
Abstract
Objective. The current study examined the use of stimulus control, self-monitoring, and reinforcement by youth, parents, and interventionists as related to weight management in lifestyle intervention programs. Design. Secondary analysis of an existing data set was used to integrate the results of 14 published, randomized treatment–control intervention trials for overweight youth aged 2 to 18 years. Main outcome measure. Between-group differences in weight-related outcomes, including weight, body mass index (BMI), and percentage overweight, measured at the end of treatment, were used to calculate effect sizes for each treatment–control comparison. Additionally, average effect sizes were calculated among sets of comparisons sharing similar approaches to implementing behavioral techniques. Results. Treatment programs that taught youth to use stimulus control, taught youth to self-monitor, and taught parents to use reinforcement, produced significantly larger effect sizes than programs that did not include these components. The beneficial effects of these specific behavioral techniques appeared to be amplified when used with multiple key individuals. Conclusion. This initial study quantitatively demonstrated significant benefits associated with teaching youth stimulus control and self-monitoring, and teaching parents reinforcement to shape health behaviors in lifestyle interventions for pediatric overweight. Furthermore, teaching youth and parents the same techniques may contribute to better weight-related outcomes. These findings and descriptive information on how techniques were described, taught, and delivered may guide future research efforts aimed at identifying and examining the most effective behavioral components to include in brief interventions.
Quantitative reviews of treatments for child and adolescent overweight also support the use of behavioral techniques as part of a multicomponent approach to treatment.
To date, the majority of interventions targeting pediatric overweight* have incorporated behavioral modification techniques aimed at improving diet and physical activity. 1 Notably, both the American Dietetic Association 2 and the Expert Committee on the treatment of child and adolescent overweight and obesity 3 recommend behavioral intervention as a component of treatment. Considerable empirical support exists for programs that incorporate some combination of techniques such as stimulus control, self-monitoring, contingency management, goal setting, and modeling.4,5 Other recommended strategies include problem solving, cognitive restructuring, parent skills training, and relapse prevention. 3 These elements are similar to the most common behavioral strategies used to treat weight problems in adults. 6
Qualitative reviews consistently emphasize the benefits associated with multicomponent behavioral treatments. For example, a review of empirically supported treatments for pediatric overweight identified comprehensive programs with behavioral modification components as having the greatest support. 7 Additionally, a review of 16 randomized family-based interventions found increases in the number of behavioral techniques were associated with increases in weight loss for both parents and their children. 8
Quantitative reviews of treatments for child and adolescent overweight also support the use of behavioral techniques as part of a multicomponent approach to treatment. One of the earliest meta- analytic reviews 9 found that programs that used behavioral modification techniques produced greater weight loss, Cohen d = 0.76, than programs that did not, d = 0.10. A meta-analytic review by Snethen et al 10 also found that interventions combining some form of diet, physical activity, behavioral modification, and parental involvement produced significant positive effects on weight loss in children aged 6 to 16 years. Wilfley et al 11 also found that youth who participated in lifestyle interventions, defined as programs including any combination of diet, activity, and/or behavioral training, had better outcomes than no-treatment wait-list controls as well as information/education- only controls.
Importantly, previous reviews note the need for additional research to determine which specific behavioral components have the greatest effects on treatment outcomes.9-13 Identification and closer examination of the most effective techniques is important for several reasons. Although multicomponent treatments are successful, it is possible that program outcomes are due primarily to a specific component or subset of components. A streamlined treatment may be more cost-effective 13 and may also help stem the problem of attrition believed to be especially problematic in clinical settings. 14 Brief interventions may be especially beneficial in settings such as primary care where there may be limited resources to implement intensive treatment. 15 However, studies vary in descriptions of behavioral components for interventions for pediatric overweight, including who was taught or employed the technique. Researchers may benefit from more specific information about potentially effective components, information that can guide future research in this area.
One method for examining this issue is via meta-analysis, examining whether the presence of specific behavioral modification techniques is associated with better program outcomes. We are aware of no studies examining this issue in studies on lifestyle interventions for pediatric overweight. We did identify one meta-analysis of prevention programs that reported findings regarding specific behavioral techniques. 16 This review included randomized controlled trials with children and adolescents aged 2 to 18 years. Positive trends were found for 2 specific techniques: The use of reinforcement was associated with increased physical activity and improved diet, and the use of 2 or more cognitive restructuring techniques was associated with increased physical activity and decreased sedentary behavior. In the pediatric intervention literature, we did identify a recent meta-analysis 17 examining 11 studies that compared comprehensive behavioral interventions with the same package with an added treatment component (eg, added emphasis on increasing physical activity or reducing sedentary behavior). The results suggested that higher doses of behavioral techniques and expanded targets for intervention were associated with better outcomes. However, the study only examined broad categories of techniques preventing identification and examination of specific behavioral components.
