
Abstract
Objective
There are no reports on the burden of suicidal ideation and suicide attempts in the general population of French Polynesia (FP). We aimed to improve suicide prevention and mental health care by assessing the prevalence of suicide risk and major mental health disorders and care among adults in FP.
Methods
We conducted the Mental Health in General Population Survey in FP during 2015 to 2017. Participants were selected using the quota method to obtain a representative sample of the general population. Suicide risk and psychiatric diagnoses were assessed using the Mini International Neuropsychiatric Interview.
Results
We included 968 people aged 18 years or older. The prevalence of current suicidal ideation (13.1%) and current (2.6%) and lifetime suicide attempts (18.6%), as well as mental health disorders (42.8%), was high in FP. A notable proportion of participants with these conditions did not seek medical assistance.
Conclusion
A high prevalence of suicide risk and mental health disorders was found in the general population of FP. Suicide prevention and mental health plans are needed in FP that include better access to primary care for the diagnosis and treatment of mental health disorders. Further research is needed to clarify cultural risk and protective factors.
Introduction
Good understanding regarding the prevalence of suicide risk and mental health disorders in the general population, as well as knowledge regarding risk factors for suicide, are important for improving global suicide prevention strategies and mental health care policies. In a cross-national comparison of community surveys conducted in the 1980s in nine countries, the lifetime prevalence of suicidal ideation varied between 2.1% and 18.5% and that of suicidal attempts varied between 0.7% and 5.9%. 1 Similar results have been found in other countries, including the United States. 2 The Multisite Intervention Study on Suicidal Behaviors (SUPRE-MISS) in eight countries examined the frequency of suicide attempts (0.4%–4.2%), planning (1.1%–15.6%), and ideation (2.6%–25.4%) with a variation factor of 10–14 among sites. 3 In other surveys in Western and Asian countries, the nationwide prevalence of suicidal thoughts and behaviors was found to range from 0.9% to 15.9%.4,5 Mental health disorders are frequently associated with suicide attempts,6,7 with a lower rate of suicide attempts among young people. 8 Other meta-analyses suggest a lower prevalence of psychiatric disorders among individuals who report suicidal behavior in low- and middle-income countries. 9
Since 1997, the French cross-sectional survey “Mental Health in the General Population – Images and Realities” or MHGP (Santé Mentale en Population Générale – Images et Réalité, SMPG-IR) has been administered to assess sociodemographic data as well as the prevalence of the most frequent mental health disorders and suicidal behaviors using representative samples of the general population. The MHGP is conducted by the Northern French Psychiatric Epidemiology Association and the French World Health Organization Collaborating Centre in Lille, France, in collaboration with the French Ministry of Health. For each site, approximately 900 participants are recruited in public settings using the quota sampling method. 10 The MHGP survey has been conducted at 76 sites in mainland France, other countries (Algeria, Italy, Belgium, Comoros, Greece, Madagascar, Mauritius, Mauritania, Tunisia, Spain, Morocco, Seychelles, Tonga, and Andorra), and French Overseas Territories in the French West Indies,11–14 the Indian Ocean, and the South Pacific (e.g., New Caledonia). 15
Herein, we describe the results of the MHGP survey in French Polynesia (FP), which aimed to identify the prevalence of suicidal thoughts, suicidal attempts, and mental health disorders in the general population. The objectives were to better identify suicide protective and risk factors, and particularly their link with psychiatric disorders. Our hypothesis was that psychiatric disorders and how they are addressed influence suicidal behaviors. Sociodemographic aspects, such as cultural factors and help-seeking behaviors are also described. We present a more comprehensive analysis of these topics presented in a forthcoming paper. 16
Methods
Sample and questionnaires
The sample included people aged 18 years and older from among the general population of four main islands of FP (total population: 153,408). The study was conducted between October and November 2015 in Tahiti and Moorea and during February 2017 in Huahine and Bora Bora islands. The sample was recruited using the quota method to obtain a representative sample of the general population according to sex, age, employment, and level of education, based on data from the most recent census adjusted for the time of the survey (FP Institute of Statistics, Institut de la statistique de Polynésie française, 2014). Data were collected anonymously by 30 trained interviewers (nursing and psychology students) under the supervision of clinicians, using questionnaires administered during face-to-face interviews. Participants were randomly recruited in public places, with the exception of medical centers. After each interview, missing data were addressed by the supervisor and obtained.
