
Abstract
Background
Provider lifestyle counseling is important for improving lifestyles and cardiometabolic disease (CMD) prognosis. However, an examination of the relationship between sociodemographic characteristics, lifestyle modification and provider lifestyle counseling receipt among adults with CMD is scarce. The study examined the prevalence and associations of lifestyle modification and sociodemographic characteristics with provider lifestyle counseling among adults with CMD diagnosis.
Methods
We used cross-sectional data from 2017-2020 National Health and Nutrition Examination Survey (N = 4847). Provider lifestyle counseling (i.e., advice to control/lose weight, exercise, reduce salt, and reduce fat/calories), and lifestyle modification (yes or no) were assessed. Adjusted odds ratios were evaluated using logistic regression models.
Results
Among the sample of adults with CMD, 44.6% received advice to lose weight, 56.1% to exercise, 36.1% to reduce salt, and 43.9% to reduce fat/calories. Adults who made lifestyle modifications had higher odds of receiving advice to lose weight (OR: 1.81), exercise (OR: 1.95), reduce salt (OR: 2.23) and reduce calories (OR: 2.66). Age, sex, race/ethnicity, educational attainment, and insurance were associated with provider lifestyle counseling.
Conclusion
Provider lifestyle counseling is generally suboptimal among U.S. adults with lifetime diagnosis of CMD, and the odds of counseling receipt differ by sociodemographic characteristics and lifestyle modification. CMD control should involve training providers to increase lifestyle counseling.
Keywords
“In our study focused on adults with a diagnosis of CMD, racial and ethnic minorities had higher odds of receiving provider lifestyle counseling.”
Introduction
Despite advances in cardiovascular and metabolic care, cardiometabolic disease (CMD) is a leading preventable contributor to mortality and disease burden globally.1,2 Indeed, CMD is responsible for approximately 50% of non-communicable disease deaths and 25% of disability-adjusted life years lost globally. 3 In the United States (U.S.), 50 million adults have a diagnosis of CMD, 4 and CMD accounts for about 422 billion of U.S. health care costs annually, 5 providing evidence that CMD remains a critical public health issue that needs to be addressed. Pathophysiological mechanisms behind CMD including endothelial dysfunction, insulin resistance, systemic inflammation, DNA methylation, and ferroptosis have been discussed in the literature.6-9 Notably, the burden of CMD persists disproportionately among underserved communities including racial/ethnic minorities, individuals with low income, uninsured, and low educational attainment.2,5 For example, African American and South Asian adults are more likely to be diagnosed with and die from CMD complications compared to white adults, 2 while adults with low socioeconomic status and the uninsured are more likely to have poor CMD control.10,11
Prior research has evaluated cardiometabolic protective therapeutics in primary and secondary CMD prevention; however, the utility of provider lifestyle counseling and lifestyle modification has not been thoroughly investigated in adults with CMD.12,13 CMD is difficult to control as it can be present long before becoming clinically apparent, 14 thus health care providers have an essential role in addressing CMD disparities by identifying adults predisposed to lifestyle risk factors and advising for lifestyle modifications. Lifestyle modifications including increasing physical activity or exercise, dietary changes (i.e., reducing salt, fat or calorie intake), and weight loss are the cornerstone for CMD treatment and are generally recommended as initial therapy or as an adjunct to pharmacotherapy.13,15,16 However, health care providers tend to manage and treat CMD with multiple medications as opposed to prescribing lifestyle modifications, thus increasing the risk of complications, side effects and costs.13,17 The importance of providers prescribing lifestyle modification for adults with CMD risk factors is well-established in the literature. For example, Wijesuriya et al found that implementing a lifestyle modification program for South Asian young adults reduced their incidence of CMD, 18 Neter et al found that lifestyle modifications including weight reduction, reduction of caloric intake, and increased physical activity reduced CMD risk significantly for adults, 19 and Lin et al. found that lifestyle counseling improved lifestyle behaviors and reduced cholesterol, blood pressure, weight, and glucose levels among adults with cardiovascular disease risk factors. 20 Despite these findings, and public health recommendations for providers to routinely advise healthy lifestyle changes, lifestyle counseling from health care providers remains low in the U.S. for adults with and without chronic conditions.17,21
There is a paucity of research investigating the prevalence of provider lifestyle counseling among adults with CMD diagnoses, and whether lifestyle modification and sociodemographic characteristics are associated with provider lifestyle counseling for U.S. adults with CMD specifically. Given the CMD disparities borne by adult members of structurally marginalized populations, 5 and the influence providers have on promoting lifestyle modification for adults, these concepts are important to understand as they may aid in informing health care interventions and public health policies prioritizing CMD control.