As a first step to better understanding specific behavioral techniques in lifestyle interventions for pediatric overweight, the current study used secondary analysis of an existing data set 1 to estimate the impact of the presence of specific behavioral techniques that appear to be promising in multicomponent lifestyle interventions for pediatric overweight. Secondary analysis is an acceptable approach in this case, as comprehensive or multicomponent behavioral treatments have been implemented in similar ways for at least 2 decades and consistently found to be the preferred treatment modality.7,9,12 Of interest in the current study are 3 behavioral modification techniques, namely stimulus control (environmental change to promote positive health behaviors), self-monitoring or monitoring (recording specific health behaviors), and reinforcement (rewarding positive health behaviors). These techniques were chosen because of their ubiquity in behavioral treatments, their identification as 3 important behavior skills in the treatment of pediatric obesity, 15 and their availability in the primary data set. Because parent involvement is highly recommended and common in the treatment of youth who are overweight, 18 we also distinguish each of these techniques in terms of whether it is the youth, the parent, or the interventionist who is using (or being taught to use) the technique.
The analyses addressed whether treatment effects varied significantly depending on (a) the presence or absence of specific behavioral techniques; (b) how many of these techniques were used in the multicomponent treatment; (c) sets of techniques taught to youth, parents, or interventionists; (d) whether only the youth or parent versus both the youth and parent were taught the behavioral technique; and (e) whether the behavioral technique was taught to one or to multiple key individuals. Additionally, we provide descriptive information regarding the frequency of use and how these techniques were described, taught, and implemented.
Methods
Literature Review
The literature search strategy involved review of more than 60 previous reviews, including reference lists cited in these reviews and more than 39 000 abstracts identified through computer searches of PsycInfo, Dissertation Abstracts, and PubMed. A total of 865 studies were identified based on Boolean combinations of keywords (ie, related to intervention, overweight, age) and individually examined. Selection criteria to identify studies for review in the original data set are shown in Table 1. The original study identified 76 studies for review (40 treatment– control comparisons and 36 alternate treatment comparisons). Additional details pertaining to the literature search and selection criteria for the original data set may be found elsewhere. 1