The interviews began with a general presentation of the goals and methods of the study, during which interviewees were informed that their information would remain anonymous, and written informed consent was obtained from each respondent. Participants were then asked a series of open-ended questions in the first (sociodemographic) section of the survey questionnaire and social representations of mental health. In the second section, the Mini International Neuropsychiatric Interview (MINI) 17 was used to obtain psychiatric diagnoses according to criteria of the International Classification of Diseases, Tenth Revision. At the end of the interview, a series of questions on specific cultural aspects was included in a supplementary questionnaire administered to all respondents.
Suicidal behaviors were assessed using the MINI according to three suicide risk categories: low (“wish to be dead” or “desire to hurt oneself in the past month” or “lifetime suicide attempt”), medium (“suicidal ideation in the past month” or “desire to hurt oneself in the past month” and “lifetime suicide attempt”), and high (“suicide attempt in the past month” or “suicidal ideation in the past month” and “lifetime suicide attempt”). We defined high suicide risk as both the medium and high categories.
There is a lack of clear nomenclature and consensus on the definition of suicidal ideation. 18 Some definitions of suicidal ideation include suicide planning and deliberation whereas others consider planning to be a distinct stage. In the MINI, the questions referred to the following definitions: suicidal ideation was defined as thinking about suicide within a scenario of a suicidal act; suicide attempt was defined as the concept of non-fatal suicidal behavior used by De Leo et al., 19 a nonhabitual act “with or without injuries [that] the individual expecting to, or taking the risk, to die or to inflict bodily harm, initiated and carried out with the purpose of bringing about wanted changes.”
The World Health Organization Five Well-Being Index (WHO-5) was used to assess well-being based on a five-question scale (with responses ranging from 0 for never to 5 for always, then multiplied by 4 to give the final score), with a total possible score from 0 to 100. 20
The survey was approved by the ethics committee of the government of French Polynesia (CEPF, Avis No. 55, 24 May 2012). There were no refusals to participate at any stage of the questionnaire assessment.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 21
Statistical analysis
Statistical analysis was performed using R version 3.5.2 (www.r-project.org) and SAS 9.1 software (SAS Institute Inc., Cary, NC, USA). For comparisons, we calculated odds ratios (ORs) with 95% confidence intervals (CIs). Fisher’s exact test was used when the expected number of participants in the group were five or less. A probability threshold of 0.05 was used for statistical significance.
Results
The sample included 968 people aged 18 years and older from four main islands of French Polynesia. The sociodemographic characteristics of the sample (Table 1) reflected the FP census, with 50.6% women. The study population mostly comprised Polynesians (75.6%), followed by Europeans (11.1%), individuals with mixed ethnicity (9.8%), and Chinese participants (1.6%). The prevalence of both medium and high suicide risk, was higher in men than in women (8.6% vs. 6.1%). A higher risk of suicide was found in the age group 18 to 29 years (10.7%; p < 0.01), separated or divorced participants (14.5%; p < 0.01), those with a primary school level education (12.2%; p < 0.01), unemployed individuals (14.6%; p < 0.01), and individuals in the lowest monthly family income group (13.0%; p < 0.01).
Sociodemographic characteristics of the study population and suicide risk level assessed by the MINI questionnaire.

NS, not significant.
*p < 0.05, **p < 0.01, ***p < 0.0001.