The current study utilizes a nationally representative data and aims to: (1) examine the prevalence of provider lifestyle counseling, and lifestyle modification among U.S. adults diagnosed with CMD, and (2) investigate the associations between sociodemographic characteristics, lifestyle modification and provider lifestyle counseling among U.S. adults with CMD diagnosis
Methods
Data
We analyzed data from the 2017-2020 National Health and Nutrition Examination Survey (NHANES), a cross-sectional, nationally representative survey of the civilian noninstitutionalized US population. NHANES employs a complex, stratified multistage cluster sample design to estimate the prevalence of health, nutrition, and potential risk factors among the US population. 22 Interviews and physical examinations were conducted to obtain data on sociodemographic characteristics, lifestyle characteristics, body measurements, and medical conditions during the cycle. Additional information about NHANES sampling methods and survey design can be found online. 22 The NHANES data is publicly available and deidentified and thus this study’s use was deemed exempt from review by the University of Mississippi Medical Center’s Institutional Review Board. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline. 23
Participants
A total of 15,560 participants completed the 2017-2020 NHANES. Questions about CMD were only administered to participants ages 20 years and older, thus for our analysis we excluded participants if they were ages 19 and younger (n = 6328). Further participants were excluded if they did not report being told by a doctor or health professional that they had CMD during their lifetime (n = 3423) as this study focused on adults with a lifetime diagnosis of CMD. Participants who had missing information on CMD (n = 67), provider lifestyle counseling (n = 16), lifestyle modification (n = 10), and sociodemographic characteristics (n = 869) were excluded. Details of exclusion criteria are shown in the study flow chart (see Figure 1). The final analytic sample included 4847 adults with lifetime diagnosis of CMD. Flow chart of study.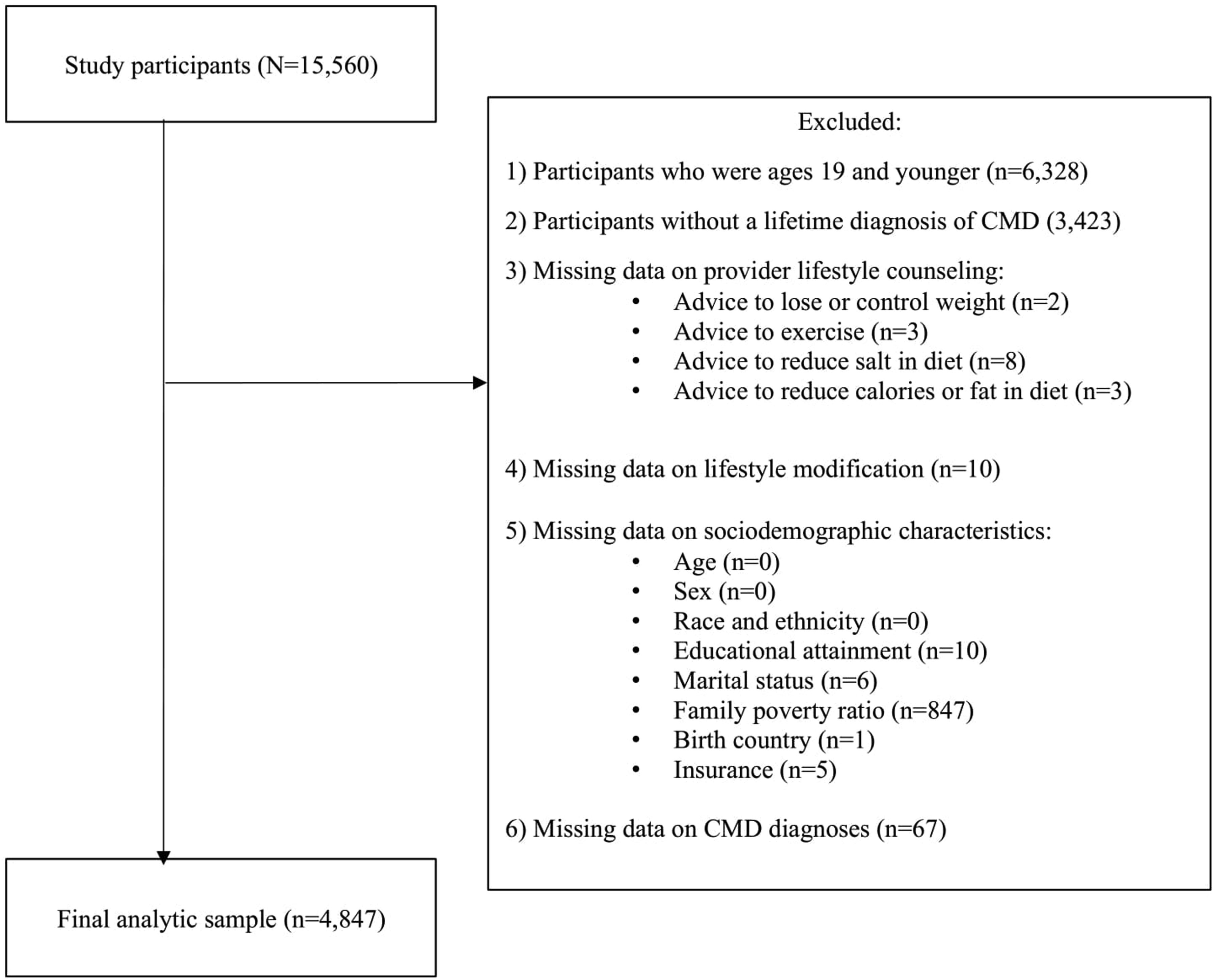
Primary Measures
Sociodemographic Characteristics
Sociodemographic characteristics included age (20-39 years, 40-59 years, 60 years and older), sex (female, male), race/ethnicity (Mexican American, Other Hispanic, Non-Hispanic White, Non-Hispanic Black, Other races including multiracial), educational attainment (less than high school, high school graduate/GED, associate degree, college graduate or above), family poverty ratio (<1.3 (lowest income), 1.3-<3.5, 3.5 and > (highest income)), marital status (married, not married), country of birth (the U.S., foreign country), and health insurance coverage (yes, no).
