, flexibility, and balance training, as well as practices like yoga and Pilates—in alleviating symptoms of long COVID, such as dyspnea, fatigue, and depression. 62 The advanced mean age, low socioeconomic status, and elevated disease severity within our cohort may have constrained our findings. Further inquiry is warranted to elucidate the relationship between physical activity and psychiatric outcomes in individuals affected by long COVID, along with an exploration of the potential for targeted interventions within this demographic.
Among the covariates, being male and older age were linked to lower odds of CMD, PTSD, and suicidal ideation. Considering the unadjusted P-value, lower socioeconomic status was associated with higher odds of GAD and CMD. Female gender was also associated with all our outcomes, showing the importance of considering it as an important covariate in post-COVID studies. In fact, anxiety and depression were more prevalent among females and individuals with lower socioeconomic status during the pandemic, as observed in studies across different populations.63,64 The finding that older age was protective for CMD, PTSD, and suicidal ideation in our sample has also been reported in large studies during the pandemic65-68 and might be mediated by higher resilience and coping strategies expressed by older adults. 67 It should not be inferred that older adults are immune to elevated levels of psychological burden, as our study revealed significant levels of all diagnoses spread across all age groups. Furthermore, although body mass index (BMI) at the time of admission was included as a covariate to evaluate its possible impact due to its intrinsic relationship with lifestyle behaviors, it demonstrated no significant correlation with any psychiatric outcome in the current study.
Our study has some limitations. First, the cross-sectional design limits the ability to infer causality between lifestyle factors and psychiatric outcomes. Second, the reliance on self-reported data for dietary habits and substance use may introduce recall bias, as well as social desirability bias, affecting the accuracy of the information provided. Third, we did not conduct a mediation analysis examining the relationship between pre-COVID psychiatric history, sedative use, and alcohol consumption. As a result, pre-COVID psychiatric history remains a potential confounder that has not been fully addressed. Additionally, the study population was composed of survivors of moderate to severe COVID-19 from a single hospital, which may limit the generalizability of the findings to other settings or populations. The exclusion criteria for reinfections, which are based on clinical symptoms rather than PCR testing, may have inadvertently excluded individuals with more severe cases. Statistical limitations were encountered due to the existence of categories comprising fewer than ten data points. In order to address this issue, specific values from various categories, including pork consumption and processed meat consumption, were consolidated; instances defined as “once a day” and “more than once a day” were classified together as “daily.” This adjustment may have influenced the outcomes of the analysis. Future studies could incorporate objective measures (e.g., biomarkers or validated tools) to reduce bias and expand the sample to include diverse populations and milder COVID-19 cases to address these limitations. Additionally, ensuring adequate sample sizes, confirming reinfections with PCR testing, and minimizing data consolidation would improve the accuracy and generalizability of the findings.
In conclusion, this study underscores the correlation between lifestyle factors, including substance use—specifically sedatives, opioids, and alcohol—and the consumption of fruits and vegetables in safeguarding psychiatric outcomes among survivors of COVID-19. This highlights the necessity of incorporating lifestyle considerations into the care of individuals experiencing long COVID. Future investigations should aim to examine these predictors via longitudinal studies to gain a deeper understanding of how these variables can influence psychiatric symptoms. Furthermore, there is a pressing need to undertake clinical trials that explore lifestyle interventions. From a clinical perspective, health care providers ought to prioritize lifestyle assessments and the implementation of integrated care strategies. Concurrently, public health initiatives should concentrate on enhancing awareness and promoting resources that encourage healthier behavioral choices to improve mental health outcomes in this population.
Supplemental Material
Supplemental Material - Exploring the Relationship Between Lifestyle and Post-COVID Psychiatric Symptoms: Findings from a Brazilian Cohort
Supplemental Material for Exploring the Relationship Between Lifestyle and Post-COVID Psychiatric Symptoms: Findings from a Brazilian Cohort by Sophia Aguiar Monteiro Borges, Guilherme Pimenta Roncete, Felipe Couto Amendola, Marcus Vinicius Zanetti, Euripedes Constantino Miguel, Geraldo Busatto Filho, Orestes V. Forlenza, Rodolfo Furlan Damiano, and HCFMUSP COVID-19 Study in American Journal of Lifestyle Medicine.
Footnotes
Author contributions
Conceptualization and Manuscript Drafting: S.A.M.B., R.F.D.; Follow-up Interviews: S.A.M.B., G.P.R., F.C.A.; Data Collection: S.A.M.B., G.P.R., F.C.A.; Data Analysis: S.A.M.B., R.F.D.; Supervision: R.F.D. within the HCFMUSP COVID-19 Study Group (The HCFMUSP COVID-19 Study Group is Eloisa Bonfá, Edivaldo M. Utiyama, Aluisio C. Segurado, Beatriz Perondi, Anna Miethke-Morais, Amanda C. Montal, Leila Harima, Solange R.G.Fusco, Marjorie F. Silva, Marcelo C. Rocha, Izabel Marcilio, Izabel Cristina Rios, Fabiane Yumi Ogihara Kawano, Maria Amélia de Jesus, Carolina Carmo, Clarice Tanaka, Julio F. M. Marchini, Juliana C Ferreira, Anna Sara Levin, Maura Salaroli Oliveira, Thaís Guimarães, Carolina dos Santos Lázari, Ester Sabino, Marcello M. C. Magri, Tarcisio E. P. Barros-Filho, Maria Cristina Peres Braido Francisco, Silvia Figueiredo Costa.); Critical Review and Approval: All authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: S.A.M.B. received a grant from CNPq (process number 106488/2023-6). R.F.D. received a grant from FAPESP (process number #2021/14379-8) and This work was partially supported by donations from the general public under the HC-COMVIDA crowdfunding scheme and the Fundação Faculdade de Medicina (ALA)..
Ethical approval
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.