Selection Criteria for Original Data Set a
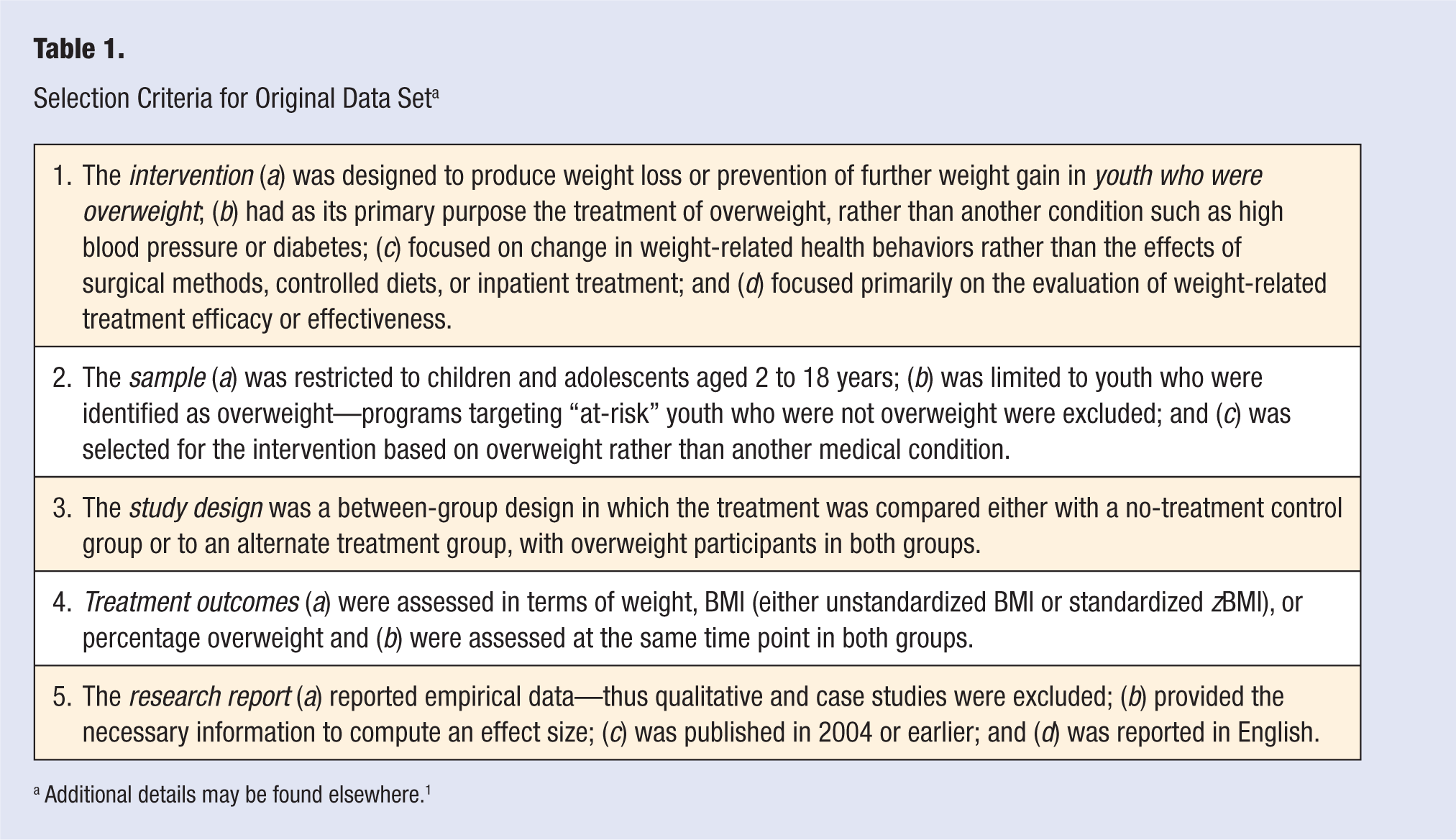
Additional details may be found elsewhere. 1
As an initial step in examining specific behavioral modification techniques, the current study focused on a subset of the original data set. Specifically, the current study focused on those studies within the larger data set that were (a) published, (b) used randomization, and (c) included treatment–control comparisons for overweight youth aged 2 to 18 years. This decision was made based on the preliminary and descriptive nature of the study. Specifically, we hoped to include those studies with the most rigorous research methodology. Further support for exclusion of unpublished studies was found in the larger meta-analysis, which revealed a lack of publication bias in the larger set of treatment–control studies. 1 This resulted in the identification of 14 studies.19-32 Several studies included extra treatment groups19,22,26 allowing examination of a total of 18 treatment–control comparisons. Interventions targeted weight loss or weight gain prevention among overweight youth via behavior changes in youth, parents, or both youth and parents. Descriptions of each intervention are provided in Table 2.
Descriptions of Behavioral Techniques Taught to Youth, Taught to Parent, and Employed by Interventionist
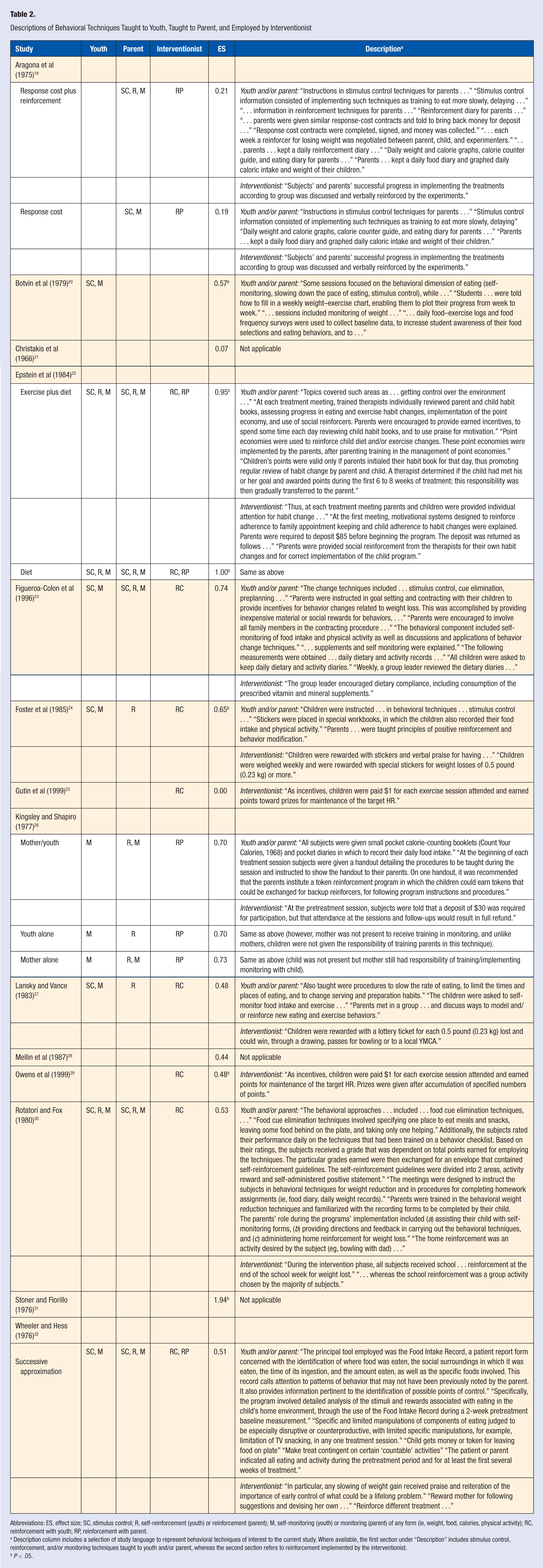
Abbreviations: ES, effect size; SC, stimulus control; R, self-reinforcement (youth) or reinforcement (parent); M, self-monitoring (youth) or monitoring (parent) of any form (ie, weight, food, calories, physical activity); RC, reinforcement with youth; RP, reinforcement with parent.
Description column includes a selection of study language to represent behavioral techniques of interest to the current study. Where available, the first section under “Description” includes stimulus control, reinforcement, and/or monitoring techniques taught to youth and/or parent, whereas the second section refers to reinforcement implemented by the interventionist.
P < .05.
Coding Procedures
A coding manual (available from the first author) was developed by the research team and included operational definitions of a variety of factors related to study characteristics, design, and treatment approach. Each intervention was coded in terms of whether or not the techniques of (a) stimulus control, (b) self-monitoring, and (c) reinforcement were used. For the current study, monitoring was further subdivided into categories representing weight, eating, calories, and activity, as