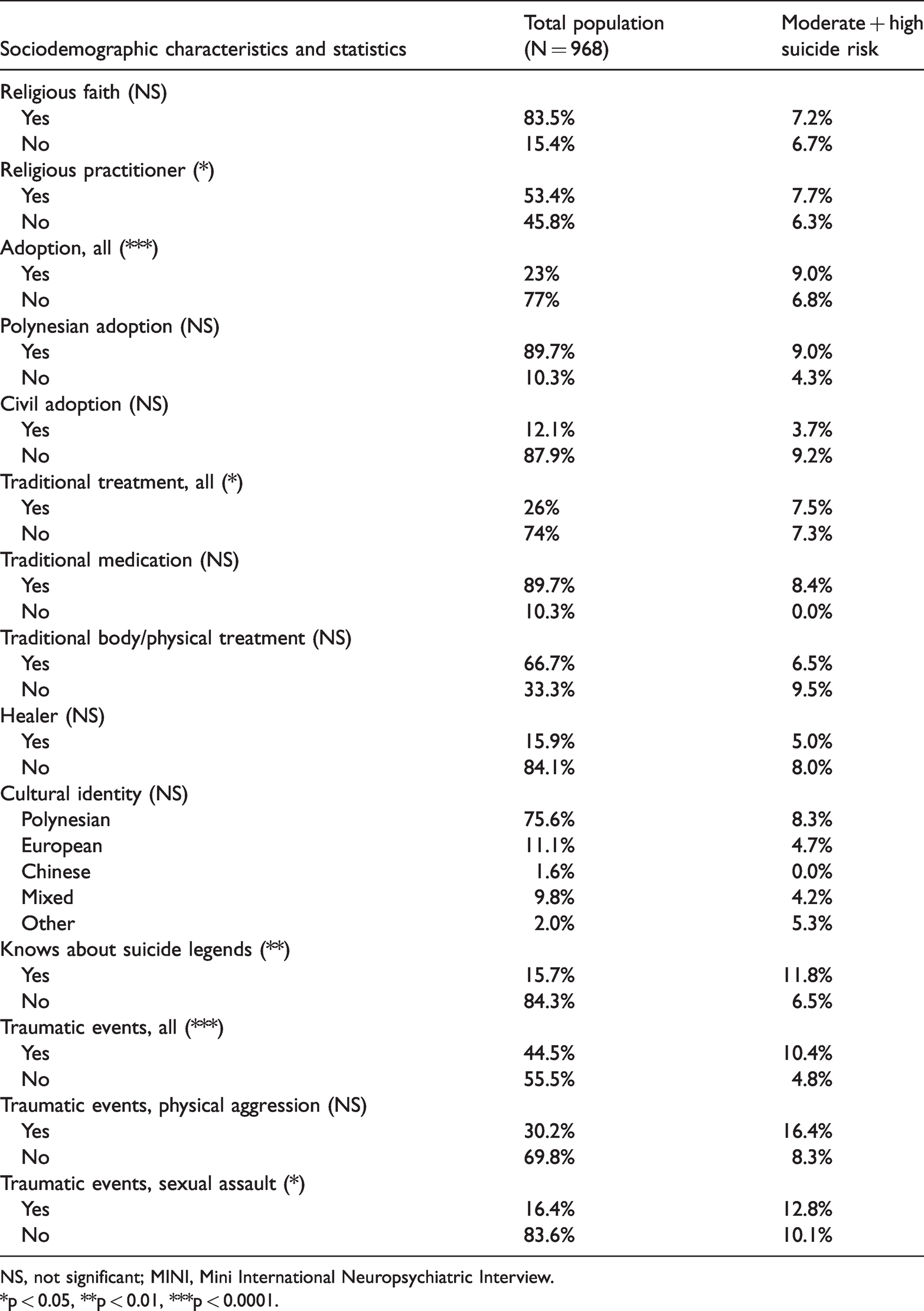
Table 2 shows cultural and clinical characteristics that were associated with a higher suicide risk. Medium and high suicide risk was significantly associated with being adopted (9.0%; p < 0.0001), knowing about Polynesian legends having to do with suicide (11.8%; p < 0.01), experiencing any type of traumatic event (10.4%; p < 0.0001), and experiencing sexual assault (12.8%; p < 0.05). Neither Polynesian ethnicity nor Polynesian adoption was associated with a high suicide risk. Having a religious practice showed a significant association with moderate and high suicide risk, as did receiving traditional treatment and the category of all types of adoption. A low well-being index (WHO-5) score was also a strong suicide risk factor (52.3; p < 0.0001; data not shown).
Cultural characteristics of the population and suicide risk assessed using the MINI questionnaire.