Lifestyle Modification
Lifestyle modification was defined from participants’ responses (yes or no) to each of the following questions, “Are you now doing any of the following: (1) controlling your weight or losing weight; (2) increasing physical activity or exercise; (3) watching or reducing the amount of sodium or salt in your diet; (4) watching or reducing the amount of fat or calories in your diet.” We categorized lifestyle modification as yes (i.e., yes to one or more lifestyle changes), and no.
Provider Lifestyle Counseling
Provider lifestyle counseling was defined from participants’ responses (yes or no) to each of the following questions, “To lower your risk of a certain disease, during the past 12 months have you ever been told by a doctor or health professional to: (1) control or lose weight; (2) increase your physical activity or exercise; (3) reduce salt in your diet; (4) reduce the amount of fat/calories in your diet.”
Cardiometabolic Disease
CMD was defined as provider diagnosis of coronary heart disease, stroke, myocardial infarction, diabetes, obesity, hypercholesterolemia, or chronic kidney disease during lifetime. CMD diagnosis was obtained from participants’ responses (yes or no) to the questions, “Has a doctor or other health professional ever told you that you had coronary heart disease?”, “Has a doctor or other health professional ever told you that you had stroke?”, “Has a doctor or other health professional ever told you that you had a heart attack?”, “Have you ever been told by a doctor or other health professional that you have diabetes or sugar diabetes?”, “Has a doctor or other health professional ever told you that you were overweight?”, “Have you ever been told by a doctor or other health professional that your blood cholesterol level was high?”, and “Have you ever been told by a doctor or other health professional that you had weak or failing kidneys?”. Participants who responded yes to one or more of the questions above were included in the analysis as this paper focused on adults with a lifetime diagnosis of CMD.
Statistical Analysis
Weighted percentages and confidence intervals of sociodemographic characteristics, lifestyle modification, and provider lifestyle counseling were examined. Sociodemographic characteristics, and lifestyle modification by provider lifestyle counseling were evaluated using chi-square tests of independence. Further pairwise tests were conducted to compare among sociodemographic groups using chi-square tests of independence or Fisher’s exact tests when appropriate. Univariable and multivariable logistic regression models for each outcome (i.e., provider advice to control/lose weight, exercise, reduce salt in diet, and reduce fat/calories) were performed to examine associations between sociodemographic characteristics, lifestyle modification and provider lifestyle counseling among adults with CMD. The outcome referent group was no provider lifestyle counseling. In addition, a multivariable logistic regression evaluating the relationship between sociodemographic characteristics and lifestyle modification among adults with CMD was conducted; outcome referent group was no lifestyle modification. Adjusted odds ratios and 95% confidence intervals are reported. Results were considered statistically significant at α = 0.05. Data were analyzed using Stata 18.0. We accounted for the NHANES complex survey design and adjusted for the probability of non-response by using the svy command. Following the recommendations of the NHANES analytic guidelines, 22 the sample weights specific to the NHANES 2017-March 2020 pre-pandemic data were used.
Results
Descriptive Characteristics
Participant Characteristics of U.S. Adults Diagnosed With Cardiometabolic Disease in the National Health and Nutrition Examination Survey, 2017-2020 (N = 4847).