well as a fifth variable that represented monitoring in any of these forms, to reflect the diversity of methods used by researchers in this literature to assess monitoring. For each of these techniques, a distinction was made between whether the youth was taught the technique, the parent was taught the technique, or (for reinforcement only) the interventionist used the technique. This resulted in 16 codes, representing whether or not the youth was taught to use stimulus control (1 code), to self-monitor (5 codes), or to use self-reinforcement (1 code); whether or not the parent was taught to use stimulus control (1 code), monitoring (5 codes), or reinforcement to shape youth behavior (1 code); and whether or not the interventionist used reinforcement to shape youth (1 code) or parent (1 code) behavior.
Studies were coded by advanced doctoral students and doctoral-level researchers, with disagreements resolved by consensus. Effect sizes were calculated as Cohen d 33 (using the pooled standard deviation) with the analysis software of Shadish et al. 34 Group comparisons could be based on posttest scores or on change scores (taking into account the intraclass correlation); in both cases, however, effect sizes represented between-group differences at end of treatment, rather than within-group change from baseline. Results reported simply as “not statistically significant” were estimated conservatively as d = 0.0. 35 Other details regarding the statistical calculation of effect size can be found elsewhere. 1
Statistical Analyses
Effect sizes were first calculated for individual studies. In treatment–control studies, an effect size that is significantly different from 0 means that outcomes in the treatment group are significantly different from the control group. Average effect sizes were also calculated for sets of studies that shared important characteristics. For example, an average effect size was calculated for the set of treatments that taught the child to use stimulus control, and another average effect size was calculated for treatments that did not teach the child to use stimulus control. The Qb statistic was then used to test whether one of these effect sizes was significantly larger than the other. In the case of treatment–control studies, a statistically significant Qb value means that differences between participants and controls at the end of treatment were significantly greater in one type of treatment (or one set of treatments) than in another. Finally, some analyses used multiple regression to examine whether certain treatment characteristics were significantly correlated with the average effect size in a set of studies.