NS, not significant; MINI, Mini International Neuropsychiatric Interview.
*p < 0.05, **p < 0.01, ***p < 0.0001.
Table 3 shows detailed responses to MINI items addressing age and sex. Lifetime suicide attempts were reported by 18.6% of participants. Current (in the past month) suicidal ideation and suicide attempts were reported by 6.6% and 2.6% of participants, respectively. In the present survey in FP, 25 (2.6%) of 968 respondents had made a suicide attempt in the month before the interview. Age, but not sex, was significantly associated with suicidal behaviors, according to MINI criteria. Lifetime suicide attempts were more common in the age group 50 to 59 years (22.9%; p < 0.01), and wishing to harm oneself in the previous month was more commonly reported in the age group 18 to 19 years (10.3%; p < 0.01).
Suicide risk assessed using the MINI questionnaire.

Comparisons are between French Polynesia subgroups.
Suicide risk level: yes to O1 or O2 or O6, ow; yes to O3 or (O2 + O6), moderate; yes to O5 or (O3 + O6), high.
NS: not significant; MINI, Mini International Neuropsychiatric Interview.
*p < 0.05, **p < 0.01.
According to levels of suicide risk, 73.35% of participants in FP were assessed as having no risk, 19.32% as low risk, and 7.33% as medium and high risk (data not shown).
Table 4 presents results regarding mental health disorders found to be associated with a high suicide risk. The global proportion of suicide risk in our study population was 26.7%, with a higher frequency in women than in men (27.8% vs. 25.5%, data not shown). Of this group, 7.3% had a higher (medium and high) suicide risk. The prevalence of having at least one mental health disorder according to the MINI was 42.8%. Nearly all mental health disorders were significantly associated with higher suicide risk (p < 0.05, p < 0.01, p < 0.001). The most frequent disorders were anxiety disorders (26.0%) and mood disorders (20.5%). There were frequent isolated psychotic symptoms, with hallucinations (visuals 13.5%; auditory, 10.3%) and feelings of persecution (18.4%) (data not shown). Among participants reporting mental health disorders, more than half (52.4%) said that the disorder had an adverse impact on their everyday life (data not shown).
Moderate and high levels of suicide risk across individuals with different mental health disorders in French Polynesia.

NS: not significant.
*p < 0.05, **p < 0.01, ***p < 0.0001.
WHO-5 scores were significantly higher in the general population (mean 70.1 ± 21.9; median 72) than among participants with medium and high suicide risk (mean 52.2; median 60; p < 0.001) (data not shown).
Table 5 shows the results of logistic regression analysis and multivariate analysis. Older age and higher WHO-5 scores were significant protective factors against high suicide risk. All other factors (mental health disorders) were significant risk factors for a high suicide risk, especially depressive episodes (OR: 5.0; 95% CI: 2.6–9.6).
Logistic regression to assess moderate and high levels of suicide risk in French Polynesia.

CI, confidence interval.
*p < 0.05, **p < 0.01, ***p < 0.0001.
 Risk factor.
Risk factor.  Protective factor.
Protective factor.
Discussion
Prevalence of suicide risk in FP
This was the first survey aimed at estimating the prevalence of mental health disorders and suicide risk in the general population of FP. The suicide risk (26.7%) in FP was found to be higher than that of all other sites in the survey: 13.7% in the national sample of France; 22 19.6% in New Caledonia, the site closest to FP; 15 15% in the North Pas de Calais Region in France; 23 and 11% in Martinique, 14 another French Overseas Territory.
Considering levels of suicide risk, the proportion of each among participants in FP (no risk: 73.35%; low risk: 19.32%; medium and high risk: 7.33%) was significantly different (p < 0.0001; χ2 = 241.56) compared with these risk levels in the national sample (89.22%, 7.55%, and 3.23%, respectively).