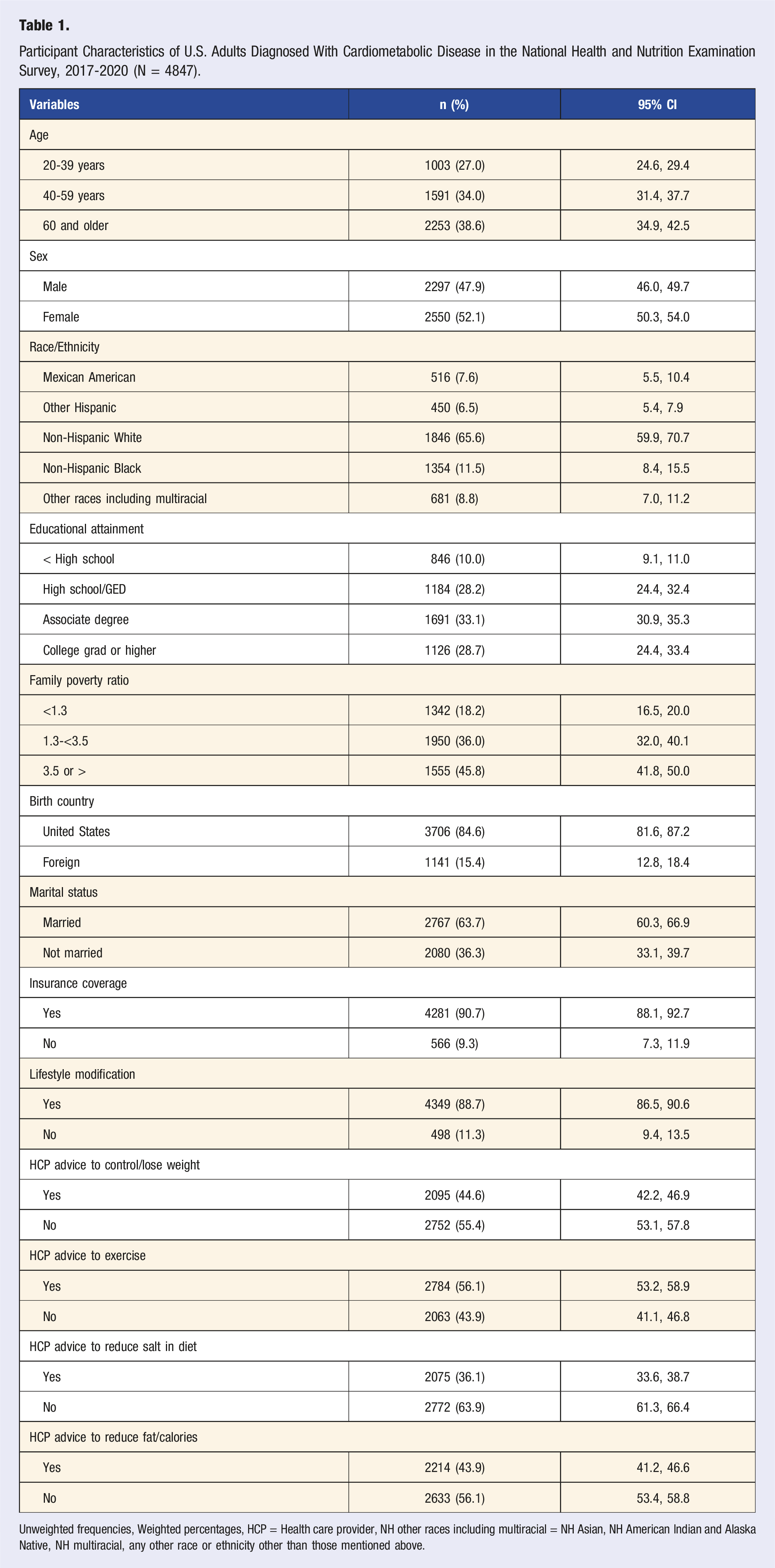
Unweighted frequencies, Weighted percentages, HCP = Health care provider, NH other races including multiracial = NH Asian, NH American Indian and Alaska Native, NH multiracial, any other race or ethnicity other than those mentioned above.
Provider Lifestyle Counseling by Sociodemographic Characteristics and Lifestyle Modification in U.S. Adults With Cardiometabolic Disease (N = 4847).