Results
Study Characteristics
The 14 studies used in the current analyses examined samples of youth aged 2 to 18 years, with an average age of 12 years. Three samples were all female; the other samples were 42% to 79% female. The samples included youth who were 10% to 80% overweight. One study explicitly ruled out severely overweight participants, one study explicitly did not rule out these participants, and the remaining studies did not provide information about this selection criterion. All studies included interventions that were compared with a no-treatment control; however, some control groups were placed on waiting lists or had an understanding they would receive treatment at a later point19,22,25,26,28,30 and one study 27 also included a self-selected control group consisting of those families who chose not to participate. There was considerable diversity in terms of which behavioral components were included in each program. The components that were most commonly included were youth self-monitoring of eating (61%), parents monitoring youth’s eating (50%), and interventionists reinforcing the youth (50%). Other components were present in 17% to 44% of the programs (see Table 3).
Relation of Behavioral Techniques Taught to Youth, Taught to Parent, or Employed by Interventionist to Treatment Outcomes
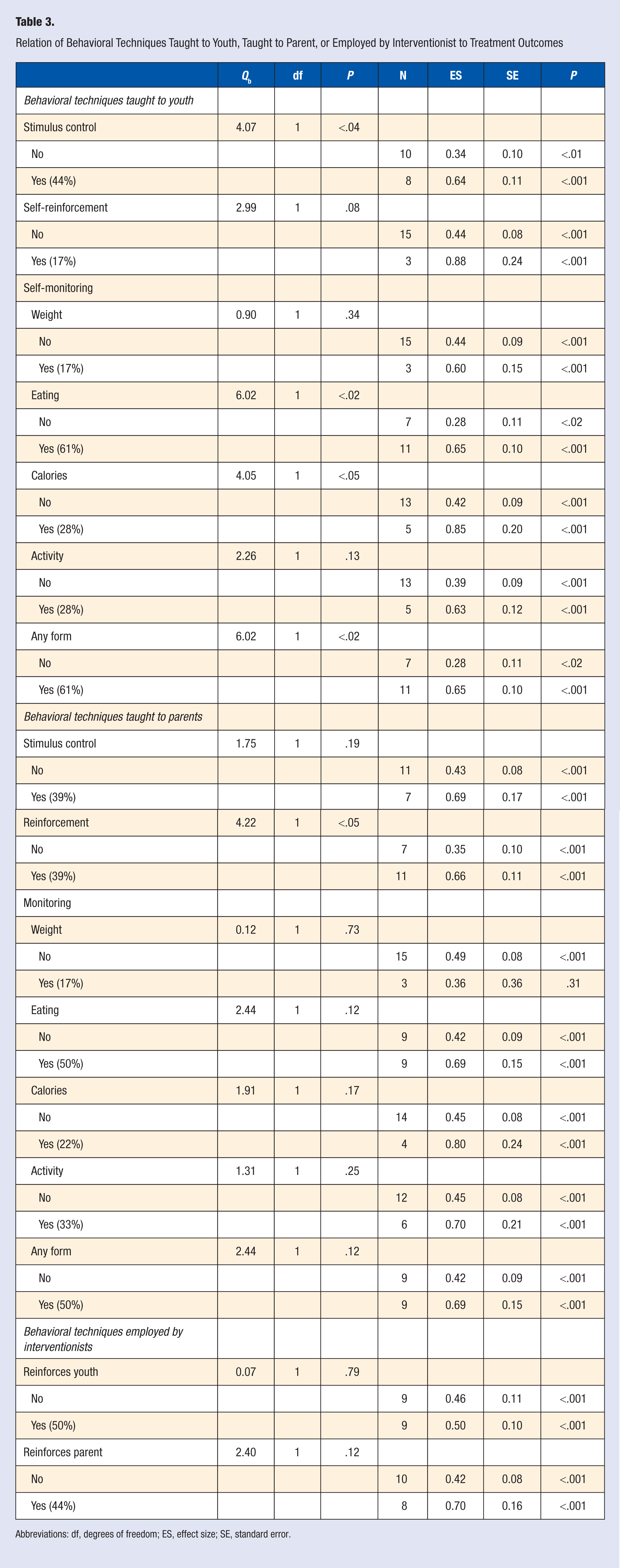
Abbreviations: df, degrees of freedom; ES, effect size; SE, standard error.