The high prevalence of suicide risk in FP is in contrast to the lower rates of death by suicide in FP 24 as compared with those in France. 25 In the national French sample (39,617 participants), the suicide risk according to the MINI questionnaire was 9.7% for low risk, 2.1% for medium risk, and 1.9% for high risk. 26
In the present survey, 25 (2.6%) of 968 respondents in FP had made a suicide attempt in the previous month. With extrapolation, the number of suicide attempts per year might be as high as 302 (25 × 12 months). In a previous study, 27 only 185 individuals who attempted suicide per year were admitted to the emergency room of the general hospital in French Polynesia and emergency care facilities. The main hypothesis explaining this difference is that seeking medical care is not frequent in FP, which was confirmed in responses to the MHGP sociodemographic questionnaire items. Comparisons among different countries is complex because of different types of representations or definitions of suicidal behavior. For example, the terms “suicidal ideation,” “suicide attempts,” and “suicide” differ widely among countries, which could lead to confusion in completing surveys and the resulting frequencies for each of these terms. 28
We were unable to find data on the distribution of WHO-5 scores in different general populations worldwide. However, in some populations of India and Japan, the WHO-5 score was lower among suicidal individuals than controls, similar to our results in FP. Vijayakumar et al. 29 found that a group of individuals in India with repeated suicide attempts scored lower on the WHO-5 than individuals who made a first suicide attempt (49.6 vs. 58.6; p = 0.01). Similarly, Awata et al. 30 showed that Japanese study participants with suicidal ideation scored significantly lower on the WHO-5 than those without suicidal ideation (45.6 vs. 67.6; p = 0.01). In Estonia, the WHO-5 well-being index score was low (40.44) among individuals who attempted suicide and was correlated with suicide risk scales. 31 Our results suggested that this index could be used in FP to complement other scales to detect suicide risk among the general population and to aid improvement in the management of suicide risk.
Prevalence of mental health disorders and suicide risk in FP
In our study, the lifetime prevalence of any mental health disorder was 42.8%, with mood and anxiety disorders being the most frequent (20.5% and 26.0%, respectively). In our sample, nearly all mental disorders were correlated with a significantly higher suicide risk. The literature indicates that psychiatric comorbidity is the primary risk factor for suicide attempts. Among young people, the presence of any mental health disorder is associated with a greater risk of a suicide attempt; however, some authors have reported that only affective disorders are statistically significant. 8
On the basis of the above findings, the high prevalence of suicide risk in FP could be explained by the high prevalence of mental health disorders, which were found at higher rates than those at all other sites of the MHGP survey. Certain isolated psychotic symptoms that are very frequent, such as hallucinations and feelings of persecution, may contribute to medium or high levels of suicide risk. Single psychotic episodes, however, may differ in terms of psychopathology from recurrent episodes, which are more likely to involve schizophrenia or chronic psychosis. Paradoxically, the lowest rates of suicide and suicide risk was in the French West Indies (Martinique), despite an excess prevalence of psychosis in the general population. 13 Another survey showed a higher suicide attempt rate (18%) in a population with psychiatric disorders in Martinique. 32 We could not find an explanation for these contradictory data.
The high prevalence of suicide risk in FP may also be owing to cultural aspects. A higher suicide risk was present among participants who knew of Polynesian legends about people who died by suicide. This may be a facilitating factor because individuals may unconsciously feel it is permissible to act out in accordance with stories in their culture. 33 Our finding could also suggest that people who know of these legends have suicidal ideation and look for answers in well-known cultural references.
We found a higher prevalence of suicide attempts (18.6%) than suicidal ideation (13.1%, which is a total of “ideas to harm oneself” [6.6%] and “thoughts about suicide” [6.6%]). The relative over-reporting of suicide attempts by Polynesians could explain the higher suicide risk in FP proportional to suicide rates. A higher prevalence of suicide attempts compared with suicidal ideation has also been reported in a few other countries, such as Sri Lanka. 4 These findings could be related to impulsive suicidal behavior, which is more frequent in clinical practice than scenarios involving careful preparation with the expression of suicidal ideation.
This interpretation, i.e., a greater impulsiveness in acting out, hence, less preparation for a suicide attempt, is consistent with the observation that deaths by suicide are less frequent in FP than in France, although suicide attempts are more frequent in FP. In FP, suicide attempts may be less frequently lethal because people present during a suicide attempt (e.g., family or friends) can act quickly to help and care for the suicidal individual.