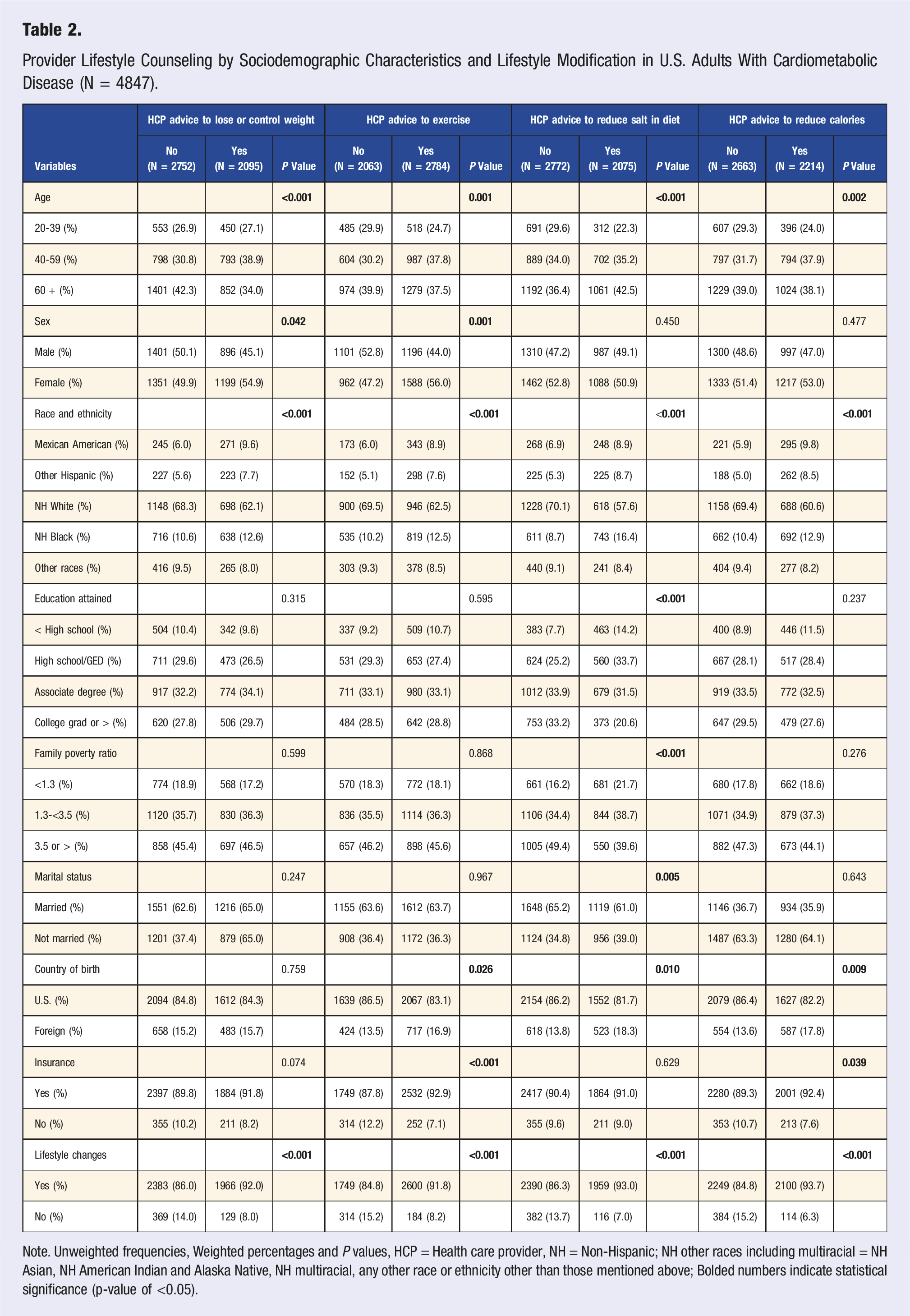
Note. Unweighted frequencies, Weighted percentages and P values, HCP = Health care provider, NH = Non-Hispanic; NH other races including multiracial = NH Asian, NH American Indian and Alaska Native, NH multiracial, any other race or ethnicity other than those mentioned above; Bolded numbers indicate statistical significance (p-value of <0.05).
Logistic Regression
Univariable Logistic Regression Estimating Associations Between Sociodemographic, Lifestyle Modification and Provider Lifestyle Counseling Among Adults With Cardiometabolic Disease (n = 4847).