Overall Treatment Effects
Individual comparison-level effect sizes in the 18 randomized treatment–control comparisons ranged from d = 0.00 to d = 1.90. The overall average effect size was d = 0.48, standard error (SE) = 0.07, N = 18, a value that was significantly different from 0 at P < .001. This suggests that as a group, participants in these 18 treatment programs showed significantly better weight management compared with controls at the end of treatment.
Specific Behavioral Techniques and Weight Outcomes
Treatment programs were coded in terms of whether or not they used each of the 16 behavioral techniques listed in Table 3. The results showed significantly larger effect sizes in programs including 5 of the 16 techniques, and a trend toward significance in one other. In comparisons between treatments and control groups, treatment programs that taught the youth about stimulus control produced significantly larger effect sizes than those that did not. Treatment programs teaching the youth to self-monitor eating and calorie intake were also associated with significantly larger effect sizes, as were those teaching the youth about self-monitoring in any form, as compared with programs that did not include these techniques. Effect sizes were also significantly larger in treatment programs where parents were taught to use reinforcement than in those that did not include this technique, and there was a trend toward larger effect sizes in programs where the youth was taught to use self-reinforcement as compared with those that did not include this component. Although the other results were statistically nonsignificant, the pattern of means was in most cases in the expected direction (see Table 3).
Although the treatments could be reliably coded in terms of whether or not each specific behavioral technique was included as a component of treatment, it should be noted that there was variability in how the technique was described and implemented across studies. Descriptions of these various methods for teaching behavioral techniques are included in Table 2.
Number of Techniques Used
Regression analyses were used to assess the association between number of techniques and effect sizes. The number of techniques used in treatment ranged from 0 to 12 (out of a possible 16). There was a significant correlation between the number of behavioral techniques used in the treatment and overall effect size, with R2 = .33, N = 18, P < .02.
Who Was Taught the Technique
The behavioral techniques were grouped as techniques taught to the youth, techniques taught to the parent, and techniques used by the interventionist (reinforcement with the youth or parent). No one set explained significant variance in effect sizes; for behavioral techniques used with youth, R2 = .43, N = 18, nonsignificant; for parent behavioral techniques, R2 = .31, N = 18, nonsignificant; and for the 2 interventionist variables, R2 = .13, N = 18, nonsignificant.
We tested the possibility that using the same technique with both the youth and a parent would produce larger effect sizes than using the technique with only one or the other. The results showed findings approaching a trend toward significance in the case of four techniques. In treatment–control comparisons, treatments that taught both the parent and youth about reinforcement tended to produce larger effect sizes than programs that taught reinforcement to only one of them, Qb(1) = 2.99, P = .09. Similar trends were found for teaching the parent and youth to monitor eating, Qb(1) = 3.33, P < .07; to monitor calories, Qb(1) = 3.54, P < .06; and to use monitoring in any form, Qb(1) = 3.33, P < .07.
There were 3 programs in which reinforcement was used by multiple key individuals to shape behavior. These were programs in which the youth was taught to use self-reinforcement, the parent was taught to use reinforcement to shape youth behavior, and the interventionist used reinforcement to shape child or parent involvement in treatment. Together, these programs had a relatively large average effect size of d = 0.88, P < .001, suggesting that consistency across multiple key individuals may be a key to treatment effectiveness.
Discussion
Behavioral modification has been identified as a core component of successful lifestyle interventions targeting pediatric overweight7,9 and current evidence-based guidelines recommend behavioral interventions as a part of treatment.2,3 However, less is known about the effectiveness of specific behavioral modification techniques. Research in this area may be especially important for developing brief and cost-effective empirically supported interventions. This study represents a first step to better understanding this issue by using secondary data analysis of an existing data set 1 to examine the inclusion of 3 specific behavioral components (ie, stimulus control, monitoring, and reinforcement) in published, randomized controlled intervention trials targeting pediatric overweight and including treatment–control comparisons.
The current study builds on previous literature by quantitatively demonstrating significant benefits associated with teaching youth to use stimulus control and to self-monitor, and with teaching parents to use reinforcement to shape youth behavior. Furthermore, findings demonstrated that a greater number of techniques were associated with better weight management and that teaching both youth and parents the same techniques may be beneficial. The study also provides descriptive information on the frequency of use of these techniques as well as how the techniques were described, taught, and delivered. This understanding may guide future research.