Addiction can have an amplifying effect on other disorders. Additionally, acculturation could be an explanatory factor in suicide attempts as well as for other disorders. Among Hawaiian youths, high levels of acculturation are identified as a risk factor for suicide attempts. 34 Specific migrant populations and ethnic minorities have a higher risk of suicidal behavior than native populations, including a higher risk of death by suicide. 35 Polynesian society is a society in transition and migration between islands within French Polynesia is common. Finally, a history of child abuse has been identified as a risk factor for suicidal behavior in other studies among general populations, similar to our study findings. 36
Implications for prevention
The discrepancy between high rates of suicide attempts in the general population and relatively low suicide death rates in FP requires further investigation. We identified certain protective factors against lethality of suicide attempts that could explain this discrepancy. Being a religious practitioner may not prevent suicidal ideation but could prevent acting on suicidal thoughts. This may be owing to an individual’s belief in a spiritual force that can help them to control their actions or a belief that only God can decide whether one lives or dies. Additionally, the use of traditional medicine and family structure may not influence impulsiveness in acting out but may protect against severity of a suicide attempt. As mentioned above, the presence of others who can intervene and prevent a lethal suicide attempt. As we noted previously, half of individuals who attempted suicide did not seek help from a medical professional, were not well screened, and did not receive proper care. 27 Primary (i.e., nonselective) prevention strategies should be developed in the community to promote mental health and help-seeking behaviors, which can contribute to reducing the risk of dying by suicide. To make medical care more acceptable in the Polynesian population, religion or traditional medicine (e.g., herbal medications, body treatments) can be integrated with Western medicine. A pilot suicide prevention trial using this cultural approach is currently being tested, with encouraging preliminary results, 37 which are better thus far than those of a previous suicide prevention strategy using the START study protocol. 38
Limitations and strengths
Use of the MINI questionnaire to assess suicide risk and mental health disorders is not common in the literature. Comparisons with other surveys using different methods (other questionnaires, no face-to-face interviews, sampling methods other than the quota method), may introduce bias. 39 However, the MHPG survey used the same questionnaire at all study sites, including for the French national sample. This permitted reliable comparisons across the sample.
The exclusive use of the French language and the necessity to ask standard questions (without explaining them in Tahitian to avoid interviewers’ influence or interpretation) may have led to misunderstanding of the questions, potentially altering the reliability of the results. However, in French Polynesia, the French language is widely used in education, business, justice, and health settings.
Participants were recruited via the quota sampling method, using data from the most recent French Polynesian census. According to self-reports, our sample mostly included Polynesian participants, followed by Europeans, individuals of mixed ethnicity, and Chinese participants. The results regarding specific cultural characteristics (traditional adoption and care, belief in life after death, knowledge of Polynesian legends dealing with suicide, and traumatic events) were used in our analyses. The culture of French Polynesia is very strong and specific. Therefore, the generalizability of our study findings is poor with regard to these cultural aspects. However, their important influence on the risk of suicide means that clinicians and researchers should take sociocultural factors into account in assessing suicidal behavior.
Conclusions
We found a high prevalence of suicide risk, according to the presence of suicidal ideation and attempts and of mental health disorders in the general population of FP, as compared with rates in France and other French territories. Our results showed lower rates of death by suicide in FP than in most countries, including France, with low rates of medical help-seeking behaviors. As assessed using the MINI, the high suicide risk in our population, as compared with other MHGP survey sites was not reflected proportionally in a high rate of death by suicide, as compared with the suicide rates in other countries. Taken together, these results call for the elaboration of a governmental suicide prevention and mental health plan that includes (1) the promotion of mental health in primary care and encouragement of professional help-seeking behaviors, for better identification and treatment of mental health disorders in FP; and (2) further research to identify and use culturally appropriate protective factors to help prevent the acting out of suicidal ideation and/or decrease the severity of suicide attempts.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received grants from the Pacific Fund, an organization of the Ministry of Foreign Affairs of France, the SOS Suicide Association, the Centre Hospitalier de Polynésie française, and le Centre Hospitalier Universitaire de Fort-de-France.