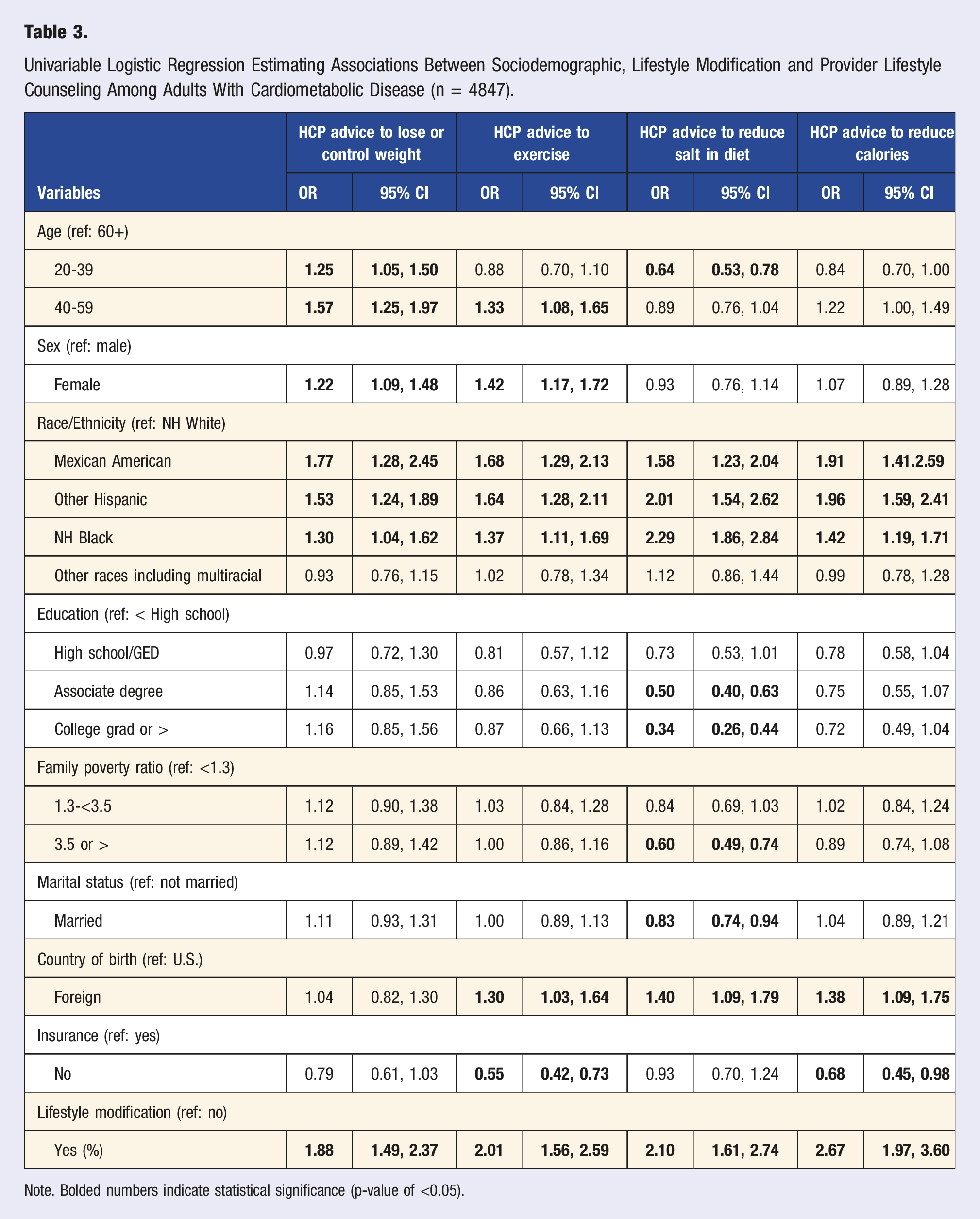
Note. Bolded numbers indicate statistical significance (p-value of <0.05).
Multivariable Logistic Regression Estimating Associations Between Sociodemographic, Lifestyle Modification and Provider Lifestyle Counseling Among Adults With Cardiometabolic Disease (n = 4847).