The results of this study suggest support for all 3 behavioral techniques examined (ie, stimulus control, self-monitoring, and reinforcement). The findings suggest that these 3 specific components should be evaluated further in terms of their value relative to other techniques. One potential benefit is that it may be more efficient to focus on these techniques rather than large multicomponent treatments. Consistent with a previous review, 8 the current study showed that treatment programs that included a greater number of techniques were associated with larger effect sizes. However, no advantage was found depending on which person was taught or used the technique (ie, youth, parent, or interventionist). It appears more important that the specific techniques are simply being used by some key individual. On the other hand, the results did suggest that teaching both parents and their children the same techniques may be more beneficial than targeting one or the other. For example, programs that taught both parents and youth about reinforcement yielded greater weight management than programs that taught only the parent or youth about reinforcement. Similar findings were found for monitoring in general as well as specific forms of monitoring (ie, eating and calories). Additional support for teaching all participants the same technique is provided by the fact that the 3 treatment programs22,30 that taught or used reinforcement across settings (ie, youth, parent, interventionist), each yielded large effect sizes. This consistency across multiple contexts may be a key for increasing the effectiveness of specific behavioral modification components.
Importantly, studies varied in terms of how these behavioral techniques were used in treatment. Researchers’ descriptions of the use of stimulus control and reinforcement were quite varied, making it difficult to create subcategories for coding. For example, several studies stated specifically that “stimulus control” was taught but provided no description such as whether the technique was aimed at changing eating, physical activity, or other behaviors. Those that did provide more descriptive information tended to focus on eating behaviors, for example, teaching the youth to slow rates of eating or change serving habits, 27 or implement techniques to eliminate food cues. 30 Parents were primarily trained to administer reinforcement in the context of contingency contracting, although two programs instead taught parents to provide ongoing positive reinforcement for healthy eating and physical activity behaviors. The target behaviors for reinforcement varied, including weight loss, increased motivation, following program instructions and procedures, healthy eating and exercise behaviors, and leaving food on the plate. Self-monitoring was typically reported in a more consistent manner, with the major form of self-monitoring being focused on eating, followed by calories and physical activity and then weight.
The analyses of self-monitoring excluded 3 studies25,28,31 that reported using brief self-monitoring as a form of assessment or as a method for tracking progress rather than as a form of intervention (ie, 7-day physical activity recall at baseline and 2-day dietary recalls at baseline, 2, 4, 6, and 8 months, “voluntary” weigh-in during weekly treatment sessions, and weigh-in at each treatment session, respectively). Although the use of self-monitoring solely for assessment or tracking purposes was not the focus of the current analyses, it may be a fruitful avenue for future research. Periodic self-monitoring, even just as a measure of treatment outcomes, may prove to be a useful intervention component.
A limitation of the current study is the inability to control for additional intervention strategies contributing to weight management. That is, the majority of studies to date have evaluated treatments that included multiple behavioral components, making it difficult to tease apart the unique contributions specific to each component. Despite this limitation, the current study contributes to the limited literature by identifying and providing additional knowledge regarding 3 specific behavioral techniques that may be well suited for research aimed at more efficient approaches to treatment. Future intervention studies that maximize internal validity will be needed. To date, Epstein et al 36 provide one of the closest attempts. This research compared the addition of reinforcement versus stimulus control as strategies for reducing sedentary behavior to a comprehensive family-based intervention that included other behavioral components. Future studies using this approach will need to specifically control for other intervention effects in an effort to better understand the contributions of specific techniques. We would recommend comparing groups that differ with respect only to one behavioral technique (or a small set of techniques) in order to increase internal validity. This may be accomplished by offering both groups dietary and physical activity information but providing behavioral training in a specific technique or set of techniques to only one group.
A second limitation concerns the fact that the studies included in the current analysis provide a range of detail about the interventions being evaluated. Although all the studies identified the intervention as behavioral in nature, it was sometimes unclear which specific techniques were used, how they were used, and the degree to which they were actually implemented by the interventionists and then by the participants. Three studies21,28,31 provided insufficient information to determine whether the specific techniques of stimulus control, monitoring, and reinforcement were used. For example, Christakis et al 21 reported that diet history reviews were offered as part of the nutritional program but because of lack of information we could not confirm this as a form of monitoring. Other studies did use these specific techniques but did not provide the same training to all participants.24,32 For example, Foster et al 24 provided training in positive reinforcement to only half of participants; similarly, Wheeler and Hess 32 allowed the family to guide the treatment and to collaborate in determining the time line for follow-up visits. In these cases it was difficult to identify specific behavioral techniques that were implemented with all families (rather than just being representative of an average family in these treatments). Future studies should include descriptive information as well as assessments of therapist fidelity and youth and parent adherence to better isolate the effects of specific behavioral strategies. The Consolidated Standards for Reporting Trials (CONSORT) guidelines, 37 which were designed to contribute to improved reporting of interventions, may aid in this effort. Additionally, researchers 38 have suggested standardizing definitions for behavior change techniques.
Future research on behavioral techniques in the treatment of pediatric overweight will benefit from two types of expanded focus. First, the current review focused on 3 behavioral techniques of interest, but other techniques also warrant attention. For example, cognitive restructuring was found to be a significant contributor to positive outcomes in prevention programs for pediatric overweight 16 and is a treatment component recommended by the Expert Committee. 3 Other promising techniques, including goal setting, modeling, problem solving, parent training, and relapse prevention have been identified in previous literature.3-5 Similarly, it may be important to study small sets of techniques (eg, stimulus control and monitoring taught together as part of the same treatment), rather than to consider a technique in isolation. In addition to comparing specific behavioral components researchers may also consider taking a Multiphase Optimization Strategy (MOST) approach 39 where a screening, refining, and optimization phase assist in selecting optimal components. Second, it will be important to expand the definition of positive outcomes in treatment, to include not just changes in weight but also changes in weight-related health behaviors such as eating and physical activity.7,16 Among the 18 interventions in the current study (all of which reported outcomes in terms of weight), only 1 reported outcomes in terms of eating and 2 in terms of physical activity. Future studies may contribute to this knowledge base by examining other health behaviors as well as psychosocial outcomes in addition to weight management.
The current study used secondary data analysis as a first step in examining the effect of specific behavioral techniques on weight management in pediatric lifestyle interventions. Among studies published in 2004 or earlier only 14 met inclusion criteria for this secondary analysis. We do not believe an updated review would affect the findings in the current study because of the small changes in behavioral treatments over time.7,9,12 In fact, our review documents use of behavioral techniques in interventions published across a wide time frame (1966 to 1999). Nevertheless, an updated review may be important for other reasons. For example, with rapid technological advances treatment is now being delivered via a variety of methods (eg, Web-based, tele-medicine) and by a variety of professionals with varying degrees of training and understanding of behavioral theory. Furthermore, several of the studies in the current review were conducted prior to significant rises in rates of obesity, 40 thus more recent interventions may be directed toward novel social and environmental challenges. Findings in our larger data set revealed consistent effect scores over time suggesting that newer programs show similar effects. 1 However, Epstein et al 41 note that rising rates and more stringent inclusion criteria suggest that newer programs may be outperforming earlier attempts thus making this an important area of inquiry.
Although the current study excluded unpublished studies because of the study’s focus and the evidence of no publication bias in the larger data set, 1 the inclusion of unpublished studies in future reviews may allow researchers to assess variables such as delivery methods, producing results that may have greater generalizability to applied settings (eg, primary care, school, mental health). Finally, future studies may seek to examine age as a moderator of treatment effects (ie, it may be that in studies with younger children parental involvement is more important). However, as alluded to previously, a potential barrier to understanding this factor may be the limited descriptive information provided in published trials (eg, results with specified age ranges).
The increasing rates of pediatric overweight mean increasing pressure on primary care providers to intervene. An entire supplement in Pediatrics (2007, volume 120) provided guidelines on the prevention, assessment, and treatment of child and adolescent overweight. However, as described by Saelens and Liu, 15 numerous barriers prevent providers from addressing child overweight, including inadequate time. 42 Research is needed to better understand the most effective components of treatment in order to develop brief interventions. Identification and understanding of the effects of specific behavioral components may facilitate this progress.
The current study is a first attempt at examining specific behavioral components in lifestyle interventions targeting pediatric overweight. The results suggest that the benefits of these interventions may be attributable in part to the inclusion of teaching youth to use stimulus control and self-monitoring, and teaching parents to use reinforcement to shape youth behaviors. Furthermore, consistent with a review of family-based interventions, 8 our findings suggest that teaching a greater number of techniques and the same techniques to both youth and parents may be beneficial. However, these summary analyses should be viewed as preliminary and research should focus on well-designed intervention studies that compare the sole effects of specific behavioral modification techniques. Given the strong evidence for the effectiveness of lifestyle interventions for pediatric overweight, future research may identify the most effective components to include in brief interventions.
Footnotes
Acknowledgements
We thank William S. Frye for assistance with preparing drafts of the article.