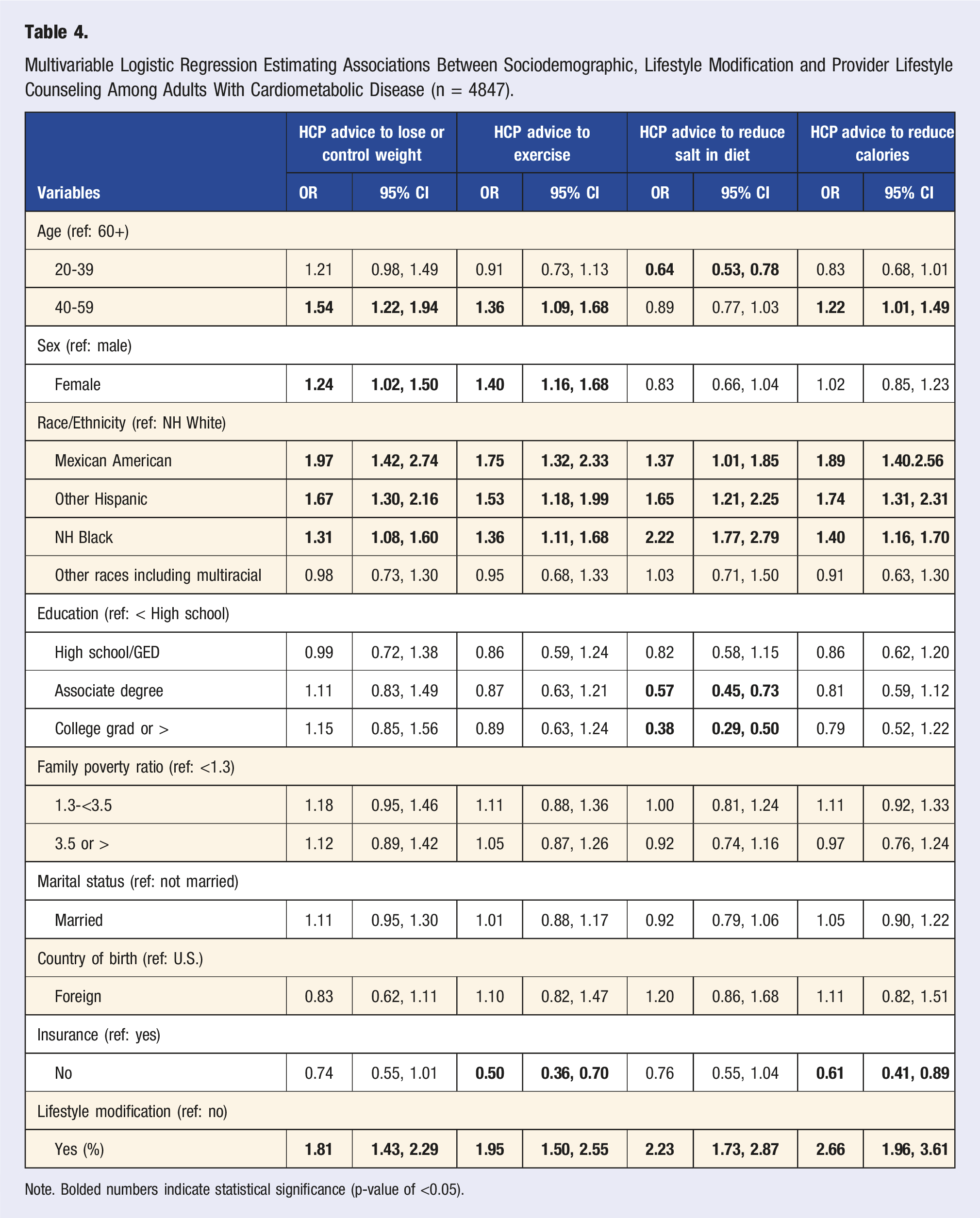
Note. Bolded numbers indicate statistical significance (p-value of <0.05).
Discussion
The current study examined the prevalence of provider lifestyle counseling among U.S. adults diagnosed with CMD, and the associations between lifestyle modification, sociodemographic characteristics, and provider lifestyle counseling. In general, we found that providers are not routinely prescribing lifestyle modification for U.S. adults with CMD, with more than half of adults with CMD diagnosis not receiving advice to lose weight, reduce salt in diet, and reduce fat/calories. Notably, current lifestyle modification was associated with receipt of provider advice to lose weight, exercise, reduce dietary salt and calories, providing further evidence of the utility of provider lifestyle counseling. Furthermore, provider lifestyle counseling receipt differed based on sociodemographic characteristics. Taken together, these findings suggest that providers may be missing a chance to appropriately use lifestyle counseling as a cost-effective and humanizing approach to prevent and address CMD disparities. Our findings mirror previous work that found provider lifestyle counseling continues to be suboptimal among U.S. adults with chronic conditions.17,21,24,25 This is a cause for concern because of the known efficacy of lifestyle counseling and lifestyle modifications in CMD control.18,20,26-28 Potential reasons for the low rates of lifestyle counseling such as provider’s perceptions of lifestyle modification effectiveness, lack of knowledge and confidence in counseling skills, non-adherence, and inadequate time have been discussed in the literature.29-31 Therefore, more medical education and residency training programs focused on improving provider lifestyle knowledge, counseling skills, and efficacy perceptions are needed to increase provider lifestyle modification prescriptions,32,33 and subsequently patient lifestyle modifications that could aid in reducing the mortality attributable to CMD.
Previous studies assessing sociodemographic differences in provider lifestyle counseling receipt have reported varying odds for racial and ethnic minorities compared to white adults.34-36 In our study focused on adults with a diagnosis of CMD, racial and ethnic minorities had higher odds of receiving provider lifestyle counseling. These findings are promising because adults who are members of racial/ethnic minority groups are impacted disproportionately by CMD and thus may require more attention from their providers.21,34 Moreover, similar to prior research, 17 females were more likely than males to receive provider advice to lose or control weight and exercise. However, in contrast, a recent study found that among obese adults with diabetes, females were less likely to report receiving lifestyle counseling. 34 The current study is one of the first to examine sociodemographic differences in receipt of provider lifestyle counseling among adults with CMD, thus future research that explores the complexities in sex and gender identity with regards to receipt of provider lifestyle counseling is warranted. Significant disparities in CMD outcomes exists for underserved communities,37-39 and thus the study’s finding that adults who were males and uninsured were less likely to receive lifestyle counseling further emphasizes the need for community-based interventions that make lifestyle counseling accessible and affordable for the uninsured and males. 17 Interestingly, adults aged 20-39 and adults with higher than high school educational attainment reported lower likelihood of receiving provider advice to reduce salt in diet. Although older adults have higher risks of CMD mortality, 37 the incidence of CMD among younger adults has skyrocketed in the past two decades.40,41 Similarly, CMD risk is more pronounced for the uneducated, 42 thus it is important for providers to tailor lifestyle counseling to ensure it is understandable, feasible, practical and meeting the needs of adults with CMD regardless of age and education level. 43
In addition to the impact of lifestyle counseling on patient lifestyle modification and CMD control,18,20,27 previous research indicates that lifestyle counseling also reduces the likelihood of burnout among providers and increased their feelings of accomplishment due to improved patient outcomes. 44 Therefore, health care policies and clinical training that require providers to routinely and optimally deliver lifestyle counseling to adults with CMD is critical for CMD control and for improving patient-provider relationships. Further, more culturally appropriate and sensitive community-based participatory efforts promoting lifestyle modifications in underserved and structurally disadvantaged communities are needed. 45 Public health promotion and prevention campaigns that focus on increasing provider awareness of the low rates of counseling for young adults, males, uninsured and uneducated may aid in increasing provider lifestyle counseling among these population groups. Future longitudinal research is needed to further examine lifestyle and sociodemographic differences in the receipt of provider lifestyle counseling among adults with diagnoses of CMD.
Limitations
The results of our study should be interpreted in light of several limitations. First, we relied on self-reported responses on CMD diagnoses, lifestyle modification and provider lifestyle counseling, which may be subject to recall and response bias. Second, the NHANES data is cross-sectional and thus causality cannot be inferred. Third, because of the nature of the NHANES data, we could not examine other provider lifestyle counseling advice (e.g., cessation of tobacco, marijuana and alcohol use), provider type or specialty, clinic type setting, duration of counseling, and quality of counseling provided. Fourth, CMD diagnoses were based on report of a health care provider diagnosis of CMD during lifetime, and examination of current CMD diagnosis might differ. However, the study’s use of a large nationally representative dataset may foster extrapolation of these findings to contemporary populations.
Conclusion
This study’s findings provide evidence of an association between lifestyle modification, sociodemographic characteristics and provider lifestyle counseling among U.S. adults diagnosed with CMD. The findings reinforce the importance of provider’s counseling for lifestyle modifications such as dietary changes, increasing physical activity or exercise, and losing or controlling weight. These findings also indicate the need for health care policies and interventions that require providers to consistently provide lifestyle counseling to adults with a diagnosis of CMD or predisposed to CMD risk due to structural disadvantages. Future research is needed to further explore “why” health care providers are not providing this service, as it may be multi-factorial existing beyond just a lack of knowledge and time. Further, the development and implementation of culturally sensitive lifestyle medicine curriculums in medical and health professions education and residency training programs are essential going forward to increase provider lifestyle counseling for adults. Public health efforts should prioritize community-based programs that ensure lifestyle counseling is accessible and affordable for all adults diagnosed with CMD including the uninsured and uneducated.
Supplemental Material
Supplemental Material - Provider Lifestyle Counseling Among Adults With Cardiometabolic Disease Diagnosis Differs by Sociodemographic Characteristics and Lifestyle Modification: NHANES 2017-2020
Supplemental Material for Provider Lifestyle Counseling Among Adults With Cardiometabolic Disease Diagnosis Differs by Sociodemographic Characteristics and Lifestyle Modification: NHANES 2017-2020 by Osayande Agbonlahor, Abigail Gamble, Caroline Compretta, Joshua R. Mann, Josie Bidwell, and Brian D. Williams in American Journal of Lifestyle Medicine
Footnotes
Author Contributions
O.A. Conceptualization, Methodology, Formal Analysis, Data interpretation, Writing—original draft, Writing—review and editing. A.G. Conceptualization, Methodology, Writing—review and editing. C.C. Conceptualization, Methodology, Writing—review and editing. J.R.M. Conceptualization, Methodology, Writing—review and editing. J.B. Conceptualization, Writing—review and editing. B.D.W. Conceptualization, Writing—review and editing. All authors have read and approved the final manuscript as submitted to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.